

Clinical Manifestations of Infections with the Omicron Sub-Lineages BA.1, BA.2, and BA.5: A Retrospective Follow-Up Analysis of Public Health Data from Mecklenburg-Western Pomerania, Germany

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. 5 May 2023. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic?adgroupsurvey=%7badgroupsurvey%7d&gclid=EAIaIQobChMIqLi84tmagAMVld2yCh2-FAecEAAYASABEgIjPfD_BwE (accessed on 28 September 2022).
- World Health Organization. Weekly Epidemiological Update on COVID-19—28 September 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---28-september-2022 (accessed on 28 September 2022).
- Robert Koch-Institut (RKI). Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). RKI-Coronavirus SARS-CoV-2-Wochenbericht vom 29.9.2022. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2022-09-29.pdf (accessed on 30 September 2022).
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants/ (accessed on 30 September 2022).
- Hu, J.; Peng, P.; Cao, X.; Wu, K.; Chen, J.; Wang, K.; Tang, N.; Huang, A.L. Increased immune escape of the new SARS-CoV-2 variant of concern Omicron. Cell. Mol. Immunol. 2022, 19, 293–295. [Google Scholar] [CrossRef]
- Robert Koch-Institut (RKI). Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). RKI-Coronavirus SARS-CoV-2 Wochenbericht vom 7.7.2022. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Wochenbericht/Wochenbericht_2022-07-07.pdf (accessed on 7 July 2022).
- Lyngse, F.P.; Kirkeby, C.T.; Denwood, M.; Christiansen, L.E.; Mølbak, K.; Møller, C.H.; Skov, R.L.; Krause, T.G.; Rasmussen, M.; Sieber, R.N.; et al. Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: Evidence from Danish Households. medRxiv 2022. [Google Scholar] [CrossRef]
- Abbas, Q.; Kusakin, A.; Sharrouf, K.; Jyakhwo, S.; Komissarov, A.S. Follow-up investigation and detailed mutational characterization of the SARS-CoV-2 Omicron variant lineages (BA.1, BA.2, BA.3 and BA.1.1). bioRxiv 2022. [Google Scholar] [CrossRef]
