

Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
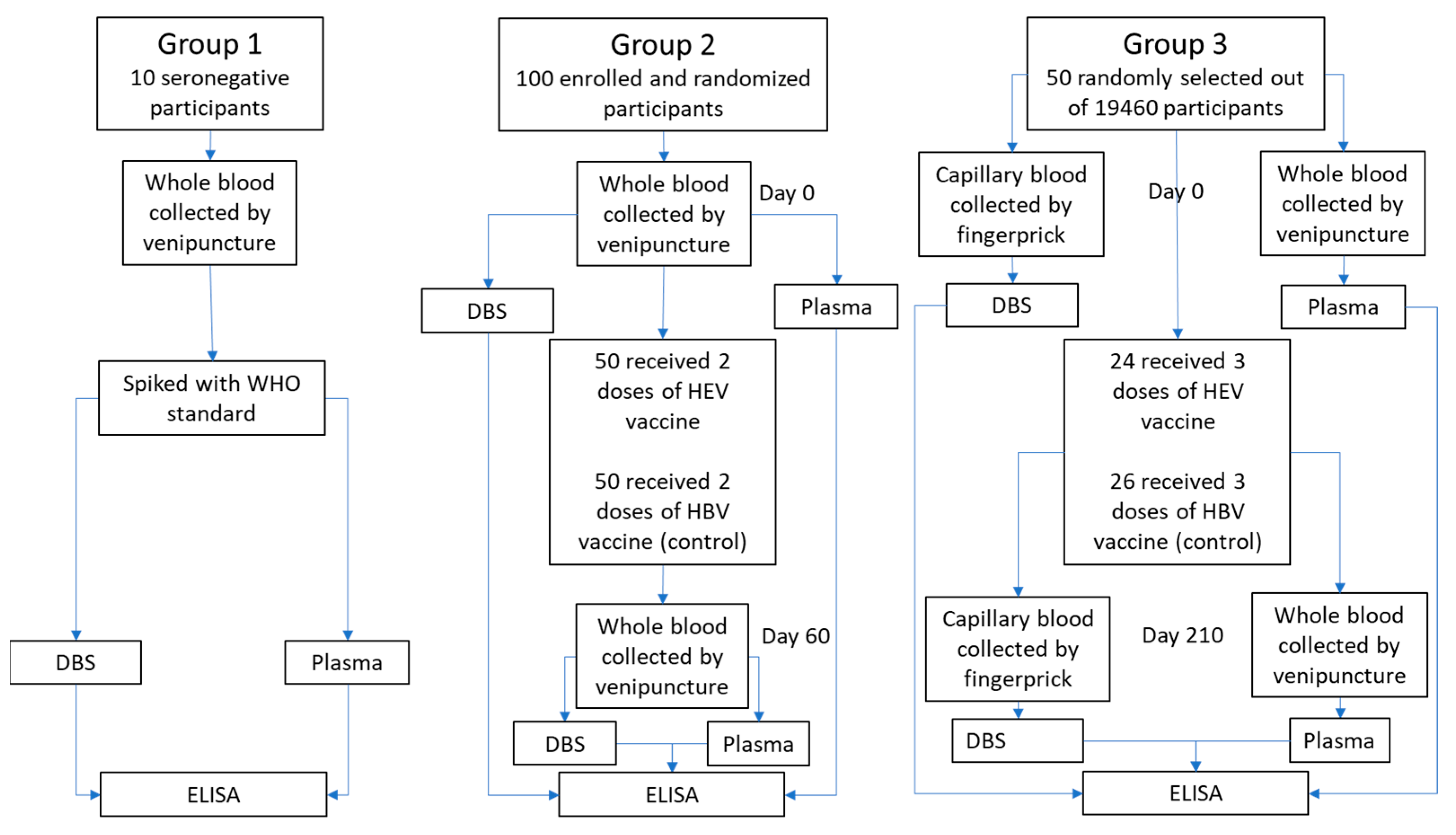
2.1. Sample Material
2.2. Specimen Preparation
2.3. DBS Extraction
2.4. Serology
2.5. Optimization (Dilution and Cut-Off)
2.6. Precision, Linearity and Stability (Group 1)
