
COVID-19 Infection in Pregnancy: PCR Cycle Thresholds, Placental Pathology, and Perinatal Outcomes

 ,
,  ,
,  , ,
, ,  ,
,  , , ,
, , ,  and add
Show full author list
and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design and Approach
2.2. Reverse Transcription Quantitative Real-Time Polymerase Chain Reaction (RT-qPCR) for SARS-CoV-2
2.3. CT Values
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics, CTs, and Placental Pathology
3.1.1. Maternal Demographic and Clinical Characteristics
3.1.2. PCR Test CTs
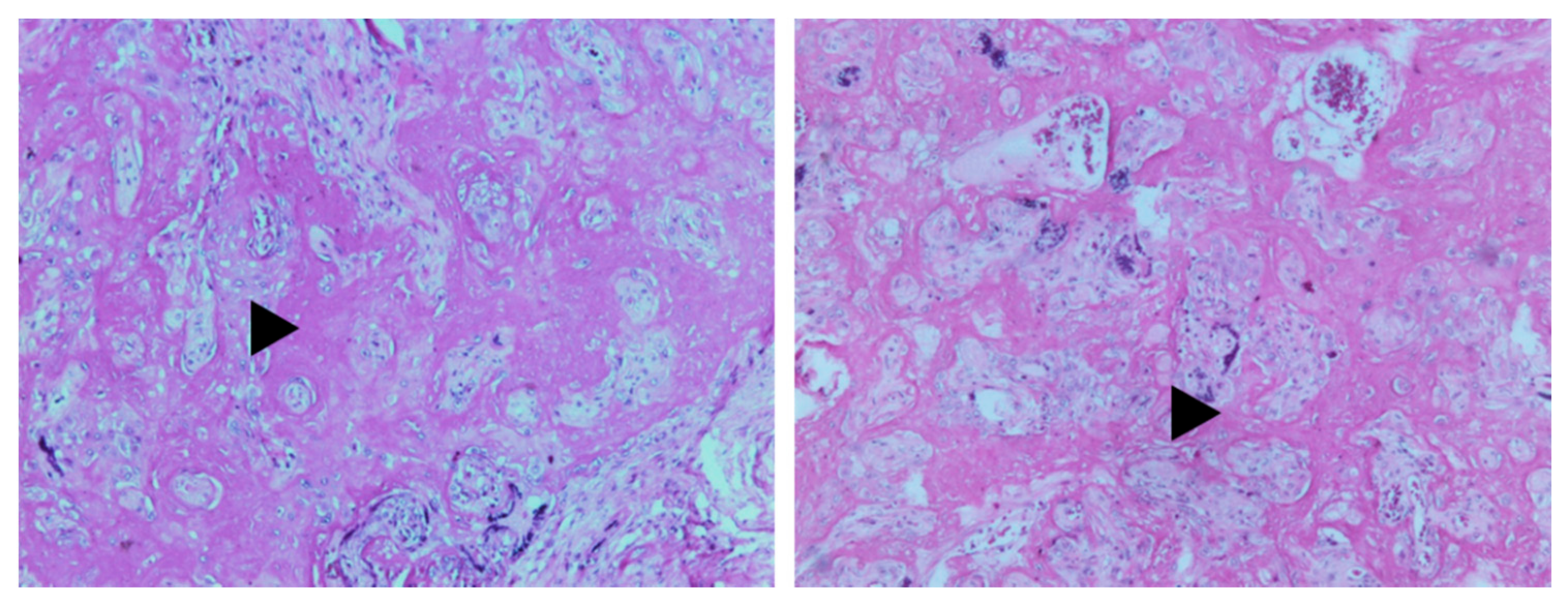
3.1.3. Placental Pathology and CTs
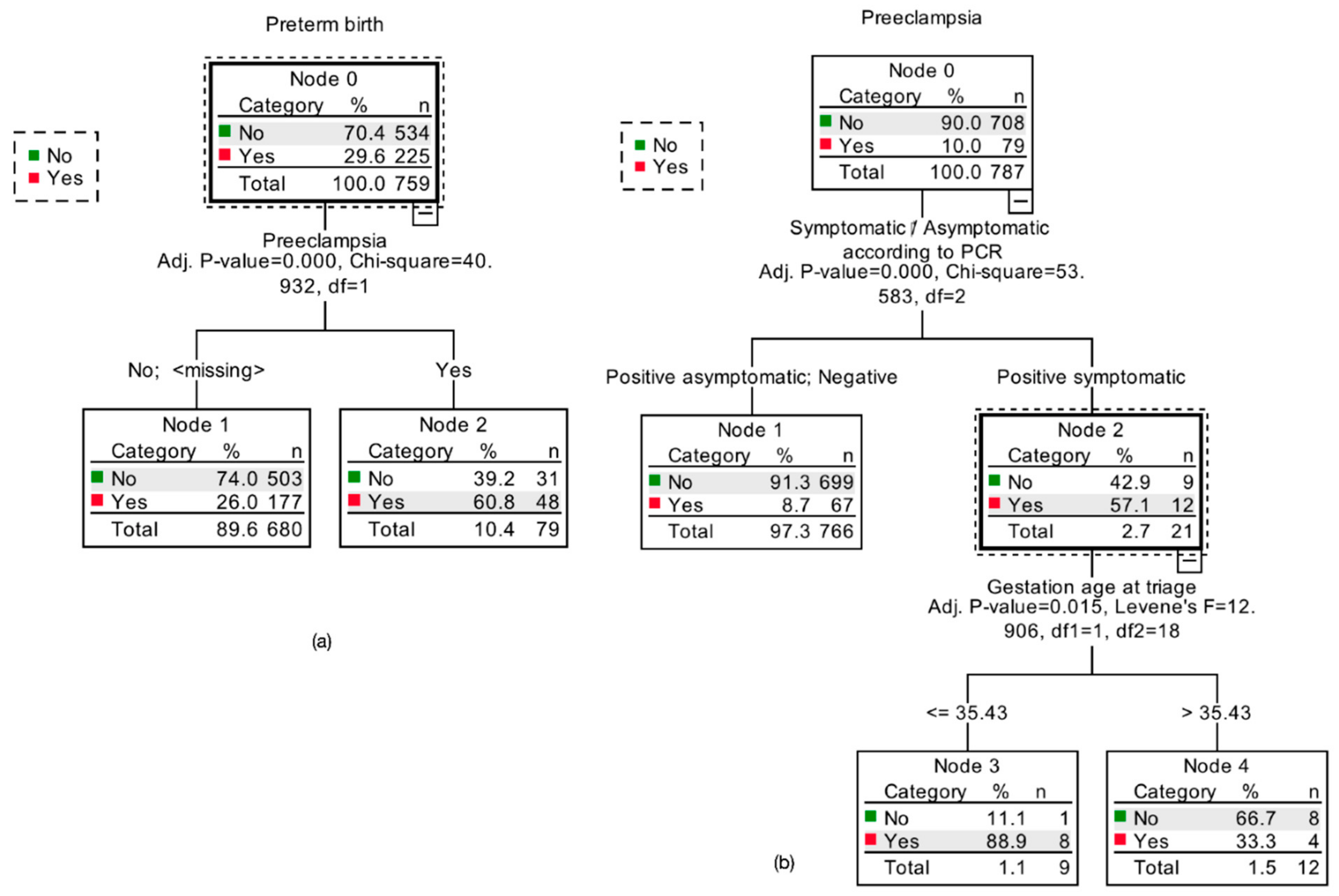
3.2. Pregnancy Outcomes
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Guleria, I.; Sayegh, M.H. Maternal Acceptance of the Fetus: True Human Tolerance. J. Immunol. 2007, 178, 3345–3351. [Google Scholar] [CrossRef]
- Alberca, R.W.; Pereira, N.Z.; Oliveira, L.M.D.S.; Gozzi-Silva, S.C.; Sato, M.N. Pregnancy, Viral Infection, and COVID-19. Front. Immunol. 2020, 11, 1672. [Google Scholar] [CrossRef] [PubMed]
- Neggers, Y. The Association between Viral Infections, Maternal and Fetal Mortality/Morbidity. Glob. J. Reprod. Med. 2018, 4, 45–46. [Google Scholar] [CrossRef]
- Prabhu, M.; Cagino, K.; Matthews, K.C.; Friedlander, R.L.; Glynn, S.M.; Kubiak, J.M.; Yang, Y.J.; Zhao, Z.; Baergen, R.N.; DiPace, J.I.; et al. Pregnancy and Postpartum Outcomes in a Universally Tested Population for SARS-CoV-2 in New York City: A Prospective Cohort Study. BJOG An. Int. J. Obstet. Gynaecol. 2020, 127, 1548–1556. [Google Scholar] [CrossRef]
- Valdespino-Vázquez, M.Y.; Helguera-Repetto, C.A.; León-Juárez, M.; Villavicencio-Carrisoza, O.; Flores-Pliego, A.; Moreno-Verduzco, E.R.; Díaz-Pérez, D.L.; Villegas-Mota, I.; Carrasco-Ramírez, E.; López-Martínez, I.E.; et al. Fetal and Placental Infection with SARS-CoV-2 in Early Pregnancy. J. Med. Virol. 2021, 93, 4480–4487. [Google Scholar] [CrossRef] [PubMed]
