

Association between Pulmonary Aspergillosis and Cytomegalovirus Reactivation in Critically Ill COVID-19 Patients: A Prospective Observational Cohort Study

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Treatment Protocol
2.2. Data Collection
2.3. CAPA Definition
2.4. CMV Blood Reactivation Definition
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, G.D.; Denning, D.W.; Gow, N.A.R.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden killers: Human fungal infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [PubMed]
- Schauwvlieghe, A.F.; Rijnders, B.J.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19-associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [PubMed]
- Dimopoulos, G.; Almyroudi, M.-P.; Myrianthefs, P.; Rello, J. COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Intensive Med. 2021, 1, 71–80. [Google Scholar]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect Dis. 2020, 71, 1367–1376. [Google Scholar] [PubMed]
- Mikulska, M.; Raiola, A.M.; Bruno, B.; Furfaro, E.; Van Lint, M.T.; Bregante, S.; Ibatici, A.; Del Bono, V.; Bacigalupo, A.; Viscoli, C. Risk factors for invasive aspergillosis and related mortality in recipients of allogeneic SCT from alternative donors: An analysis of 306 patients. Bone Marrow Transpl. 2009, 44, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Rijnders, B.J.; Brüggemann, R.J.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar]
- Calderón-Parra, J.; Moreno-Torres, V.; Mills-Sanchez, P.; Tejado-Bravo, S.; Romero-Sánchez, I.; Balandin-Moreno, B.; Calvo-Salvador, M.; Portero-Azorín, F.; García-Masedo, S.; Muñez-Rubio, E.; et al. Association of COVID-19-Associated Pulmonary Aspergillosis with Cytomegalovirus Replication: A Case-Control Study. J. Fungi 2022, 8, 161. [Google Scholar]
- Ranieri, V.I.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- COVID-19 Clinical Management: Living Guidance n.d. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 14 June 2021).
