
Inflammatory Markers after Switching to a Dual Drug Regimen in HIV-Infected Subjects: A Two-Year Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Markers of Immune Activation
2.3. Demographic Parameters and Background Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vella, S.; Schwartländer, B.; Sow, S.P.; Eholie, S.P.; Murphy, R.L. The history of antiretroviral therapy and of its implementation in resource-limited areas of the world. AIDS 2012, 26, 1231–1241. [Google Scholar] [CrossRef] [PubMed]
- European AIDS Clinical Society Guidelines 2017. Version 8.2. Available online: http://www.eacsociety.org/files/guidelines_8.2-english.pdf (accessed on 15 January 2022).
- World Health Organization. Recomendations for a public approach. In Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing of HIV Infection, 2nd ed.; WHO: Geneva, Switzerland, 2016. Available online: http://apps.who.int/iris/bitstream/10665/208825/1/9789241549684_eng.pdf (accessed on 20 January 2022).
- Cahn, P.; Rolòn, M.J.; Figueroa, M.I.; Gun, A.; Paerson, P.; Sued, O. Dolutegravir lamivudine as initial therapy in HIV-infected, ARV naive patients: 48 week results of the PADDLE study. J. Int. AIDS Soc. 2017, 20, 21678. [Google Scholar] [CrossRef] [PubMed]
- Cento, V.; Perno, F.C. Two-drug regimens with dolutegravir plus rilpivirine or lamivudine in HIV-1 treatment-naïve, virologically-suppressed patients: Latest evidence from the literature on their efficacy and safety. J. Glob. Antimicrob. Resist. 2020, 20, 228–237. [Google Scholar] [PubMed]
- Hernandez, B.; Kahl, L.; Matthews, J.; Vincent, T.; Angelis, K.; Koteff, J. Bone, Renal, and Inflammatory Biomarkers Up to Week 100 Post Switch to DTG+RPV: The SWORD-1 and SWORD-2 Studies. In Proceedings of the P8 HIV & Hepatitis Nordic Conference, Stockholm, Sweden, 26–28 September 2018. [Google Scholar]
