

Higher Risk of Tumor Recurrence in NASH-Related Hepatocellular Carcinoma Following Curative Resection
 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Outcome Measurement
2.2. Diagnosis of Liver Diseases
2.3. Clinical and Histopathological Characteristics
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
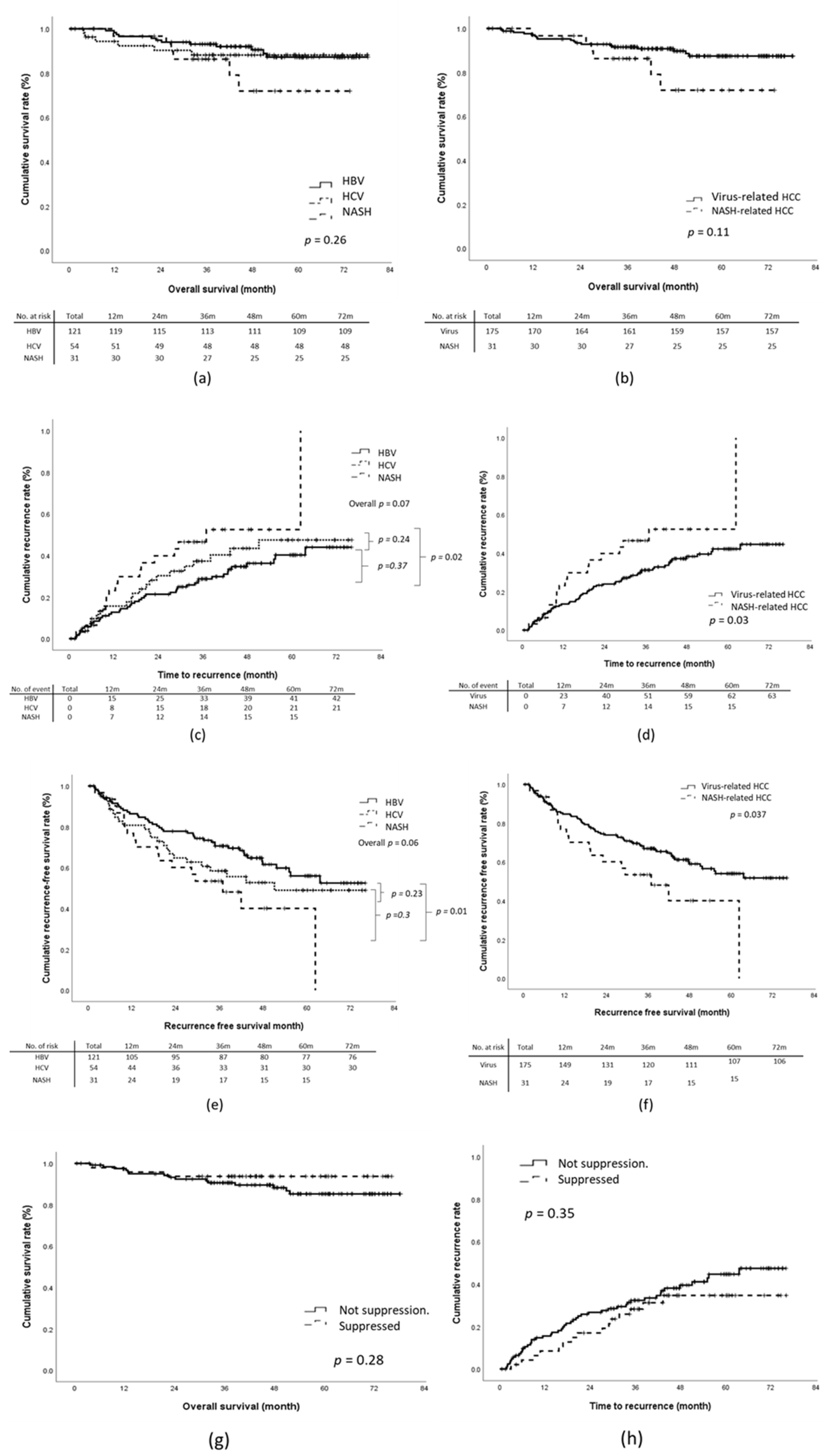
3.2. OS Analysis
3.3. Recurrence of HCC after Curative Resection
3.4. Effect of Antiviral Treatment on Outcomes
3.5. Propensity-Score-Matching Analysis of NASH-Related and HBV-Related HCC Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia-Pacific region. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Cheung, R.; Ahmed, A. Nonalcoholic steatohepatitis is the most rapidly growing indication for liver transplantation in patients with hepatocellular carcinoma in the U.S. Hepatology 2014, 59, 2188–2195. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Henry, L. Contribution of Alcoholic and Nonalcoholic Fatty Liver Disease to the Burden of Liver-Related Morbidity and Mortality. Gastroenterology 2016, 150, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C.H.; Jin, Y.J.; Lee, J.W. Nonalcoholic fatty liver disease-associated hepatocellular carcinoma in a hepatitis B virus-endemic area. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Piscaglia, F.; Svegliati-Baroni, G.; Barchetti, A.; Pecorelli, A.; Marinelli, S.; Tiribelli, C.; Bellentani, S.; Group, H.-N.I.S. Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: A multicenter prospective study. Hepatology 2016, 63, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Singal, A.G.; Kono, Y.; Tan, D.J.H.; El-Serag, H.B.; Loomba, R. Changing global epidemiology of liver cancer from 2010 to 2019: NASH is the fastest growing cause of liver cancer. Cell Metab. 2022, 34, 969–977.e2. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.J.H.; Ng, C.H.; Lin, S.Y.; Pan, X.H.; Tay, P.; Lim, W.H.; Teng, M.; Syn, N.; Lim, G.; Yong, J.N.; et al. Clinical characteristics, surveillance, treatment allocation, and outcomes of non-alcoholic fatty liver disease-related hepatocellular carcinoma: A systematic review and meta-analysis. Lancet Oncol. 2022, 23, 521–530. [Google Scholar] [CrossRef]
- Lee, Y.T.; Wang, J.J.; Luu, M.; Tseng, H.R.; Rich, N.E.; Lu, S.C.; Nissen, N.N.; Noureddin, M.; Singal, A.G.; Yang, J.D. State-Level HCC Incidence and Association With Obesity and Physical Activity in the United States. Hepatology 2021, 74, 1384–1394. [Google Scholar] [CrossRef]
- Yang, J.D.; Ahmed, F.; Mara, K.C.; Addissie, B.D.; Allen, A.M.; Gores, G.J.; Roberts, L.R. Diabetes Is Associated With Increased Risk of Hepatocellular Carcinoma in Patients With Cirrhosis From Nonalcoholic Fatty Liver Disease. Hepatology 2020, 71, 907–916. [Google Scholar] [CrossRef]
- Nakagawa, H.; Hayata, Y.; Kawamura, S.; Yamada, T.; Fujiwara, N.; Koike, K. Lipid Metabolic Reprogramming in Hepatocellular Carcinoma. Cancers 2018, 10, 447. [Google Scholar] [CrossRef]