- Mussini, C.; Falcone, M.; Nozza, S.; Sagnelli, C.; Parrella, R.; Meschiari, M.; Petrosillo, N.; Mastroianni, C.; Cascio, A.; Iaria, C.; et al. Therapeutic strategies for severe COVID-19: A position paper from the Italian Society of Infectious and Tropical Diseases (SIMIT). Clin. Microbiol. Infect. 2021, 27, 389–395. [Google Scholar]
- Steinberg, K.P.; Hudson, L.D.; Goodman, R.B.; Hough, C.L.; Lanken, P.N.; Hyzy, R.; Thompson, B.T.; Ancukiewicz, M.; National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Efficacy and Safety of Corticosteroids for Persistent Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2006, 354, 1671–1684. [Google Scholar]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. National Strategy to Diagnose Coronavirus Disease 2019-Associated Invasive Fungal Disease in the Intensive Care Unit. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e1634–e1644. [Google Scholar]
- Van Biesen, S.; Kwa, D.; Bosman, R.J.; Juffermans, N.P. Detection of invasive pulmonary aspergillosis in COVID-19 with Nondirected BAL. Am. J. Respir. Crit. Care Med. 2020, 208, 1171–1173. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of invasive pulmonary aspergillosis among COVID-19 intubated patients: A prospective study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, E3606–E3614. [Google Scholar]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef]
- Manian, F.A. IDSA Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Bloodstream Infection. Clin. Infect. Dis. 2009, 49, 1770–1771. [Google Scholar] [CrossRef]
- Lachance, P.; Chen, J.; Featherstone, R.; Sligl, W.I. Association Between Cytomegalovirus Reactivation and Clinical Outcomes in Immunocompetent Critically Ill Patients: A Systematic Review and Meta-Analysis. Open Forum Infect Dis. 2017, 13, ofx029. [Google Scholar] [CrossRef]
- Limaye, A.P.; Stapleton, R.D.; Peng, L.; Gunn, S.R.; Kimball, L.E.; Hyzy, R.; Exline, M.C.; Files, D.C.; Morris, P.E.; Frankel, S.K.; et al. Effect of Ganciclovir on IL-6 Levels Among Cytomegalovirus-Seropositive Adults with Critical Illness: A Randomized Clinical Trial. JAMA 2017, 318, 731–740. [Google Scholar] [CrossRef]
