
The Origins and Future of Sentinel: An Early-Warning System for Pandemic Preemption and Response

 , , , ,
, , , ,  ,
, {kind=link}
Abstract
:1. Background
2. Studying Lassa Fever in Nigeria
3. ACEGID: Laying the Groundwork for Local Surveillance and Outbreak Response
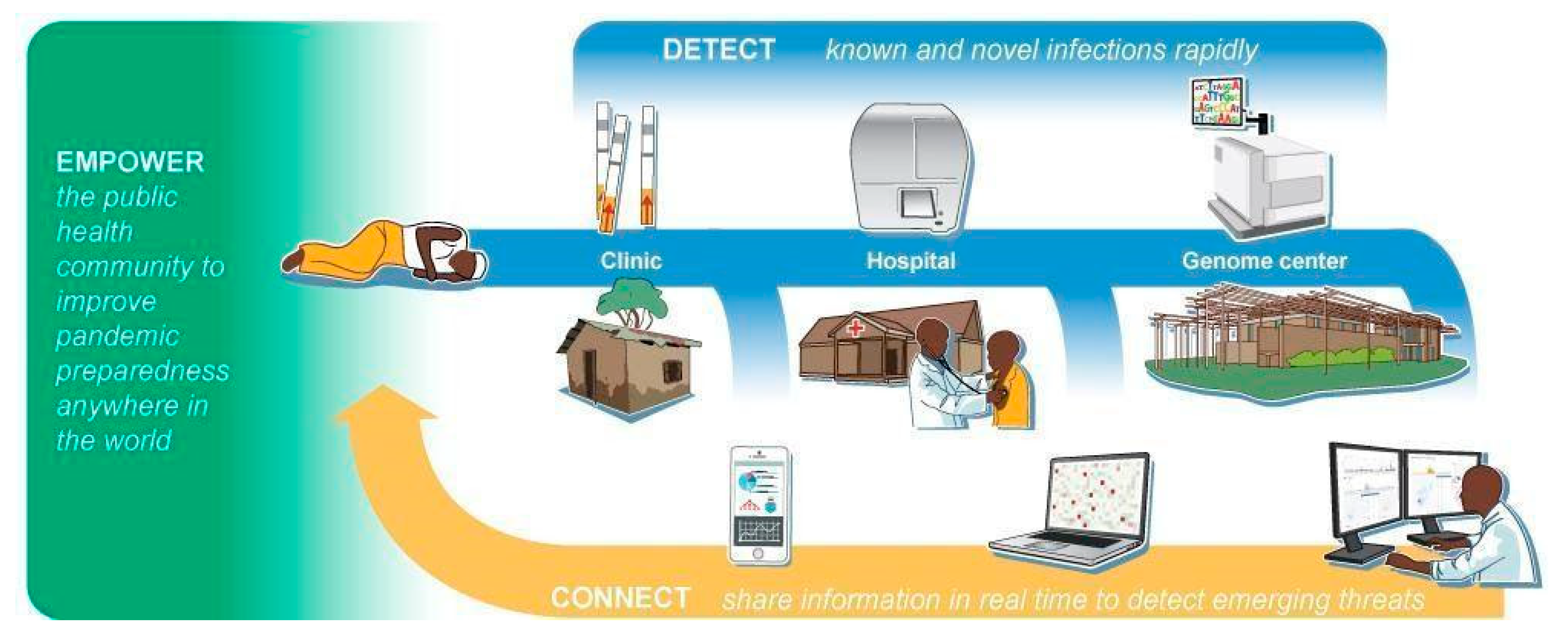
4. A New Approach to Pandemic Preparedness
5. Sentinel Pillar #1: Detect
6. Sentinel Pillar #2: Connect
7. Sentinel Pillar #3: Empower
8. Remembering Dr. Kunz in Our Work Today
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sabeti, P.C.; Varilly, P.; Fry, B.; Lohmueller, J.; Hostetter, E.; Cotsapas, C.; Xie, X.; Byrne, E.H.; McCarroll, S.A.; Gaudet, R.; et al. Genome-Wide Detection and Characterization of Positive Selection in Human Populations. Nature 2007, 449, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Kunz, S.; Rojek, J.M.; Perez, M.; Spiropoulou, C.F.; Oldstone, M.B.A. Characterization of the Interaction of Lassa Fever Virus with Its Cellular Receptor α-Dystroglycan. J. Virol. 2005, 79, 5979–5987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunz, S.; Rojek, J.M.; Kanagawa, M.; Spiropoulou, C.F.; Barresi, R.; Campbell, K.P.; Oldstone, M.B.A. Posttranslational Modification of α-Dystroglycan, the Cellular Receptor for Arenaviruses, by the Glycosyltransferase LARGE Is Critical for Virus Binding. J. Virol. 2005, 79, 14282–14296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troup, J.M.; White, H.A.; Fom, A.L.M.D.; Carey, D.E. An Outbreak of Lassa Fever on the Jos Plateau, Nigeria, in January–February 1970: A Preliminary Report. Am. J. Trop. Med. Hyg. 1970, 19, 695–696. [Google Scholar] [CrossRef] [PubMed]
- McCormick, J.B.; Fisher-Hoch, S.P. Lassa Fever. In Arenaviruses I: The Epidemiology, Molecular and Cell Biology of Arenaviruses; Oldstone, M.B.A., Ed.; Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2002; pp. 75–109. ISBN 978-3-642-56029-3. [Google Scholar]
- The 1000 Genomes Project Consortium. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassa Fever. CDC. Available online: https://www.cdc.gov/vhf/lassa/index.html (accessed on 31 May 2021).
