
Angiotensin Converting Enzyme Inhibitors May Increase While Active Vitamin D May Decrease the Risk of Severe Pneumonia in SARS-CoV-2 Infected Patients with Chronic Kidney Disease on Maintenance Hemodialysis


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Definitions
2.3. Data Collection and Procedures
2.4. Statistical Analyses
3. Results
3.1. Patients Characteristic
3.2. Clinical Presentation on Admission
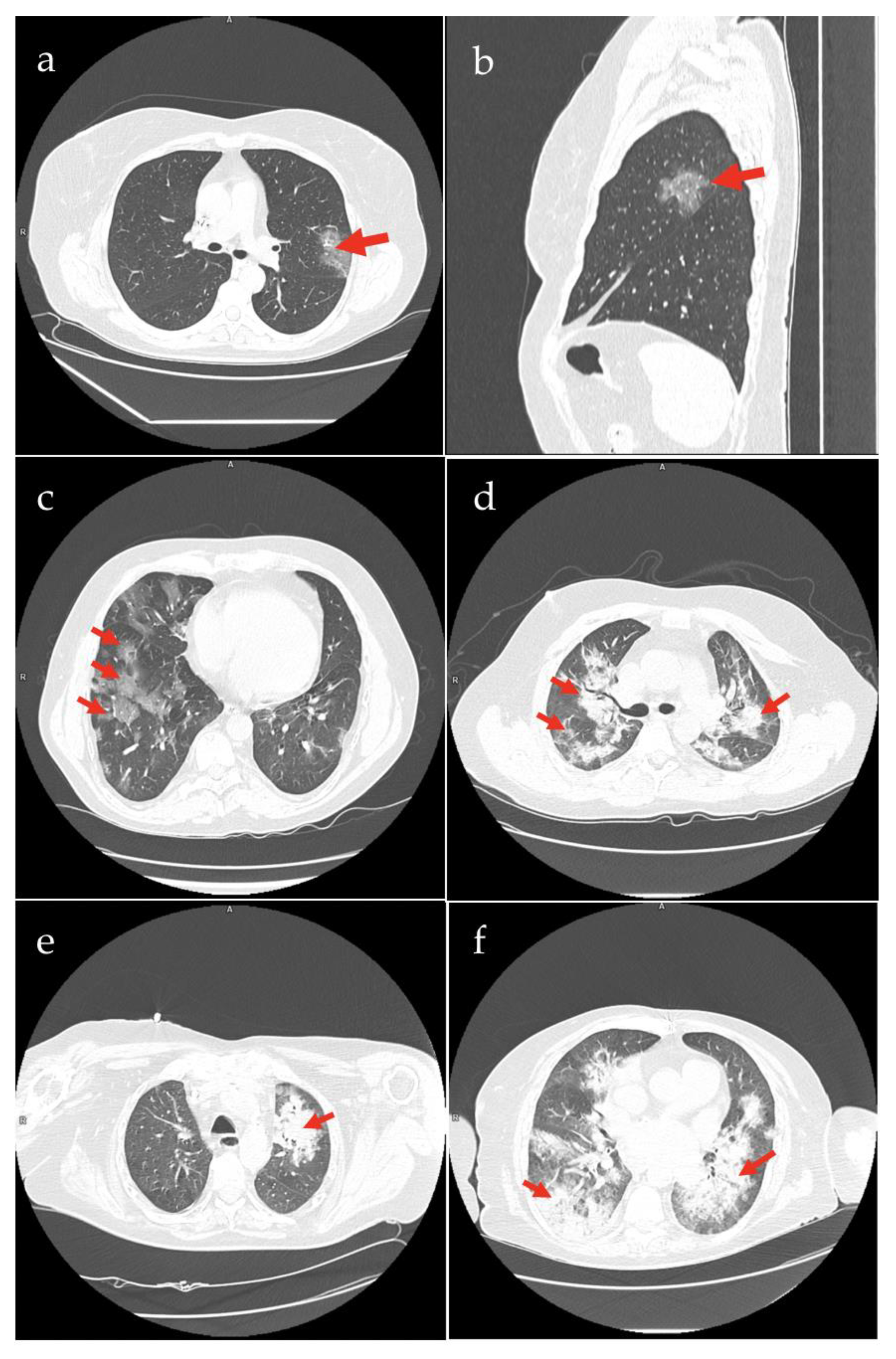
3.3. Imaging Evaluation
3.4. Factors Associated with Severe COVID-19 Pneumonia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hasan, M.N.; Haider, N.; Stigler, F.L.; Khan, R.A.; McCoy, D.; Zumla, A.; Kock, R.A.; Uddin, M.J. The Global Case-Fatality Rate of COVID-19 Has Been Declining Since May 2020. Am. J. Trop. Med. Hyg. 2021, 104, 2176. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Puchalska-Reglińska, E.; Debska-Slizien, A.; Biedunkiewicz, B.; Tylicki, P.; Polewska, K.; Rutkowski, B.; Gellert, R.; Tylicki, L. Extremely high mortality in COVID-19 hemodialyzed patients before the anti-SARS-CoV-2 vaccination era. Large database from the North of Poland. Pol. Arch. Intern. Med. 2021, 131, 643–648. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef]
- Och, A.; Tylicki, P.; Polewska, K.; Puchalska-Reglińska, E.; Parczewska, A.; Szabat, K.; Biedunkiewicz, B.; Debska Slizien, A.; Tylicki, L. Persistent post-COVID-19 syndrome in hemodialyzed patients-a longitudinal cohort study from the North of Poland. J. Clin. Med. 2021, 10, 4451. [Google Scholar] [CrossRef]
- Ojo, A.S.; Balogun, S.A.; Williams, O.T.; Ojo, O.S. Pulmonary Fibrosis in COVID-19 Survivors: Predictive Factors and Risk Reduction Strategies. Pulm. Med. 2020, 2020, 6175964. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 Pulmonary Fibrosis: Novel Sequelae of the Current Pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef]
- Surendra, N.K.; Abdul Manaf, M.R.; Hooi, L.S.; Bavanandan, S.; Mohamad Nor, F.S.; Shah Firdaus Khan, S.; Ong, L.M.; Abdul Gafor, A.H. Health related quality of life of dialysis patients in Malaysia: Haemodialysis versus continuous ambulatory peritoneal dialysis. BMC Nephrol. 2019, 20, 151. [Google Scholar] [CrossRef] [Green Version]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Biedunkiewicz, B.; Tylicki, L.; Puchalska-Reglińska, E.; Dąbrowska, M.; Ślizień, W.; Kubanek, A.; Rąbalski, Ł.; Kosiński, M.; Grzybek, M.; Renke, M.; et al. SARS-CoV-2 infection in vaccinated maintenance hemodialysis patients despite anti-spike seroconversion: A report of 3 breakthrough cases. Eur. J. Transl. Clin. Med. 2022, 5. [Google Scholar] [CrossRef]