- Llibre, J.M.; López-Cortes, L.F.; Aylott, A.; Wynne, B.; Matthews, J.; van Wyk, J. Inflammatory and atherogenesis markers 148 weeks postswitch to DTG+ROV in SWORD-1/-2. In Proceedings of the Virtual Conference on Retroviruses and Opportunistic Infections (CROI), Virtual. 6–10 March 2021. [Google Scholar]
- van Wyk, J.; Ajana, F.; Bisshop, F.; De Wit, S.; Osiyemi, O.; Sogorb, P.J.; Jean-Pierre, R.; Christoph, W.; Mounir, A.-K.; Maria, C.N.; et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Fixed-Dose Two-Drug Regimen Versus Continuing a Tenofovir Alafenamide-Based Three- or Four-Drug Regimen for Maintenance of Virologic Suppression in Adults With HIV-1: Phase 3, Randomized, Non-inf. Clin. Infect. Dis. 2020, 53, 1689–1699. [Google Scholar] [CrossRef] [Green Version]
- Serrano Villar, S.; Lopez-Huertas, M.R.; Jimenez, D.; Galera, C.; Martinez-Sanz, J.; Moreno, E.; Muriel, A.; Gutierrez, F.; Busca, C.; Portilla, J.; et al. A Retrospective Analysis of Long-Term Changes of Inflammatory Biomarkers in Individuals on Suppressive Three-Drug or Two-Drug Antiretroviral Regimens. Lancet 2021. pre-print. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3976877 (accessed on 14 March 2022). [CrossRef]
- Vassallo, M.; Durant, J.; Fabre, R.; Ticchioni, M.; Lotte, L.; Sindt, A.; Puchois, A.; de Monte, A.; Cezar, R.; Corbeau, P.; et al. Switching to a dual-drug regimen in HIV-infected patients could be associated with macrophage activation? Front. Med. 2021, 8, 712880. [Google Scholar] [CrossRef]
- Dyavar, S.R.; Gautam, N.; Podany, A.T.; Winchester, L.C.; Weinhold, J.A.; Mykris, T.M.; Campbell, K.M.; Alnouti, Y.; Fletcher, C.V. Assessing the lymphoid tissue bioavailability of antiretrovirals in human primary lymphoid endothelial cells and in mice. J. Antimicrob. Chemother. 2019, 74, 2974–2978. [Google Scholar] [CrossRef]
