
Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection?


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
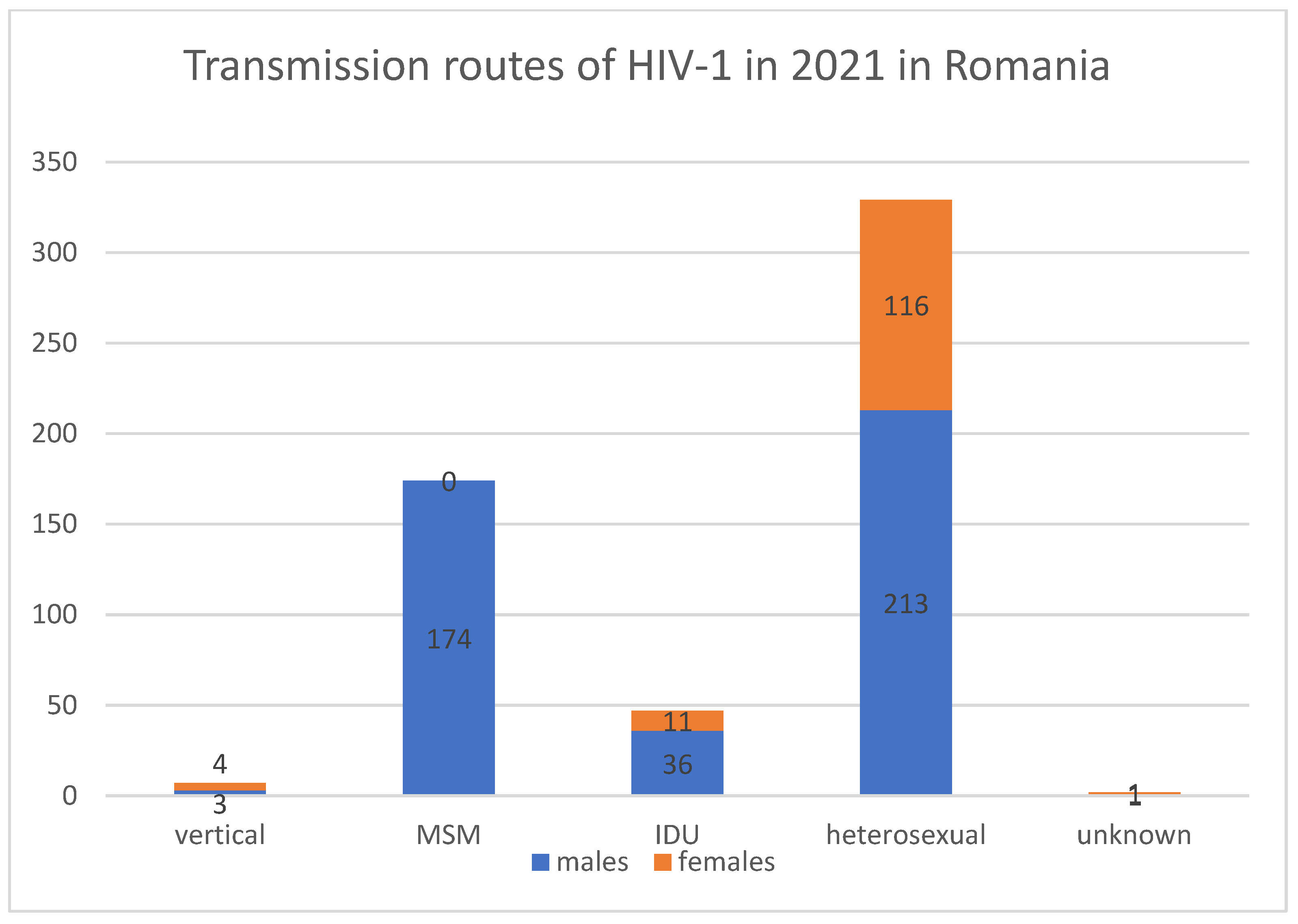
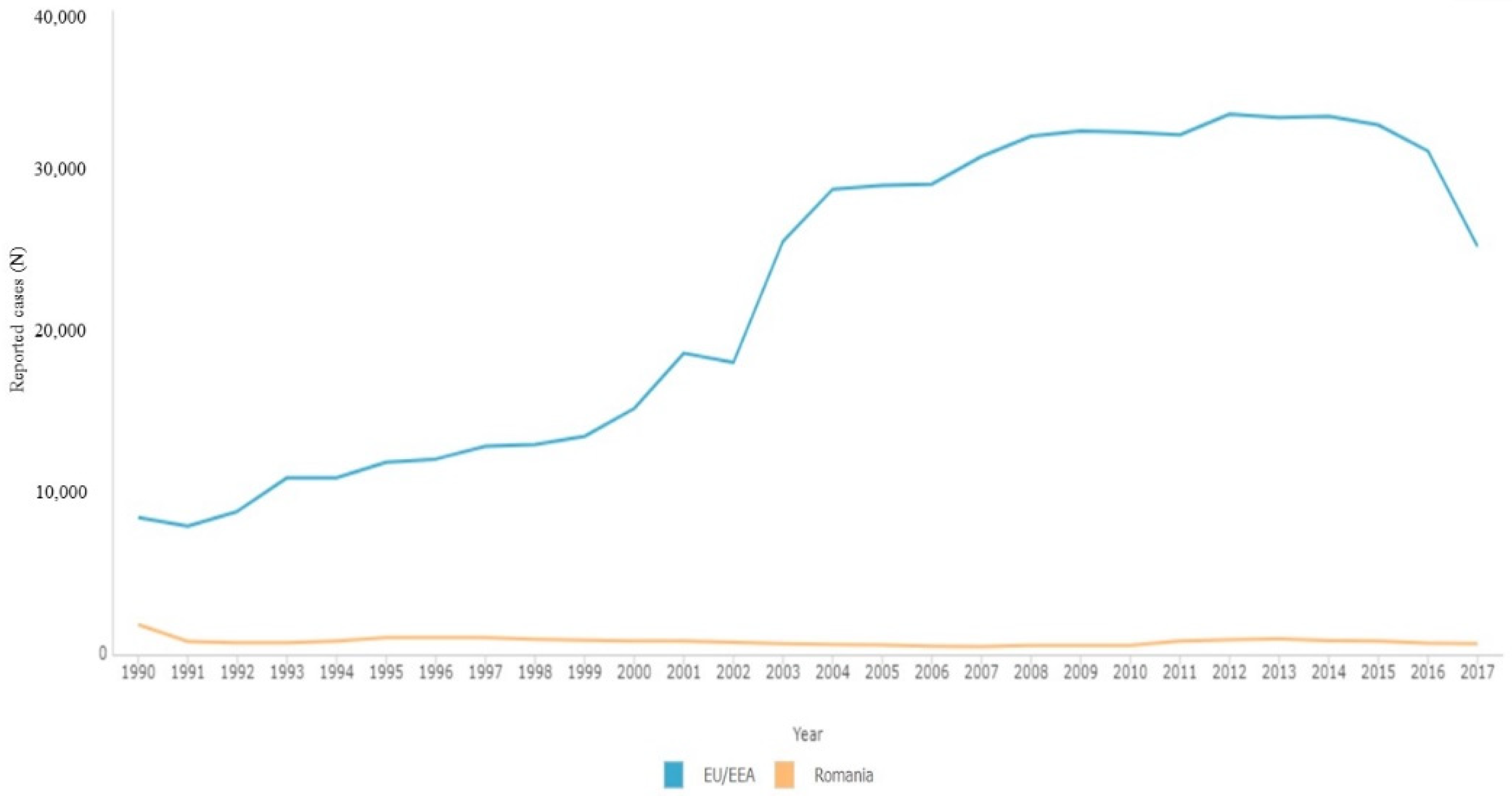
2. HIV-1 Epidemiology in Romania
3. Subtypes of HIV-1
4. Particularities of HIV-1 Subtype F
4.1. Origin of HIV-1 and Spread of HIV-1 F1
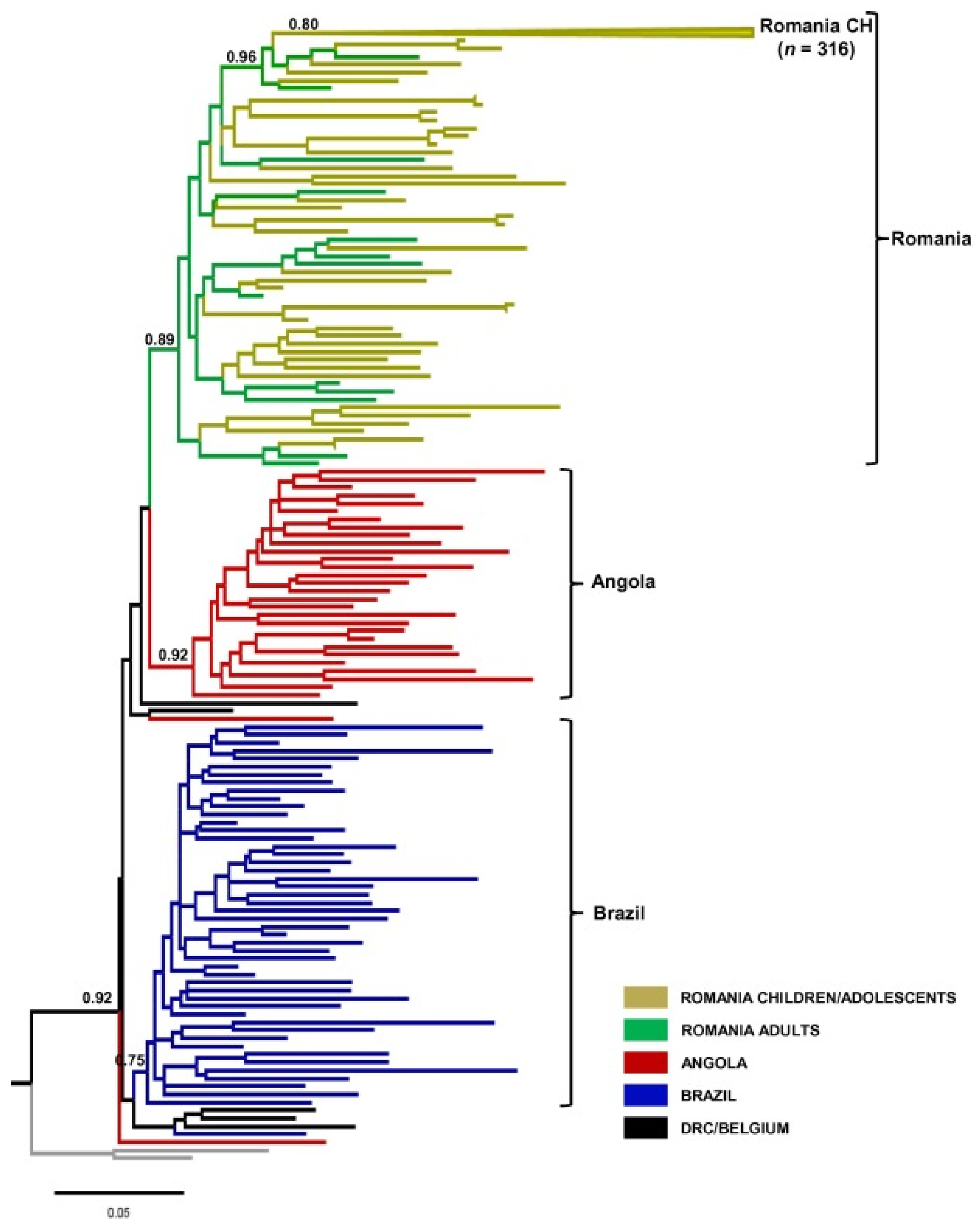
4.2. HIV-1 F1 in Romania and Global Context
5. Evolution of HIV-1 in Romania
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jianu, C.; Bolboacă, S.D.; Topan, A.V.; Filipescu, I.; Jianu, M.E.; Itu-Mureşan, C.A. View of Human Immunodeficiency Virus Infections in the North-West Region of Romania. Medicina 2019, 55, 765. