
Prevalence of MCPyV, HPyV6, HPyV7 and TSPyV in Actinic Keratosis Biopsy Specimens

 , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. DNA Extraction
2.3. Qualitative HPyVs PCR
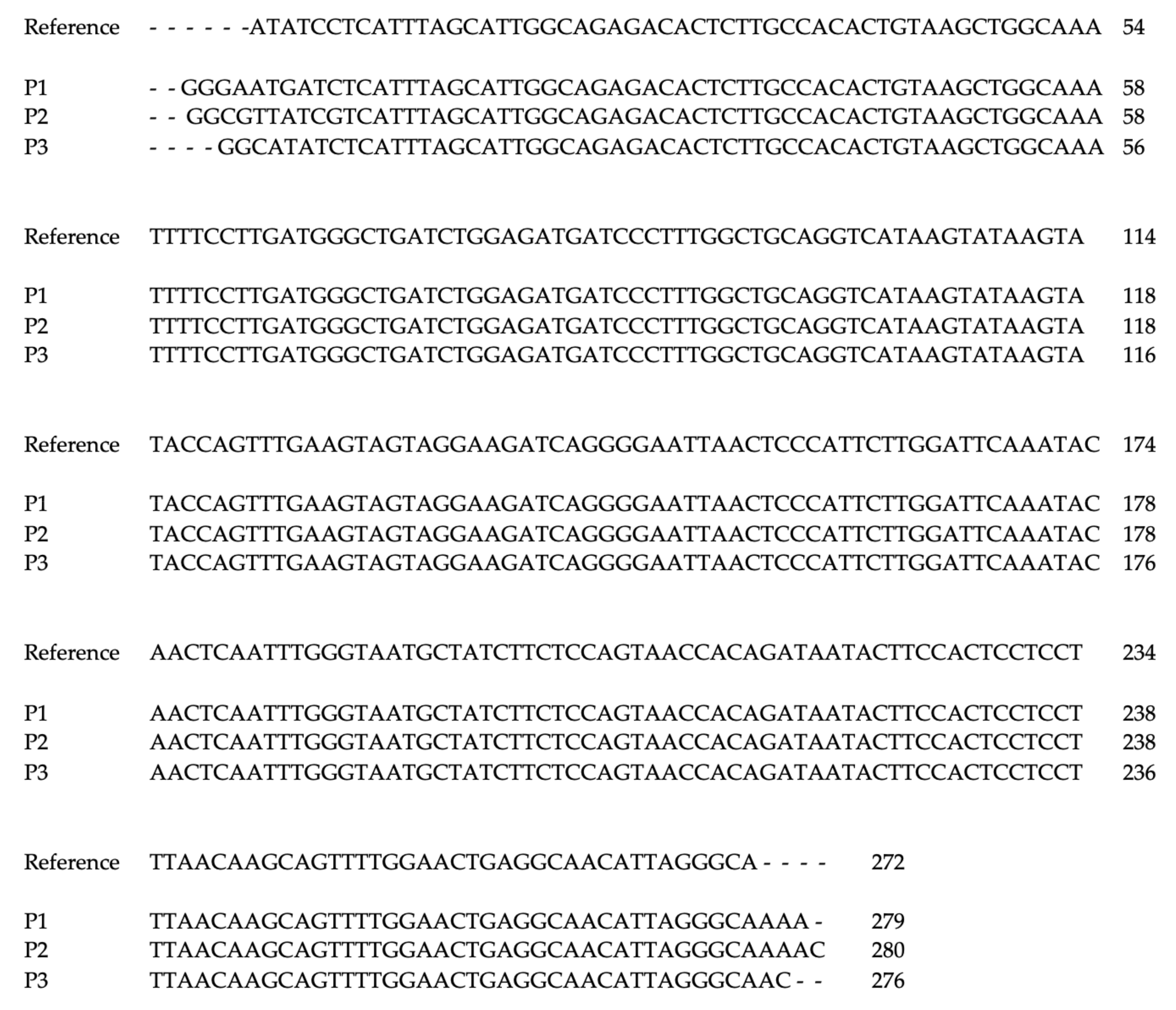
2.4. Viral DNA Sequencing and Sequence Alignment
2.5. Statistical Analysis
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moens, U.; Krumbholz, A.; Ehlers, B.; Zell, R.; Johne, R.; Calvignac-Spencer, S.; Lauber, C. Biology, evolution, and medical importance of polyomaviruses: An update. Infect. Genet. Evol. 2017, 54, 18–38. [Google Scholar] [CrossRef] [PubMed]
- Ciotti, M.; Prezioso, C.; Pietropaolo, V. An overview on human polyomaviruses biology and related diseases. Future Virol. 2019, 14, 487–501. [Google Scholar] [CrossRef]
- Kourieh, A.; Combes, J.D.; Tommasino, M.; Dalstein, V.; Clifford, G.M.; Lacau St Guily, J.; Clavel, C.; Franceschi, S.; Gheit, T.; For The Split Study Group. Prevalence and risk factors of human polyomavirus infections in non-malignant tonsils and gargles: The SPLIT study. J. Gen. Virol. 2018, 99, 1686–1698. [Google Scholar] [CrossRef] [PubMed]
- Sheu, J.C.; Tran, J.; Rady, P.L.; Dao, H., Jr.; Tyring, S.K.; Nguyen, H.P. Polyomaviruses of the skin: Integrating molecular and clinical advances in an emerging class of viruses. Br. J. Dermatol. 2019, 180, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Fava, P.; Merlino, C.; Novelli, M.; Ponti, R.; Galliano, I.; Montanari, P.; Tovo, P.A.; Fierro, M.T.; Bergallo, M. HPyV6, HPyV7 and TSPyV DNA sequences detection in skin disease patients and healthy subjects. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 624–627. [Google Scholar] [CrossRef]
- Hashida, Y.; Higuchi, T.; Matsuzaki, S.; Nakajima, K.; Sano, S.; Daibata, M. Prevalence and Genetic Variability of Human Polyomaviruses 6 and 7 in Healthy Skin Among Asymptomatic Individuals. J. Infect. Dis. 2018, 217, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Bopp, L.; Wieland, U.; Hellmich, M.; Kreuter, A.; Pfister, H.; Silling, S. Natural History of Cutaneous Human Polyomavirus Infection in Healthy Individuals. Front. Microbiol. 2021, 12, 740947. [Google Scholar] [CrossRef]
- Mishra, N.; Pereira, M.; Rhodes, R.H.; An, P.; Pipas, J.M.; Jain, K.; Kapoor, A.; Briese, T.; Faust, P.L.; Lipkin, W.I. Identification of a novel polyomavirus in a pancreatic transplant recipient with retinal blindness and vasculitic myopathy. J. Infect. Dis. 2014, 210, 1595–1599. [Google Scholar] [CrossRef] [Green Version]