2.7. Clinical Performance (Groups 2 and 3)
3. Results
3.1. Optimization of ELISA Assay for DBS
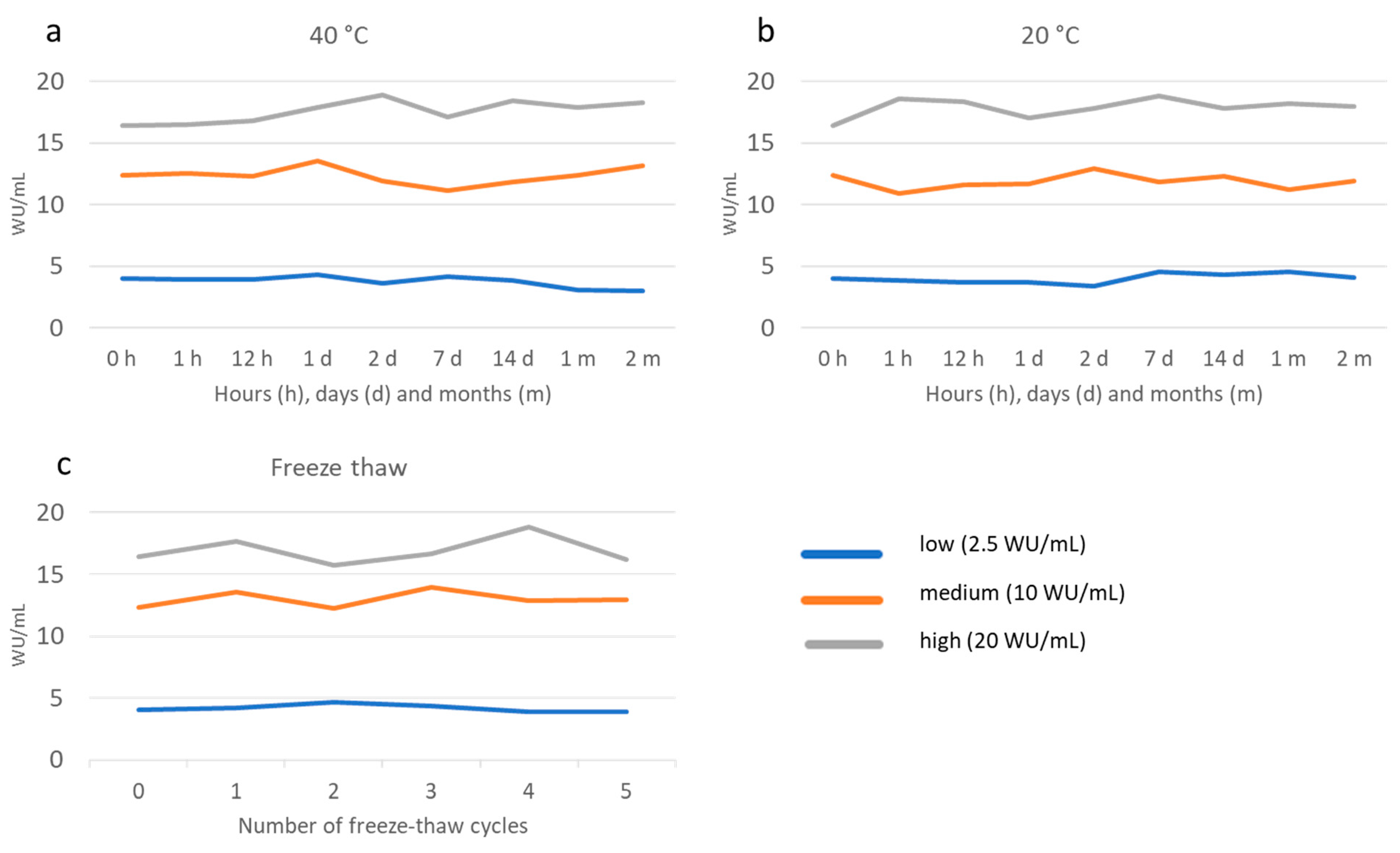
3.2. Precision, Linearity and Stability
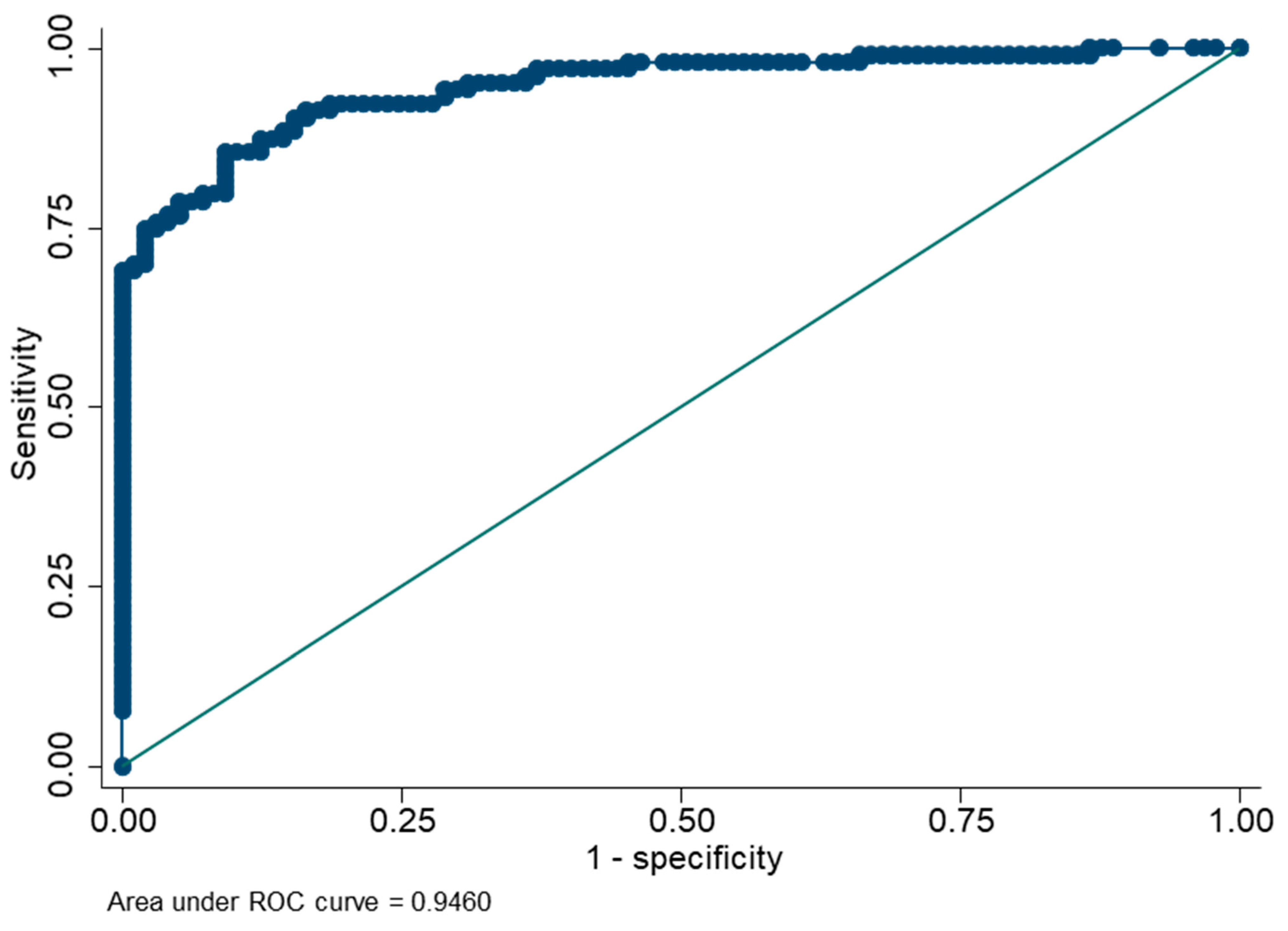
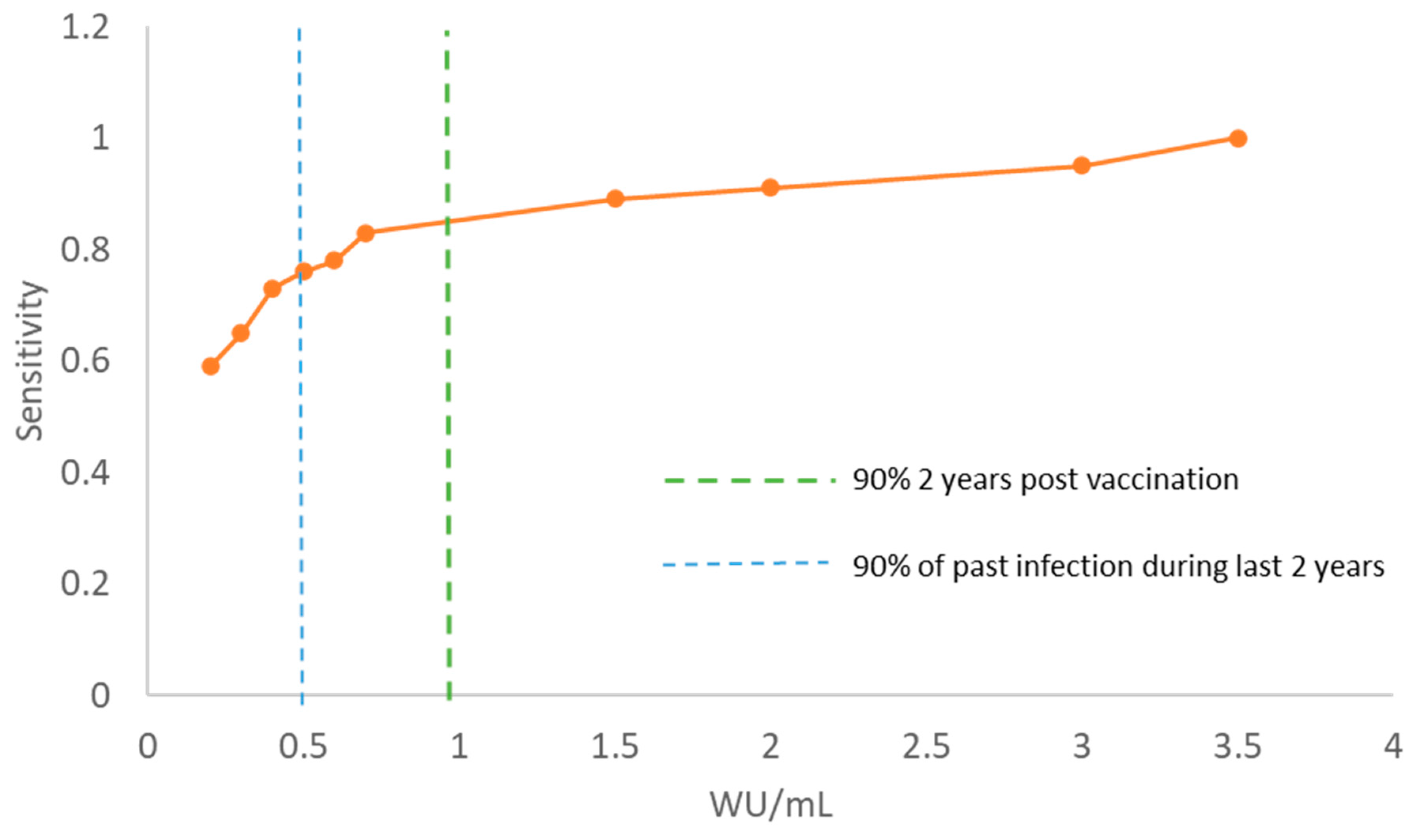