- Simon, B.; Rubey, H.; Treipl, A.; Gromann, M.; Hemedi, B.; Zehetmayer, S.; Kirsch, B. Haemodialysis patients show a highly diminished antibody response after COVID-19 mRNA vaccination compared to healthy controls. Nephrol. Dial. Transplant. 2021, 36, 1709–1716. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwobel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Tylicki, L.; Biedunkiewicz, B.; Dabrowska, M.; Slizien, W.; Tylicki, P.; Polewska, K.; Rosenberg, I.; Rodak, S.; Debska-Slizien, A. Humoral response to SARS-CoV-2 vaccination promises to improve the catastrophic prognosis of hemodialysis patients as a result of COVID-19: The COViNEPH Project. Pol. Arch. Intern. Med. 2021, 131, 797–801. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Alonso, R.; Camon, A.M.; Cardozo, C.; Albiach, L.; Aguero, D.; Marcos, M.A.; Ambrosioni, J.; Bodro, M.; Chumbita, M.; et al. Impact of remdesivir according to the pre-admission symptom duration in patients with COVID-19. J. Antimicrob. Chemother. 2021, 76, 3296–3302. [Google Scholar] [CrossRef]
- Petrak, R.M.; Van Hise, N.W.; Skorodin, N.C.; Fliegelman, R.M.; Chundi, V.; Didwania, V.; Han, A.; Harting, B.P.; Hines, D.W. Early Tocilizumab Dosing Is Associated With Improved Survival in Critically Ill Patients Infected With Severe Acute Respiratory Syndrome Coronavirus-2. Crit. Care Explor. 2021, 3, e0395. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Nicolau, D.V., Jr.; Langford, B.; Mahdi, M.; Jeffers, H.; Mwasuku, C.; Krassowska, K.; Fox, R.; Binnian, I.; Glover, V.; et al. Inhaled budesonide in the treatment of early COVID-19 (STOIC): A phase 2, open-label, randomised controlled trial. Lancet Respir. Med. 2021, 9, 763–772. [Google Scholar] [CrossRef]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef]
- Pongpirul, W.A.; Wiboonchutikul, S.; Charoenpong, L.; Panitantum, N.; Vachiraphan, A.; Uttayamakul, S.; Pongpirul, K.; Manosuthi, W.; Prasithsirikul, W. Clinical course and potential predictive factors for pneumonia of adult patients with Coronavirus Disease 2019 (COVID-19): A retrospective observational analysis of 193 confirmed cases in Thailand. PLoS Negl. Trop. Dis. 2020, 14, e0008806. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 393. [Google Scholar] [CrossRef] [PubMed]
- Saeed, G.A.; Gaba, W.; Shah, A.; Al Helali, A.A.; Raidullah, E.; Al Ali, A.B.; Elghazali, M.; Ahmed, D.Y.; Al Kaabi, S.G.; Almazrouei, S. Correlation between Chest CT Severity Scores and the Clinical Parameters of Adult Patients with COVID-19 Pneumonia. Radiol. Res. Pract. 2021, 2021, 6697677. [Google Scholar] [CrossRef]