- Sadler, E.M.; Mehta, N.; Bhat, M.; Ghanekar, A.; Greig, P.D.; Grant, D.R.; Yao, F.; Sapisochin, G. Liver Transplantation for NASH-Related Hepatocellular Carcinoma Versus Non-NASH Etiologies of Hepatocellular Carcinoma. Transplantation 2018, 102, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.K.; Steel, J.L.; Chen, H.W.; DeMateo, D.J.; Cardinal, J.; Behari, J.; Humar, A.; Marsh, J.W.; Geller, D.A.; Tsung, A. Outcomes of curative treatment for hepatocellular cancer in nonalcoholic steatohepatitis versus hepatitis C and alcoholic liver disease. Hepatology 2012, 55, 1809–1819. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Hu, L.Y.; Li, Z.L.; Liu, K.; Wu, H.; Xing, H.; Lau, W.Y.; Pawlik, T.M.; Zeng, Y.Y.; Zhou, Y.H.; et al. Liver Resection for Hepatocellular Carcinoma in Non-alcoholic Fatty Liver Disease: A Multicenter Propensity Matching Analysis with HBV-HCC. J. Gastrointest. Surg. 2020, 24, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Weinmann, A.; Alt, Y.; Koch, S.; Nelles, C.; Duber, C.; Lang, H.; Otto, G.; Zimmermann, T.; Marquardt, J.U.; Galle, P.R.; et al. Treatment and survival of non-alcoholic steatohepatitis associated hepatocellular carcinoma. BMC Cancer 2015, 15, 210. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Ariizumi, S.I.; Nakano, M.; Yamamoto, M. Diabetes Mellitus and/or Nonalcoholic Steatohepatitis-related Hepatocellular Carcinoma Showed Favorable Surgical Outcomes After Hepatectomy. Anticancer Res. 2019, 39, 5639–5643. [Google Scholar] [CrossRef]
- Choi, H.S.J.; Brouwer, W.P.; Zanjir, W.M.R.; de Man, R.A.; Feld, J.J.; Hansen, B.E.; Janssen, H.L.A.; Patel, K. Nonalcoholic Steatohepatitis Is Associated With Liver-Related Outcomes and All-Cause Mortality in Chronic Hepatitis B. Hepatology 2020, 71, 539–548. [Google Scholar] [CrossRef]
- Nishibatake Kinoshita, M.; Minami, T.; Tateishi, R.; Wake, T.; Nakagomi, R.; Fujiwara, N.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; et al. Impact of direct-acting antivirals on early recurrence of HCV-related HCC: Comparison with interferon-based therapy. J. Hepatol. 2019, 70, 78–86. [Google Scholar] [CrossRef]
- Sapena, V.; Enea, M.; Torres, F.; Celsa, C.; Rios, J.; Rizzo, G.E.M.; Nahon, P.; Marino, Z.; Tateishi, R.; Minami, T.; et al. Hepatocellular carcinoma recurrence after direct-acting antiviral therapy: An individual patient data meta-analysis. Gut 2022, 71, 593–604. [Google Scholar] [CrossRef]
- Ikeda, K.; Kawamura, Y.; Kobayashi, M.; Kominami, Y.; Fujiyama, S.; Sezaki, H.; Hosaka, T.; Akuta, N.; Saitoh, S.; Suzuki, F.; et al. Direct-Acting Antivirals Decreased Tumor Recurrence After Initial Treatment of Hepatitis C Virus-Related Hepatocellular Carcinoma. Dig. Dis. Sci. 2017, 62, 2932–2942. [Google Scholar] [CrossRef]
- Hannah, W.N., Jr.; Harrison, S.A. Effect of Weight Loss, Diet, Exercise, and Bariatric Surgery on Nonalcoholic Fatty Liver Disease. Clin. Liver Dis. 2016, 20, 339–350. [Google Scholar] [CrossRef]