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, O.; Kalis, M.L.; Kliks, S.C.; Bandea, C.I.; Levy, J.A. Characterization of Human Immunodeficiency Virus Type 1 Isolates from Children in Romania: Identification of a New Envelope Subtype. J. Infect. Dis. 1994, 69, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Leires Marques, B.C.; Gonçalves Morgado, M.; Lindenmeyer Guimarães, M. Potential overestimation of HIV-1 sub-subtype F1 circulation in Rio de Janeiro, Brazil. Mem. Inst. Oswaldo Cruz 2018, 113, e170483. [Google Scholar] [CrossRef] [PubMed]
- Bello, G.; Morais Afonso, J.; Morgado, M.G. Phylodynamics of HIV-1 subtype F1 in Angola, Brazil and Romania. Infect. Genet. Evol. 2012, 12, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Manolescu, L.S.; Temereanca, A.; Ruţă, S. HIV-1 circulating subtypes in Romania. Roum. Arch. Microbiol. Immunol. 2013, 72, 121–134. [Google Scholar] [PubMed]
- Lai, A.; Ciccozzi, M.; Franzetti, M.; Simonetti, F.R.; Bozzi, G.; Binda, F.; Rosi, A.; Bonora, S.; De Luca, A.; Balotta, C.; et al. Local and global spatio-temporal dynamics of HIV-1 subtype F1. J. Med. Virol. 2014, 86, 186–192. [Google Scholar] [CrossRef]
- Beloukas, A.; Psarris, A.; Giannelou, P.; Kostaki, E.; Hatzakis, A.; Paraskevis, D. Molecular epidemiology of HIV-1 infection in Europe: An overview. Infect. Genet. Evol. 2016, 46, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Paraschiv, S.; Otelea, D.; Baicus, C.; Tinischi, M.; Costache, M.; Neaga, E. Nucleoside reverse transcriptase inhibitor resistance mutations in subtype F1 strains isolated from heavily treated adolescents in Romania. Int. J. Infect. Dis. 2009, 13, 81–89. [Google Scholar] [CrossRef][Green Version]
- Paraschiv, S.; Otelea, D.; Batan, I.; Baicus, C.; Magiorkinis, G.; Paraskevis, D. Molecular typing of the recently expanding subtype B HIV-1 epidemic in Romania: Evidence for local spread among MSMs in Bucharest area. Infect. Genet. Evol. 2012, 12, 1052–1057. [Google Scholar] [CrossRef]
- HIV/SIDA Romanian Monitoring and Evaluation Compartment; Matei Bals Infectious Diseases National Institute. HIV Evolution in Romania. 30 June 2022. Available online: https://www.cnlas.ro/images/doc/31122021.pdf (accessed on 27 July 2022).