- Goicoechea, M.; Sanchez Camara, L.A.; Macias, N.; Munoz de Morales, A.; Rojas, A.G.; Bascunana, A.; Arroyo, D.; Vega, A.; Abad, S.; Verde, E.; et al. COVID-19: Clinical course and outcomes of 36 hemodialysis patients in Spain. Kidney Int. 2020, 98, 27–34. [Google Scholar] [CrossRef]
- Petrulewicz, A.; Rydzewska-Rosolowska, A.; Fiderkiewicz, B.; Wasinska-Krawczyk, A.; Brzosko, S.; Walecki, J.; Rydzewski, A. The clinical course and short-term outcomes of coronavirus disease 2019 in a cohort of hemodialysis patients. Pol. Arch. Intern. Med. 2020, 130, 809–812. [Google Scholar] [CrossRef]
- Turgutalp, K.; Ozturk, S.; Arici, M.; Eren, N.; Gorgulu, N.; Islam, M.; Uzun, S.; Sakaci, T.; Aydin, Z.; Sengul, E.; et al. Determinants of mortality in a large group of hemodialysis patients hospitalized for COVID-19. BMC Nephrol. 2021, 22, 29. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutierrez-Ocampo, E.; Villamizar-Pena, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Creput, C.; Fumeron, C.; Toledano, D.; Diaconita, M.; Izzedine, H. COVID-19 in Patients Undergoing Hemodialysis: Prevalence and Asymptomatic Screening During a Period of High Community Prevalence in a Large Paris Center. Kidney Med. 2020, 2, 716–723. [Google Scholar] [CrossRef]
- Tang, H.; Tu, C.; Xiong, F.; Sun, X.; Tian, J.B.; Dong, J.W.; Wang, X.H.; Lei, C.T.; Liu, J.; Zhao, Z.; et al. Risk factors for the mortality of hemodialysis patients with COVID-19: A multicenter study from the overall hemodialysis population in Wuhan. Semin. Dial. 2022, 35, 71–80. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Zheng, C. Evolution of CT Manifestations in a Patient Recovered from 2019 Novel Coronavirus (2019-nCoV) Pneumonia in Wuhan, China. Radiology 2020, 295, 20. [Google Scholar] [CrossRef]
- Yuan, M.; Yin, W.; Tao, Z.; Tan, W.; Hu, Y. Association of radiologic findings with mortality of patients infected with 2019 novel coronavirus in Wuhan, China. PLoS ONE 2020, 15, e0230548. [Google Scholar] [CrossRef] [Green Version]
- Bayraktaroglu, S.; Cinkooglu, A.; Ceylan, N.; Savas, R. The novel coronavirus pneumonia (COVID-19): A pictorial review of chest CT features. Diagn. Interv. Radiol. 2021, 27, 188–194. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Tylicki, L.; Puchalska-Reglińska, E.; Tylicki, P.; Och, A.; Polewska, K.; Biedunkiewicz, B.; Parczewska, A.; Szabat, K.; Wolf, J.; Dębska-Ślizień, A. Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection. J. Clin. Med. 2022, 11, 285. [Google Scholar] [CrossRef]
