
Impaired Vagal Activity in Long-COVID-19 Patients

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Heart Rate Variability Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-COVID syndrome in individuals admitted to hospital with covid-19: Retrospective cohort study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef] [PubMed]
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long-term effects of COVID-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; ARC Study Group; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalization for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Fogarty, H.; Dyer, A.; Martin-Loeches, I.; Bannan, C.; Nadarajan, P.; Bergin, C.; O’Farrelly, C.; Conlon, N.; Bourke, N.M.; et al. Prolonged elevation of D-dimer levels in convalescent COVID-19 patients is independent of the acute phase response. J. Thromb. Haemost. 2021, 19, 1064–1070. [Google Scholar] [CrossRef]
- Acanfora, D.; Acanfora, C.; Ciccone, M.M.; Scicchitano, P.; Bortone, A.S.; Uguccioni, M.; Casucci, G. The Cross-Talk between Thrombosis and Inflammatory Storm in Acute and Long-COVID-19: Therapeutic Targets and Clinical Cases. Viruses 2021, 13, 1904. [Google Scholar] [CrossRef]
- Barizien, N.; Le Guen, M.; Russel, S.; Touche, P.; Huang, F.; Vallée, A. Clinical characterization of dysautonomia in long COVID-19 patients. Sci. Rep. 2021, 7, 14042. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Kleiger, R.E.; Rottman, J.N. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 1992, 85, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Task Force of the European Society of Cardiology; The North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Takabatake, N.; Nakamura, H.; Minamihaba, O.; Inage, M.; Inoue, S.; Kagaya, S.; Yamaki, M.; Tomoike, H. A novel pathophysiologic phenomenon in cachexic patients with chronic obstructive pulmonary disease: The relationship between the circadian rhythm of circulating leptin and the very low-frequency component of heart rate variability. Am. J. Respir. Crit. Care Med. 2001, 163, 1314–1319. [Google Scholar] [CrossRef]
- Vinik, A.I.; Ziegler, D. Diabetic cardiovascular autonomic neuropathy. Circulation 2007, 115, 387–397. [Google Scholar] [CrossRef]
- Marvar, P.J.; Harrison, D.G. Inflammation, immunity and the autonomic nervous system. In Primer on the Autonomic Nervous System; Robertson, D., Biaggioni, I., Burnstock, G., Low, P.A., Paton, J.F.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2012; pp. 325–329. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2021; Epub ahead of print. [Google Scholar] [CrossRef]
- De Terwangne, C.; Laouni, J.; Jouffe, L.; Lechien, J.; Bouillon, V.; Place, S.; Capulzini, L.; Machayekhi, S.; Ceccarelli, A.; Saussez, S.; et al. Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE). Pathogens 2020, 9, 880. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Boon, G.J.; Barco, S.; Endres, M.; Geelhoed, J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef] [PubMed]
- Antonelli Incalzi, R.; Corsonello, A.; Trojano, L.; Pedone, C.; Acanfora, D.; Spada, A.; D’Addio, G.; Maestri, R.; Rengo, F.; Rengo, G. Heart rate variability and drawing impairment in hypoxemic COPD. Brain Cogn. 2009, 70, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA; Hillsdale, NJ, USA, 1988. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 30 September 2021).