- Chakraborty, S.; Saha, A.; Saha, C.; Ghosh, S.; Mondal, T. Decoding the effects of spike receptor binding domain mutations on antibody escape abilities of omicron variants. Biochem. Biophys. Res. Commun. 2022, 627, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Loucera, C.; Perez-Florido, J.; Casimiro-Soriguer, C.S.; Ortuño, F.M.; Carmona, R.; Bostelmann, G.; Martínez-González, L.J.; Muñoyerro-Muñiz, D.; Villegas, R.; Rodriguez-Baño, J. Assessing the impact of SARS-CoV-2 lineages and mutations on patient survival. Viruses 2022, 14, 1893. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Sievers, C.; Zacher, B.; Ullrich, A.; Huska, M.; Fuchs, S.; Buda, S.; Haas, W.; Diercke, M.; an der Heiden, M.; Kroger, S. SARS-CoV-2 Omicron variants BA.1 and BA.2 both show similarly reduced disease severity of COVID-19 compared to Delta, Germany, 2021 to 2022. Eurosurveillance 2022, 27, 2200396. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Eales, O.; Steyn, N.; Tang, D.; Bodinier, B.; Wang, H.; Elliott, J.; Whitaker, M.; Atchison, C.; Diggle, P.J.; et al. Twin peaks: The Omicron SARS-CoV-2 BA.1 and BA.2 epidemics in England. Science 2022, 376, eabq4411. [Google Scholar] [CrossRef]
- Tozer, K.; Sjaarda, C.P.; Moslinger, E.; Wong, H.; Mubareka, S.; Maguire, F.; Fattouh, R.; Brabant-Kirwan, D.; Kozak, R.; Sheth, P.M. Comparison of SARS-CoV-2 Viral Loads in the Nasal Mucosa of Patients Infected with BA.1, BA.2, or BA.5 Omicron Lineages. Open Forum Infect. Dis. 2022, 9, ofac564. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, J.; Jiang, L.; Chen, Q.; Fu, Y.; Jin, Y.; Chen, Z.; Tang, F.; Zeng, X.; Wen, H.; et al. Comparison of SARS-CoV-2 aerosol emission from patients with Omicron BA.1 or BA.2 subvariant infection. J. Infect. 2022, 85, e37–e39. [Google Scholar] [CrossRef]
- Webster, H.H.; Nyberg, T.; Sinnathamby, M.A.; Aziz, N.A.; Ferguson, N.; Seghezzo, G.; Blomquist, P.B.; Bridgen, J.; Chand, M.; Groves, N.; et al. Hospitalisation and mortality risk of SARS-CoV-2 variant omicron sub-lineage BA.2 compared to BA.1 in England. Nat. Commun. 2022, 13, 6053. [Google Scholar] [CrossRef] [PubMed]
- Townsley, H.; Carr, E.J.; Russell, T.W.; Adams, L.; Mears, H.V.; Bailey, C.; Black, J.R.; Fowler, A.S.; Wilkinson, K.; Hutchinson, M.; et al. Non-hospitalised, vaccinated adults with COVID-19 caused by Omicron BA.1 and BA.2 present with changing symptom profiles compared to those with Delta despite similar viral kinetics. medRxiv 2022. [Google Scholar] [CrossRef]
