
The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing


 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Monkeypox
2. Human Infection
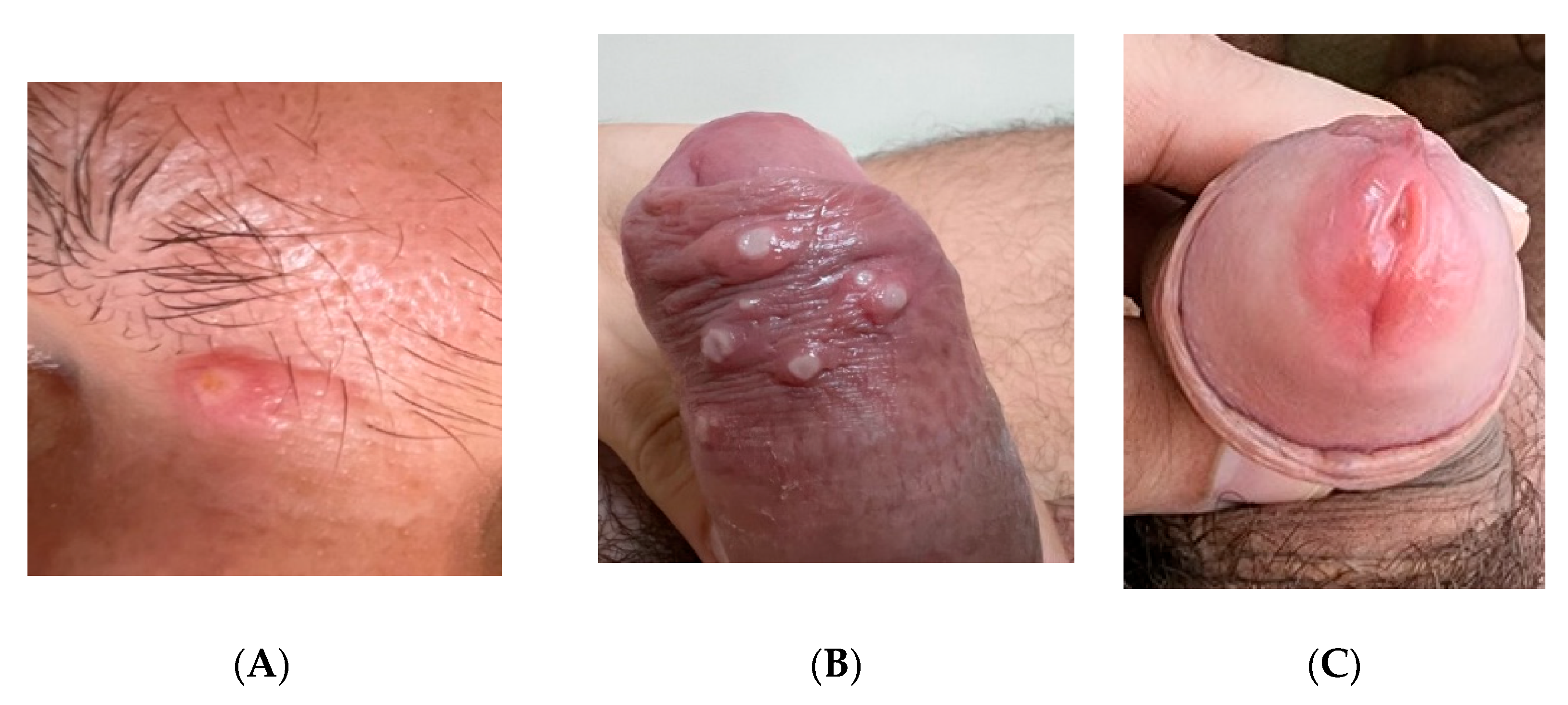
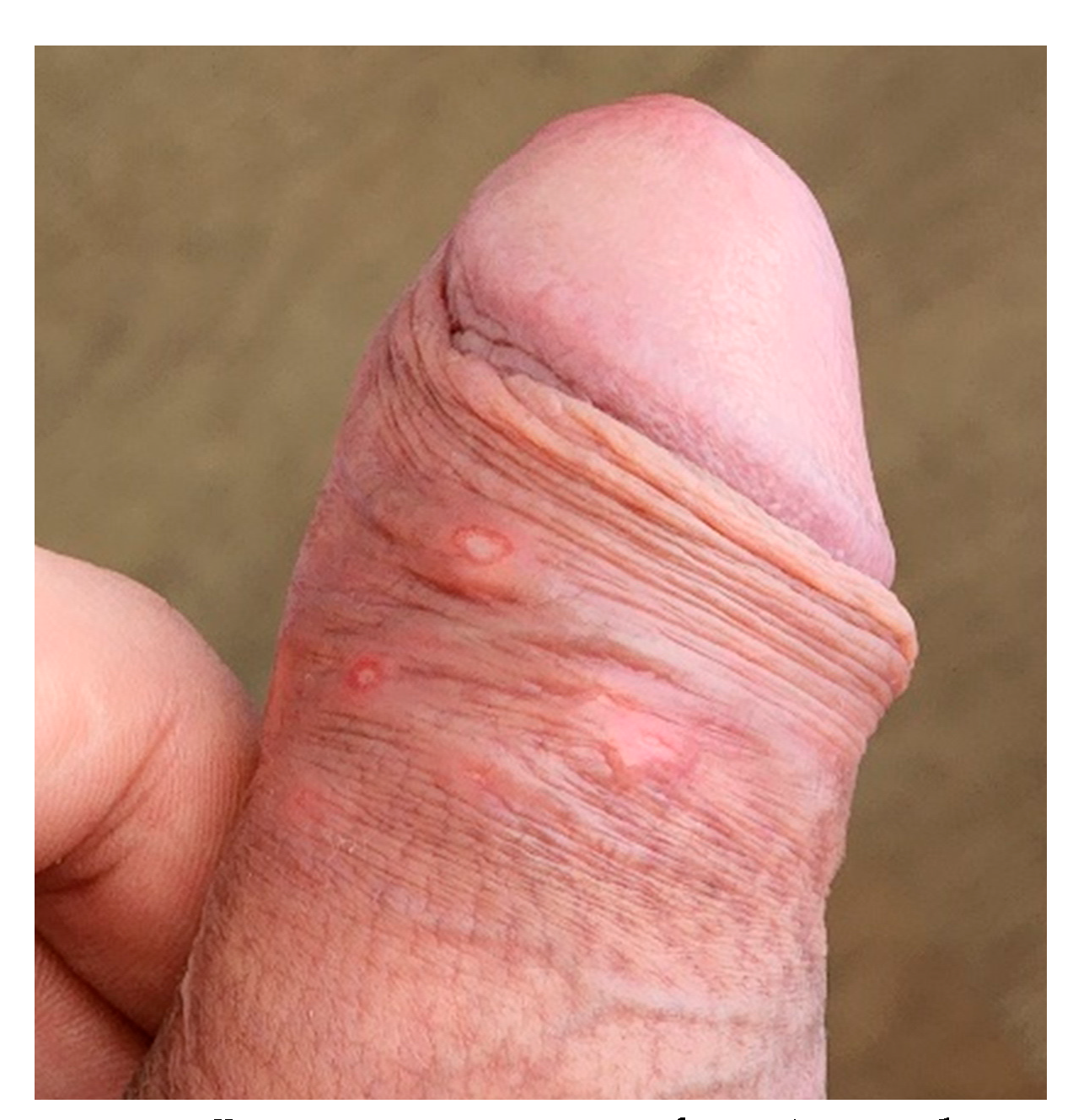
2.1. Case Report 1
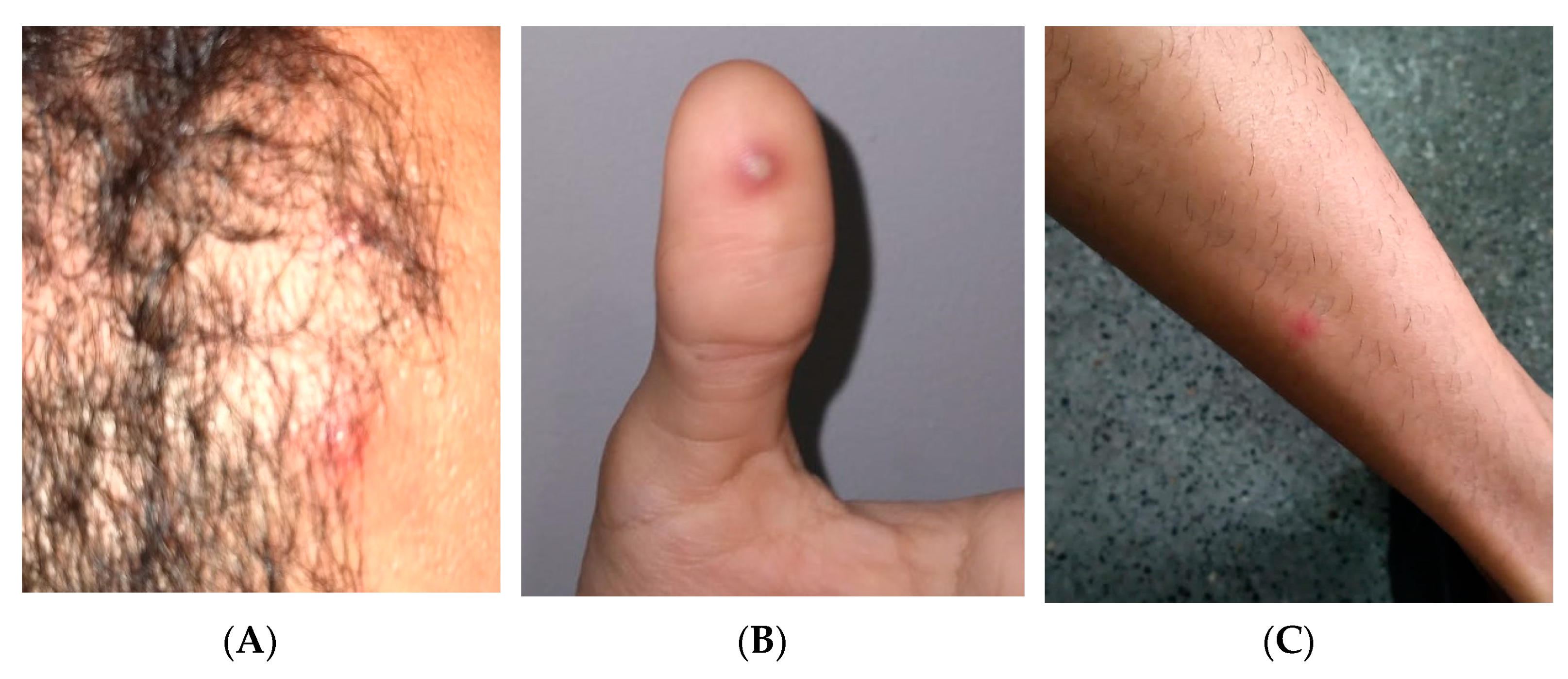
2.2. Case Report 2
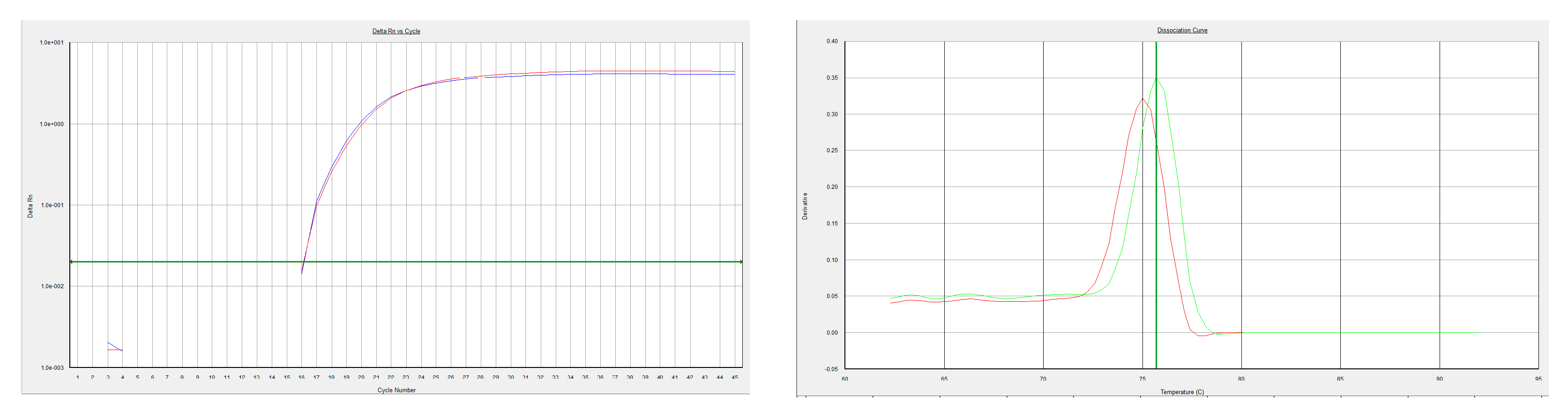
3. Laboratorial Diagnostic Procedures
4. Discussion and Literature Review
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magnus, P.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A pox-like disease in cynomolgus monkeys. Acta Path. Micro Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Chen, N.; Li, G.; Liszewski, M.K.; Atkinson, J.P.; Jahrling, P.B.; Feng, Z.; Schriewer, J.; Buck, C.; Wang, C.; Lefkowitz, E.J.; et al. Virulence differences between monkeypox virus isolates from West Africa and the Congo basin. Virology 2005, 340, 46–63. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.O.; Brink, E.W.; Hutchins, D.L.; Pifer, J.M.; Lourie, B.; Moser, C.R.; Cummings, E.C.; Kuteyi, O.E.; Eke, R.E.; Titus, J.B.; et al. Human monkeypox. Bull. World Health Organ. 1972, 46, 569–576. [Google Scholar] [PubMed]