- Riddler, S.A.; Aga, E.; Bosch, R.J.; Bastow, B.; Bedison, M.; Vagratian, D.; Vaida, F.; Eron, J.J.; Gandhi, R.T.; Mellors, J.W.; et al. Continued Slow Decay of the Residual Plasma Viremia Level in HIV-1-Infected Adults Receiving Long-term Antiretroviral Therapy. J. Infect. Dis. 2016, 213, 556–560. [Google Scholar] [CrossRef] [Green Version]
- Ryscavage, P.; Kelly, S.; Li, J.Z.; Harrigan, P.R.; Taiwo, B. Significance and clinical management of persistent low-level viremia and very-low-level viremia in HIV-1-infected patients. Antimicrob. Agents Chemother. 2014, 58, 3585–3598. [Google Scholar] [CrossRef] [Green Version]
- Lambert-Niclot, S.; Flandre, P.; Valantin, M.A.; Peytavin, G.; Duvivier, C.; Haim-Boukobza, S.; Algarte-Genin, M.; Yazdanpanah, Y.; Girard, P.; Katlama, C.; et al. Factors associated with virological failure in HIV-1-infected patients receiving darunavir/ritonavir monotherapy. J. Infect. Dis. 2011, 204, 1211–1216. [Google Scholar]
- Serrano-Villar, S.; Pérez-Elías, M.J.; Dronda, F.; Casado, J.L.; Moreno, A.; Royuela, A.; Pérez-Molina, J.A.; Sainz, T.; Navas, E.; Hermida, J.M.; et al. Increased risk of serious non-AIDS-related events in HIV-infected subjects on antiretroviral therapy associated with a low CD4/CD8 ratio. PLoS ONE 2014, 9, e85798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidofsky, A.; Holmes, J.A.; Feeney, E.R.; Kruger, A.J.; Salloum, S.; Zheng, H.; Seguin, I.S.; Altinbas, A.; Masia, R.; Corey, K.E.; et al. Macrophage Activation Marker Soluble CD163 Is a Dynamic Marker of Liver Fibrogenesis in Human Immunodeficiency Virus/Hepatitis C Virus Coinfection. J. Infect. Dis. 2018, 218, 1394–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKibben, R.A.; Margolick, J.B.; Grinspoon, S.; Li, X.; Palella, F.J., Jr.; Kingsley, L.A.; Witt, M.D.; George, R.T.; Jacobson, L.P.; Budoff, M.; et al. Elevated levels