- Feng, H.; Shuda, M.; Chang, Y.; Moore, P.S. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008, 319, 1096–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietropaolo, V.; Prezioso, C.; Moens, U. Merkel Cell Polyomavirus and Merkel Cell Carcinoma. Cancers 2020, 12, 1774. [Google Scholar] [CrossRef]
- Ho, J.; Jedrych, J.J.; Feng, H.; Natalie, A.A.; Grandinetti, L.; Mirvish, E.; Crespo, M.M.; Yadav, D.; Fasanella, K.E.; Proksell, S.; et al. Human polyomavirus 7-associated pruritic rash and viremia in transplant recipients. J. Infect. Dis. 2015, 211, 1560–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, K.D.; Lee, E.E.; Yue, Y.; Stork, J.; Pock, L.; North, J.P.; Vandergriff, T.; Cockerell, C.; Hosler, G.A.; Pastrana, D.V.; et al. Human polyomavirus 6 and 7 are associated with pruritic and dyskeratotic dermatoses. J. Am. Acad. Dermatol. 2017, 76, 932–940.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.D.B.; Erdag, G.; Cuda, J.D.; Rangwala, S.; Girardi, N.; Bibee, K.; Orens, J.B.; Prono, M.D.; Toptan, T.; Loss, M.J. Treatment of human polyomavirus-7-associated rash and pruritus with topical cidofovir in a lung transplant patient: Case report and literature review. Transpl. Infect. Dis. 2018, 20, e12793. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, R.K.; Pastrana, D.V.; Starrett, G.J.; Sapio, M.R.; Hill, N.T.; Jo, J.H.; Lee, C.R.; Iadarola, M.J.; Buck, C.B.; Kong, H.H.; et al. Host-Pathogen Interactions in Human Polyomavirus 7—Associated Pruritic Skin Eruption. J. Investig. Dermatol. 2021, 141, 1344–1348.e8. [Google Scholar] [CrossRef] [PubMed]
- Kwan, K.; Sears, S.; Callen, J.; Rady, P.; Tyring, S.; Bahrami, S.; Huelsman, M.; Malone, J. Keratotic spines in a patient with pruritic and dyskeratotic dermatosis: A new clinical finding. JAAD Case Rep. 2020, 7, 103–106. [Google Scholar] [CrossRef] [PubMed]
- van der Meijden, E.; Janssens, R.W.; Lauber, C.; Bouwes Bavinck, J.N.; Gorbalenya, A.E.; Feltkamp, M.C. Discovery of a new human polyomavirus associated with trichodysplasia spinulosa in an immunocompromized patient. PLoS Pathog. 2010, 6, e1001024. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, K.D.; Chamseddin, B.H.; Cockerell, C.J.; Wang, R.C. The Biology and Clinical Features of Cutaneous Polyomaviruses. J. Investig. Dermatol. 