
Collaborative Referral Model for Hepatitis C Screening and Treatment in a Remote Mountainous Region of Taiwan during the COVID-19 Pandemic

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Collaboration of a Multidisciplinary Team
2.2.1. Anti-HCV Testing at LDPHC
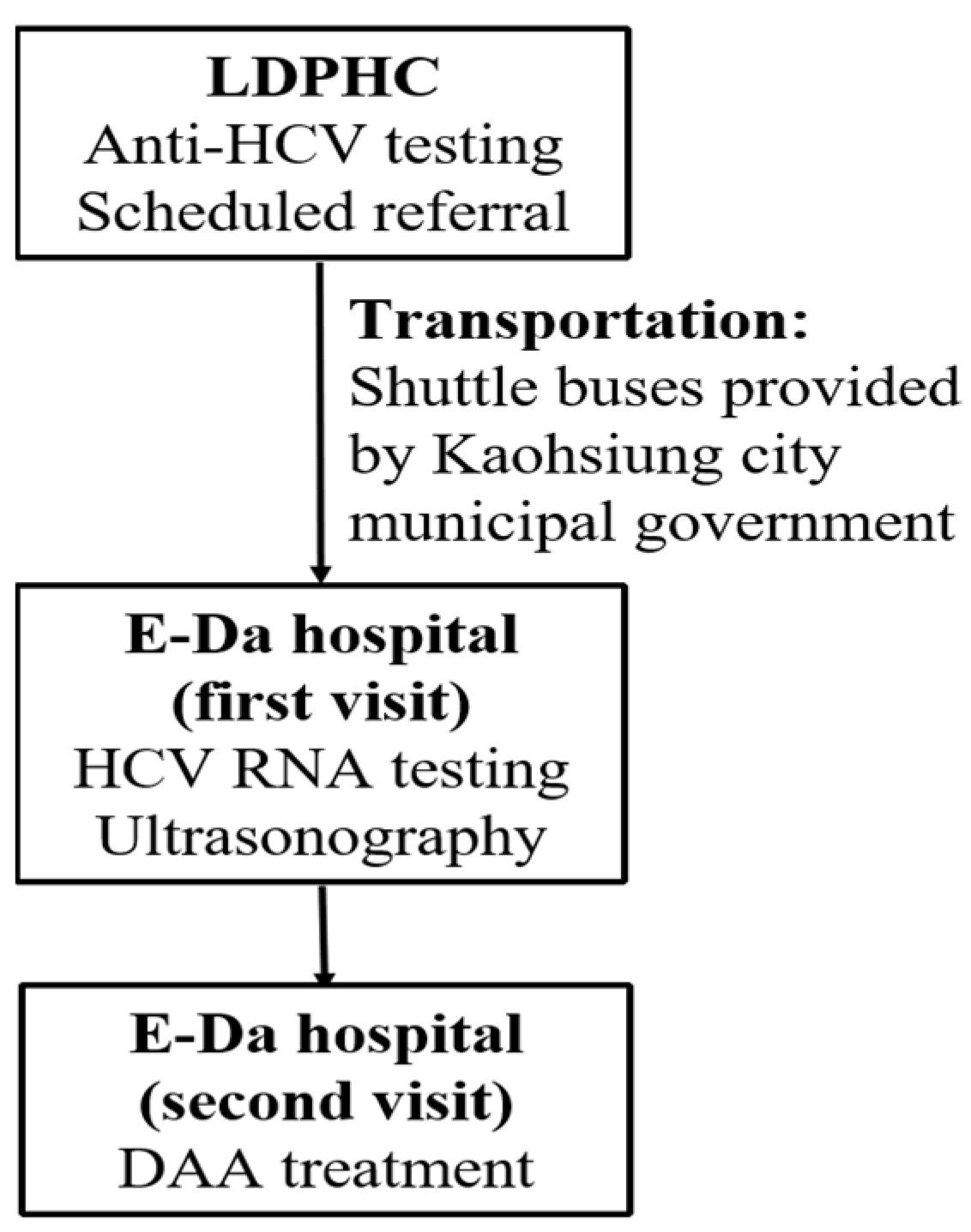
2.2.2. Referral to E-Da Hospital
2.2.3. DAA Treatment and Pre-Treatment Evaluation in E-Da Hospital
2.3. Assessment of Treatment Responses
2.4. Statistical Analysis
3. Results
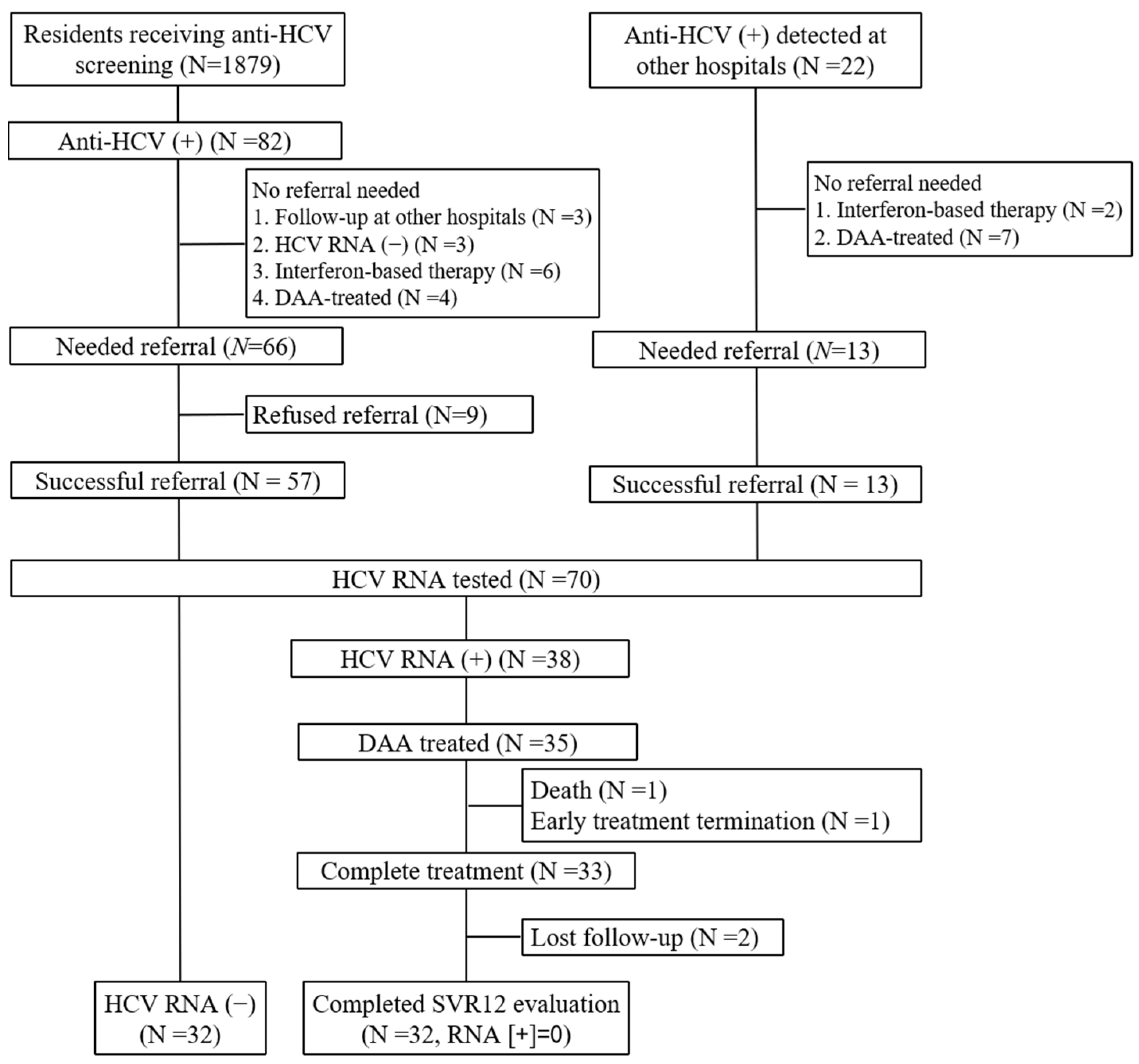
3.1. Screening Coverage Rate and Referral Rate
3.2. Characteristics of the Anti-HCV-Seropositive Subjects with Successful Referral
3.3. Treatment Outcomes of 35 Patients Receiving DAA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, M.H.; Yang, H.I.; Lu, S.N.; Jen, C.-L.; You, S.-L.; Wang, L.-Y.; Wang, C.-H.; Chen, W.J.; Chen, C.-J.; Reveal-HCV Study Group. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: A community-based long-term prospective study. J. Infect. Dis. 2012, 206, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory HCV Collaborators. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef]
- Falade-Nwulia, O.; Suarez-Cuervo, C.; Nelson, D.R.; Fried, M.W.; Segal, J.B.; Sulkowski, M.S. Oral Direct-Acting Agent Therapy for Hepatitis C Virus Infection: A Systematic Review. Ann. Intern. Med. 2017, 166, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: A modelling study. Lancet Gastroenterol. Hepatol. 2022, 7, 396–415. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Bennett, H.; Waser, N.; Johnston, K.; Kao, J.-H.; Lim, Y.-S.; Duan, Z.-P.; Lee, Y.-J.; Wei, L.; Chen, C.-J.; Sievert, W.; et al. A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol. Int. 2011, 9, 378–390. [Google Scholar] [CrossRef]
- Wu, G.H.; Pwu, R.F.; Chen, S.C.; Chen, D.S. Taiwan is on track of accelerating hepatitis C elimination by 2025. Liver Int. 2020, 40, 1506–1507. [Google Scholar] [CrossRef]