- Goller, K.V.; Moritz, J.; Ziemann, J.; Kohler, C.; Becker, K.; Hübner, N.O.; Group, C.-G.S. Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022. Viruses 2022, 14, 2033. [Google Scholar] [CrossRef] [PubMed]
- Tom-Aba, D.; Silenou, B.C.; Doerrbecker, J.; Fourie, C.; Leitner, C.; Wahnschaffe, M.; Strysewske, M.; Arinze, C.C.; Krause, G. The Surveillance Outbreak Response Management and Analysis System (SORMAS): Digital Health Global Goods Maturity Assessment. JMIR Public Health Surveill. 2020, 6, e15860. [Google Scholar] [CrossRef]
- Sass, J.; Bartschke, A.; Lehne, M.; Essenwanger, A.; Rinaldi, E.; Rudolph, S.; Heitmann, K.U.; Vehreschild, J.J.; von Kalle, C.; Thun, S. The German Corona Consensus Dataset (GECCO): A standardized dataset for COVID-19 research in university medicine and beyond. BMC Med. Inform. Decis. Mak. 2020, 20, 341. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 22 September 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 28 September 2022).
- Fonager, J.; Bennedbaek, M.; Bager, P.; Wohlfahrt, J.; Ellegaard, K.M.; Ingham, A.C.; Edslev, S.M.; Stegger, M.; Sieber, R.N.; Lassauniere, R.; et al. Molecular epidemiology of the SARS-CoV-2 variant Omicron BA.2 sub-lineage in Denmark, 29 November 2021 to 2 January 2022. Eurosurveillance 2022, 27, 2200181. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; von Gottberg, A.; Cohen, C. Clinical severity of Omicron sub-lineage BA.2 compared to BA.1 in South Africa. medRxiv 2022. [Google Scholar] [CrossRef]
- Whitaker, M.; Elliott, J.; Bodinier, B.; Barclay, W.; Ward, H.; Cooke, G.; Donnelly, C.A.; Chadeau-Hyam, M.; Elliott, P. Variant-specific symptoms of COVID-19 among 1,542,510 people in England. medRxiv 2022. [Google Scholar] [CrossRef]
- Ballouz, T.; Menges, D.; Kaufmann, M.; Amati, R.; Frei, A.; von Wyl, V.; Fehr, J.S.; Albanese, E.; Puhan, M.A. Post COVID-19 condition after Wildtype, Delta, and Omicron variant SARS-CoV-2 infection and vaccination: Pooled analysis of two population-based cohorts. medRxiv 2022. [Google Scholar] [CrossRef]