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Womens Health 2022. [Google Scholar] [CrossRef]
- Swai, J.; Hu, Z.; Zhao, X.; Rugambwa, T.; Ming, G. Heart rate and heart rate variability comparison between postural orthostatic tachycardia syndrome versus healthy participants; a systematic review and meta-analysis. BMC Cardiovasc. Disord. 2019, 19, 320. [Google Scholar] [CrossRef] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.V.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Achar, A.; Ghosh, C. COVID-19-Associated Neurological Disorders: The Potential Route of CNS Invasion and Blood-Brain Relevance. Cells 2020, 9, 2360. [Google Scholar] [CrossRef]
- Fenrich, M.; Mrdenovic, S.; Balog, M.; Tomic, S.; Zjalic, M.; Roncevic, A.; Mandic, D.; Debeljak, Z.; Heffer, M. SARS-CoV-2 Dissemination Through Peripheral Nerves Explains Multiple Organ Injury. Front. Cell. Neurosci. 2020, 14, 229. [Google Scholar] [CrossRef]
- Donoghue, M.; Hsieh, F.; Baronas, E.; Godbout, K.; Gosselin, M.; Stagliano, N.; Donovan, M.; Woolf, B.; Robison, K.; Jeyaseelan, R.; et al. A Novel Angiotensin-Converting Enzyme–Related Carboxypeptidase (ACE2) Converts Angiotensin I to Angiotensin 1-9. Circ. Res. 2000, 87, e1–e9. [Google Scholar] [CrossRef]
- Gowrisankar, Y.V.; Clar, M.A. Angiotensin II regulation of angiotensin-converting enzymes in spontaneously hypertensive rat primary astrocyte cultures. J. Neurochem. 2016, 138, 74–85. [Google Scholar] [CrossRef] [Green Version]
- Xia, H.; Lazartigues, E. Angiotensin-Converting Enzyme 2: Central Regulator for Cardiovascular Function. Curr. Hypertens. Rep. 2010, 12, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Kanberg, N.; Ashton, N.J.; Andersson, L.M.; Yilmaz, A.; Lindh, M.; Nilsson, S.; Price, R.W.; Blennow, K.; Zetterberg, H.; Gisslén, M. Neurochemical evidence of astrocytic and neuronal injury commonly found in COVID-19. Neurology 2020, 95, e1754–e1759. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; Savoldi, A.; Donadello, K.; Zanzoni, S.; Bozzetti, S.; Carta, S.; Zivelonghi, C.; Alberti, D.; Piraino, F.; Minuz, P.; et al. Nervous system: Subclinical target of SARS-CoV-2 infection. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1010–1012. [Google Scholar] [CrossRef] [PubMed]