- Mejia, F.; Medina, C.; Cornejo, E.; Morello, E.; Vasquez, S.; Alave, J.; Schwalb, A.; Malaga, G. Oxygen saturation as a predictor of mortality in hospitalized adult patients with COVID-19 in a public hospital in Lima, Peru. PLoS ONE 2020, 15, e0244171. [Google Scholar] [CrossRef]
- Xie, J.; Covassin, N.; Fan, Z.; Singh, P.; Gao, W.; Li, G.; Kara, T.; Somers, V.K. Association Between Hypoxemia and Mortality in Patients With COVID-19. Mayo Clin. Proc. 2020, 95, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Sommerstein, R.; Kochen, M.M.; Messerli, F.H.; Grani, C. Coronavirus Disease 2019 (COVID-19): Do Angiotensin-Converting Enzyme Inhibitors/Angiotensin Receptor Blockers Have a Biphasic Effect? J. Am. Heart Assoc. 2020, 9, e016509. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.H. Hypothesis: Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may increase the risk of severe COVID-19. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, Y.; Kuba, K.; Rao, S.; Huan, Y.; Guo, F.; Guan, B.; Yang, P.; Sarao, R.; Wada, T.; Leong-Poi, H.; et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature 2005, 436, 112–116. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Tan, P.S.; Coupland, C. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people. Heart 2020. [Google Scholar] [CrossRef]
- Kim, G.J.; Melgoza, A.; Jiang, F.; Guo, S. The effect of renin-angiotensin-aldosterone system inhibitors on organ-specific ace2 expression in zebrafish and its implications for COVID-19. Sci. Rep. 2021, 11, 23670. [Google Scholar] [CrossRef]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 566. [Google Scholar] [CrossRef]
- Guven, M.; Gultekin, H. The effect of high-dose parenteral vitamin D3 on COVID-19-related inhospital mortality in critical COVID-19 patients during intensive care unit admission: An observational cohort study. Eur. J. Clin. Nutr. 2021, 75, 1383–1388. [Google Scholar] [CrossRef]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.D.; Karra, M.L.; Raju, I.; Ragini; Chinapaka, S.; Baba, K.; Kandakatla, M. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID 19 disease. Sci. Rep. 2021, 11, 10641. [Google Scholar] [CrossRef]
- Stroehlein, J.K.; Wallqvist, J.; Iannizzi, C.; Mikolajewska, A.; Metzendorf, M.I.; Benstoem, C.; Meybohm, P.; Becker, M.; Skoetz, N.; Stegemann, M.; et al. Vitamin D supplementation for the treatment of COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2021, 5, CD015043. [Google Scholar] [CrossRef]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D.; et al. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- Chauss, D.; Freiwald, T.; McGregor, R.; Yan, B.; Wang, L.; Nova-Lamperti, E.; Kumar, D.; Zhang, Z.; Teague, H.; West, E.E.; et al. Autocrine vitamin D signaling switches off pro-inflammatory programs of TH1 cells. Nat. Immunol. 2021, 23, 62–74. [Google Scholar] [CrossRef]