of monocyte activation markers are associated with subclinical atherosclerosis in men with and those without HIV infection. J. Infect. Dis. 2015, 211, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.E.; Meeds, H.L.; Rouster, S.D.; Abdel-Hameed, E.A.; Hernandez, J.; Tamargo, J.; Chen, J.; Ehman, R.L.; Baum, M. Soluble CD163 Identifies Those at Risk for Increased Hepatic Inflammation & Fibrosis. Open Forum Infect. Dis. 2021, 8, ofab203. [Google Scholar] [PubMed]
- Deeks, S.G.; Tracy, R.; Douek, D.C. Systemic Effects of Inflammation on Health during Chronic HIV Infection. Immunity 2013, 39, 633–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assoumou, L.; Valentin, M.A.; Kolta, S.; Bastard, J.P.; Fellahi, S.; Molina, J.M.; Bouchaud, O.; Beniguel, L.; Weiss, L.; Reynes, J.; et al. Changes in lipid parameters, body fat, bone mineral density and inflammation/immune activation markers in middle-aged HIV-infected patients with viral suppression treated with etravirine/raltegravir—Results at week 48 of the ANRS163-ETRAL trial. Antivir. Ther. 2017, 22, A8. [Google Scholar]
- Bracq, L.; Xie, M.; Benichou, S.; Bouchet, J. Mechanisms for Cell-to-Cell Transmission of HIV-1. Front. Immunol. 2018, 19, 260. [Google Scholar] [CrossRef]
- Titanji, B.K.; Aasa-Chapman, M.; Pillay, D.; Jolly, C. Protease inhibitors effectively block cell-to-cell spread of HIV-1 between T cells. Retrovirology 2013, 24, 161. [Google Scholar] [CrossRef] [Green Version]
- Agosto, L.M.; Zhong, P.; Munro, J.; Walther Mothes, W. Highly active antiretroviral therapies are effective against HIV-1 cell-to-cell transmission. PLoS Pathog. 2014, 27, e1003982. [Google Scholar] [CrossRef]