- Romero-Gomez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M.; Neuschwander-Tetri, B.A.; Bacon, B.R. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Nonalcoholic Steatohepatitis Clinical Research, N. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection-A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Bootstrap model selection had similar performance for selecting authentic and noise variables compared to backward variable elimination: A simulation study. J. Clin. Epidemiol. 2008, 61, 1009–1017.e1. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J. Clin. Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Choi, J.; Jo, C.; Lim, Y.S. Tenofovir Versus Entecavir on Recurrence of Hepatitis B Virus-Related Hepatocellular Carcinoma After Surgical Resection. Hepatology 2021, 73, 661–673. [Google Scholar] [CrossRef]
- Famularo, S.; Piardi, T.; Molfino, S.; Di Martino, M.; Ferrari, C.; Ielpo, B.; Diago, M.V.; Giani, A.; Griseri, G.; Teres, L.B.; et al. Factors Affecting Local and Intra Hepatic Distant Recurrence After Surgery for Hcc: An Alternative Perspective on Microvascular Invasion and Satellitosis-A Western European Multicentre Study. J. Gastrointest. Surg. 2021, 25, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Yamada, T.; Tanaka, H.; Ohigashi, H.; Eguchi, H.; Yano, M.; Ishikawa, O.; Imaoka, S. Risk of recurrence in a long-term follow-up after surgery in 417 patients with hepatitis B- or hepatitis C-related hepatocellular carcinoma. Ann. Surg. 2006, 244, 771–780. [Google Scholar] [CrossRef]
- Shinkawa, H.; Tanaka, S.; Kabata, D.; Takemura, S.; Amano, R.; Kimura, K.; Kinoshita, M.; Kubo, S. The Prognostic Impact of Tumor Differentiation on Recurrence and Survival after Resection of Hepatocellular Carcinoma Is Dependent on Tumor Size. Liver Cancer 2021, 10, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Tokushige, K.; Hashimoto, E.; Yatsuji, S.; Tobari, M.; Taniai, M.; Torii, N.; Shiratori, K. Prospective study of hepatocellular carcinoma in nonalcoholic steatohepatitis in comparison with hepatocellular carcinoma caused by chronic hepatitis C. J. Gastroenterol. 2010, 45, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Wakai, T.; Shirai, Y.; Sakata, J.; Korita, P.V.; Ajioka, Y.; Hatakeyama, K. Surgical outcomes for hepatocellular carcinoma in nonalcoholic fatty liver disease. J. Gastrointest. Surg. 2011, 15, 1450–1458. [Google Scholar] [CrossRef]
- Kramer, J.R.; Natarajan, Y.; Dai, J.; Yu, X.; Li, L.; El-Serag, H.B.; Kanwal, F. Effect of diabetes medications and glycemic control on risk of hepatocellular cancer in patients with nonalcoholic fatty liver disease. Hepatology 2022, 75, 1420–1428. [Google Scholar] [CrossRef]
- Simon, T.G.; King, L.Y.; Chong, D.Q.; Nguyen, L.H.; Ma, Y.; VoPham, T.; Giovannucci, E.L.; Fuchs, C.S.; Meyerhardt, J.A.; Corey, K.E.; et al. Diabetes, metabolic comorbidities, and risk of hepatocellular carcinoma: Results from two prospective cohort studies. Hepatology 2018, 67, 1797–1806. [Google Scholar] [CrossRef]