- Patti, G.; Pellegrino, C.; Ricciardi, A.; Novara, R.; Cotugno, S.; Papagni, R.; Guido, G.; Totaro, V.; De Iaco, G.; Romanelli, F.; et al. Potential Role of Vitamins A, B, C, D and E in TB Treatment and Prevention: A Narrative Review. Antibiotics 2021, 10, 1354. [Google Scholar] [CrossRef]
- Mily, A.; Rekha, R.S.; Kamal, S.M.; Akhtar, E.; Sarker, P.; Rahim, Z.; Gudmundsson, G.H.; Agerberth, B.; Raqib, R. Oral intake of phenylbutyrate with or without vitamin D3 upregulates the cathelicidin LL-37 in human macrophages: A dose finding study for treatment of tuberculosis. BMC Pulm. Med. 2013, 13, 23. [Google Scholar] [CrossRef] [Green Version]
- Fabri, M.; Stenger, S.; Shin, D.M.; Yuk, J.M.; Liu, P.T.; Realegeno, S.; Lee, H.M.; Krutzik, S.R.; Schenk, M.; Sieling, P.A.; et al. Vitamin D is required for IFN-gamma-mediated antimicrobial activity of human macrophages. Sci. Transl. Med. 2011, 3, 104ra102. [Google Scholar] [CrossRef] [Green Version]
- Gibson, C.C.; Davis, C.T.; Zhu, W.; Bowman-Kirigin, J.A.; Walker, A.E.; Tai, Z.; Thomas, K.R.; Donato, A.J.; Lesniewski, L.A.; Li, D.Y. Dietary Vitamin D and Its Metabolites Non-Genomically Stabilize the Endothelium. PLoS ONE 2015, 10, e0140370. [Google Scholar] [CrossRef] [Green Version]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef]
- Matias, P.J.; Jorge, C.; Ferreira, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. Cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac dimension parameters. Clin. J. Am. Soc. Nephrol. 2010, 5, 905–911. [Google Scholar] [CrossRef]
- Marckmann, P.; Agerskov, H.; Thineshkumar, S.; Bladbjerg, E.M.; Sidelmann, J.J.; Jespersen, J.; Nybo, M.; Rasmussen, L.M.; Hansen, D.; Scholze, A. Randomized controlled trial of cholecalciferol supplementation in chronic kidney disease patients with hypovitaminosis D. Nephrol. Dial. Transplant. 2012, 27, 3523–3531. [Google Scholar] [CrossRef] [Green Version]
- Miskulin, D.C.; Majchrzak, K.; Tighiouart, H.; Muther, R.S.; Kapoian, T.; Johnson, D.S.; Weiner, D.E. Ergocalciferol Supplementation in Hemodialysis Patients With Vitamin D Deficiency: A Randomized Clinical Trial. J. Am. Soc. Nephrol. 2016, 27, 1801–1810. [Google Scholar] [CrossRef]
- Singer, R.F. Vitamin D in dialysis: Defining deficiency and rationale for supplementation. Semin. Dial. 2013, 26, 40–46. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | ALL | Mild | Severe | p Value * |