- Le Balc’h, P.; Pinceaux, K.; Pronier, C.; Seguin, P.; Tadié, J.M.; Reizine, F. Herpes simplex virus and cytomegalovirus reactivations among severe COVID-19 patients. Crit Care 2020, 24, 530. [Google Scholar] [CrossRef]
- Moniz, P.; Brito, S.; Póvoa, P. SARS-CoV-2 and cytomegalovirus coinfections—A case series of critically ill patients. J. Clin. Med. 2021, 10, 2792. [Google Scholar] [CrossRef]
- Simonnet, A.; Engelmann, I.; Moreau, A.S.; Garcia, B.; Six, S.; El Kalioubie, A.; Robriquet, L.; Hober, D.; Jourdain, M. High incidence of Epstein-Barr virus, cytomegalovirus, and human-herpes virus-6 reactivations in critically ill patients with COVID-19. Infect. Dis. Now 2021, 51, 296–299. [Google Scholar] [CrossRef]
- Chuleerarux, N.; Thongkam, A.; Manothummetha, K.; Nematollahi, S.; Dioverti-Prono, V.; Torvorapanit, P.; Langsiri, N.; Worasilchai, N.; Plongla, R.; Chindamporn, A.; et al. Does post-transplant cytomegalovirus increase the risk of invasive aspergillosis in solid organ transplant recipients? A systematic review and meta-analysis. J. Fungi 2021, 7, 327. [Google Scholar] [CrossRef]
- Kuo, C.W.; Wang, S.Y.; Tsai, H.P.; Su, P.L.; Cia, C.T.; Lai, C.H.; Chen, C.W.; Shieh, C.C.; Lin, S.H. Invasive pulmonary aspergillosis is associated with cytomegalovirus viremia in critically ill patients—A retrospective cohort study. J. Microbiol. Immunol. Infect. 2022, 55, 291–299. [Google Scholar] [CrossRef]
- Gatto, I.; Biagioni, E.; Coloretti, I.; Farinelli, C.; Avoni, C.; Caciagli, V.; Busani, S.; Sarti, M.; Pecorari, M.; Gennari, W.; et al. Modena COVID-19 Working Group. Cytomegalovirus blood reactivation in COVID-19 critically ill patients: Risk factors and impact on mortality. Intensive Care Med. 2022, 48, 706–713. [Google Scholar]
- Moore, J.L.; Stroever, S.J.; Rondain, P.E.; Scatena, R.N. Incidence of Secondary Bacterial Infections Following Utilization of Tocilizumab for the Treatment of COVID-19—A Matched Retrospective Cohort Study. J. Glob. Infect Dis. 2021, 3, 67–71. [Google Scholar] [CrossRef]
- Karakike, E.; Dalekos, G.N.; Koutsodimitropoulos, I.; Saridaki, M.; Pourzitaki, C.; Papathanakos, G.; Kotsaki, A.; Chalvatzis, S.; Dimakopoulou, V.; Vechlidis, N.; et al. ESCAPE: An Open-Label Trial of Personalized Immunotherapy in Critically lll COVID-19 Patients. J. Innate Immun. 2022, 4, 218–228. [Google Scholar] [CrossRef]