- Reza-Zaldívar, E.E.; Hernández-Sapiéns, M.A.; Minjarez, B.; Gómez-Pinedo, U.; Márquez-Aguirre, A.L.; Mateos-Díaz, J.C.; Matias-Guiu, J.; Canales-Aguirre, A.A. Infection Mechanism of SARS-COV-2 and Its Implication on the Nervous System. Front. Immunol. 2021, 11, 621735. [Google Scholar] [CrossRef] [PubMed]
- Bulfamante, G.; Bocci, T.; Falleni, M.; Campiglio, L.; Coppola, S.; Tosi, D.; Chiumello, D.; Priori, A. Brainstem neuropathology in two cases of COVID-19: SARS-CoV-2 trafficking between brain and lung. J. Neurol. 2021, 268, 4486–4491. [Google Scholar] [CrossRef]
- Caro-Codón, J.; Rey, J.R.; Buño, A.; Iniesta, A.M.; Rosillo, S.O.; Castrejon-Castrejon, S.; Rodriguez-Sotelo, L.; Martinez, L.A.; Marco, I.; Merino, C.; et al. CARD-COVID Investigators. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur. J. Heart Fail. 2021, 23, 456–464. [Google Scholar] [CrossRef]
- Acanfora, D.; Scicchitano, P.; Acanfora, C.; Maestri, R.; Goglia, F.; Incalzi, R.A.; Bortone, A.S.; Ciccone, M.M.; Uguccioni, M.; Casucci, G. Early Initiation of Sacubitril/Valsartan in Patients with Chronic Heart Failure After Acute Decompensation: A Case Series Analysis. Clin. Drug Investig. 2020, 40, 493–501. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, Z.; Tse, G.; Zhang, L.; Wan, E.Y.; Guo, Y.; Lip, G.Y.H.; Li, G.; Lu, Z.; Liu, T. Cardiac arrhythmias in patients with COVID-19. J. Arrhythm. 2020, 36, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Courel-Ibáñez, J. Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5434. [Google Scholar] [CrossRef]
- Acanfora, C.; Casucci, G. Neprilysin inhibitor-angiotensin II receptor blocker combination (sacubitril/valsartan): Rationale for adoption in SARS-CoV-2 patients. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 135–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Demographics, Medical History and Vital Signs | Long-COVID-19 | No-COVID-19 | Effect Size Cohens-d b |
|---|---|---|---|