- Hosier, H.; Farhadian, S.F.; Morotti, R.A.; Deshmukh, U.; Lu-Culligan, A.; Campbell, K.H.; Yasumoto, Y.; Vogels, C.B.; Casanovas-Massana, A.; Vijayakumar, P.; et al. SARS-CoV-2 Infection of the Placenta. J. Clin. Investig. 2020, 130, 4947–4953. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Levitan, D. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infecting pregnant women and the fetus, intrauterine transmission, and placental pathology during the Coronavirus Disease 2019 (COVID-19) pandemic: It’s complicated. Arch. Pathol. Lab. Med. 2021, 145, 925–928. [Google Scholar] [CrossRef]
- Scwartz, D.A.; Morotti, D. Placental pathology of COVID-19 with and without fetal and neonatal infection: Trophoblast necrosis and histiocytic intervillositis as risk factor for transplacental transmission of SARS-CoV-2. Viruses 2020, 12, 1308. [Google Scholar] [CrossRef]
- Liu, H.; Wang, L.-L.; Zhao, S.-J.; Kwak-Kim, J.; Mor, G.; Liao, A.-H. Why Are Pregnant Women Susceptible to COVID-19? An Immunological Viewpoint. J. Reprod. Immunol. 2020, 139, 103122. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wang, L.; Fang, C.; Peng, S.; Zhang, L.; Chang, G.; Xia, S.; Zhou, W. Clinical Analysis of 10 Neonates Born to Mothers with 2019-nCoV Pneumonia. Transl. Pediatr. 2020, 9, 51–60. [Google Scholar] [CrossRef]
- Hernández-Cruz, R.G.; Sánchez-Cobo, D.; Acevedo-Gallegos, S.; Helguera-Repetto, A.C.; Rodriguez-Bosch, M.R.; Ramirez-Santes, V.H.; Villegas-Mota, I.; Cardona-Pérez, A.; Cortes-Bonilla, M.; Irles, C.; et al. Clinical Characteristics and Risk Factors for SARS-CoV-2 Infection in Pregnant Women Attending a Third Level Reference Center in Mexico City. J. Matern. Fetal. Neonatal Med. 2021, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Pérez, J.A.; Villegas-Mota, I.; Helguera-Repetto, A.C.; Acevedo-Gallegos, S.; Rodríguez-Bosch, M.; Aguinaga-Ríos, M.; Coronado-Zarco, I.; León-Juárez, M.; Aguilar-Ayala, D.; Valdespino-Vázquez, M.Y.; et al. Prevalence, Clinical Features, and Outcomes of SARS-CoV-2 Infection in Pregnant Women with or without Mild/moderate Symptoms: Results from Universal Screening in a Tertiary Care Center in Mexico City, Mexico. PLoS ONE 2021, 16, e0249584. [Google Scholar] [CrossRef] [PubMed]