{kind=link}
| Baseline | All Population (n = 579) | No CAPA (n = 483) | CAPA (n = 96) | p-Value |
|---|---|---|---|---|
| Sex (male; n, %) | 419 (72.4%) | 348 (72) | 71 (74) | 0.702 |
| Age (median, IQR) | 65 (56–72) | 63 (55–72) | 70 (63–75) | <0.001 |
| BMI (median, IQR) | 29 (26–33) | 29 (26–33) | 29 (26–33) | 0.761 |
| Comorbidities (n,%) | 445 (76.9) | 360 (74.5) | 85 (88.5) | 0.003 |
| Diabetes | 123 (21.3) | 97 (20.2) | 26 (27.1) | 0.131 |
| Chronic cardiac disease (n, %) | 95 (16.5) | 67 (13.9) | 28 (29.2) | <0.001 |
| Chronic respiratory disease (n, %) | 62 (10.7) | 53 (11.0) | 9 (9.4) | 0.635 |
| Chronic renal disease (n, %) | 21 (3.6) | 16 (3.3) | 5 (5.2) | 0.369 |
| Pre-existing immunosuppression (n, %) | 92 (15.9) | 66 (13.6) | 26 (27.1) | 0.001 |
| Hematologic malignancies (n, %) | 29 (5.0) | 20 (4.1) | 9 (9.4) | 0.033 |
| Cancer (n, %) | 19 (3.3) | 11 (2.3) | 8 (8.3) | 0.002 |
| SAPSII score (median, IQR) | 34 (28–39) | 33 (28–38) | 36 (33–43) | <0.001 |
| D-dimer (mcg/L; median, IQR) | 1470 (820–3020) | 1510 (820–2850) | 1325 (780–3660) | 0.992 |
| LDH (U/L; median, IQR) | 823 (634–1104) | 815 (635–1096) | 916 (624–1239) | 0.341 |
| Leukocyte count (cells/mcl; median, IQR) | 8.3 (5.9–11.2) | 8.2 (5.9–10.9) | 8.5 (5.5–11.7) | 0.829 |
| Lymphocyte count (cells/mcl; median, IQR) | 0.7 (0.5–1.0) | 0.7 (0.5–1.0) | 0.6 (0.4–0.9) | 0.008 |
| Platelet count (1000/mm3; median, IQR) | 219 (170–288) | 222 (171–288) | 205 (155–269) | 0.182 |
| CRP (mg/L; median, IQR) | 6.3 (2.2–17.1) | 6.6 (2.6–17.4) | 5.6 (1.2–16.1) | 0.069 |
| PCT (ng/mL; median, IQR) | 0.2 (0.1–0.5) | 0.2 (0.1–0.5) | 0.2 (0.1–0.6) | 0.772 |
| PaO2/FiO2 (mmHg; median, IQR) | 102 (82–135) | 102 (81–136) | 103 (91–135) | 0.347 |
| IL-6 (pg/mL; median, IQR) | 276.6 (93.3–834) | 259.5 (80.0–770.3) | 295.3 (114.9–1177.6) | 0.170 |
| Steroid (n, %) | 533 (92.2) | 441 (91.3) | 92 (96.8) | 0.066 |
| Tocilizumab administration (n, %) | 477 (82.4) | 398 (82.4) | 79 (82.3) | 0.979 |