|---|---|---|---|---|
| Changes | Changes | |||
| N | 85 | 47 | 38 | |
| Men n (%) | 45 (52.94) | 27 (57.45) | 18 (47.37) | 0.35 |
| Age, years | 69.74 (13.19) | 70.23 (14.63) | 69.13 (11.33) | 0.71 |
| Body mass index, kg/m2 | 25.34 (4.79) | 25.21 (4.73) | 25.49 (4.92) | 0.79 |
| Blood group n (%) | ||||
| A | 36 (42.35) | 17 (36.17) | 19 (50.0) | 0.19 |
| B | 14 (16.47) | 9 (19.15) | 5 (13.16) | 0.46 |
| AB | 6 (7.05) | 2 (4.25) | 4 (10.53) | 0.26 |
| O | 29 (34.12) | 19 (40.43) | 10 (26.31) | 0.17 |
| Dialysis vintages, months median (IQR) | 38 (14–84) | 33 (14–85) | 46 (21–82) | 0.74 |
| Past kidney transplantation n (%) | 7 (8.23) | 5 (10.64) | 2 (5.26) | 0.37 |
| Hemodialysis dose per week, hours | 11.63 (1.59) | 11.50 (1.69) | 11.8 (1.47) | 0.39 |
| Hemodialysis access n (%) | ||||
| AVF/AVG | 29 (34.12) | 19 (40.42) | 10 (26.31) | 0.17 |
| Dialysis catheter | 56 (65.88) | 28 (59.57) | 28 (73.68) | 0.17 |
| Charlson comorbidity index | 7.64 (2.23) | 7.49 (2.22) | 7.82 (2.26) | 0.51 |
| Fragility index | 4.16 (1.36) | 4.02 (1.34) | 4.34 (1.38) | 0.28 |
| Comorbidities n (%) | ||||
| Arterial hypertension | 83 (97.65) | 47 (100) | 36 (94.74) | 0.44 |
| Diabetes | 45 (52.94) | 24 (51.06) | 21 (55.26) | 0.69 |
| Ischemic heart disease | 34 (40.0) | 18 (38.30) | 16 (42.10) | 0.72 |
| Congestive heart failure | 31 (36.47) | 14 (29.79) | 17 (44.74) | 0.15 |
| Malignancy | 7 (8.23) | 5 (10.64) | 2 (5.26) | 0.37 |
| Chronic pulmonary disease | 4 (4.71) | 3 (6.38) | 1 (2.63) | 0.42 |
| Chronic drug treatment n (%) | ||||
| Beta-blockers | 58 (68.23) | 32 (68.08) | 26 (68.42) | 0.97 |
| Active oral vitamin D | 57 (67.05) | 37 (78.72) | 20 (52.53) | 0.011 |
| Statins | 36 (42.35) | 19 (40.42) | 17 (44.74) | 0.69 |
| Calcium channel blockers | 27 (31.76) | 14 (29.79) | 13 (34.21) | 0.66 |
| LMWH between HD session days | 20 (23.53) | 12 (25.53) | 8 (21.05) | 0.63 |
| ACEI | 17 (20.00) | 5 (10.64) | 12 (31.58) | 0.02 |
| ARBs | 3 (3.53) | 2 (4.25) | 1 (2.63) | 0.69 |
| Oral anticoagulant | 5 (5.88) | 3 (6.38) | 2 (5.26) | 0.83 |
| Cinacalcet | 3 (3.53) | 1 (2.12) | 2 (5.26) | 0.44 |
| LMWH during dialysis | 54 (63.53) | 28 (59.57) | 26 (68.42) | 0.39 |
| UFH during dialysis | 31 (36.47) | 19 (40.43) | 12 (31.58) | 0.39 |
| Variable | ALL | Mild Changes | Severe Changes | p Value * |
|---|---|---|---|---|