| Number of patients, n | 30 | 20 | |
| Sex, M/F, n | 17/13 | 8/12 | |
| Age, years a | 58.6 ± 17.6 | 56.3 ± 14.7 | 0.14 |
| Weight, kg a | 77.1 ± 14.5 | 73.8 ± 12 | 0.25 |
| Height, cm a | 164.6 ± 11.4 | 169.1 ± 8.7 | 0.44 |
| Body mass index, kg/m2 a | 28.4 ± 4.2 | 25.7 ± 2.4 | 0.79 |
| Pre-existing conditions in the last year, n (%) | |||
| Cancer | 2 (6.7%) | 1 (5.0%) | |
| Chronic heart disease | 13 (43.3%) | 6 (30.0%) | |
| Chronic kidney disease | 5 (16.6%) | 2 (10.0%) | |
| Chronic liver disease | 3 (10.0%) | 1 (5.0%) | |
| Chronic lung disease | 7 (23.3%) | 7 (35.0%) | |
| Chronic neurological disease | 9 (30.0%) | 5 (25.0%) | |
| Diabetes | 7 (23.7%) | 3 (15.0%) | |
| Hypertension | 19 (63.3%) | 11 (55.0%) | |
| Mental health conditions | 2 (6.66%) | 1 (5.0%) | |
| Obesity (Body Mass Index > 30) | 11 (36.6%) | 3 (15.0%) | |
| Heart rate, bpm a | 73 ± 15 | 70 ± 13 | 0.21 |
| Systolic blood pressure, mmHg a | 121 ± 15 | 121 ± 17 | 0 |
| Diastolic blood pressure, mmHg a | 78 ± 12 | 76 ± 10 | 0.18 |
| Therapies, n (%) | |||
| ACE-I/ARB/ARNIs | 19 (63%) | 12 (60%) | |
| Beta-blockers | 11 (37%) | 8 (40%) | |
| ASA | 13 (43%) | 9 (45%) | |
| Diuretics | 11 (37%) | 6 (30%) | |
| Anticoagulants | 12 (40%) | 6 (30%) | |
| Echocardiography Measurements | |||
| LV end diastolic dimension, cm a | 4.8 ± 1 | 4.5 ± 0.6 | 0.36 |
| LV end diastolic volume, mL a | 114.6 ± 52.5 | 94.1 ± 27.9 | 0.49 |
| LV end systolic dimension, cm a | 3.2 ± 1.04 | 2.6 ± 0.5 * | 0.73 |
| LV end systolic volume, mL a | 48.7 ± 38.5 | 28 ± 10.5 † | 0.73 |
| LV ejection fraction, % a | 61.9 ± 13.7 | 70.4 ± 5.7 • | 0.81 |
| Left atrial anteroposterior dimension, cm a | 3.7 ± 1.3 | 3.5 ± 0.5 | 0.20 |
| E/A ratio a | 1.02 ± 0.4 | 1.1 ± 0.3 | 0.22 |
| SPAP, mmHg a | 13.8 ± 10.5 | 14.6 ± 8.6 | 0.08 |
| Laboratory Values (Reference Range) | Long-COVID-19 | No-COVID-19 | Effect Size Cohens-d b |
|---|---|---|---|
| White Blood Cell count (3.7–10.3), ×109/L a | 6.84 ± 2.6 | 7.14 ± 2.3 | 0.12 |
| Red Blood Cell count (4.0–10.0), ×106/L a | 4.53 ± 0.6 | 4.8 ± 0.58 | 0.46 |
| Haemoglobin (13.7–17.5), g/dL a | 14.9 ± 6.4 | 14.2 ± 1.8 | 0.15 |