- Andeweg, S.P.; de Gier, B.; Vennema, H.; van Walle, I.; van Maarseveen, N.; Kusters, N.E.; de Melker, H.E.; Hahné, S.J.M.; van den Hof, S.; Eggink, D.; et al. Higher risk of SARS-CoV-2 Omicron BA.4/5 infection than of BA.2 infection after previous BA.1 infection, the Netherlands, 2 May to 24 July 2022. Eurosurveillance 2023, 28, 2200724. [Google Scholar] [CrossRef]
- Yamamoto, S.; Matsuda, K.; Maeda, K.; Horii, K.; Okudera, K.; Oshiro, Y.; Inamura, N.; Takeuchi, J.S.; Konishi, M.; Ozeki, M.; et al. Neutralizing antibodies following three doses of BNT162b2 vaccine, breakthrough infection, and symptoms during the Omicron predominant wave. medRxiv 2022. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Muik, A.; Lui, B.G.; Bacher, M.; Wallisch, A.-K.; Toker, A.; Finlayson, A.; Krüger, K.; Ozhelvaci, O.; Grikscheit, K.; Hoehl, S.; et al. Omicron BA.2 breakthrough infection enhances cross-neutralization of BA.2.12.1 and BA.4/BA.5. bioRxiv 2022. [Google Scholar] [CrossRef] [PubMed]
- Hachmann, N.P.; Miller, J.; Collier, A.-r.Y.; Ventura, J.D.; Yu, J.; Rowe, M.; Bondzie, E.A.; Powers, O.; Surve, N.; Hall, K.; et al. Neutralization Escape by the SARS-CoV-2 Omicron Variants BA.2.12.1 and BA.4/BA.5. medRxiv 2022. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef]
- Pulliam, J.R.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | BA.1 | BA.2 | BA.5 | p-Value 1 | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
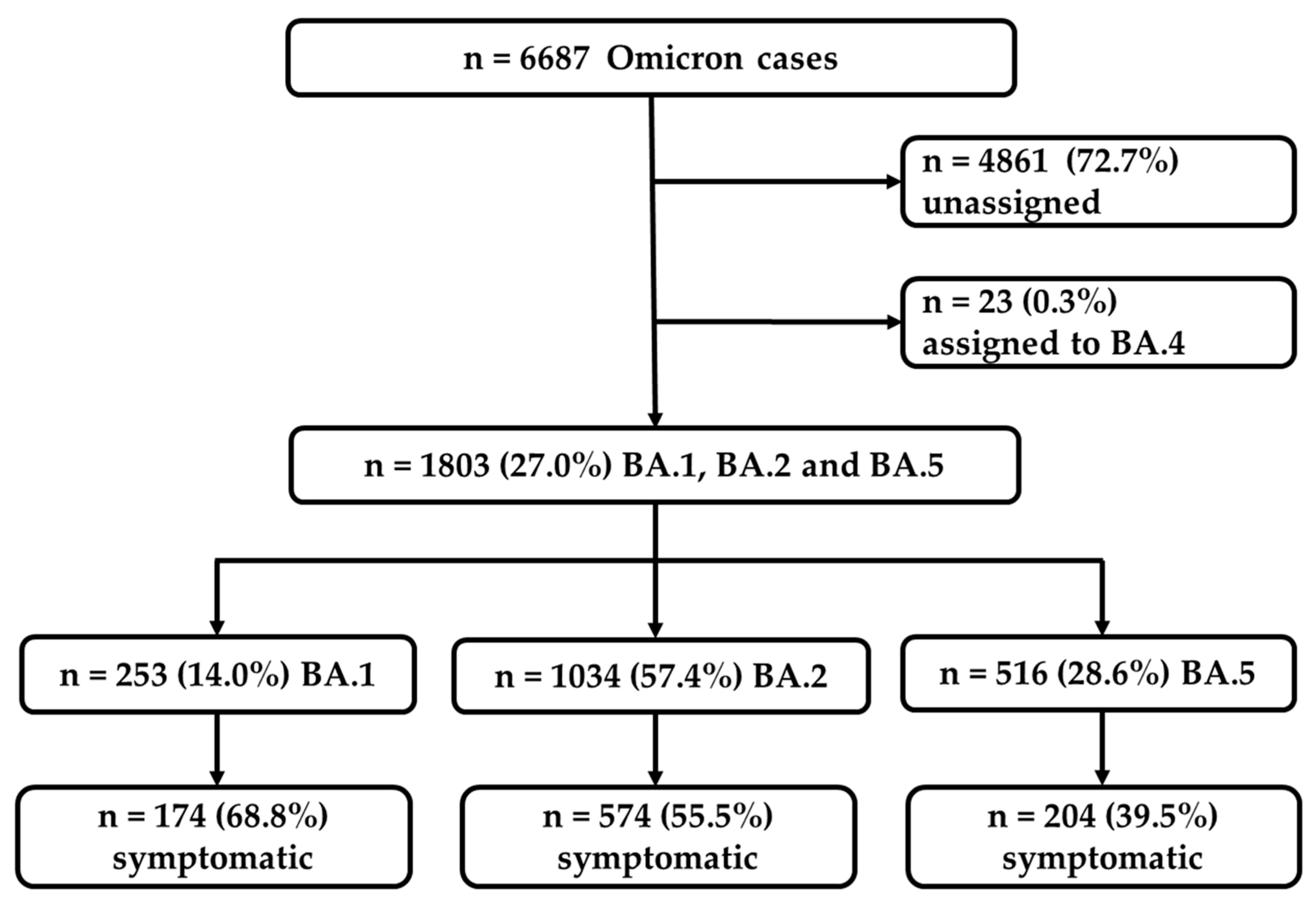
| Total | Cases | 253 | 14.0 | 1.034 | 57.4 | 516 | 28.6 | - |
| Sex | Female | 125 | 49.4 | 537 | 51.9 | 285 | 55.2 | 0.247 |
| Male | 127 | 50.2 | 491 | 47.5 | 231 | 44.8 | ||
| Unknown | 1 | 0.4 | 6 | 0.6 | 0 | 0.0 | ||
| Age groups | 0–19 | 54 | 21.3 | 164 | 15.9 | 49 | 9.5 | <0.001 |
| 20–39 | 70 | 27.7 | 286 | 27.7 | 148 | 28.7 | ||
| 40–59 | 81 | 32.0 | 328 | 31.7 | 200 | 38.8 | ||
| 60–79 | 31 | 12.3 | 180 | 17.4 | 84 | 16.3 | ||
| 80+ | 17 | 6.7 | 73 | 7.1 | 35 | 6.8 | ||
| Unknown | 0 | 0.0 | 3 | 0.3 | 0 | 0.0 | ||
| Symptoms | Yes | 174 | 68.8 | 574 | 55.5 | 204 | 39.5 | <0.001 |
| No | 79 | 31.2 | 460 | 44.5 | 312 | 60.5 | ||
| Unknown | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| Vaccination | Yes | 96 | 37.9 | 354 | 34.2 | 164 | 31.8 | <0.001 |