- Yu, M.L.; Yeh, M.L.; Tsai, P.C.; Huang, C.I.; Huang, J.F.; Huang, C.F.; Hsieh, M.H.; Liang, P.C.; Lin, Y.H.; Hsieh, M.Y.; et al. Huge gap between clinical efficacy and community effectiveness in the treatment of chronic hepatitis C: A nationwide survey in Taiwan. Medicine 2015, 94, e690. [Google Scholar] [CrossRef]
- Tai, C.M.; Huang, C.K.; Changchien, T.C.; Lin, P.-C.; Wang, D.-W.; Chang, T.-T.; Chan, H.-W.; Chen, T.-H.; Tseng, C.-H.; Chen, C.-C.; et al. Collaborative Referral Model to Achieve Hepatitis C Micro-Elimination in Methadone Maintenance Treatment Patients during the COVID-19 Pandemic. Viruses 2022, 14, 1637. [Google Scholar] [CrossRef]
- Yu, M.L.; Huang, C.F.; Wei, Y.J.; Lin, W.-Y.; Lin, Y.-H.; Hsu, P.-Y.; Hsu, C.-T.; Liu, T.W.; Lee, J.-J.; Niu, S.-W.; et al. Establishment of an outreach, grouping healthcare system to achieve microelimination of HCV for uremic patients in haemodialysis centres (ERASE-C). Gut 2021, 70, 2349–2358. [Google Scholar] [CrossRef]
- Kee, K.M.; Chen, W.M.; Hsu, N.T.; Wang, J.-H.; Chao, W.-H.; Lin, Y.-C.; Lu, S.-N. Community-based screening by Anti-HCV reflex HCV Ag test and accessible post-screening care toward elimination of hepatitis C in two hyperendemic townships. J. Formos. Med. Assoc. 2022, 121, 1850–1856. [Google Scholar] [CrossRef]
- Tien, H.M.; Cheng, T.C.; Lien, H.C.; Yang, K.-F.; Shy, C.-G.; Chen, Y.-L.; Hsu, N.-T.; Lu, S.-N.; Wang, J.-H. Liver Disease Screening and Hepatitis C Virus Elimination in Taiwan Rural Indigenous Townships: Village-By-Village Screening and Linking to Outreach Hepatology Care. Int. J. Environ. Res. Public Health 2022, 19, 3269. [Google Scholar] [CrossRef]
- Tsai, P.C.; Huang, C.I.; Yeh, M.L.; Huang, C.-F.; Hsieh, M.-H.; Yang, J.-F.; Hsu, P.-Y.; Liang, P.-C.; Lin, Y.-H.; Jang, T.Y.; et al. Significant amelioration of hepatitis C virus infection in a hyperendemic area: Longitudinal evidence from the COMPACT Study in Taiwan. BMJ Open 2021, 11, e042861. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.H.; Pwu, R.F.; Chen, S.C. Achieving hepatitis C elimination in Taiwan-Overcoming barriers by setting feasible strategies. J. Formos. Med. Assoc. 2018, 117, 1044–1045. [Google Scholar] [CrossRef] [PubMed]