- Komura, T.; Mizukoshi, E.; Kita, Y.; Sakurai, M.; Takata, Y.; Arai, K.; Yamashita, T.; Ohta, T.; Shimizu, K.; Nakamoto, Y.; et al. Impact of diabetes on recurrence of hepatocellular carcinoma after surgical treatment in patients with viral hepatitis. Am. J. Gastroenterol. 2007, 102, 1939–1946. [Google Scholar] [CrossRef]
- Shan, J.; Shen, J.; Liu, L.; Xia, F.; Xu, C.; Duan, G.; Xu, Y.; Ma, Q.; Yang, Z.; Zhang, Q.; et al. Nanog regulates self-renewal of cancer stem cells through the insulin-like growth factor pathway in human hepatocellular carcinoma. Hepatology 2012, 56, 1004–1014. [Google Scholar] [CrossRef]
- Pinyol, R.; Torrecilla, S.; Wang, H.; Montironi, C.; Pique-Gili, M.; Torres-Martin, M.; Wei-Qiang, L.; Willoughby, C.E.; Ramadori, P.; Andreu-Oller, C.; et al. Molecular characterisation of hepatocellular carcinoma in patients with non-alcoholic steatohepatitis. J. Hepatol. 2021, 75, 865–878. [Google Scholar] [CrossRef]
- Pfister, D.; Nunez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Lau, W.Y.; Wang, Z.G.; Pan, Z.Y.; Yuan, S.X.; Shen, F.; Zhou, W.P.; Wu, M.C. Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: A randomized controlled trial. Ann. Surg. 2015, 261, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Li, N.; Han, Y.; Xue, J.; Deng, Y.; Shi, J.; Guo, W.; Zhang, H.; Wang, H.; Cheng, S.; et al. Effect of antiviral treatment with nucleotide/nucleoside analogs on postoperative prognosis of hepatitis B virus-related hepatocellular carcinoma: A two-stage longitudinal clinical study. J. Clin. Oncol. 2013, 31, 3647–3655. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Chen, P.; Qian, Y. Evaluation of Antiviral Therapy Performed after Curative Therapy in Patients with HBV-Related Hepatocellular Carcinoma: An Updated Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2016, 2016, 5234969. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HBV (n = 121) | HCV (n = 54) | NASH (n = 31) | p Value | ||
|---|---|---|---|---|---|
| Age | 60 (32–88) | 68 (48–83) | 66 (52–80) | 0.000 | |
| Gender | Male vs. Female | 96 (79.3%) vs. 25 (20.7%) | 36 (66.7%) vs. 18 (33.3%) | 23 (74.2%) vs. 8 (25.8%) | 0.20 |
| Body weight (kg) | 65.0 (33.7–110.0) | 60.2 (38.8–95.5) | 70.0 (40.6–87.0) | 0.10 | |
| BMI (kg/m2) | 24.1 (14.4–34.3) | 23.9 (18.5–32.8) | 26.2 (18.0–31.9) | 0.004 | |
| Type II diabetes | Absent vs. Present | 100 (82.6%) vs. 21 (17.4%) | 33 (61.1%) vs. 21 (38.9%) | 12 (38.7%) vs. 19 (61.3%) | <0.001 |
| Hypertension | Absent vs. Present | 66 (54.5%)/55 (45.5%) | 19 (35.2%)/35 (64.8%) | 7 (22.6%)/24 (77.4%) | 0.002 |
| Hyperlipidemia | Absent vs. Present | 98 (81.0%)/23 (19.0%) | 40 (74.1%)/14 (25.9%) | 22 (71.0%)/9 (29.0%) | 0.370 |
| BCLC stage | 0/Solitary/Multinodular/B | 29 (24.0%)/83 (68.6%)/6 (5.0%)/3 (2.5%) | 14 (25.9%)/36 (66.7%)/2 (3.7%)/2 (3.7%) | 5 (16.1%)/22 (71.0%)/3 (9.7%)/1 (3.2%) | 0.87 |