2019, 139, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Mazel-Sanchez, B.; Yildiz, S.; Schmolke, M. Ménage à trois: Virus, Host, and Microbiota in Experimental Infection Models. Trends Microbiol. 2019, 27, 440–452. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Keinonen, A.; Koskenmies, S.; Pitkänen, S.; Fyhrquist, N.; Sadeghi, M.; Mäkisalo, H.; Söderlund-Venermo, M.; Hedman, K. Occurrence of newly discovered human polyomaviruses in skin of liver transplant recipients and their relation with squamous cell carcinoma in situ and actinic keratosis—A single-center cohort study. Transpl. Int. 2019, 32, 516–522. [Google Scholar] [CrossRef]
- Campione, E.; Ventura, A.; Diluvio, L.; Mazzeo, M.; Mazzilli, S.; Garofalo, V.; di Prete, M.; Bianchi, L. Current developments in pharmacotherapy for actinic keratosis. Expert. Opin. Pharmacother. 2018, 19, 1693–1704. [Google Scholar] [CrossRef]
- Frazer, I.H. The actinic keratosis virome: Can we prevent squamous cell carcinoma with a vaccine? Curr. Probl. Dermatol. 2015, 46, 28–35. [Google Scholar]
- Saiki, R.K.; Bugawan, T.L.; Horn, G.T.; Mullis, K.B.; Erlich, H.A. Analysis of enzymatically amplified beta-globin and HLA-DQ alpha DNA with allele-specific oligonucleotide probes. Nature 1986, 324, 163–166. [Google Scholar]
- Prezioso, C.; Bianchi, M.; Obregon, F.; Ciotti, M.; Sarmati, L.; Andreoni, M.; Palamara, A.T.; Pascarella, S.; Moens, U.; Pietropaolo, V. Structural Analysis of Merkel Cell Polyomavirus (MCPyV) Viral Capsid Protein 1 (VP1) in HIV-1 Infected Individuals. Int. J. Mol. Sci. 2020, 21, 7998. [Google Scholar] [CrossRef] [PubMed]
- Shikova, E.; Emin, D.; Alexandrova, D.; Shindov, M.; Kumanova, A.; Lekov, A.; Moens, U. Detection of Merkel Cell Polyomavirus in Respiratory Tract Specimens. Intervirology 2017, 60, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Prezioso, C.; Van Ghelue, M.; Moens, U.; Pietropaolo, V. HPyV6 and HPyV7 in urine from immunocompromised patients. Virol. J. 2021, 18, 24. [Google Scholar] [CrossRef]
- Rouanet, J.; Aubin, F.; Gaboriaud, P.; Berthon, P.; Feltkamp, M.C.; Bessenay, L.; Touzé, A.; Nicol, J.T.; Franck, F.; D’Incan, M. Trichodysplasia spinulosa: A polyomavirus infection specifically targeting follicular keratinocytes in immunocompromised patients. Br. J. Dermatol. 2016, 174, 629–632. [Google Scholar] [CrossRef] [PubMed]
- ClustalW2–Multiple Sequence Alignment. Available online: http://www.ebi.ac.uk/Tools/msa/clustalw2/ (accessed on 17 January 2022).