- Keyaerts, E.; Vijgen, L.; Maes, P.; Duson, G.; Neyts, J.; Van Ranst, M. Viral Load Quantitation of SARS-Coronavirus RNA Using a One-Step Real-Time RT-PCR. Int. J. Infect. Dis. 2006, 10, 32–37. [Google Scholar] [CrossRef][Green Version]
- Han, M.S.; Byun, J.-H.; Cho, Y.; Rim, J.H. RT-PCR for SARS-CoV-2: Quantitative versus Qualitative. Lancet Infect. Dis. 2021, 21, 165. [Google Scholar] [CrossRef]
- Shah, S.; Singhal, T.; Davar, N.; Thakkar, P. No Correlation between Ct Values and Severity of Disease or Mortality in Patients with COVID 19 Disease. Indian J. Med. Microbiol. 2021, 39, 116–117. [Google Scholar] [CrossRef]
- Liu, Y.; Yan, L.-M.; Wan, L.; Xiang, T.-X.; Le, A.; Liu, J.-M.; Peiris, M.; Poon, L.L.M.; Zhang, W. Viral Dynamics in Mild and Severe Cases of COVID-19. Lancet Infect. Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef]
- Magleby, R.; Westblade, L.F.; Trzebucki, A.; Simon, M.S.; Rajan, M.; Park, J.; Goyal, P.; Safford, M.M.; Satlin, M.J. Impact of SARS-CoV-2 Viral Load on Risk of Intubation and Mortality Among Hospitalized Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wong, Y.P.; Khong, T.Y.; Tan, G.C. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I. The Immune System in Pregnancy: A Unique Complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef]
- Bonney, E.A. Immune Regulation in Pregnancy: A Matter of Perspective? Obstet. Gynecol. Clin. N. Am. 2016, 43, 679–698. [Google Scholar] [CrossRef]
- Rebutini, P.Z.; Zanchettin, A.C.; Stonoga, E.T.S.; Prá, D.M.M.; de Oliveira, A.L.P.; da Silva Dezidério, F.; Fonseca, A.S.; Dagostini, J.C.H.; Hlatchuk, E.C.; Furuie, I.N.; et al. Association Between COVID-19 Pregnant Women Symptoms Severity and Placental Morphologic Features. Front. Immunol. 2021, 12, 685919. [Google Scholar] [CrossRef]
- Watkins, J.C.; Torous, V.F. and Roberts, D.J. Defining-Severe Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) placentitis: A report of 7 cases with confirmatory in situ hybridization, distinct histomorphologic features, and evidence of complement deposition. Arch. Pathol. Lab. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef]