- Shakeri, A.; Konstantelos, N.; Chu, C.; Antoniou, T.; Feld, J.; Suda, K.J.; Tadrous, M. Global Utilization Trends of Direct Acting Antivirals (DAAs) during the COVID-19 Pandemic: A Time Series Analysis. Viruses 2021, 13, 1314. [Google Scholar] [CrossRef] [PubMed]
- Easterbrook, P.J.; WHO Guidelines Development Group. Who to test and how to test for chronic hepatitis C infection—2016 WHO testing guidance for low- and middle-income countries. J. Hepatol. 2016, 65 (Suppl. S1), S46–S66. [Google Scholar] [CrossRef]
- Lombardi, A.; Mondelli, M.U.; ESCMID Study Group for Viral Hepatitis (ESGVH). Hepatitis C: Is eradication possible? Liver Int. 2019, 39, 416–426. [Google Scholar] [CrossRef]
- Oru, E.; Trickey, A.; Shirali, R.; Kanters, S.; Easterbrook, P. Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: A global systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e431–e445. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Fitzpatrick, T.; Walsh, N.; Kim, J.Y.; Chou, R.; Lackey, M.; Scott, J.; Lo, Y.-R.; Tucker, J.D. Interventions to optimise the care continuum for chronic viral hepatitis: A systematic review and meta-analyses. Lancet Infect. Dis. 2016, 16, 1409–1422. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Lee, M.H.; Yang, H.I.; Lu, S.N.; Jen, C.-L.; Yeh, S.-H.; Liu, C.-J.; Chen, P.-J.; You, S.-L.; Wang, L.-Y.; Chen, W.J.; et al. Hepatitis C virus seromarkers and subsequent risk of hepatocellular carcinoma: Long-term predictors from a community-based cohort study. J. Clin. Oncol. 2010, 28, 4587–4593. [Google Scholar]