- Chen, T.; Mattila, P.S.; Jartti, T.; Ruuskanen, O.; Söderlund-Venermo, M.; Hedman, K. Seroepidemiology of the newly found trichodysplasia spinulosa-associated polyomavirus. J. Infect. Dis. 2011, 204, 1523–1526. [Google Scholar] [CrossRef] [Green Version]
- Scola, N.; Wieland, J.; Silling, S.; Altmeyer, P.; Stucker, M.; Kreuter, A. Prevalence of human polyomaviruses in common and rare types of non-Merkel cell carcinoma skin cancer. Brit. J. Dermatol. 2012, 167, 1315–1320. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Patients | Sex | Age | Diagnosis | Lesion Biopsy | Non-Lesion Biopsy |
|---|---|---|---|---|---|
| 1 | M | 70 | AK | + | + |
| 2 | M | 83 | AK | + | + |
| 3 | M | 80 | AK | + | − |
| 4 | M | 81 | AK | + | + |
| 5 | M | 82 | AK | + | + |
| 6 | M | 75 | AK | + | + |
| 7 | M | 86 | AK | + | + |
| 8 | M | 78 | AK | + | + |
| 9 | M | 72 | AK | + | + |
| Samples | n | MCPyV | HPyV6 | HPyV7 | TSPyV |
|---|---|---|---|---|---|
| Lesion biopsy | 9 | 9 (100%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Non-lesion biopsy | 8 | 5 (62.5%) | 1 (12.5%) | 0 (0%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prezioso, C.; Brazzini, G.; Passerini, S.; Di Fabio, C.; Cosio, T.; Bernardini, S.; Campione, E.; Moens, U.; Pietropaolo, V.; Ciotti, M. Prevalence of MCPyV, HPyV6, HPyV7 and TSPyV in Actinic Keratosis Biopsy Specimens. Viruses 2022, 14, 427. https://doi.org/10.3390/v14020427
Prezioso C, Brazzini G, Passerini S, Di Fabio C, Cosio T, Bernardini S, Campione E, Moens U, Pietropaolo V, Ciotti M. Prevalence of MCPyV, HPyV6, HPyV7 and TSPyV in Actinic Keratosis Biopsy Specimens. Viruses. 2022; 14(2):427. https://doi.org/10.3390/v14020427
Chicago/Turabian StylePrezioso, Carla, Gabriele Brazzini, Sara Passerini, Carlotta Di Fabio, Terenzio Cosio, Sergio Bernardini, Elena Campione, Ugo Moens, Valeria Pietropaolo, and Marco Ciotti. 2022. "Prevalence of MCPyV, HPyV6, HPyV7 and TSPyV in Actinic Keratosis Biopsy Specimens" Viruses 14, no. 2: 427. https://doi.org/10.3390/v14020427
APA StylePrezioso, C., Brazzini, G., Passerini, S., Di Fabio, C., Cosio, T., Bernardini, S., Campione, E., Moens, U., Pietropaolo, V., & Ciotti, M. (2022). Prevalence of MCPyV, HPyV6, HPyV7 and TSPyV in Actinic Keratosis Biopsy Specimens. Viruses, 14(2), 427. https://doi.org/10.3390/v14020427