| No | 41 | 16.2 | 79 | 7.6 | 10 | 1.9 | ||
| Unknown | 116 | 45.8 | 601 | 58.1 | 342 | 66.3 | ||
| Re-infection | Yes | 2 | 0.8 | 10 | 1.0 | 12 | 2.3 | 0.012 |
| No | 116 | 45.8 | 303 | 29.3 | 133 | 25.8 | ||
| Unknown | 135 | 53.4 | 721 | 69.7 | 371 | 71.9 | ||
| Status | Vital | 197 | 77.9 | 588 | 56.9 | 94 | 18.2 | 0.145 |
| Deceased | 2 | 0.8 | 10 | 1.0 | 4 | 0.8 | ||
| Unknown | 54 | 21.3 | 436 | 42.2 | 418 | 81.0 | ||
| Symptom | Status | BA.1 | BA.2 | BA.5 | p-Value 1 | |||
|---|---|---|---|---|---|---|---|---|
| n (%) | CI 95 [%] | n (%) | CI 95 [%] | n (%) | CI 95 [%] | |||
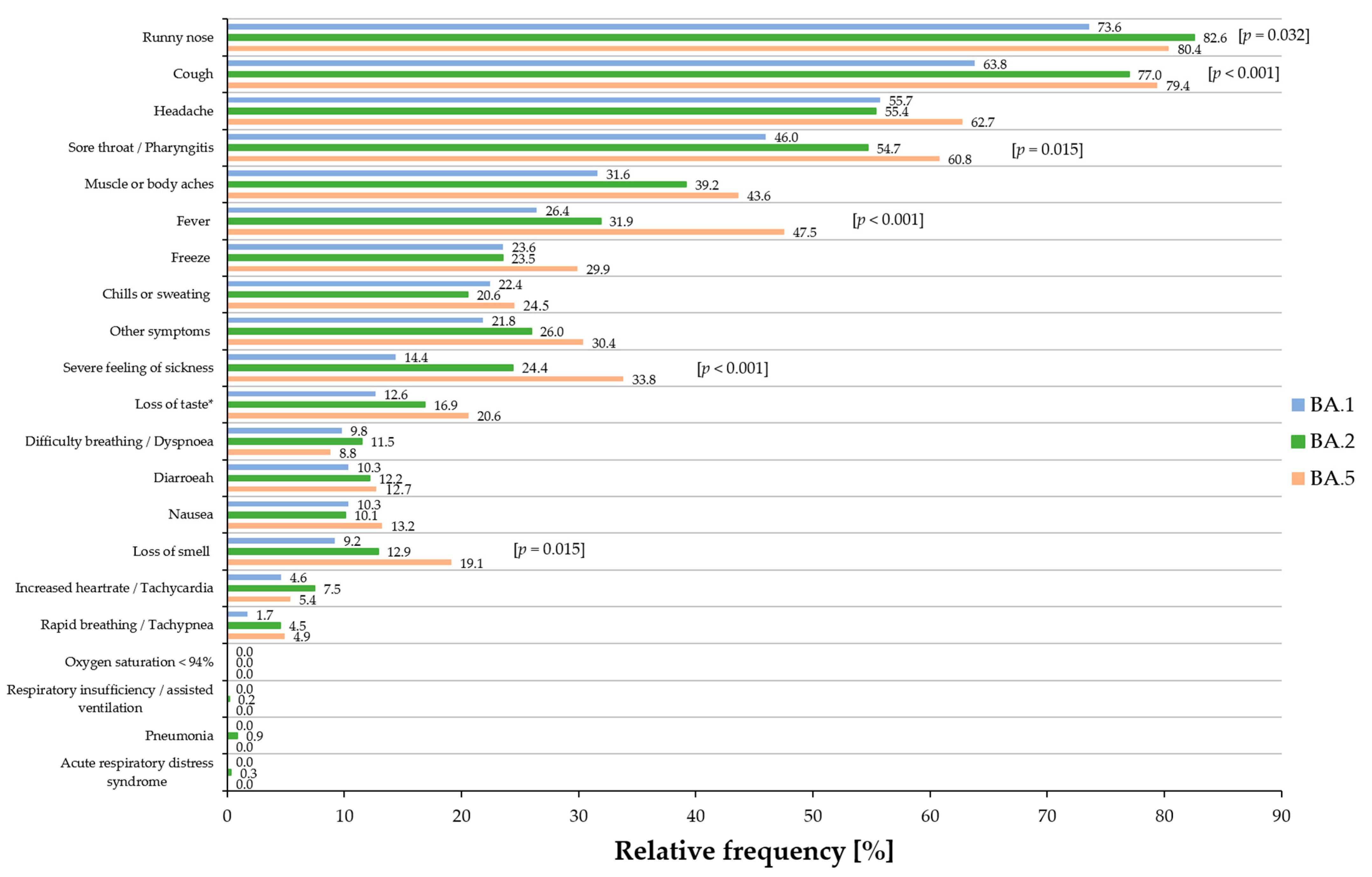
| Runny nose | Positive | 128 (73.6%) | [66.7–79.7] | 474 (82.6%) | [79.3–85.5] | 164 (80.4%) | [74.5–85.4] | 0.032 |
| n.r. | 46 (26.4%) | [20.3–33.3] | 100 (17.4%) | [14.5–20.7] | 40 (19.6%) | [14.6–25.5] | ||
| Cough | Positive | 111 (63.8%) | [56.5–70.7] | 442 (77%) | [73.4–80.3] | 162 (79.4%) | [73.5–84.5] | <0.001 |
| n.r. | 63 (36.2%) | [29.3–43.5] | 132 (23%) | [19.7–26.6] | 42 (20.6%) | [15.5–26.5] | ||
| Headache | Positive | 97 (55.7%) | [48.3–63.0] | 318 (55.4%) | [51.3–59.4] | 128 (62.7%) | [56.0–69.2] | 0.177 |
| n.r. | 77 (44.3%) | [37.0–51.7] | 256 (44.6%) | [40.6–48.7] | 76 (37.3%) | [30.8–44.0] | ||
| Sore throat/pharyngitis | Positive | 80 (46%) | [38.7–53.4] | 314 (54.7%) | [50.6–58.7] | 124 (60.8%) | [54.0–67.3] | 0.015 |
| n.r. | 94 (54%) | [46.6–61.3] | 260 (45.3%) | [41.3–49.4] | 80 (39.2%) | [32.7–46.0] | ||
| Muscle or body aches | Positive | 55 (31.6%) | [25.0–38.8] | 225 (39.2%) | [35.3–43.2] | 89 (43.6%) | [37.0–50.5] | 0.054 |
| n.r. | 119 (68.4%) | [61.2–75.0] | 349 (60.8%) | [56.8–64.7] | 115 (56.4%) | [49.5–63.0] | ||
| Fever | Positive | 46 (26.4%) | [20.3–33.3] | 183 (31.9%) | [28.2–35.8] | 97 (47.5%) | [40.8–54.4] | <0.001 |
| n.r. | 128 (73.6%) | [66.7–79.7] | 391 (68.1%) | [64.2–71.8] | 107 (52.5%) | [45.6–59.2] | ||
| Other symptoms | Positive | 38 (21.8%) | [16.2–28.4] | 149 (26%) | [22.5–29.7] | 62 (30.4%) | [24.4–36.9] | 0.166 |
| n.r. | 136 (78.2%) | [71.6–83.8] | 425 (74%) | [70.3–77.5] | 142 (69.6%) | [63.1–75.6] | ||