| N Asymptomatic course n (%) Symptomatic course n (%) Fatigue Fever Shortness of breath Cough Chills Diarrhea Appetite loss Smell/taste loss Headache Joint pains Rhinorrhea Myalgia Sore throat Sleep disturbances Symptoms duration days | 85 25 (29.41) 60 (70.59) 38 (44.71) 34 (40.00) 27 (31.76) 26 (30.59) 12 (14.12) 12 (14.12) 6 (7.06) 2 (2.35) 4 (4.71) 4 (4.71) 2 (2.35) 3 (3.53) 2 (2.35) 1 (1.18) 2.2 (1.41) | 47 14 (29.79) 33 (70.21) 22 (46.81) 13 (27.66) 14 (29.79) 12 (25.53) 7 (14.89) 6 (12.77) 3 (6.38) 1 (2.13) 4 (8.51) 2 (4.25) 2 (4.25) 2 (4.25) 0 (0.0) 1 (2.13) 2.51 (3.58) | 38 11 (29.95) 27 (71.05) 16 (42.10) 21 (55.26) 13 (34.21) 14 (36.84) 5 (13.16) 6 (15.79) 3 (7.89) 1 (2.63) 0 (0.0) 2 (5.26) 0 (0.0) 1 (2.63) 2 (5.26) 0 (0.0) 1.8 (2.61) | 0.93 0.93 0.66 0.01 0.66 0.26 0.82 0.69 0.79 0.88 0.25 0.83 0.87 0.87 0.44 0.88 0.82 |
| Observations on admission Body temperature, °C Body temperature > 37.5 °C n (%) Finger oxygen saturation, % Finger oxygen saturation < 90% n (%) Systolic blood pressure, mmHg Diastolic blood pressure, mmHg Heart rate, beats/min | 36.92 (0.68) 17 (20) 93.47 (5.62) 17 (20) 140.76 (24.54) 79.27 (13.21) 80.81 (14.12) | 36.85 (0.61) 8 (17.02) 95.44 (3.14) 4 (8.5) 141.91 (23.86) 80.3 (13.12) 81.81 (14.33) | 37.0 (0.76) 9 (23.68) 90.87 (7.03) 13 (34.21) 139 (25.6) 77.97 (13.38) 79.74 (13.96) | 0.31 0.44 <0.001 0.003 0.64 0.43 0.56 |
| Laboratory values on admission Haemoglobin (g/dL; nr: 13.0–17.5) Leucocytes (×109 per L; nr: 3.5–9.5) Neutrophils (×109 per L; nr: 1.8–6.3) ** Lymphocytes (×109 per L; nr: 1.1–3.2) ** Lymphocytes < 1.1 × 109 Platelets (×109 per L; nr: 125.0–350.0) C-reactive protein (mg/L; nr: 0.0–5.0) ** Serum ferritin (ng/mL; nr: 21.0–274.7) ** ALAT (U/L; nr: 9.0–50.0) Prothrombin time (s; nr: 10.5–13.5) APTT (s; nr: 21.0–37.0) D-dimer (ng/mL; nr: 0–500) ** Arterial pO2, mmHg Arterial pO2 < 60 mmHg Arterial pCO2, mmHg | 10.75 (1.75) 6.13 (2.87) 3.72 (2.65–6.03) 0.87 (0.63–1.27) 49 (57.65) 192 (69.84) 53 (13.60–117.40) 1039.0 (678.2–2022.0) 21 (11–29) 13.58 (5.62) 43.03 (13.57) 1161.8 (685.89–1842.2) 67.04 (22.94) 12 (14.12) 34.13 (6.77) | 10.81 (1.71) 5.8 (2.69) 3.22 (2.38–5.06) 1.09 (0.76–1.46) 22 (46.81) 187.91 (64.68) 23.55 (6.9–95.0) 820.7 (680.45–1319) 22 (12–28) 13.35 (5.26) 42.98 (15.88) 946.65 (712.8–1501.4) 75.68 (15.95) 2 (4.25) 34.16 (4.69) | 10.66 (1.81) 6.52 (3.07) 4.26 (2.9–6.79) 0.72 (0.57–1.02) 27 (71.05) 197.08 (75.96) 93.4 (53–176.7) 1820 (678.2–2300) 20.5 (11–30) 13.87 (6.13) 43.09 (10.39) 1257.25 (646.5–1845.4) 60.99 (25.42) 10 (26.31) 34.11 (8.1) | 0.26 0.94 0.94 0.001 0.025 0.56 <0.001 0.03 0.31 0.72 0.97 0.64 0.02 0.004 0.98 |
| Variable | ALL | Mild Changes | Severe Changes | p Value * |
|---|---|---|---|---|