- Tanacan, A.; Anuk, A.T.; Erol, S.A.; Keskin, H.L.; Altinboga, O.; Yakistiran, B.; Aydogan, S.; Unlu, S.; Eyi, E.G.Y.; Tayman, C.; et al. The Effect of Real-Time Polymerase Chain Reaction Cycle Threshold Values on Perinatal Outcomes of Pregnant Women with COVID-19. J. Matern. Fetal. Neonatal Med. 2021, 1–8, online ahead of print. [Google Scholar] [CrossRef]
- Papageorghiou, A.T.; Deruelle, P.; Gunier, R.B.; Rauch, S.; García-May, P.K.; Mhatre, M.; Usman, M.A.; Abd-Elsalam, S.; Etuk, S.; Simmons, L.E.; et al. Preeclampsia and COVID-19: Results from the INTERCOVID Prospective Longitudinal Study. Am. J. Obstet. Gynecol. 2021, 225, 289.e1–289.e17. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality among Pregnant Women with and without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Laresgoiti-Servitje, E.; Gomez-Lopez, N. The Pathophysiology of Preeclampsia Involves Altered Levels of Angiogenic Factors Promoted by Hypoxia and Autoantibody-Mediated Mechanisms. Biol. Reprod. 2012, 87, 36. [Google Scholar] [CrossRef]
- Mendoza, M.; Garcia-Ruiz, I.; Maiz, N.; Rodo, C.; Garcia-Manau, P.; Serrano, B.; Lopez-Martinez, R.M.; Balcells, J.; Fernandez-Hidalgo, N.; Carreras, E.; et al. Pre-Eclampsia-like Syndrome Induced by Severe COVID-19: A Prospective Observational Study. BJOG 2020, 127, 1374–1380. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | COVID-19 Positive (298) Mean ± SD N (%) | COVID-19 Negative (828) Mean ± SD N (%) | All Patients (1126) Mean ± SD N (%) | p | |
|---|---|---|---|---|---|
| Maternal age | 27.94 ± 7.2 | 28.3 ± 7.4 | 28.04 ± 7.3 | 0.48 | |
| Pre-pregnancy BMI | 27.05 ± 5.4 | 27.17 ± 5.8 | 27.12 ± 5.2 | 0.74 | |
| Weight gain per week | 0.09 ± 0.52 | 0.20 ± 0.22 | 0.17 ± 0.35 | 0.08 | |
| Pre-pregnancy BMI category: | underweight | 1 (12.5) | 7 (87.5) | 8 | >0.05 |
| normal weight | 38 (36.9) | 65 (87.5) | 103 | >0.05 | |
| overweight | 38 (33) | 77 (67) | 115 | >0.05 | |
| class I obesity | 15 (36.6) | 26 (63.4) | 41 | >0.05 | |