| Maximal Tumor length (cm) | 3.1 (0.9–26.0) | 2.8 (0.8–11.5) | 3.5 (0.9–8.0) | 0.17 | |
| Tumor number | 1 vs. 2 | 112 (92.6%)/9 (7.4%) | 50 (92.6%)/4 (7.4%) | 27 (87.1%)/4 (12.9%) | 0.59 |
| Histologic differentiation | Well/moderate/poor | 26 (21.5%)/85 (70.2%)/10 (8.3%) | 10 (18.5%)/35 (64.8%)/9 (16.7%) | 4 (12.9%)/25 (80.6%)/2 (6.5%) | 0.31 |
| Cytological grade | G1/G2/G3 | 19 (16.7%)/66 (57.9%)/29 (25.4%) | 9 (17.0%)/24 (45.3%)/20 (37.7%) | 4 (13.3%)/21 (70.0%)/5 (16.7%) | 0.21 |
| Tumor capsulation | Well capsulated | 27 (22.3%) | 23 (42.6%) | 7 (22.6%) | 0.03 |
| Partly capsulated | 70 (57.9%) | 18 (33.3%) | 16 (51.6%) | ||
| Non-capsulated | 24 (19.8%) | 13 (24.1%) | 8 (25.8%) | ||
| Invasion of tumor capsule | No vs. Yes | 62 (51.2%) vs. 59 (48.8%) | 29 (53.7%) vs. 25 (46.3%) | 22 (71.0%) vs. 9 (29.0%) | 0.14 |
| Satellite nodule | Absent vs. presented | 104 (86.0%) vs. 17 (14.0%) | 50 (92.6%) vs. 4 (7.4%) | 30 (96.8%) vs. 1 (3.2%) | 0.15 |
| Distance from margin | >10 mm vs. <10 mm | 36 (30.0%) vs. 84 (70.0%) | 13 (24.5%) vs. 40 (75.5%) | 11 (35.5%) vs. 20 (64.5%) | 0.56 |
| Microvascular invasion | Absent vs. Presented | 91 (75.2%) vs. 30 (24.8%) | 40 (74.1%) vs. 14 (25.9%) | 24 (77.4%) vs. 7 (22.6%) | 0.94 |
| Type of liver resection | Non-anatomical vs. anatomical | 40 (33.1%)/88 (66.9%) | 29 (53.7%)/25 (46.3%) | 14 (45.2%)/17 (54.8%) | 0.03 |
| Fibrosis stage (Metavir) | ½/3/4 | 20 (16.5%)/11 (9.1%)/46 (38.0%)/44 (36.4%) | 1 (1.9%)/6 (11.1%)/26 (48.1%)/21 (38.9%) | 4 (12.9%)/4 (12.9%)/6 (19.4%)/17 (54.8%) | 0.04 |
| Steatosis (%) | 3.0% (0.0–35.0%) | 2.5% (0.9–30.0%) | 25.0% (5.0–65.0%) | 0.000 | |
| Brunt inflammatory grade | No | 121 (100%) | 54 (100%) | 0 | NA. |
| Grade 1 | 0 | 0 | 24 (77.4%) | ||
| Grade 2 | 0 | 0 | 7 (22.6%) | ||
| Antiviral treatment | Before diagnosis | 35 (31.5%) | 19 (36.5%) | NA | 0.26 |
| After diagnosis | 56 (50.5%) | 27 (51.9%) | |||
| No treatment and low viral load * | 12 (10.8%) | 1 (1.9%) | |||
| No treatment and high viral load * | 8 (7.2%) | 5 (9.6%) | |||
| Viral suppression # | No suppression before surgery | 58 (65.2%) | 30 (65.2%) | NA. | 0.58 |
| Suppressed before surgery $ | 31 (34.8%) | 16 (34.8%) | |||
| Pre-surgical AFP (ng/mL) | 10.6 (0.6–60,500.0) | 5.5 (1.5–3519.0) | 4.3 (0.9–3076.0) | 0.43 | |
| ALT (U/L) | 26 (10–162) | 25 (9–258) | 37 (10–180) | 0.05 | |
| AST (U/L) | 34 (14–205) | 39 (16–140) | 36 (16–93) | 0.75 | |
| Platelet (103/μL) | 179 (75–420) | 165 (66–446) | 196 (75–311) | 0.16 | |
| Alb (g/dL) | 4.5 (3.0–5.4) | 4.4 (1.8–5.3) | 4.5 (3.5–5.3) | 0.24 | |
| Bil-T (mg/dL) | 0.6 (0.2–6.4) | 0.6 (0.2–1.2) | 0.6 (0.2–2.7) | 0.41 | |
| PT (INR) | 1.04 (0.88–1.27) | 1.03 (0.88–1.24) | 1.04 (0.90–1.14) | 0.28 | |
| Ascites | Absent vs. presented | 113 (95.0%) vs. 6 (5.0%) | 48 (96.0%) vs. 2 (4.0%) | 28 (93.3%) vs. 2 (6.7%) | 0.87 |
| Hepatic encephalopathy | No vs. presented. | 120 (100.0%) vs. 0% | 54 (100.0%) vs. 0% | 31 (100.0%) vs. 0% | |