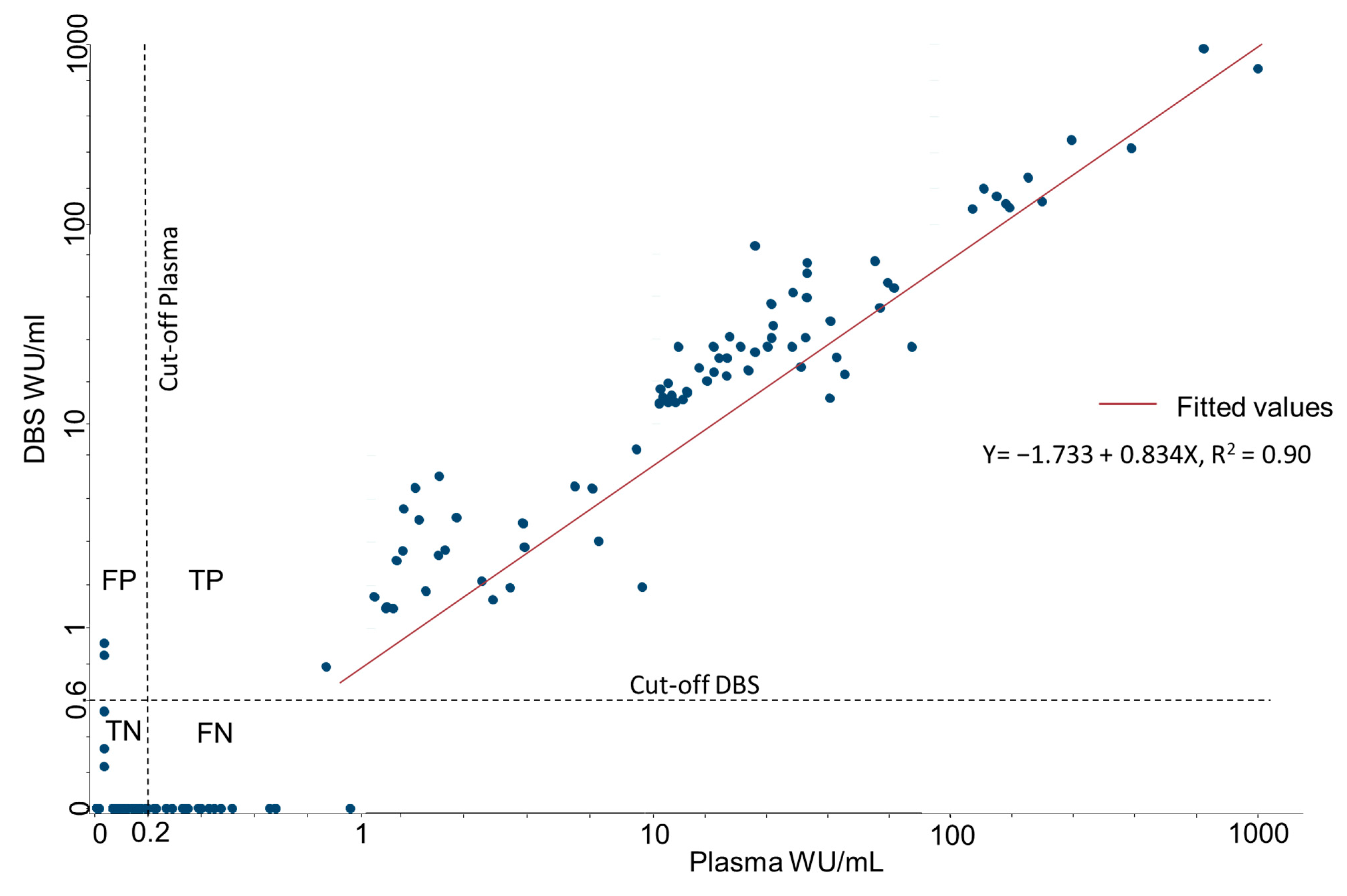
3.3. Clinical Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nimgaonkar, I.; Ding, Q.; Schwartz, R.E.; Ploss, A. Hepatitis E virus: Advances and challenges. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Hoa, T.N.; Munshi, S.U.; Ngoc, K.N.; Ngoc, C.L.; Thanh TT, T.; Akther, T.; Tabassum, S.; Parvin, N.; Baker, S.; Rahman, M. A tightly clustered hepatitis E virus genotype 1a is associated with endemic and outbreak infections in Bangladesh. PLoS ONE 2021, 16, e0255054. [Google Scholar] [CrossRef] [PubMed]
- Group, H.E.V.W. Recommendations of HEV Working Group on the Use of Hepatitis E Vaccine. 2014. Available online: http://www.who.int/immunization/sage/meetings/2014/october/3_Hep_E_vacc_WG_SAGE_Recs_final_1Oct2014.pdf (accessed on 1 October 2014).