| class II obesity | 8 (40) | 12 (60) | 20 | >0.05 | |
| class III obesity | 2 (20) | 8 (80) | 10 | >0.05 | |
| Number of pregnancies | 2.19 ± 1.3 | 2.23 ± 1.3 | 2.22 ± 1.33 | 0.14 | |
| Number of deliveries | 0.41 ± 0.8 | 0.44 ± 0.8 | 0.43 ± 0.8 | 0.46 | |
| Number of c-sections | 0.57 ± 0.82 | 0.48 ± 0.75 | 0.51 ± 0.77 | 0.03 | |
| Number of miscarriages | 0.42 ± 0.77 | 0.50 ± 0.90 | 0.48 ± 0.87 | 0.01 | |
| Diabetes | No | 257 (25.8) | 740 (74.2) | 997 | >0.05 |
| Type 1 Diabetes | 3 (30) | 7 (70) | 10 | >0.05 | |
| Type 2 Diabetes | 11 (24.4) | 34 (75.6) | 45 | >0.05 | |
| Gestational diabetes | 15 (33.3) | 30 (66.7) | 45 | >0.05 | |
| Chronic hypertension | No | 260 (26.3) | 729 (73.8) | 989 | >0.05 |
| Yes | 12 (23.5) | 39 (76.5) | 51 | >0.05 | |
| Autoimmunity (SLE, RA) | No | 262 (25.5) | 756 (74.5) | 1027 | >0.05 |
| Yes | 15 (33.3) | 30 (66.7) | 45 | >0.05 | |
| Asthma | No | 287 (26.1) | 811 (73.9) | 1098 | >0.05 |
| Yes | 11 (68.8) | 5 (31.3) | 16 | >0.05 | |
| Cardiopathy | No | 288 (26.3) | 807 (73.7) | 1095 | >0.05 |
| Yes | 4 (21.1) | 15 (78.9) | 19 | >0.05 | |
| Hypothyroidism | No | 157 (25.4) | 460 (74.6) | 617 | 0.001 |
| Yes | 18 (51.4) | 17 (48.6) | 35 | 0.001 | |
| Characteristics | COVID-19 Positive (298) Mean ± SD N (%) | COVID-19 Negative (828) Mean ± SD N (%) | All Patients (1126) Mean ± SD N (%) | p | |
|---|---|---|---|---|---|
| Gestational age at triage | 33.40 ± 8.3 | 33.35 ± 8.3 | 33.37 ± 8.4 | 0.91 | |
| Temperature at triage | 36.31 ± 0.49 | 36.35 ± 0.48 | 36.34 ± 0.48 | 0.58 | |
| Breathing rate at triage | 19.01 ± 3.3 | 19.4 ± 5.4 | 19.12 ± 3.9 | 0.07 | |
| Heart rate at triage | 79.01 ± 13.2 | 78.28 ± 10.1 | 78.46 ± 11 | 0.008 | |
| O2 saturation at triage | 94.82 ± 1.9 | 94.43 ± 1.7 | 94.61 ± 1.8 | 0.73 | |
| SBP at triage | 112.2 ± 16.4 | 110.47 ± 13 | 110.9 ± 14 | 0.07 | |
| DBP at triage | 70.41 ± 9.6 | 69.98 ± 8.7 | 70 ± 8.9 | 0.03 | |
| Triage distribution of patients | Programmed visit/asymptomatic patient | 131(28.7) | 325 (71.3%) | 456 | >0.05 |