| Platelet count (155–369), ×109/L a | 221 ± 92 | 244 ± 50 | 0.31 |
| Prothrombin time (9.6–12.5), second a | 14.2 ± 2.5 | 13.5 ± 1.2 | 0.36 |
| International normalized ratio (0.9–1.2) a | 1.07 ± 0.2 | 1.00 ± 0.09 | 0.45 |
| Activated Partial Thromboplastin Time (19–30), s a | 30.6 ± 5.1 | 28.8 ± 2.6 | 0.44 |
| Fibrinogen (150–450), mg/dL a | 364.8 ± 154.4 | 326.9 ± 86.1 | 0.30 |
| Lactate dehydrogenase (140–280), U/L a | 448.1 ± 133 | 342.45 ± 90.5 * | 0.93 |
| Creatinine (0.8–1.30), mg/dL a | 0.92 ± 0.25 | 0.86 ± 0.23 | 0.25 |
| Aspartate Aminotransferase (0–31), U/L a | 25.04 ± 12.2 | 21.6 ± 12.2 | 0.28 |
| Alanine Aminotransferase (0–34), U/L a | 25.2 ± 14.5 | 20.9 ± 14.6 | 0.3 |
| High Sensitivity C Reactive Protein (0–45), mg/L a | 16.3 ± 50.1 | 3.95 ± 8.8 | 0.34 |
| Sodium (135–155), mEq/L a | 139 ± 2.7 | 139 ± 2.02 | 0 |
| Potassium (3.5–5.5), mEq/L a | 4.1 ± 0.27 | 4.3 ± 0.4 | 0.59 |
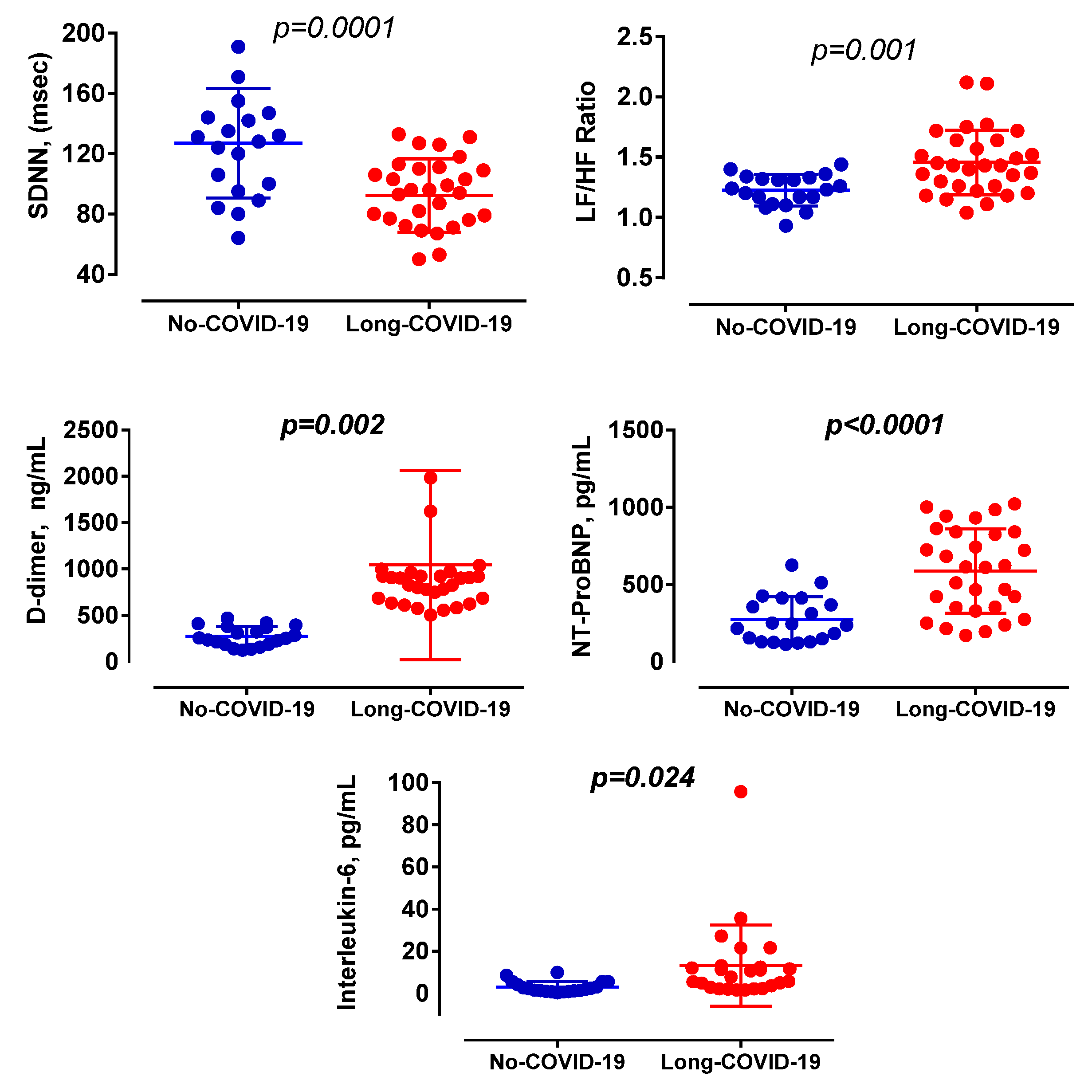
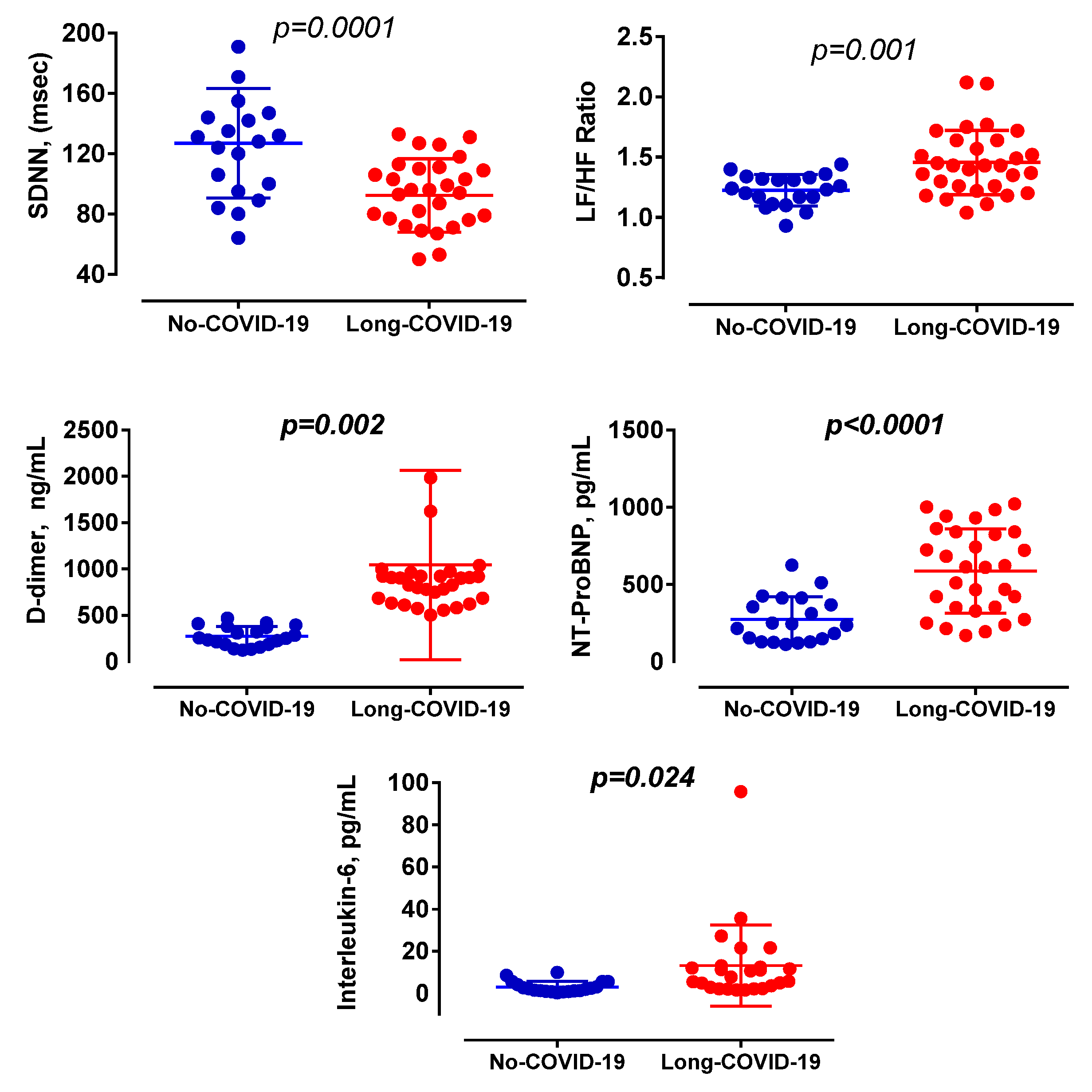
| D-dimer (250–500), ng/mL a | 1044.4 ± 1022 | 273.7 ± 106 † | 1.06 |
| Erythrocyte Sedimentation Rate (0–15), mm a | 25.7 ± 33.2 | 15.5 ± 17.2 | 0.38 |
| Albuminuria (0–2.5), mg/dL a | 120.7 ± 134.7 | 64.6 ± 17.7 | 0.58 |
| Interleukin-6 (0–6.4), pg/mL a | 13.2 ± 3 | 3 ± 2.7 • | 3.58 |
| High-sensitivity Cardiac Troponin (<19), ng/mL a | 9 ± 26.3 | 1.6 ± 0.3 | 0.4 |
| NT-ProBNP (<450), pg/mL a | 587.4 ± 273 | 273.5 ± 147.9 ◊ | 1.43 |
| SARS-CoV-2 Anti-Spike IgM (<1), EU/mL a | 12.2 ± 35.5 | 1.04 ± 2.4 | 0.44 |
| SARS-CoV-2 Anti-Spike IgG (<10), EU/mL a | 91.5 ± 130.1 | 35.9 ± 61.5 | 0.54 |
| Serum Ferritin (20–300), ng/mL a | 144.6 ± 158.6 | 113 ± 85.7 | 0.3 |
| Long-COVID-19 | No-COVID-19 | Effect Size Cohens-d b | |
|---|---|---|---|
| Average Heart Rate (beats/min) a | 72.6 ± 12.4 | 67.1 ± 7.2 | 0.54 |
| Minimum Heart Rate (beats/min) a | 53.4 ± 8.0 | 48.5 ± 7.4 * | 0.64 |
| Maximum Heart Rate (beats/min) a | 112.9 ± 20.8 | 108.5 ± 23.7 | 0.20 |
| Supraventricular ectopic beats (ln + 1) a | 4.6 ± 2.3 | 4.16 ± 2.2 | 0.19 |
| Ventricular Ectopic Beats (ln + 1) a | 4.6 ± 2.6 | 3.0 ± 2.0 | 0.69 |