- Azman, A.S.; Ciglenecki, I.; Wamala, J.F.; Lynch, J.; Aggarwal, R.; Rahman, M.; Wong, S.; Serafini, M.; Moussa, A.M.; Dalton, H.R.; et al. Hepatitis E should be considered a neglected tropical disease. PLoS Negl. Trop. Dis. 2019, 13, e0007453. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Deeks, S.L.; Hatchette, T.F.; Crowcroft, N.S. The role of seroepidemiology in the comprehensive surveillance of vaccine-preventable diseases. Can. Med. Assoc. J. 2012, 184, E70–E76. [Google Scholar] [CrossRef] [PubMed]
- Malsagova, K.; Kopylov, A.; Stepanov, A.; Butkova, T.; Izotov, A.; Kaysheva, A. Dried Blood Spot in Laboratory: Directions and Prospects. Diagnostics 2020, 10, 248. [Google Scholar] [CrossRef] [PubMed]
- Amini, F.; Auma, E.; Hsia, Y.; Bilton, S.; Hall, T.; Ramkhelawon, L.; Heath, P.T.; Le Doare, K. Reliability of dried blood spot (DBS) cards in antibody measurement: A systematic review. PLoS ONE 2021, 16, e0248218. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, B.; Taylor, R.; Dawkins, C.; Banks, T.; Watson, N.; Sundaram, A.; Ewing, D.; Danko, J.R. The use of dried blood spot cards to assess serologic responses of individuals vaccinated against measles, hepatitis A, tetanus, influenza and varicella zoster. PLoS ONE 2022, 17, e0265813. [Google Scholar] [CrossRef] [PubMed]
- Sultana, R.; Bhuiyan, T.R.; Sathi, A.S.; Sharmin, S.; Yeasmin, S.; Uddin, M.I.; Bhuiyan, S.; Mannoor, K.; Karim, M.M.; Zaman, K.; et al. Developing and validating a modified enzyme linked immunosorbent assay method for detecting HEV IgG antibody from dried blood spot (DBS) samples in endemic settings. Microbes Infect. 2022, 24, 104890. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, Q.; Xia, N. Prophylactic Hepatitis E Vaccine. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2016; Volume 948, pp. 223–246. [Google Scholar]
- Zaman, K.; Dudman, S.; Stene-Johansen, K.; Qadri, F.; Yunus; Sandbu, S.; Gurley, E.S.; Overbo, J.; Julin, C.H.; Dembinski, J.L.; et al. HEV study protocol: Design of a cluster-randomised, blinded trial to assess the safety, immunogenicity and effectiveness of the hepatitis E vaccine HEV 239 (Hecolin) in women of childbearing age in rural Bangladesh. BMJ Open 2020, 10, e033702. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.M.; Flores, S.R.; De Jesús, V.R. Influence of Hematocrit and Total-Spot Volume on Performance Characteristics of Dried Blood Spots for Newborn Screening. Int. J. Neonatal Screen. 2015, 1, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Bendall, R.; Ellis, V.; Ijaz, S.; Ali, R.; Dalton, H. A comparison of two commercially available anti-HEV IgG kits and a re-evaluation of anti-HEV IgG seroprevalence data in developed countries. J. Med. Virol. 2010, 82, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, P.G.; Dunn, J.R. The five-parameter logistic: A characterization and comparison with the four-parameter logistic. Anal. Biochem. 2005, 343, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Nicholas Cox, N.J.; Steichen, T. CONCORD: Stata module for concordance correlation. In Statistical Software Components S404501; Boston College Department of Economics: Newton, MA, USA, 2007. [Google Scholar]