- Jezek, Z.; Marennikova, S.S.; Jutumbo, M.; Nakano, J.H.; Paluku, K.M.; Szczeniowski, M. Human monkeypox: A study of 2510 contacts of 214 patients. J. Infect. Dis. 1986, 154, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.; Perrichot, M.; Stemmler, M.; Emmerich, P.; Schmitz, H.; Varaine, F.; Shungu, R.; Tshioko, F.; Formenty, P. Outbreaks of disease suspected of being due to human monkeypox virus infection in the Democratic Republic of Congo in 2001. J. Clin. Microbiol. 2002, 40, 2919–2921. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Multistate outbreak of monkeypox—Illinois, Indiana, and Wisconsin, 2003. MMWR Morb. Mortal Wkly. Rep. 2003, 52, 642–646. [Google Scholar]
- Li, Y.; Zhao, H.; Wilkins, K.; Hughes, C.; Damon, I.K. Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J. Virol. Methods 2010, 169, 223–227. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Disease Outbreak News; Multi-Country Monkeypox Outbreak in Non-Endemic Countries. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385 (accessed on 2 August 2022).
- Oprea, C.; Ianache, I.; Piscu, S.; Tardei, G.; Nica, M.; Ceausu, E.; Popescu, C.P.; Florescu, S.A. First report of monkeypox in a patient living with HIV from Romania. Travel Med. Infect. Dis. 2022, 49, 102395. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, D.; Patrocínio, J.; Frade, J.; Correia, C.; Borges-Costa, J.; Filipe, P. Human monkeypox coinfection with acute HIV: An exuberant presentation. Int. J. STD AIDS 2022. [Google Scholar] [CrossRef] [PubMed]
- Bížová, B.; Veselý, D.; Trojánek, M.; Rob, F. Coinfection of syphilis and monkeypox in HIV positive man in Prague, Czech Republic. Travel Med. Infect. Dis. 2022, 49, 102368. [Google Scholar] [CrossRef] [PubMed]
- Adalja, A.; Inglesby, T. A Novel International Monkeypox Outbreak. Ann. Intern. Med. 2022, 175, 1175–1176. [Google Scholar] [CrossRef] [PubMed]
- Daskalakis, D.; McClung, R.P.; Mena, L.; Mermin, J.; Centers for Disease Control and Prevention’s Monkeypox Response Team. Monkeypox: Avoiding the Mistakes of Past Infectious Disease Epidemics. Ann. Intern. Med. 2022, 175, 1177–1178. [Google Scholar] [CrossRef] [PubMed]
- Iñigo Martínez, J.; Gil Montalbán, E.; Jiménez Bueno, S.; Martín Martínez, F.; Nieto Juliá, A.; Sánchez Díaz, J.; García Marín, N.; Córdoba Deorador, E.; Nunziata Forte, A.; Alonso García, M.; et al. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Euro Surveill. 2022, 27, 2200471. [Google Scholar] [CrossRef] [PubMed]
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending Aftereffect of Smallpox Eradication? Front. Trop. Dis. 2022, 3, 951380. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brites, C.; Deminco, F.; Sá, M.S.; Brito, J.T.; Luz, E.; Stocker, A. The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing. Viruses 2022, 14, 1841. https://doi.org/10.3390/v14091841
Brites C, Deminco F, Sá MS, Brito JT, Luz E, Stocker A. The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing. Viruses. 2022; 14(9):1841. https://doi.org/10.3390/v14091841
Chicago/Turabian StyleBrites, Carlos, Felice Deminco, Marcia Sampaio Sá, Jean Tadeu Brito, Estela Luz, and Andreas Stocker. 2022. "The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing" Viruses 14, no. 9: 1841. https://doi.org/10.3390/v14091841
APA StyleBrites, C., Deminco, F., Sá, M. S., Brito, J. T., Luz, E., & Stocker, A. (2022). The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing. Viruses, 14(9), 1841. https://doi.org/10.3390/v14091841