- Chiu, H.M.; Jen, G.H.; Wang, Y.W.; Fann, J.C.-Y.; Hsu, C.-Y.; Jeng, Y.-C.; Yen, A.M.-F.; Chiu, S.Y.-H.; Chen, S.L.-S.; Hsu, W.-F.; et al. Long-term effectiveness of faecal immunochemical test screening for proximal and distal colorectal cancers. Gut 2021, 70, 2321–2329. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1. Integration of a team to strengthen collaboration between LDPHC and E-Da hospital. A team was established comprising LDPHC staff, hepatologists, and case managers from E-Da hospital. A consensus meeting was held before HCV screening and referral began. Online meetings were held as needed to overcome barriers. |
| 2. Provision of HCV screening as part of integrated services at LDPHC. LDPHC staff educated residents who visited LDPHC for medical needs about the importance of HCV treatment and encouraged the residents to receive HCV screening, even when residents initially came to LDPHC for the COVID-19 vaccine. 3. A shuttle bus and scheduled referrals to increase referral acceptance. Direct transportation to E-Da hospital and appointment with a physician who was familiar with this model increased the convenience of referral, which improved patients’ accessibility. 4. A simplified process to reduce outpatient waiting time. A simplified process was built to reduce waiting time to see a doctor and to receive ultrasonography, which is especially important to those unfamiliar with the processes in a tertiary referral center. 5. Routine referral model. This model was developed through its integration into the daily practice of two medical institutions without increasing the workload. Therefore, it is a routine referral model that can work sustainably without interruption. |
| Characteristics | Patients with Detectable HCV RNA | Patients without Detectable HCV RNA | p Value |
|---|---|---|---|
| (n = 38) | (n = 32) | ||
| Age, years | 64.8 ± 8.1 | 64.0 ± 12.0 | 0.754 |
| Male sex | 20 (52.6) | 11 (34.4) | 0.126 |
| HBV co-infection | 3 (7.9) | 4 (12.5) | 0.695 |
| Liver cirrhosis * | 2 (5.3) | 1 (3.1) | 1.0 |
| Hepatocellular carcinoma | 4 (10.5) | 0 (0) | 0.122 |
| AST, IU/L | 70.6 ± 87.4 | 25.8 ± 11.2 | 0.005 |
| ALT, IU/L | 69.0 ± 79.8 | 24.0 ± 10.7 | 0.003 |
| White cell count ×103/μL | 6.1 ± 2.4 | 7.2 ± 2.4 | 0.066 |