- Baize, S.; Pannetier, D.; Oestereich, L.; Rieger, T.; Koivogui, L.; Magassouba, N.; Soropogui, B.; Sow, M.S.; Keïta, S.; De Clerck, H.; et al. Emergence of Zaire Ebola Virus Disease in Guinea. N. Engl. J. Med. 2014, 371, 1418–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gire, S.K.; Stremlau, M.; Andersen, K.G.; Schaffner, S.F.; Bjornson, Z.; Rubins, K.; Hensley, L.; McCormick, J.B.; Lander, E.S.; Garry, R.F.; et al. Emerging Disease or Diagnosis? Science 2012, 338, 750–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ultra-Secure Lab in Gabon Equipped for Ebola Studies|Voice of America—English. Available online: https://www.voanews.com/africa/ultra-secure-lab-gabon-equipped-ebola-studies (accessed on 8 July 2021).
- Omilabu, S.A.; Badaru, S.O.; Okokhere, P.; Asogun, D.; Drosten, C.; Emmerich, P.; Becker-Ziaja, B.; Schmitz, H.; Günther, S. Lassa Fever, Nigeria, 2003 and 2004. Emerg. Infect. Dis. 2005, 11, 1642–1644. [Google Scholar] [CrossRef] [PubMed]
- Asogun, D.A.; Adomeh, D.I.; Ehimuan, J.; Odia, I.; Hass, M.; Gabriel, M.; Ölschläger, S.; Becker-Ziaja, B.; Folarin, O.; Phelan, E.; et al. Molecular Diagnostics for Lassa Fever at Irrua Specialist Teaching Hospital, Nigeria: Lessons Learnt from Two Years of Laboratory Operation. PLoS Negl. Trop. Dis. 2012, 6, e1839. [Google Scholar] [CrossRef] [PubMed]
- Sabeti, P.C. How Africa Is Fighting Back against Ebola. Available online: https://www.weforum.org/agenda/2014/05/fighting-ebola-forum-africa-2014/ (accessed on 31 May 2021).
- Andersen, K.G.; Shapiro, B.J.; Matranga, C.B.; Sealfon, R.; Lin, A.E.; Moses, L.M.; Folarin, O.A.; Goba, A.; Odia, I.; Ehiane, P.E.; et al. Clinical Sequencing Uncovers Origins and Evolution of Lassa Virus. Cell 2015, 162, 738–750. [Google Scholar] [CrossRef] [Green Version]
- Fisher-Hoch, S.P.; Khan, J.A.; Rehman, S.; Mirza, S.; Khurshid, M.; McCormick, J.B. Crimean Congo-Haemorrhagic Fever Treated with Oral Ribavirin. Lancet 1995, 346, 472–475. [Google Scholar] [CrossRef]
- 2014–2016 Ebola Outbreak in West Africa. CDC. Available online: https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/index.html (accessed on 31 May 2021).