- Psomas, C.; Younas, M.; Reynes, C.; Cezar, R.; Portalès, P.; Tuaillon, E.; Guigues, A.; Merle, C.; Atoui, N.; Fernandez, C.; et al. One of the immune activation profiles observed in HIV-1-infected adults with suppressed viremia is linked to metabolic syndrome: The ACTIVIH study. EBioMedicine 2016, 8, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Castley, A.; Williams, L.; James, I.; Guelfi, G.; Berry, C.; Nolan, D. Plasma CXCL10, sCD163 and sCD14 levels have distinct associations with antiretroviral treatment and cardiovascular disease risk factors. PLoS ONE 2016, 11, e0158169. [Google Scholar]
- Li, J.Z.; Arnold, K.B.; Lo, J.; Dugast, A.S.; Plants, J.; Ribaudo, H.J.; Cesa, K.; Heisey, A.; Kuritzkes, D.R.; Lauffenburger, D.A.; et al. Differential levels of soluble inflammatory markers by human immunodeficiency virus controller status and demographics. Open Forum Infect. Dis. 2015, 2, ofu117. [Google Scholar] [CrossRef] [PubMed]
- Kroeze, S.; Wit, F.W.; Rossouw, T.M.; Steel, H.C.; Kityo, C.M.; Siwale, M.; Akanmu, S.; Mandaliya, K.; de Jager, M.; Ondoa, P.; et al. Plasma Biomarkers of Human Immunodeficiency Virus-Related Systemic Inflammation and Immune Activation in Sub-Saharan Africa Before and During Suppressive Antiretroviral Therapy. J. Infect. Dis. 2019, 6, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, T.B.; Ertner, G.; Petersen, J.; Møller, H.J.; Moestrup, S.K.; Eugen-Olsen, J.; Kronborg, G.; Benfield, T. Plasma CD163 independently predicts all-cause mortality from HIV-1 infection. J. Infect. Dis. 2016, 214, 1198–1204. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| N (%) or Median [Q1–Q3] | |
|---|---|
| Number of patients | 14 |
| Male gender | 12 (86%) |
| Age (years) | 56.7 [54.6; 63.9] |
| Years since HIV infection | 27.0 [20.7; 30.2] |
| Comorbid conditions | |
| Hypertension | 8 (57%) |
| Dyslipidemia | 4 (29%) |
| Hepatitis C coinfection | 2 (14%) |
| CD4 cell count at inclusion (cc/mm3) | 645.5 [496.8; 713.8] |
| CD8 cell count at inclusion (cc/mm3) | 687.0 [612.0; 893.0] |