| Hemoglobin, g/dL | 13.8 ± 2.0 | 13.3 ± 1.9 | 0.315 |
| Platelet count, ×103/μL | 208.3 ± 68.1 | 256.2 ± 91.0 | 0.016 |
| Albumin, g/dL | 4.2 ± 0.4 | 4.3 ± 0.4 | 0.179 |
| Total bilirubin, mg/dL | 0.7 ± 0.3 | 0.6 ± 0.4 | 0.291 |
| Baseline HCVRNA, log IU | 5.9 ± 1.0 | - | - |
| HCV genotype, | - | - | |
| 1/2/3/6 | 15 (39.5)/15 (39.5)/ 1 (2.6)/6 (15.8) | - | - |
| 1 + 2 | 1 (2.6) | - | - |
| n/N (%) | |
|---|---|
| DAA regimens | |
| GLE/PIB | 28/35 (80.0) |
| SOF/VEL | 7/35 (20.0) |
| Complete treatment | 33/35 (94.3) |
| EOTVR | 33/35 (94.3) |
| SVR12 (ITT) | 32/35 (91.4) |
| SVR12 (PP) | 32/32 (100) |
| Explanation for non-SVR12 | n = 3 |
| Virological failure | 0 |
| Non-virological failure | |
| Death during treatment | 1 |
| Lost to follow-up | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, C.-M.; Bair, M.-J.; Chen, T.-H.; Tseng, C.-H.; Chen, C.-C.; Lam, H.; Yu, M.-L. Collaborative Referral Model for Hepatitis C Screening and Treatment in a Remote Mountainous Region of Taiwan during the COVID-19 Pandemic. Viruses 2023, 15, 827. https://doi.org/10.3390/v15040827
Tai C-M, Bair M-J, Chen T-H, Tseng C-H, Chen C-C, Lam H, Yu M-L. Collaborative Referral Model for Hepatitis C Screening and Treatment in a Remote Mountainous Region of Taiwan during the COVID-19 Pandemic. Viruses. 2023; 15(4):827. https://doi.org/10.3390/v15040827
Chicago/Turabian StyleTai, Chi-Ming, Ming-Jong Bair, Tzu-Haw Chen, Cheng-Hao Tseng, Chih-Cheng Chen, Hung Lam, and Ming-Lung Yu. 2023. "Collaborative Referral Model for Hepatitis C Screening and Treatment in a Remote Mountainous Region of Taiwan during the COVID-19 Pandemic" Viruses 15, no. 4: 827. https://doi.org/10.3390/v15040827
APA StyleTai, C.-M., Bair, M.-J., Chen, T.-H., Tseng, C.-H., Chen, C.-C., Lam, H., & Yu, M.-L. (2023). Collaborative Referral Model for Hepatitis C Screening and Treatment in a Remote Mountainous Region of Taiwan during the COVID-19 Pandemic. Viruses, 15(4), 827. https://doi.org/10.3390/v15040827