| Severe feeling of sickness | Positive | 25 (14.4%) | [9.8–20.2] | 140 (24.4%) | [21.0–28.0] | 69 (33.8%) | [27.6–40.5] | <0.001 |
| n.r. | 149 (85.6%) | [79.8–90.2] | 434 (75.6%) | [72.0–79.0] | 135 (66.2%) | [59.5–72.4] | ||
| Freeze | Positive | 41 (23.6%) | [17.7–30.3] | 135 (23.5%) | [20.2–27.1] | 61 (29.9%) | [23.9–36.4] | 0.175 |
| n.r. | 133 (76.4%) | [69.7–82.3] | 439 (76.5%) | [72.9–79.8] | 143 (70.1%) | [63.6–76.1] | ||
| Chills or sweating | Positive | 39 (22.4%) | [16.7–29] | 118 (20.6%) | [17.4–24] | 50 (24.5%) | [19–30.7] | 0.487 |
| n.r. | 135 (77.6%) | [71.0–83.3] | 456 (79.4%) | [76.0–82.6] | 154 (75.5%) | [69.3–81.0] | ||
| Loss of taste | Positive | 22 (12.6%) | [8.3–18.2] | 97 (16.9%) | [14.0–20.1] | 42 (20.6%) | [15.5–26.5] | 0.121 |
| n.r. | 152 (87.4%) | [81.8–91.7] | 477 (83.1%) | [79.9–86] | 162 (79.4%) | [73.5–84.5] | ||
| Loss of smell | Positive | 16 (9.2%) | [5.6–14.2] | 74 (12.9%) | [10.3–15.8] | 39 (19.1%) | [14.2–24.9] | 0.015 |
| n.r. | 158 (90.8%) | [85.8–94.4] | 500 (87.1%) | [84.2–89.7] | 165 (80.9%) | [75.1–85.8] | ||
| Diarrhea | Positive | 18 (10.3%) | [6.5–15.5] | 70 (12.2%) | [9.7–15.1] | 26 (12.7%) | [8.7–17.8] | 0.748 |
| n.r. | 156 (89.7%) | [84.5–93.5] | 504 (87.8%) | [84.9–90.3] | 178 (87.3%) | [82.2–91.3] | ||
| Breathing difficulties/dyspnea | Positive | 17 (9.8%) | [6.0–14.8] | 66 (11.5%) | [9.1–14.3] | 18 (8.8%) | [5.5–13.3] | 0.524 |
| n.r. | 157 (90.2%) | [85.2–94] | 508 (88.5%) | [85.7–90.9] | 186 (91.2%) | [86.7–94.5] | ||
| Nausea | Positive | 18 (10.3%) | [6.5–15.5] | 58 (10.1%) | [7.8–12.8] | 27 (13.2%) | [9.1–18.4] | 0.454 |
| n.r. | 156 (89.7%) | [84.5–93.5] | 516 (89.9%) | [87.2–92.2] | 177 (86.8%) | [81.6–90.9] | ||
| Increased heartrate/tachycardia | Positive | 8 (4.6%) | [2.2–8.5] | 43 (7.5%) | [5.5–9.9] | 11 (5.4%) | [2.9–9.1] | 0.306 |
| n.r. | 166 (95.4%) | [91.5–97.8] | 531 (92.5%) | [90.1–94.5] | 193 (94.6%) | [90.9–97.1] | ||
| Rapid breathing/tachypnea | Positive | 3 (1.7%) | [0.5–4.5] | 26 (4.5%) | [3.1–6.5] | 10 (4.9%) | [2.5–8.5] | 0.212 |
| n.r. | 171 (98.3%) | [95.5–99.5] | 548 (95.5%) | [93.5–96.9] | 194 (95.1%) | [91.5–97.5] | ||
| Pneumonia | Positive | 0 (0%) | [0–0] | 5 (0.9%) | [0.3–1.9] | 0 (0%) | [0–0] | 0.191 |