| SDD (n, %) | 83 (14.3) | 60 (12.4) | 23 (24.0) | 0.003 |
| Invasive mechanical ventilation (n, %) | 347 (59.9) | 263 (54.5) | 84 (87.5) | <0.001 |
| Waves | ||||
| 1st wave 25 February–6 July 2020 | 102 | 88 (86.3) | 14 (13.7) | |
| 2nd wave 20 September 2020–13 February 2021 | 166 | 142 (85.5) | 24 (14.5) | |
| 3rd wave 14 February–30 April 2021 | 172 | 136 (79.1) | 36 (20.9) | |
| 4th wave 30 April 2021–8 May 2022 | 139 | 117 (84.2) | 22 (15.8) | |
| Variable | Total (n = 96) | No CMV Reactivation (n = 56) | CMV Reactivation (n = 40) | p-Value |
|---|---|---|---|---|
| Sex (male; n, %) | 71 (74) | 39 (69.9) | 32 (80.0) | 0.254 |
| Age (median, QR) | 70 (63–75) | 70 (63–75) | 71 (63–76) | 0.663 |
| Comorbidities (n, %) | 85 (88.5) | 48 (85.7) | 37 (92.5) | 0.303 |
| Diabetes | 26 (27.1) | 15 (26.8) | 11 (27.5) | 0.938 |
| Chronic cardiac disease (n, %) | 28 (29.2) | 19 (33.9) | 9 (22.5) | 0.225 |
| Chronic respiratory disease (n, %) | 9 (9.4) | 4 (7.1) | 5 (12.5) | 0.375 |
| Chronic renal disease (n, %) | 5 (5.2) | 3 (5.4) | 2 (5.0) | 0.938 |
| Pre-existing immunosuppression (n, %) | 26 (27.1) | 10 (17.9) | 16 (40.0) | 0.016 |
| Hematologic malignancies (n, %) | 9 (9.4) | 5 (8.9) | 4 (10.0) | 0.895 |
| Cancer (n, %) | 8 (8.3) | 3 (5.4) | 5 (12.5) | 0.212 |
| SOFA (median, IQR) | 4 (3–6) | 4 (3–6) | 5 (4–6) | 0.158 |
| SAPSII score (median, IQR) | 36 (33–43) | 36 (33–42) | 37 (32–44) | 0.519 |
| D-dimer (mcg/L; median, IQR) | 1325 (780–3660) | 1360 (760–3355) | 1305 (800–4866) | 0.994 |
| LDH (U/L; median, IQR) | 916 (624–1239) | 991 (697–1264) | 788 (532–1104) | 0.065 |
| Leukocyte count (cells/mcl; median, IQR) | 8.5 (5.5–11.7) | 8.7 (5.6–11.6) | 8.3 (5.4–15.8) | 0.749 |
| Lymphocyte count (cells/mcl; median, IQR) | 0.6 (0.4–0.9) | 0.6 (0.4–0.8) | 0.6 (0.4–0.9) | 0.624 |
| Platelet count (1000/mm3; median, IQR) | 205 (155–269) | 219 (155–289) | 198 (153–255) | 0.205 |
| CRP (mg/L; median, IQR) | 5.6 (1.2–16.1) | 4.6 (1.4–16.9) | 6.0 (1.1–14.7) | 0.649 |
| PCT T0 (ng/mL; median, IQR) | 0.2 (0.1–0.6) | 0.2 (0.1–0.5) | 0.2 (0.1–0.6) | 0.777 |