- German Advisory Committee Blood (Arbeitskreis Blut), Subgroup ‘Assessment of Pathogens Transmissible by Blood’. Human Immunodeficiency Virus (HIV). Transfus. Med. Hemother. 2016, 43, 203–222. [Google Scholar] [CrossRef]
- Taylor, B.S.; Sobieszczyk, M.E.; McCutchan, F.E.; Hammer, S.M. The challenge of HIV-1 subtype diversity. N. Engl. J. Med. 2008, 358, 1590–1602, Erratum in: N. Engl. J. Med. 2008, 359, 1965–1966. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Elangovan, R.; Yun, J.; Dickson-Tetteh, L.; Fleminger, I.; Kirtley, S.; Williams, B.; Gouws-Williams, E.; Ghys, P.D. WHO–UNAIDS Network for HIV Isolation Characterisation. Global and regional molecular epidemiology of HIV-1, 1990–2015: A systematic review, global survey, and trend analysis. Lancet Infect. Dis. 2019, 19, 143–155, Erratum in: Lancet Infect. Dis. 2020, 20, e27. [Google Scholar] [CrossRef]
- Désiré, N.; Cerutti, L.; Le Hingrat, Q.; Perrier, M.; Emler, S.; Calvez, V.; Descamps, D.; Marcellin, A.-G.; Hué, S.; Viseaux, B. Characterization update of HIV-1 M subtypes diversity and proposal for subtypes A and D sub-subtypes reclassification. Retrovirology 2018, 15, 80. [Google Scholar] [CrossRef] [PubMed]
- Bobkova, M. Current status of HIV-1 diversity and drug resistance monitoring in the former USSR. AIDS Rev. 2013, 15, 204–212. [Google Scholar] [PubMed]
- Lebedev, A.; Lebedeva, N.; Moskaleychik, F.; Pronin, A.; Kazennova, E.; Bobkova, M. Human Immunodeficiency Virus-1 Diversity in the Moscow Region, Russia: Phylodynamics of the Most Common Subtypes. Front. Microbiol. 2019, 10, 320. [Google Scholar] [CrossRef] [PubMed]
- Abidi, S.H.; Aibekova, L.; Davlidova, S.; Amangeldiyeva, A.; Foley, B.; Ali, S. Origin and evolution of HIV-1 subtype A6. PLoS ONE 2021, 16, e0260604. [Google Scholar] [CrossRef]
- Rudometova, N.B.; Shcherbakova, N.S.; Shcherbakov, D.N.; Taranov, O.S.; Zaitsev, B.N.; Karpenko, L.I. Construction and Characterization of HIV-1 env-Pseudoviruses of the Recombinant Form CRF63_02A and Subtype A6. Bull. Exp. Biol. Med. 2022, 172, 729–733. [Google Scholar] [CrossRef]
- Kazennova, E.; Laga, V.; Lapovok, I.; Glushchenko, N.; Neshumaev, D.; Vasilyev, A.; Bobkova, M. HIV-1 genetic variants in the Russian Far East. AIDS Res. Hum. Retrovir. 2014, 30, 742–752. [Google Scholar] [CrossRef]
- Crispim, M.A.E.; Reis, M.N.D.G.; Abrahim, C.; Kiesslich, D.; Fraiji, N.; Bello, G.; Stefani, M.M.A. Homogenous HIV-1 subtype B from the Brazilian Amazon with infrequent diverse BF1 recombinants, subtypes F1 and C among blood donors. PLoS ONE 2019, 14, e0221151. [Google Scholar] [CrossRef]
- Paraschiv, S.; Foley, B.; Otelea, D. Diversity of HIV-1 subtype C strains isolated in Romania. Infect. Genet. Evol. 2011, 11, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Rubio, A.E.; Abraha, A.; Carpenter, C.A.; Troyer, R.M.; Reyes-Rodríguez, Á.L.; Salomon, H.; Arts, E.J.; Tebit, D.M. Similar replicative fitness is shared by the subtype B and unique BF recombinant HIV-1 isolates that dominate the epidemic in Argentina. PLoS ONE 2014, 9, e92084. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, M.L.; Vicente, A.C.; Otsuki, K.; da Silva, R.F.; Francisco, M.; da Silva, F.G.; Serrano, D.; Morgado, M.G.; Bello, G. Close phylogenetic relationship between Angolan and Romanian HIV-1 subtype F1 isolates. Retrovirology 2009, 6, 39. [Google Scholar] [CrossRef]
- Mbisa, J.L.; Hué, S.; Buckton, A.J.; Myers, R.E.; Duiculescu, D.; Ene, L.; Oprea, C.; Tardei, G.; Rugina, S.; Mardarescu, M.; et al. Phylodynamic and phylogeographic patterns of the HIV type 1 subtype F1 parenteral epidemic in Romania. AIDS Res. Hum. Retrovir. 2012, 28, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Atlas of Infectious Diseases. ECDC. Available online: https://atlas.ecdc.europa.eu/public/index.aspx (accessed on 27 July 2022).