| CD4/CD8 ratio at inclusion | 0.77 [0.67; 1.10] |
| CD4 nadir (cc/mm3) | 287.0 [235.3; 352.5] |
| Years on cART | 18.5 [15.0; 22.0] |
| cART regimens received | 7.0 [3.0; 7.8] |
| Months on current cART | 54.0 [37.5; 65.0] |
| cART received when switching 2 NRTI + 1 INSTI 2 NRTI + 1 NNRTI Other | 8 5 1 |
| Dual cART prescribed at inclusion: DTG + RPV DTG + 3TC | 11 3 |
| All Patients n = 14 | Likelihood of Immune Activation | ||||||
|---|---|---|---|---|---|---|---|
| Lower-n = 7 | Greater-n = 7 | ||||||
| Median | [Q1; Q3] | Median | [Q1; Q3] | Median | [Q1; Q3] | p-value * | |
| Age (years) | 56.7 | [54.6; 63.9] | 55.5 | [54.3; 58.3] | 62.4 | [55.9; 70.1] | 0.259 |
| Years since HIV infection | 27.0 | [20.7; 30.2] | 27.4 | [19.1; 29.2] | 26.7 | [23.2; 31.2] | 0.654 |
| CD4/CD8 ratio inclusion | 0.8 | [0.7; 1.1] | 0.7 | [0.6; 0.9] | 0.8 | [0.8; 1.1] | 0.383 |
| Years on cART | 18.5 | [15.0; 22.0] | 16.0 | [14.5; 22.0] | 20.0 | [16.0; 22.5] | 0.653 |
| Number of regimens received | 7.0 | [3.0; 7.8] | 6.0 | [2.0; 7.0] | 7.0 | [6.5; 8.0] | 0.295 |
| Median changes from inclusion to 6 months after the switch | |||||||
| CD4/CD8 (%) | −1.5 | [−7.1; 10.2] | 5.9 | [−1.6; 9.6] | −5.9 | [−10.7; 8.1] | 0.628 |
| sCD14 (%) | −15.0 | [−24.8; −9.9] | −17.7 | [−34.7; −8.4] | −12.3 | [−22.0; −11.3] | 0.295 |
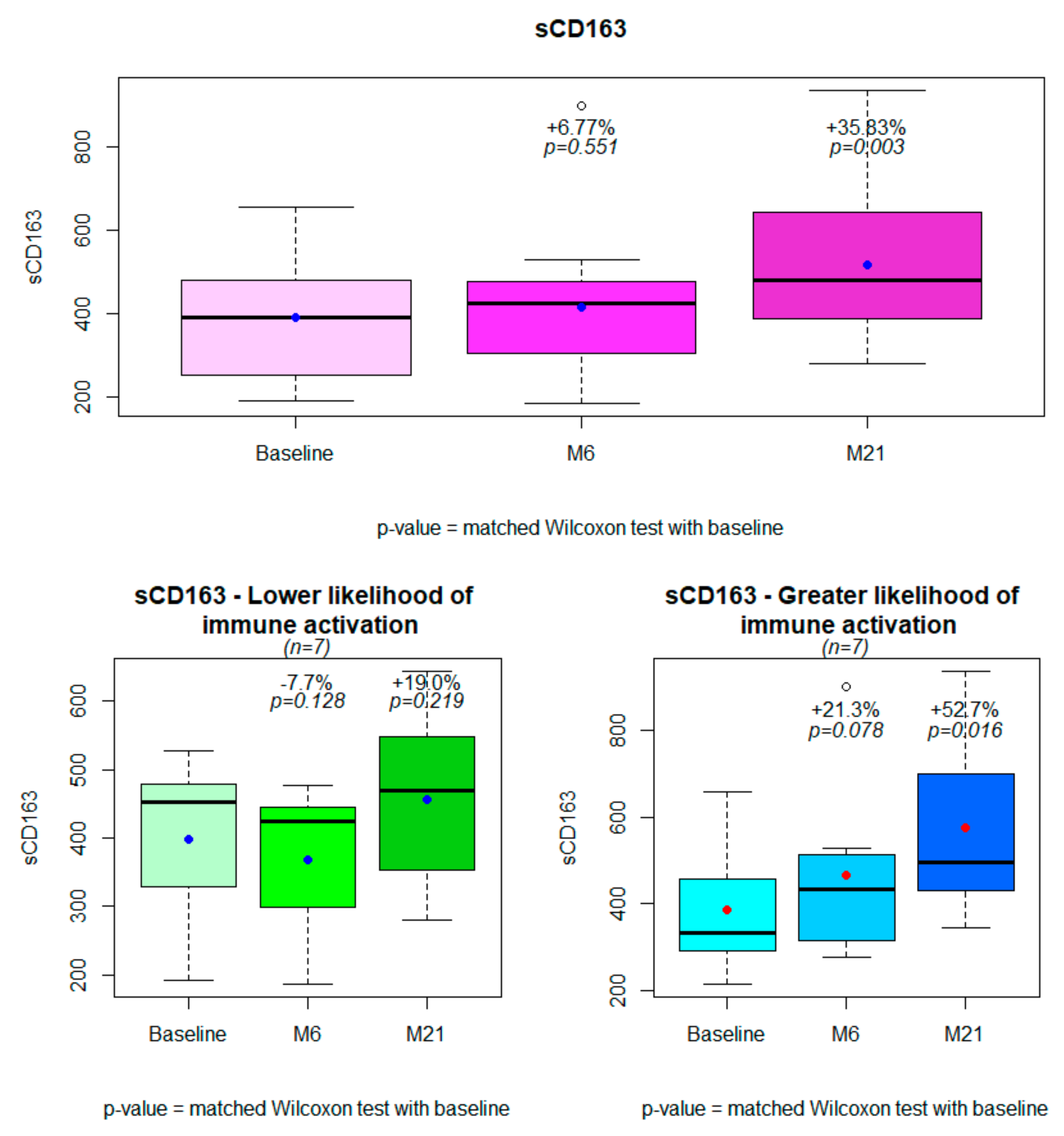
| sCD163 (%) | 0.7 | [−9.6; 29.6] | −10.0 | [−12.2; 0.7] | 29.9 | [10.8; 33.7] | 0.017 |
| LBP (%) | 8.5 | [−20.0; 25.9] | −16.8 | [−19.1; 17.7] | 15.9 | [−13.0; 81.6] | 0.456 |
| MCP-1 (%) | −19.9 | [−24.3; −3.3] | −20.6 | [−23.2; −11] | −8.4 | [−24.7; 6.1] | 0.902 |
| IP-10 (%) | −29.5 | [38.2; −19.0] | −32.1 | [−37; −24.8] | −25.7 | [−40.9; −9.0] | 0.383 |
| Median changes from inclusion to 21 months after the switch | |||||||
| CD4/CD8 (%) | −1.8 | [−11.3; 7.9] | 7.0 | [−3.8; 10.5] | −10.8 | [−14.3; 1.5] | 0.259 |