- Diehl, W.E.; Lin, A.E.; Grubaugh, N.D.; Carvalho, L.M.; Kim, K.; Kyawe, P.P.; McCauley, S.M.; Donnard, E.; Kucukural, A.; McDonel, P.; et al. Ebola Virus Glycoprotein with Increased Infectivity Dominated the 2013–2016 Epidemic. Cell 2016, 167, 1088–1098.e6. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.K.; Lim, S.-Y.; Lee, S.M.; Cunningham, J.M. Biochemical Basis for Increased Activity of Ebola Glycoprotein in the 2013–16 Epidemic. Cell Host Microbe 2017, 21, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Marzi, A.; Chadinah, S.; Haddock, E.; Feldmann, F.; Arndt, N.; Martellaro, C.; Scott, D.P.; Hanley, P.W.; Nyenswah, T.G.; Sow, S.; et al. Recently Identified Mutations in the Ebola Virus-Makona Genome Do Not Alter Pathogenicity in Animal Models. Cell Rep. 2018, 23, 1806–1816. [Google Scholar] [CrossRef] [Green Version]
- About Us. ACEGID 2020. Available online: https://acegid.org/about-us/ (accessed on 31 May 2021).
- Munshi, N. Christian Happi: ‘With Pathogens, We Need to Play Offence’. Financial Times. 2021. Available online: https://www.ft.com/content/16c8d40f-39eb-496a-8f0f-e6761a10bbeb (accessed on 31 May 2021).
- Siliezar, J. Responding to This Pandemic, Preparing for the Next. Harvard Gazette. 2020. Available online: https://news.harvard.edu/gazette/story/2020/05/pardis-sabetis-work-on-infectious-disease-coronavirus/ (accessed on 31 May 2021).
- Ackerman, C.M.; Myhrvold, C.; Thakku, S.G.; Freije, C.A.; Metsky, H.C.; Yang, D.K.; Ye, S.H.; Boehm, C.K.; Kosoko-Thoroddsen, T.-S.F.; Kehe, J.; et al. Massively Multiplexed Nucleic Acid Detection with Cas13. Nature 2020, 582, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Myhrvold, C.; Freije, C.A.; Gootenberg, J.S.; Abudayyeh, O.O.; Metsky, H.C.; Durbin, A.F.; Kellner, M.J.; Tan, A.L.; Paul, L.M.; Parham, L.A.; et al. Field-Deployable Viral Diagnostics Using CRISPR-Cas13. Science 2018, 360, 444–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botti-Lodovico, Y.; Nair, P.; Nosamiefan, D.; Stremlau, M.; Schaffner, S.; Agignoae, S.V.; Aiyepada, J.O.; Ajogbasile, F.V.; Akpede, G.O.; Alhasan, F.; et al. The Origins and Future of Sentinel: An Early-Warning System for Pandemic Preemption and Response. Viruses 2021, 13, 1605. https://doi.org/10.3390/v13081605
Botti-Lodovico Y, Nair P, Nosamiefan D, Stremlau M, Schaffner S, Agignoae SV, Aiyepada JO, Ajogbasile FV, Akpede GO, Alhasan F, et al. The Origins and Future of Sentinel: An Early-Warning System for Pandemic Preemption and Response. Viruses. 2021; 13(8):1605. https://doi.org/10.3390/v13081605
Chicago/Turabian StyleBotti-Lodovico, Yolanda, Parvathy Nair, Dolo Nosamiefan, Matthew Stremlau, Stephen Schaffner, Sebastian V. Agignoae, John Oke Aiyepada, Fehintola V. Ajogbasile, George O. Akpede, Foday Alhasan, and et al. 2021. "The Origins and Future of Sentinel: An Early-Warning System for Pandemic Preemption and Response" Viruses 13, no. 8: 1605. https://doi.org/10.3390/v13081605
APA StyleBotti-Lodovico, Y., Nair, P., Nosamiefan, D., Stremlau, M., Schaffner, S., Agignoae, S. V., Aiyepada, J. O., Ajogbasile, F. V., Akpede, G. O., Alhasan, F., Andersen, K. G., Asogun, D. A., Ayodeji, O. O., Badiane, A. S., Barnes, K., Bauer, M. R., Bell-Kareem, A., Benard, M. E., Benevolence, E. O., ... Happi, C. (2021). The Origins and Future of Sentinel: An Early-Warning System for Pandemic Preemption and Response. Viruses, 13(8), 1605. https://doi.org/10.3390/v13081605