| CTP score | 5/6/7 | 100 (92.6%)/4 (3.7%)/4 (3.7%) | 47 (95.9%)/2 (4.1%)/0 (0.0%) | 25 (89.3%)/3 (10.7%)/0 (0.0%) | 0.26 |
| APRI score | 0.52 (0.11–1.93) | 0.62 (0.11–3.02) | 0.48 (0.17–1.92) | 0.06 | |
| ALBI score | −3.20 (−3.88~−1.54) | −3.07 (−3.76~−2.48) | −3.07 (−3.95~−1.88) | 0.76 | |
| OS | TTR | RFS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | ||||||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Etiology | NASH vs. viral | 2.09 (0.83–5.29) | 0.12 | 1.81 (0.63–5.21) | 0.27 | 1.81 (1.04–3.15) | 0.036 | 2.27 (1.25–4.12) | 0.01 | 1.75 (1.03–3.00) | 0.040 | 1.51 (0.81–2.81) | 0.20 |
| Age | >60 vs. ≤60 | 1.20 (0.52–2.81) | 0.67 | 1.03 (0.65–1.63) | 0.90 | 1.06 (0.68–1.65) | 0.79 | ||||||
| Gender | Female vs. Male | 1.23 (0.51–2.97) | 0.64 | 0.95 (0.56–1.59) | 0.83 | 1.02 (0.63–1.66) | 0.94 | ||||||
| BMI | <23 | Ref. | 0.96 | Ref. | 0.44 | Ref. | 0.43 | ||||||
| 23–30 | 1.09 (0.46–2.56) | 0.85 | 1.33 (0.82–2.17) | 0.25 | 1.34 (0.84–2.14) | 0.22 | |||||||
| >30 | 0.83 (0.10–6.66) | 0.86 | 1.59 (0.60–4.16) | 0.35 | 1.46 (0.56–3.80) | 0.44 | |||||||
| Type II DM | Presented vs. Absent | 1.65 (0.73–3.72) | 0.22 | 1.20 (0.75–1.93) | 0.44 | 1.46 (0.94–2.26) | 0.09 | 1.16 (0.69–1.95) | 0.57 | ||||
| Hypertension | Presented vs. Absent | 1.63 (0.70–3.81) | 0.26 | 1.26 (0.80–1.98) | 0.32 | 1.30 (0.84–2.01) | 0.23 | ||||||
| Hyperlipidemia | Presented vs. Absent | 1.39 (0.58–3.36) | 0.46 | 0.95 (0.55–1.62) | 0.84 | 1.05 (0.64–1.73) | 0.85 | ||||||
| BCLC stage | 0 | Ref. | 0.03 | Ref. | 0.01 | Ref. | 0.99 | Ref. | 0.91 | ||||
| Solitary | 1.49 (0.50–4.47) | 0.47 | 2.06 (0.67–6.35) | 0.21 | 1.08 (0.64–1.82) | 0.77 | 1.05 (0.64–1.72) | 0.86 | |||||
| Multiple within Milan | 0.99 (0.11–8.82) | 0.99 | 0.56 (0.06–5.06) | 0.60 | 1.01 (0.34–2.96) | 0.99 | 0.91 (0.31–2.64) | 0.86 | |||||
| B | 7.97 (1.78–35.69) | 0.01 | 12.57 (2.61–60.52) | 0.0016 | 1.15 (0.27–4.96) | 0.85 | 1.53 (0.46–5.13) | 0.49 | |||||
| Tumor number | 2 vs. 1 | 2.12 (0.72–6.20) | 0.17 | 0.99 (0.43–2.28) | 0.99 | 1.06 (0.49–2.30) | 0.88 | ||||||
| Tumor length (cm) | <2 | Ref. | 0.75 | Ref. | 0.88 | Ref. | 0.99 | ||||||
| 2–4.9 | 1.37 (0.49–3.80) | 0.55 | 1.01 (0.60–1.70) | 0.97 | 1.03 (0.62–1.69) | 0.92 | |||||||
| ≥5 | 1.59 (0.46–5.50) | 0.46 | 1.17 (0.60–2.26) | 0.65 | 1.05 (0.55–2.02) | 0.88 | |||||||
| Histologic differentiation | Well | Ref. | 0.60 | Ref. | 0.48 | 0.47 | |||||||
| Moderate | 1.25 (0.42–3.67) | 0.69 | 1.40 (0.77–2.56) | 0.27 | 1.33 (0.76–2.33) | 0.33 | |||||||
| Poor | 0.46 (0.05–4.15) | 0.49 | 1.07 (0.43–2.69) | 0.88 | 0.94 (0.38–2.30) | 0.89 | |||||||
| Cytological grade | Grade 1 | Ref. | 0.92 | Ref. | 0.44 | 0.59 | |||||||
| Grade 2 | 0.85 (0.27–2.64) | 0.78 | 1.55 (0.76–3.19) | 0.23 | 1.37 (0.71–2.65) | 0.35 | |||||||
| Grades 3–4 | 1.02 (0.30–3.47) | 0.98 | 1.61 (0.74–3.49) | 0.23 | 1.43 (0.70–2.93) | 0.32 | |||||||
| Tumor Capsulation | Well | Ref. | 0.00 | Ref. | 0.001 | Ref. | 0.89 | 0.54 | |||||