| n.r. | 174 (100%) | [0–0] | 569 (99.1%) | [98.1–99.7] | 204 (100%) | [0–0] | ||
| Acute respiratory distress syndrome | Positive | 0 (0%) | [0–0] | 2 (0.3%) | [0.1–1.1] | 0 (0%) | [0–0] | 0.517 |
| n.r. | 174 (100%) | [0–0] | 572 (99.7%) | [98.9–99.9] | 204 (100%) | [0–0] | ||
| Respiratory insufficiency/assisted ventilation | Positive | 0 (0%) | [0–0] | 1 (0.2%) | [0–0.8] | 0 (0%) | [0–0] | 0.719 |
| n.r. | 174 (100%) | [0–0] | 573 (99.8%) | [99.2–100] | 204 (100%) | [0–0] | ||
| Oxygen saturation < 94% | Positive | 0 | [–] | 0 | [–] | 0 | [–] | - |
| n.r. | 174 (100%) | [0–0] | 574 (100%) | [0–0] | 204 (100%) | [0–0] | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goller, K.V.; Ziemann, J.; Kohler, C.; Becker, K.; Hübner, N.-O.; on behalf of the CoMV-Gen Study Group. Clinical Manifestations of Infections with the Omicron Sub-Lineages BA.1, BA.2, and BA.5: A Retrospective Follow-Up Analysis of Public Health Data from Mecklenburg-Western Pomerania, Germany. Viruses 2024, 16, 454. https://doi.org/10.3390/v16030454
Goller KV, Ziemann J, Kohler C, Becker K, Hübner N-O, on behalf of the CoMV-Gen Study Group. Clinical Manifestations of Infections with the Omicron Sub-Lineages BA.1, BA.2, and BA.5: A Retrospective Follow-Up Analysis of Public Health Data from Mecklenburg-Western Pomerania, Germany. Viruses. 2024; 16(3):454. https://doi.org/10.3390/v16030454
Chicago/Turabian StyleGoller, Katja Verena, Janine Ziemann, Christian Kohler, Karsten Becker, Nils-Olaf Hübner, and on behalf of the CoMV-Gen Study Group. 2024. "Clinical Manifestations of Infections with the Omicron Sub-Lineages BA.1, BA.2, and BA.5: A Retrospective Follow-Up Analysis of Public Health Data from Mecklenburg-Western Pomerania, Germany" Viruses 16, no. 3: 454. https://doi.org/10.3390/v16030454
APA StyleGoller, K. V., Ziemann, J., Kohler, C., Becker, K., Hübner, N.-O., & on behalf of the CoMV-Gen Study Group. (2024). Clinical Manifestations of Infections with the Omicron Sub-Lineages BA.1, BA.2, and BA.5: A Retrospective Follow-Up Analysis of Public Health Data from Mecklenburg-Western Pomerania, Germany. Viruses, 16(3), 454. https://doi.org/10.3390/v16030454