| PaO2/FiO2 (mmHg; median, IQR) | 103 (91–135) | 107 (92–142) | 101 (91–129) | 0.483 |
| IL6 (pg/mL; median, IQR) | 295.3 (114.9–1177.6) | 385.6 (194.1–1491.0) | 165.2 (95.9–875.0) | 0.069 |
| BMI (median, IQR) | 29 (26–33) | 29 (26–33) | 29 (27–33) | 0.642 |
| Steroid (n, %) | 92 (96.8) | 52 (94.5) | 40 (100) | 0.133 |
| Tocilizumab administration (n, %) | 79 (82.3) | 47 (83.9) | 32 (80.0) | 0.619 |
| SDD (n, %) | 23 (24.0) | 14 (25.0) | 9 (22.5) | 0.777 |
| Invasive mechanical ventilation (n, %) | 84 (87.5) | 45 (80.4) | 39 (97.5) | 0.012 |
| Waves | ||||
| 1st wave 25 February–6 July 2020 | 14 (13.7) | 8 (14.3) | 6 (15.0) | 0.969 |
| 2nd wave 20 September 2020–13 February 2021 | 24 (14.5) | 14 (25.0) | 10 (25.0) | |
| 3rd wave 14 February–30 April 2021 | 36 (20.9) | 22 (39.3) | 14 (35.0) | |
| 4th wave 30 April 2021–8 May 2022 | 22 (15.8) | 12 (21.4) | 10 (25.0) | |
| OUTCOME | Total (n = 96) | No CMV Reactivation (n = 56) | CMV Reactivation (n = 40) | p-Value |
|---|---|---|---|---|
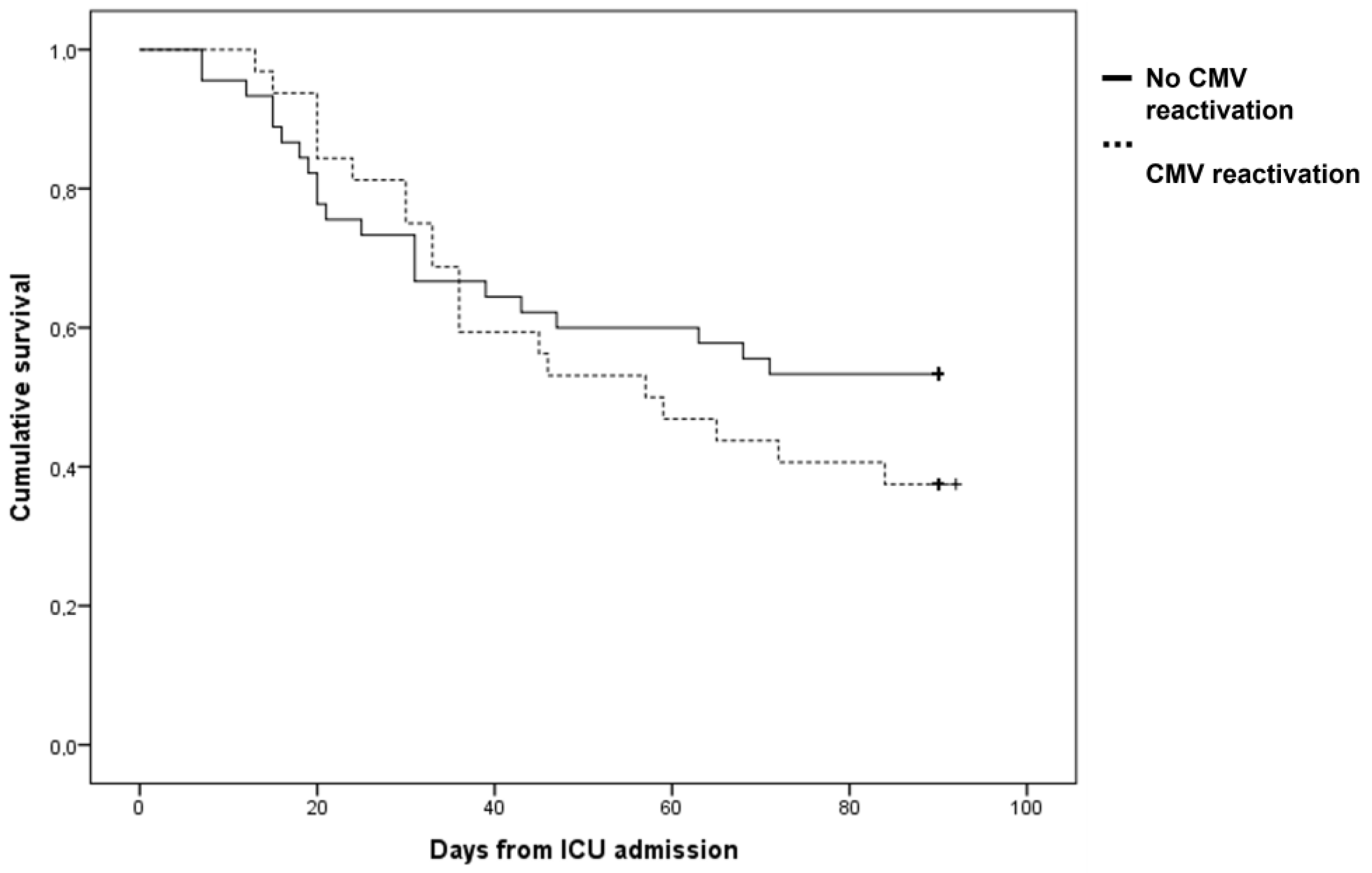
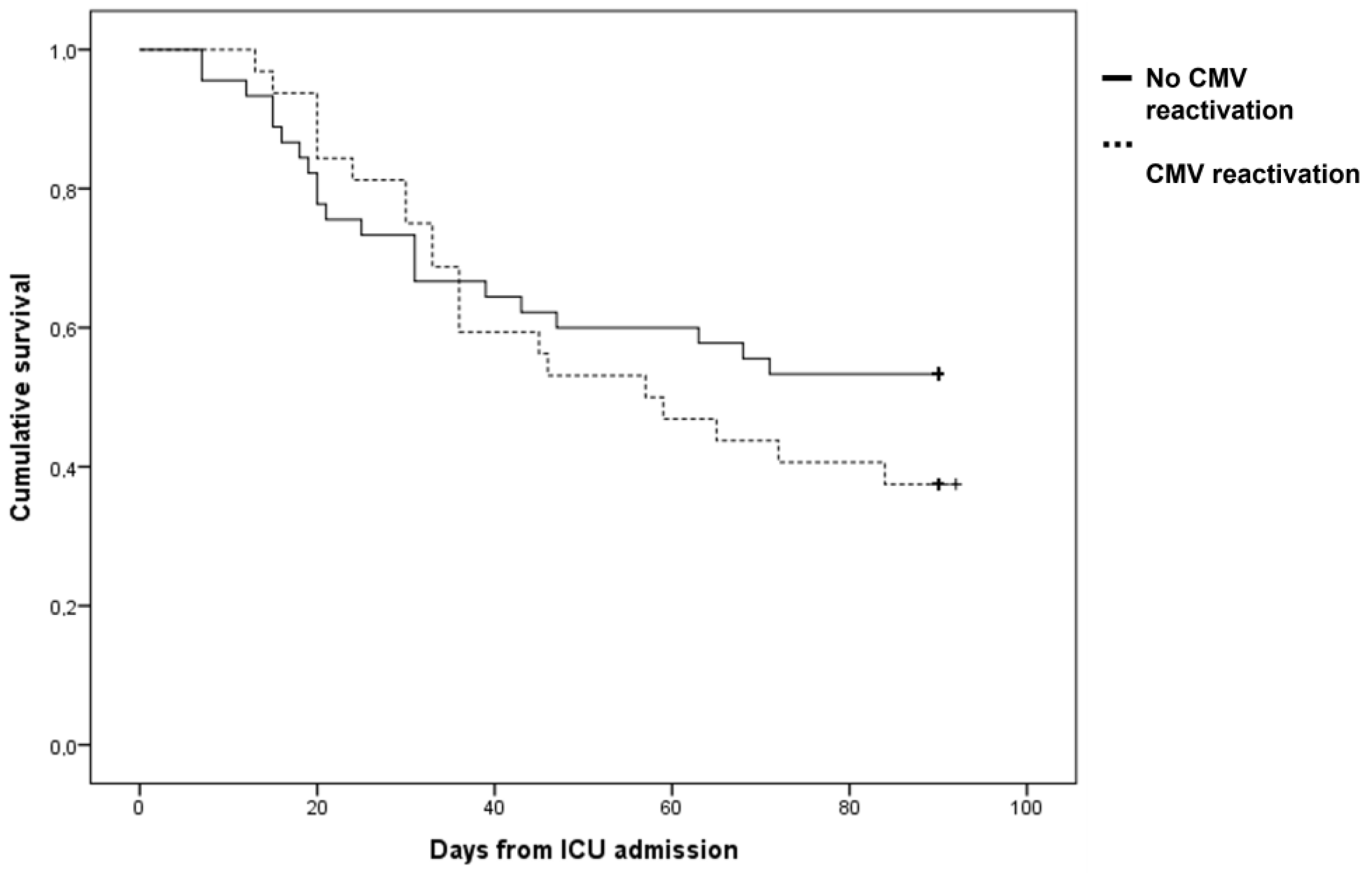
| 90-day mortality (n, %) | 52 (54.2%) | 27 (48.2) | 25 (62.5) | 0.166 |
| ICU mortality (n, %) | 48 (50%) | 24 (42.9) | 24 (60.0) | 0.098 |
| ICU length of stay (days; median, IQR) | 19 (8–39) | 12 (6–23) | 35 (20–59) | <0.001 |
| Invasive mechanical ventilation-free days at day 60 (days; median, IQR) | 9 (1–48) | 13 (1–56) | 7 (0–15) | 0.020 |
| Mechanical ventilation-free days at day 60 (days; median, IQR) | 0 (0–35) | 0 (0–53) | 0 (0–0) | 0.001 |
| Secondary bacterial infection (n, %) | 61 (63.5%) | 30 (53.6) | 31 (77.5) | 0.016 |
| Bacteremia (n, %) | 24 (25%) | 12 (21.4) | 12 (30) | 0.339 |
| Pneumonia (n, %) | 49 (51%) | 25 (44.6) | 24 (60) | 0.914 |
| Time to CAPA occurrence (days; median, IQR) | 5.5 (1.0–12.0) | 2 (1–7.5) | 9.5 (5–20.5) | <0.001 |
| Time to secondary bacterial infection (days; median, IQR) | 11 (6–17) | 10 (8–12) | 19 (6–29) | 0.667 |
| CMV Blood Reactivation at Day 90 (n = 40) | No CMV Blood Reactivation at Day 90 (n =56) | Unadjusted HR (95% CI); | p-Value | Adjusted HR (95% CI); | p-Value | |
|---|---|---|---|---|---|---|