| Programmed visit/symptomatic patient | 8 (40) | 12 (60%) | 20 | >0.05 | |
| Obstetric emergency | 140 (24.9) | 422 (75.1) | 562 | >0.05 | |
| Hospitalized/suspicious patient | 15 (19.2) | 63 (80.8) | 78 | >0.05 | |
| Women with a positive test and at least one symptom during evaluation | Asymptomatic Symptomatic | 90.2 (269) 9.8 (29) | 298 | <0.001 | |
| Decision after test | Ambulatory treatment | 81 (37.9%) | 133 (62.1%) | 214 | <0.001 |
| Hospital admission | 216 (23.6) | 696 (76.4%) | 912 | <0.001 | |
| Characteristics | COVID-19 Positive (298) Mean ± SD N (%) | COVID-19 Negative (828) Mean ± SD N (%) | All Patients (1126) Mean ± SD N (%) | p | |
|---|---|---|---|---|---|
| Week at delivery | 37.5 ± 3 | 36.44 ± 3.7 | 37 ± 3.4 | 0.28 | |
| Hospitalization days at delivery | 1.72 ± 1.8 | 1.76 ± 1.8 | 1.75 ± 1.3 | 0.13 | |
| Pregnancy resolution | Uterine curettage | 9 (22.5) | 31 (77.5) | 40 | >0.05 |
| Forceps delivery | 3 (37.5) | 5 (62.5) | 8 | >0.05 | |
| Eutocic delivery | 64 (26.7) | 176 (73.3) | 240 | >0.05 | |
| C-section | 124 (25.2) | 368 (74.8) | 492 | >0.05 | |
| Ectopic pregnancy | 0 | 1 (100) | 1 | >0.05 | |
| Manual vacuum aspiration | 0 | 6 (100) | 6 | >0.05 | |
| Pregnancy hypertensive disorders | No | 173 (24.5) | 533 (75.5) | 706 | >0.05 |
| Gestational hypertension | 3 (37.5) | 5 (62.5) | 8 | >0.05 | |
| Preeclampsia | 8 (30.8) | 18 (69.2) | 26 | >0.05 | |
| Preeclampsia with severity features | 16 (34.8) | 30 (65.2) | 46 | >0.05 | |
| HELLP | 1 (20) | 4 (80) | 5 | >0.05 | |
| Eclampsia | 0 | 1 (100) | 1 | >0.05 | |
| Premature rupture of membranes | No | 177 (25.8) | 510 (74.2) | 687 | >0.05 |
| Yes | 23 (22.3) | 80 (77.7) | 103 | >0.05 | |
| Preterm birth | No | 161 (25.9) | 461 (74.1) | 622 | >0.05 |
| Yes | 39 (23.2) | 129 (76.8) | 168 | >0.05 | |
| Obstetric hemorrhage | No | 193 (25.7) | 559 (74.3) | 752 | >0.05 |
| Yes | 7 (18.4) | 31 (81.6) | 38 | >0.05 | |
| Fetal death | No | 190 (25.1) | 566 (74.9) | 756 | >0.05 |
| Yes | 19 (33.3) | 38 (66.7) | 57 | >0.05 | |
| Newborn weight (grams) | 2672.29 ± 823 | 2661.43 ± 836 | 2666.9 ± 825 | 0.83 | |