| Partial | 1.52 (0.41–5.62) | 0.53 | 1.30 (0.35–4.85) | 0.70 | 1.07 (0.63–1.83) | 0.80 | 1.00 (0.60–1.68) | 0.99 | |||||
| No capsule | 5.28 (1.49–18.71) | 0.01 | 5.88 (1.59–21.70) | 0.01 | 1.17 (0.62–2.21) | 0.63 | 1.32 (0.73–2.38) | 0.36 | |||||
| Invasion of tumor capsule | Yes vs. no | 1.39 (0.62–3.11) | 0.42 | 1.42 (0.91–2.21) | 0.12 | 1.31 (0.81–2.09) | 0.27 | 1.31 (0.86–2.00) | 0.21 | ||||
| Satellite nodule | Present vs. absent. | 2.88 (1.14–7.26) | 0.03 | 2.02 (1.11–3.67) | 0.02 | 1.92 (1.01–3.65) | 0.045 | 1.84 (1.02–3.32) | 0.04 | 1.66 (0.84–3.27) | 0.14 | ||
| Safety margin (mm) | ≥10 vs. <10 | 1.55 (0.58–4.16) | 0.38 | 0.97 (0.59–1.57) | 0.89 | 0.98 (0.61–1.56) | 0.93 | ||||||
| Microvascular invasion | Present vs. absent | 1.50 (0.64–3.51) | 0.35 | 1.55 (0.96–2.49) | 0.07 | 1.20 (0.69–2.08) | 0.52 | 1.44 (0.91–2.28) | 0.12 | 1.38 (0.81–2.34) | 0.24 | ||
| Resection type | Anatomical vs. non-anatomical resection | 0.44 (0.19–0.98) | 0.05 | 0.58 (0.23–1.46) | 0.25 | 0.62 (0.40–0.97) | 0.04 | 0.65 (0.41–1.03) | 0.07 | 0.60 (0.39–0.92) | 0.02 | 0.65 (0.42–1.01) | 0.055 |
| Recurrence after surgery | Yes vs. no | 5.10 (1.88–13.83) | 0.00 | 4.43 (1.72–11.42) | 0.002 | ||||||||
| Cirrhosis | Present vs. Absent | 1.14 (0.51–2.56) | 0.75 | 1.92 (1.23–2.99) | 0.00 | 1.41 (0.88–2.26) | 0.16 | 1.96 (1.28–3.01) | 0.00 | 1.76 (1.14–2.73) | 0.01 | ||
| CTP score | A5 | Ref. | 0.47 | Ref. | 0.95 | Ref. | 0.08 | (-) | 0.02 | 0.05 | (-) | 0.06 | |
| A6 | 1.94 (0.45–8.28) | 0.37 | 1.31 (0.26–6.73) | 0.75 | 1.26 (0.46–3.45) | 0.65 | 1.14 (0.39–3.32) | 0.82 | 1.76 (0.77–4.06) | 0.18 | 1.30 (0.52–3.24) | 0.57 | |
| B7 | 2.51 (0.34–18.80) | 0.37 | 0.92 (0.08–10.44) | 0.95 | 3.68 (1.15–11.78) | 0.03 | 5.17 (1.58–16.95) | 0.01 | 3.50 (1.10–11.19) | 0.03 | 4.09 (1.25–13.37) | 0.02 | |
| APRI | APRI >1 vs. <1 | 1.20 (0.41–3.50) | 0.74 | 1.68 (0.96–2.95) | 0.07 | 1.64 (0.95–2.82) | 0.08 | ||||||
| ALBI grade | Grade 2 vs. Grade 1 | 2.43 (0.83–7.15) | 0.11 | 1.86 (0.44–7.90) | 0.40 | 1.28 (0.59–2.78) | 0.54 | 1.33 (0.64–2.76) | 0.44 | ||||
| Baseline AFP | >20 vs. ≤20 | 1.09 (0.46–2.54) | 0.85 | 1.49 (0.95–2.33) | 0.08 | 1.72 (1.05–2.83) | 0.03 | 1.36 (0.88–2.09) | 0.17 | ||||
| HBV (n = 26) | NASH (n = 26) | |||
|---|---|---|---|---|
| Median (Range) or n (%) | Median (Range) or n (%) | p Value | ||
| Age | 65 (37–77) | 66 (52–80) | 0.14 | |
| Gender | Male vs. female | 20 (76.9%) vs. 6 (23.1%) | 20 (76.9%) vs. 6 (23.1%) | 1.00 |
| BMI | 25.9 (19.6–33.0) | 26.3 (22.1–31.9) | 0.45 | |
| Type II diabetes | Absent vs. present | 16 (61.5%) vs. 10 (38.5%) | 15 (57.7%) vs. 11 (42.3%) | 0.78 |
| BCLC stage | 0/solitary/multinodular within Milan/B | 4 (15.4%)/20 (76.9%)/1 (3.8%)/1 (3.8%) | 4 (15.4%)/19 (73.1%)/2 (7.7%)/1 (3.8%) | 0.95 |
| Maximal Tumor length (cm) | 3.5 (1.2–14.0) | 4.0 (0.9–8.0) | 1.00 | |
| Tumor number | 1 vs. 2 | 24 (92.3%) vs. 2 (7.7%) | 23 (88.5%) vs. 3 (11.5%) | 0.64 |