- Dilernia, D.A.; Jones, L.R.; Pando, M.A.; Rabinovich, R.D.; Damilano, G.D.; Turk, G.; Rubio, A.E.; Pampuro, S.; Gomez-Carrillo, M.; Salomón, H. Analysis of HIV type 1 BF recombinant sequences from South America dates the origin of CRF12_BF to a recombination event in the 1970s. AIDS Res. Hum. Retrovir. 2011, 27, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Vinken, L.; Fransen, K.; Cuypers, L.; Alexiev, I.; Balotta, C.; Debaisieux, L.; Seguin-Devaux, C.; Ribas, S.G.; Gomes, P.; Incardona, F.; et al. Earlier Initiation of Antiretroviral Treatment Coincides With an Initial Control of the HIV-1 Sub-Subtype F1 Outbreak Among Men-Having-Sex-With-Men in Flanders, Belgium. Front. Microbiol. 2019, 10, 613. [Google Scholar] [CrossRef]
- Paraschiv, S.; Otelea, D.; Dinu, D.; Maxim, D.; Tinischi, T. Polymorphisms and resistance mutations in the protease and reverse transcriptase genes of HIV-1 F subtype Romanian strains. Int. J. Infect. Dis. 2007, 11, 123–128. [Google Scholar] [CrossRef][Green Version]
- Niculescu, I.; Paraschiv, S.; Paraskevis, D.; Abagiu, A.; Batan, I.; Banica, L.; Otelea, D. Recent HIV-1 Outbreak Among Intravenous Drug Users in Romania: Evidence for Cocirculation of CRF14_BG and Subtype F1 Strains. AIDS Res. Hum. Retrov. 2015, 31, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Temereanca, A.; Oprea, C.; Wertheim, J.O.; Ianache, I.; Ceausu, E.; Cernescu, C.; Mehta, S.R.; Ruta, S. HIV transmission clusters among injecting drug users in Romania. Rom. Biotechnol. lett. 2017, 22, 12307–12315. [Google Scholar]
- Temereanca, A.; Ene, L.; Mehta, S.; Manolescu, L.S.C.; Duiculescu, D.; Ruta, S. Transmitted HIV drug resistance in newly diagnosed, treatment-naive Romanian patients. J. Med. Virol. 2013, 85, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Manolescu, L.; Temereanca, A.; Diaconu, C.C.; Ruta, S. Correlation between resistance profile and immunosuppression in heavily treated HIV-1 infected Romanian patients. Rom. Biotechnol. Lett. 2011, 16, 6439–6449. [Google Scholar] [PubMed]
- Manolescu, L.; Marinescu, P. Sex differences in HIV-1 viral load and absolute CD4 cell count in long term survivors HIV-1 infected patients from Giurgiu, Romania. Rom. Rev. Lab. Med. 2013, 21, 217–224. [Google Scholar] [CrossRef][Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preda, M.; Manolescu, L.C.S. Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection? Viruses 2022, 14, 2081. https://doi.org/10.3390/v14092081
Preda M, Manolescu LCS. Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection? Viruses. 2022; 14(9):2081. https://doi.org/10.3390/v14092081
Chicago/Turabian StylePreda, Mădălina, and Loredana Cornelia Sabina Manolescu. 2022. "Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection?" Viruses 14, no. 9: 2081. https://doi.org/10.3390/v14092081
APA StylePreda, M., & Manolescu, L. C. S. (2022). Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection? Viruses, 14(9), 2081. https://doi.org/10.3390/v14092081