| Newborn head circumference (cm) | 33.24 ± 2.7 | 32.63 ± 2.9 | 32.9 ± 2.9 | 0.93 | |
| Apgar 1 | 7 ± 2.2 | 6.5 ± 2.4 | 6.79 ± 2.3 | 0.08 | |
| Apgar 5 | 8.36 ± 1.7 | 8.33 ± 1.5 | 8.35 ± 1.7 | 0.85 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laresgoiti-Servitje, E.; Cardona-Pérez, J.A.; Hernández-Cruz, R.G.; Helguera-Repetto, A.C.; Valdespino-Vázquez, M.Y.; Moreno-Verduzco, E.R.; Villegas-Mota, I.; Acevedo-Gallegos, S.; Rodríguez-Bosch, M.; León-Juárez, M.; et al. COVID-19 Infection in Pregnancy: PCR Cycle Thresholds, Placental Pathology, and Perinatal Outcomes. Viruses 2021, 13, 1884. https://doi.org/10.3390/v13091884
Laresgoiti-Servitje E, Cardona-Pérez JA, Hernández-Cruz RG, Helguera-Repetto AC, Valdespino-Vázquez MY, Moreno-Verduzco ER, Villegas-Mota I, Acevedo-Gallegos S, Rodríguez-Bosch M, León-Juárez M, et al. COVID-19 Infection in Pregnancy: PCR Cycle Thresholds, Placental Pathology, and Perinatal Outcomes. Viruses. 2021; 13(9):1884. https://doi.org/10.3390/v13091884
Chicago/Turabian StyleLaresgoiti-Servitje, Estibalitz, Jorge Arturo Cardona-Pérez, Rosa Gabriela Hernández-Cruz, Addy Cecilia Helguera-Repetto, María Yolotzin Valdespino-Vázquez, Elsa Romelia Moreno-Verduzco, Isabel Villegas-Mota, Sandra Acevedo-Gallegos, Mario Rodríguez-Bosch, Moisés León-Juárez, and et al. 2021. "COVID-19 Infection in Pregnancy: PCR Cycle Thresholds, Placental Pathology, and Perinatal Outcomes" Viruses 13, no. 9: 1884. https://doi.org/10.3390/v13091884
APA StyleLaresgoiti-Servitje, E., Cardona-Pérez, J. A., Hernández-Cruz, R. G., Helguera-Repetto, A. C., Valdespino-Vázquez, M. Y., Moreno-Verduzco, E. R., Villegas-Mota, I., Acevedo-Gallegos, S., Rodríguez-Bosch, M., León-Juárez, M., Aguinaga-Ríos, M., Coronado-Zarco, I., Ortiz-Calvillo, A., Rivera-Rueda, M. A., Valencia-Contreras, C., Gómez-Sousa, M. d. L., Solis-Paredes, M., Rodriguez-Aldama, J. C., Galván-Contreras, R., ... Irles, C. (2021). COVID-19 Infection in Pregnancy: PCR Cycle Thresholds, Placental Pathology, and Perinatal Outcomes. Viruses, 13(9), 1884. https://doi.org/10.3390/v13091884