| Invasive mechanical ventilation (n, %) | 39 (97.5) | 45 (80.4) | 7.02 (0.96–51.14) | 0.094 | 6.00 (0.74–48.75) | 0.094 |
| Secondary bacterial infection (n, %) | 31 (77.55) | 30 (53.6) | 2.20 (1.04–4.62) | 0.038 | 1.32 (0.60–2.93) | 0.491 |
| Tocilizumab administration (n, %) | 32 (80.0) | 47 (83.9) | 0.74 (0.34–1.60) | 0.438 | 0.98 (0.44–2.16) | 0.951 |
| Previous immune-suppression (n, %) | 16 (40.0) | 10 (17.9) | 2.33 (1.24–4.40) | 0.009 | 2.33 (1.21–4.48) | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caciagli, V.; Coloretti, I.; Talamonti, M.; Farinelli, C.; Gatto, I.; Biagioni, E.; Sarti, M.; Franceschini, E.; Meschiari, M.; Mussini, C.; et al. Association between Pulmonary Aspergillosis and Cytomegalovirus Reactivation in Critically Ill COVID-19 Patients: A Prospective Observational Cohort Study. Viruses 2023, 15, 2260. https://doi.org/10.3390/v15112260
Caciagli V, Coloretti I, Talamonti M, Farinelli C, Gatto I, Biagioni E, Sarti M, Franceschini E, Meschiari M, Mussini C, et al. Association between Pulmonary Aspergillosis and Cytomegalovirus Reactivation in Critically Ill COVID-19 Patients: A Prospective Observational Cohort Study. Viruses. 2023; 15(11):2260. https://doi.org/10.3390/v15112260
Chicago/Turabian StyleCaciagli, Valeria, Irene Coloretti, Marta Talamonti, Carlotta Farinelli, Ilenia Gatto, Emanuela Biagioni, Mario Sarti, Erica Franceschini, Marianna Meschiari, Cristina Mussini, and et al. 2023. "Association between Pulmonary Aspergillosis and Cytomegalovirus Reactivation in Critically Ill COVID-19 Patients: A Prospective Observational Cohort Study" Viruses 15, no. 11: 2260. https://doi.org/10.3390/v15112260
APA StyleCaciagli, V., Coloretti, I., Talamonti, M., Farinelli, C., Gatto, I., Biagioni, E., Sarti, M., Franceschini, E., Meschiari, M., Mussini, C., Tonelli, R., Clini, E., Girardis, M., Busani, S., & Modena COVID-19 Working Group. (2023). Association between Pulmonary Aspergillosis and Cytomegalovirus Reactivation in Critically Ill COVID-19 Patients: A Prospective Observational Cohort Study. Viruses, 15(11), 2260. https://doi.org/10.3390/v15112260