| Maximum QT (msec) a | 464.97 ± 44.5 | 462 ± 83.2 | 0.04 |
| Maximum QTc (msec) a | 488.5 ± 38.2 | 488.6 ± 79.7 | 0.01 |
| Heart Rate Variability (Time Domain) | |||
| SDNN (msec) a | 92.3 ± 24.4 | 127 ± 36.4 † | 1.12 |
| SDANN (msec) a | 79 ± 21.9 | 109.9 ± 36.8 • | 1.02 |
| SDNNi a | 41.9 ± 15.3 | 57.6 ± 14.5 • | 1.05 |
| rMSSD (msec) a | 24.5 ± 12.3 | 33.9 ± 20.9 | 0.55 |
| pNN50 (%)a | 5.7 ± 7.8 | 10.8 ± 11.2 | 0.53 |
| Heart Rate Variability (Spectral Power) | |||
| Total Power (ln msec2) a | 7.46 ± 0.5 | 8.08 ± 0.6 ◊ | 1.12 |
| VLF (ln msec2) a | 6.84 ± 0.8 | 7.66 ± 0.6 ◊ | 1.16 |
| LF (ln msec2) a | 6.55 ± 0.42 | 6.44 ± 0.74 | 0.18 |
| HF (ln msec2) a | 4.65 ± 0.9 | 5.33 ± 0.9 •• | 0.76 |
| LF/HF Ratio a | 1.46 ± 0.27 | 1.23 ± 0.13 • | 1.09 |
| Standardized β-Coefficient | p | |
|---|---|---|
| D-dimer (250–500), ng/mL | 0.259 | 0.047 |
| NT-ProBNP (<450), pg/mL | 0.281 | 0.043 |
| HF (ln msec2) | 0.696 | 0.029 |
| LF/HF Ratio | 0.820 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acanfora, D.; Nolano, M.; Acanfora, C.; Colella, C.; Provitera, V.; Caporaso, G.; Rodolico, G.R.; Bortone, A.S.; Galasso, G.; Casucci, G. Impaired Vagal Activity in Long-COVID-19 Patients. Viruses 2022, 14, 1035. https://doi.org/10.3390/v14051035
Acanfora D, Nolano M, Acanfora C, Colella C, Provitera V, Caporaso G, Rodolico GR, Bortone AS, Galasso G, Casucci G. Impaired Vagal Activity in Long-COVID-19 Patients. Viruses. 2022; 14(5):1035. https://doi.org/10.3390/v14051035
Chicago/Turabian StyleAcanfora, Domenico, Maria Nolano, Chiara Acanfora, Camillo Colella, Vincenzo Provitera, Giuseppe Caporaso, Gabriele Rosario Rodolico, Alessandro Santo Bortone, Gennaro Galasso, and Gerardo Casucci. 2022. "Impaired Vagal Activity in Long-COVID-19 Patients" Viruses 14, no. 5: 1035. https://doi.org/10.3390/v14051035
APA StyleAcanfora, D., Nolano, M., Acanfora, C., Colella, C., Provitera, V., Caporaso, G., Rodolico, G. R., Bortone, A. S., Galasso, G., & Casucci, G. (2022). Impaired Vagal Activity in Long-COVID-19 Patients. Viruses, 14(5), 1035. https://doi.org/10.3390/v14051035