| Histologic differentiation | well/moderate/poor | 3 (11.5%)/20 (76.9%)/3 (11.5%) | 2 (7.7%)/23 (88.5%)/1 (3.8%) | 0.49 |
| Cytological grade | G1/G2/G3 | 2 (8.7%)/13 (56.5%)/8 (34.8%) | 2 (8.0%)/19 (76.0%)/4 (16.0%) | 0.30 |
| Tumor capsule formation | Well capsulated | 6 (23.1%) | 6 (23.1%) | 0.60 |
| Partially capsulated | 12 (46.2%) | 15 (57.7%) | ||
| Non-capsulated | 8 (30.8%) | 5 (19.2%) | ||
| Invasion of tumor capsule | No vs. Yes | 14 (53.8%) vs. 12 (46.2%) | 18 (69.2%) vs. 8 (30.8%) | 0.25 |
| Satellite nodule | Absent vs. Presented | 23 (88.5%) vs. 3 (11.5%) | 25 (96.2%) vs. 1 (3.8%) | 0.30 |
| Safety margin | >10 mm vs. <10 mm | 8 (30.8%) vs. 18 (69.2%) | 8 (30.8%) vs. 18 (69.2%) | 1.00 |
| Microvascular invasion | Absent vs. Presented | 19 (73.1%) vs. 7 (26.9%) | 20 (76.9%) vs. 6 (23.1%) | 0.75 |
| Cirrhosis | Absent vs. Presented | 17 (65.4%) vs. 9 (34.6%) | 13 (50.0%) vs. 13 (50.0%) | 0.26 |
| ALT (U/L) | 26 (10–162) | 54 (10–180) | 0.10 | |
| AST (U/L) | 34 (14–184) | 46 (22–87) | 0.92 | |
| Platelet ((103/μL) | 168 (96–400) | 201 (97–311) | 0.24 | |
| Alb (g/dL) | 4.5 (3.4–5.1) | 4.4 (3.5–5.3) | 0.77 | |
| Bil-T (mg/dL) | 0.7 (0.3–4.3) | 0.7 (0.2–2.7) | 0.67 | |
| PT (INR) | 1.0 (0.9–1.2) | 1.0 (0.9–1.1) | 0.16 | |
| Ascites | Absent vs. Presented | 25 (96.2%) vs. 1 (3.8%) | 24 (96.0%) vs. 1 (4.0%) | 0.98 |
| CTP score | 5/6/7 | 22 (88.0%)/2 (8.0%)/1 (4.0%) | 22 (91.7%)/2 (8.3%)/0 (0.0%) | 0.61 |
| ALBI score | −3.18 (−3.67~−2.18) | −3.09 (−3.95~−1.88) | 0.87 | |
| Baseline AFP before surgery (ng/mL) | 8.5 (1.1–60,500.0) | 251.6 (0.9–3076.0) | 0.34 | |
| APRI score | 0.57 (0.18–1.93) | 0.65 (0.22–1.92) | 0.98 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, S.-C.; Lin, Y.-J.; Lee, C.-T.; Chiu, Y.-C.; Chou, T.-C.; Chiu, H.-C.; Tsai, H.-W.; Su, C.-M.; Yang, T.-H.; Chiang, H.-C.; et al. Higher Risk of Tumor Recurrence in NASH-Related Hepatocellular Carcinoma Following Curative Resection. Viruses 2022, 14, 2427. https://doi.org/10.3390/v14112427
Chien S-C, Lin Y-J, Lee C-T, Chiu Y-C, Chou T-C, Chiu H-C, Tsai H-W, Su C-M, Yang T-H, Chiang H-C, et al. Higher Risk of Tumor Recurrence in NASH-Related Hepatocellular Carcinoma Following Curative Resection. Viruses. 2022; 14(11):2427. https://doi.org/10.3390/v14112427
Chicago/Turabian StyleChien, Shih-Chieh, Yih-Jyh Lin, Chun-Te Lee, Yen-Cheng Chiu, Tsung-Ching Chou, Hung-Chih Chiu, Hung-Wen Tsai, Che-Min Su, Tsung-Han Yang, Hsueh-Chien Chiang, and et al. 2022. "Higher Risk of Tumor Recurrence in NASH-Related Hepatocellular Carcinoma Following Curative Resection" Viruses 14, no. 11: 2427. https://doi.org/10.3390/v14112427
APA StyleChien, S.-C., Lin, Y.-J., Lee, C.-T., Chiu, Y.-C., Chou, T.-C., Chiu, H.-C., Tsai, H.-W., Su, C.-M., Yang, T.-H., Chiang, H.-C., Tsai, W.-C., Yang, K.-C., & Cheng, P.-N. (2022). Higher Risk of Tumor Recurrence in NASH-Related Hepatocellular Carcinoma Following Curative Resection. Viruses, 14(11), 2427. https://doi.org/10.3390/v14112427