| N Type of lungs changes n (%) Unilateral infiltration Bilateral infiltration Ground-glass opacity (GGO) Consolidation Air bronchogram Linear opacities Crazy-paving pattern Pleural effusion Involved lung lobes n (%) Upper lobes Middle lobe Lower lobes | 85 12 (14.12) 68 (80) 63 (74.12) 35 (41.18) 14 (16.47) 24 (28.24) 53 (62.35) 34 (40) 74 (87.06) 55 (65.7) 80 (94.18) | 47 11 (23.40) 31 (65.96) 25 (53.19) 4 (8.5) 7 (14.89) 12 (25.53) 22 (46.81) 12 (25.53) 36 (76.60) 20 (42.55) 42 (89.36) | 38 1 (2.63) 37 (97.37) 38 (100) 31 (81.58) 7 (18.42) 12 (31.58) 31 (81.56) 22 (57.89) 38 (100) 35 (92.1) 38 (100) | 0.006 <0.001 <0.001 <0.001 0.66 0.001 0.001 0.002 0.006 <0.001 0.15 |
| Degree of lung involvement ** Total opacities—% lungs GGO—% lungs Consolidation—% lungs Total severity score (TSS)—points | 5 (1–22) 4 (1–17) 1 (3–5) 7 (4–11) | 1 (0–4) 1 (0–3) 0 (0–1) 5 (2–6) | 24 (10–38) 20 (10–31) 3 (1–9) 14 (10–16) | <0.001 <0.001 <0.001 <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tylicki, P.; Polewska, K.; Och, A.; Susmarska, A.; Puchalska-Reglińska, E.; Parczewska, A.; Biedunkiewicz, B.; Szabat, K.; Renke, M.; Tylicki, L.; et al. Angiotensin Converting Enzyme Inhibitors May Increase While Active Vitamin D May Decrease the Risk of Severe Pneumonia in SARS-CoV-2 Infected Patients with Chronic Kidney Disease on Maintenance Hemodialysis. Viruses 2022, 14, 451. https://doi.org/10.3390/v14030451
Tylicki P, Polewska K, Och A, Susmarska A, Puchalska-Reglińska E, Parczewska A, Biedunkiewicz B, Szabat K, Renke M, Tylicki L, et al. Angiotensin Converting Enzyme Inhibitors May Increase While Active Vitamin D May Decrease the Risk of Severe Pneumonia in SARS-CoV-2 Infected Patients with Chronic Kidney Disease on Maintenance Hemodialysis. Viruses. 2022; 14(3):451. https://doi.org/10.3390/v14030451
Chicago/Turabian StyleTylicki, Piotr, Karolina Polewska, Aleksander Och, Anna Susmarska, Ewelina Puchalska-Reglińska, Aleksandra Parczewska, Bogdan Biedunkiewicz, Krzysztof Szabat, Marcin Renke, Leszek Tylicki, and et al. 2022. "Angiotensin Converting Enzyme Inhibitors May Increase While Active Vitamin D May Decrease the Risk of Severe Pneumonia in SARS-CoV-2 Infected Patients with Chronic Kidney Disease on Maintenance Hemodialysis" Viruses 14, no. 3: 451. https://doi.org/10.3390/v14030451
APA StyleTylicki, P., Polewska, K., Och, A., Susmarska, A., Puchalska-Reglińska, E., Parczewska, A., Biedunkiewicz, B., Szabat, K., Renke, M., Tylicki, L., & Dębska-Ślizień, A. (2022). Angiotensin Converting Enzyme Inhibitors May Increase While Active Vitamin D May Decrease the Risk of Severe Pneumonia in SARS-CoV-2 Infected Patients with Chronic Kidney Disease on Maintenance Hemodialysis. Viruses, 14(3), 451. https://doi.org/10.3390/v14030451