- Kodani, M.; Kamili, N.A.; Tejada-Strop, A.; Poe, A.; Denniston, M.M.; Drobeniuc, J.; Kamili, S. Variability in the performance characteristics of IgG anti-HEV assays and its impact on reliability of seroprevalence rates of hepatitis E. J. Med. Virol. 2017, 89, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- De Kesel, P.M.; Sadones, N.; Capiau, S.; Lambert, W.E.; Stove, C.P. Hemato-critical issues in quantitative analysis of dried blood spots: Challenges and solutions. Bioanalysis 2013, 5, 2023–2041. [Google Scholar] [CrossRef] [PubMed]
- Moat, S.J.; Zelek, W.M.; Carne, E.; Ponsford, M.J.; Bramhall, K.; Jones, S.; El-Shanawany, T.; Wise, M.P.; Thomas, A.; George, C.; et al. Development of a high-throughput SARS-CoV-2 antibody testing pathway using dried blood spot specimens. Ann. Clin. Biochem. 2021, 58, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Colson, K.; Potter, A.; Conde-Glez, C.; Hernandez, B.; Ríos-Zertuche, D.; Zúñiga-Brenes, P.; Collaborators, S.; Iriarte, E.; Mokdad, A.H. Use of a commercial ELISA for the detection of measles-specific immunoglobulin G (IgG) in dried blood spots collected from children living in low-resource settings. J. Med. Virol. 2015, 87, 1491–1499. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DBS | Dilution Factor | |||||
|---|---|---|---|---|---|---|
| Undiluted | 1.50 | 3 | 24 | 48 | ||
| 1 | WU/mL | 30.7 | 19.4 | 10.6 | 1.0 | 0.6 |
| % Expected value | 102 | 97 | 106 | 79 | 93 | |
| 2 | WU/mL | 27.3 | 21.5 | 9.6 | 1.6 | 0.9 |
| % Expected value | 91 | 107 | 96 | 125 | 137 | |
| Mean | % Expected value | 97 | 102 | 101 | 102 | 115 |
| Plasma | ||||||
|---|---|---|---|---|---|---|
| Group 2 | Group 3 | Group 2 + 3 | ||||
| DBS | Positive | Negative | Positive | Negative | Positive | Negative |
| Total | ||||||
| Positive | 84 | 3 | 41 | 2 | 125 | 5 |
| Negative | 16 | 97 | 13 | 44 | 29 | 141 |
| Unvaccinated | ||||||
| Positive | 34 | 3 | 16 | 2 | 50 | 5 |
| Negative | 16 | 97 | 13 | 44 | 29 | 141 |
| Vaccinated | ||||||
| Positive | 50 | 0 | 25 | 0 | 75 | 0 |
| Negative | 0 | 0 | 0 | 0 | 0 | 0 |
| Group 2 | Group 3 | Group 2 + 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Vac | Unvac | Total | Vac | Unvac | Total | Vac | Unvac | Total | |
| Sensitivity (%) | 100 | 68 | 84 | 100 | 55 | 76 | 100 | 63 | 81 |
| Specificity (%) | 100 | 97 | 97 | 100 | 96 | 96 | 100 | 97 | 97 |
| PPV | 1.00 | 0.92 | 0.97 | 1.00 | 0.89 | 0.95 | 1.00 | 0.91 | 0.96 |
| NPV | 1.00 | 0.86 | 0.86 | 1.00 | 0.77 | 0.77 | 1.00 | 0.83 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Øverbø, J.; Aziz, A.; Zaman, K.; Julin, C.H.; Qadri, F.; Stene-Johansen, K.; Biswas, R.; Islam, S.; Bhuiyan, T.R.; Haque, W.; et al. Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting. Viruses 2022, 14, 2525. https://doi.org/10.3390/v14112525
Øverbø J, Aziz A, Zaman K, Julin CH, Qadri F, Stene-Johansen K, Biswas R, Islam S, Bhuiyan TR, Haque W, et al. Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting. Viruses. 2022; 14(11):2525. https://doi.org/10.3390/v14112525
Chicago/Turabian StyleØverbø, Joakim, Asma Aziz, K. Zaman, Cathinka Halle Julin, Firdausi Qadri, Kathrine Stene-Johansen, Rajib Biswas, Shaumik Islam, Taufiqur Rahman Bhuiyan, Warda Haque, and et al. 2022. "Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting" Viruses 14, no. 11: 2525. https://doi.org/10.3390/v14112525
APA StyleØverbø, J., Aziz, A., Zaman, K., Julin, C. H., Qadri, F., Stene-Johansen, K., Biswas, R., Islam, S., Bhuiyan, T. R., Haque, W., Sandbu, S., Dembinski, J. L., & Dudman, S. (2022). Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting. Viruses, 14(11), 2525. https://doi.org/10.3390/v14112525