| sCD14 (%) | −63.7 | [−66.0; −58.2] | −57.7 | [−63.9; −52.2] | −65.1 | [−66.5; −63.4] | 0.128 |
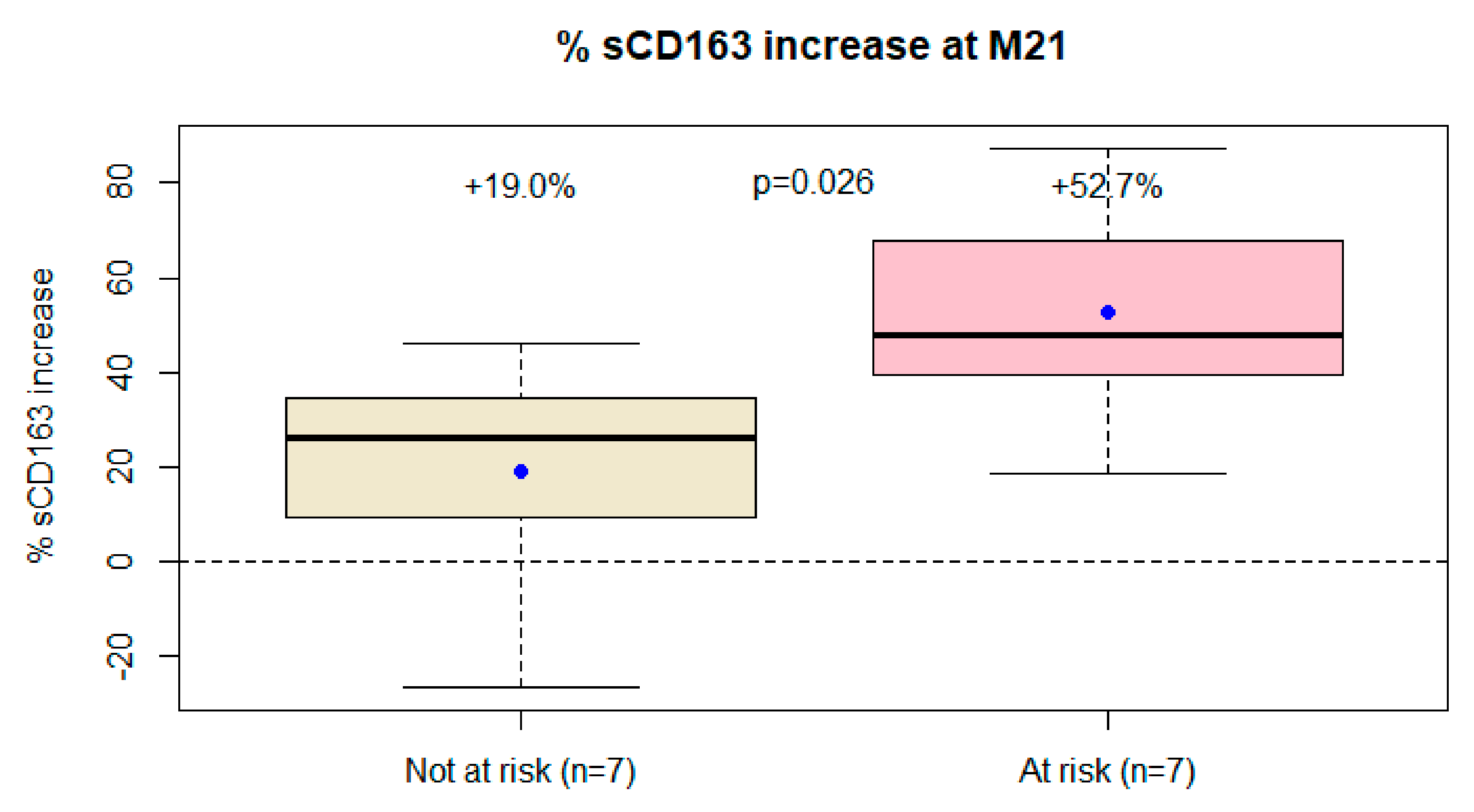
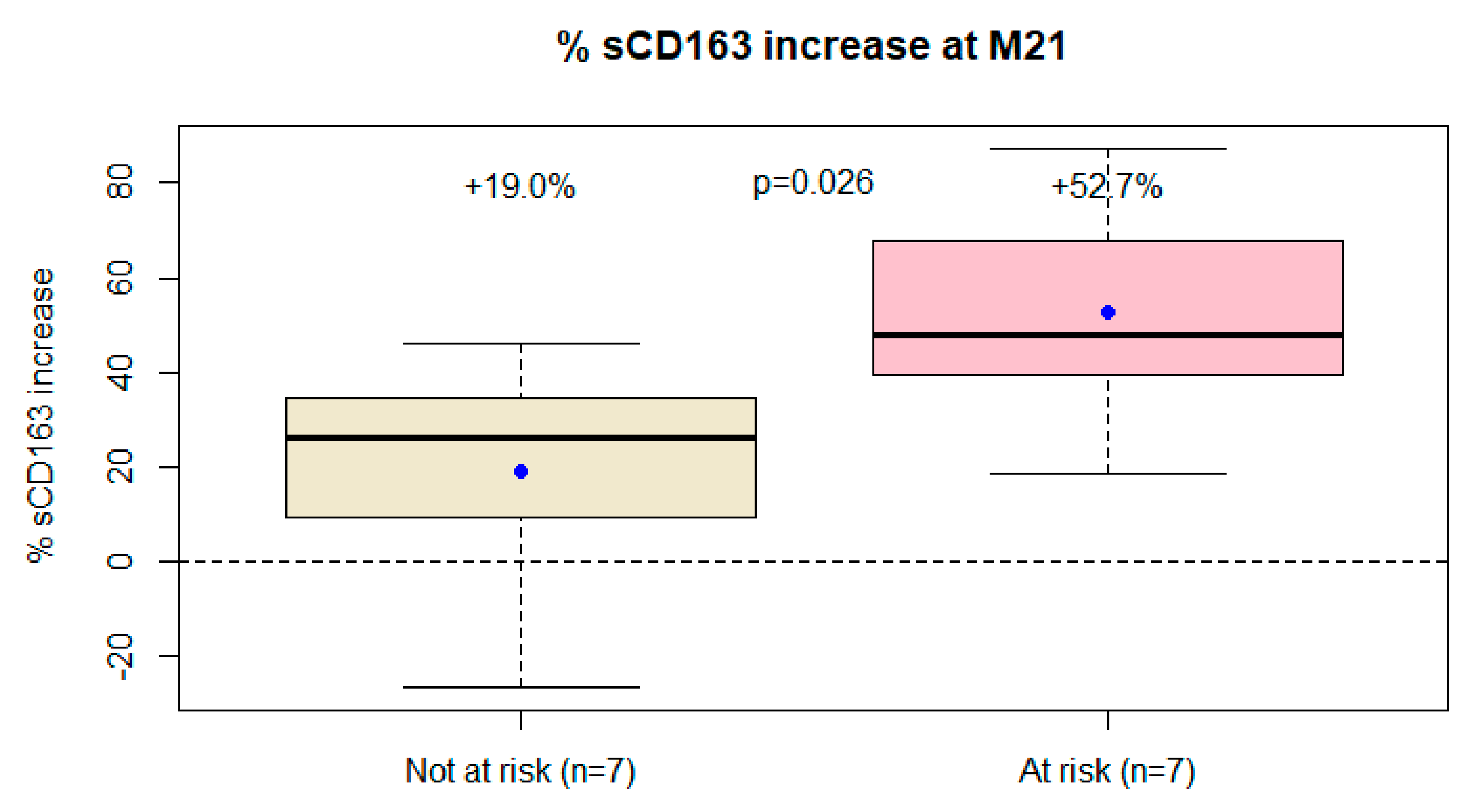
| sCD163 (%) | 39.5 | [20.3; 47.5] | 26.0 | [9.4; 34.3] | 47.9 | [39.6; 67.8] | 0.026 |
| LBP (%) | 33.0 | [−2.7; 57.8] | 8.4 | [−10.8; 40.5] | 61.6 | [15.9; 69.3] | 0.128 |
| MCP-1 (%) | −61.4 | [−64.9; −20.6] | −63.7 | [−67.9; −61.8] | −41.2 | [−60.1; 8.3] | 0.097 |
| IP-10 (%) | −57.5 | [−68.7; −43.6] | −63.4 | [−75.7; −53.0] | −53.3 | [−57.5; −25.3] | 0.209 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassallo, M.; Durant, J.; Fabre, R.; Lotte, L.; Sindt, A.; Puchois, A.; De Monte, A.; Cezar, R.; Corbeau, P.; Pradier, C. Inflammatory Markers after Switching to a Dual Drug Regimen in HIV-Infected Subjects: A Two-Year Follow-Up. Viruses 2022, 14, 927. https://doi.org/10.3390/v14050927
Vassallo M, Durant J, Fabre R, Lotte L, Sindt A, Puchois A, De Monte A, Cezar R, Corbeau P, Pradier C. Inflammatory Markers after Switching to a Dual Drug Regimen in HIV-Infected Subjects: A Two-Year Follow-Up. Viruses. 2022; 14(5):927. https://doi.org/10.3390/v14050927
Chicago/Turabian StyleVassallo, Matteo, Jacques Durant, Roxane Fabre, Laurene Lotte, Audrey Sindt, Annick Puchois, Anne De Monte, Renaud Cezar, Pierre Corbeau, and Christian Pradier. 2022. "Inflammatory Markers after Switching to a Dual Drug Regimen in HIV-Infected Subjects: A Two-Year Follow-Up" Viruses 14, no. 5: 927. https://doi.org/10.3390/v14050927
APA StyleVassallo, M., Durant, J., Fabre, R., Lotte, L., Sindt, A., Puchois, A., De Monte, A., Cezar, R., Corbeau, P., & Pradier, C. (2022). Inflammatory Markers after Switching to a Dual Drug Regimen in HIV-Infected Subjects: A Two-Year Follow-Up. Viruses, 14(5), 927. https://doi.org/10.3390/v14050927