
Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective



Abstract
1. Introduction
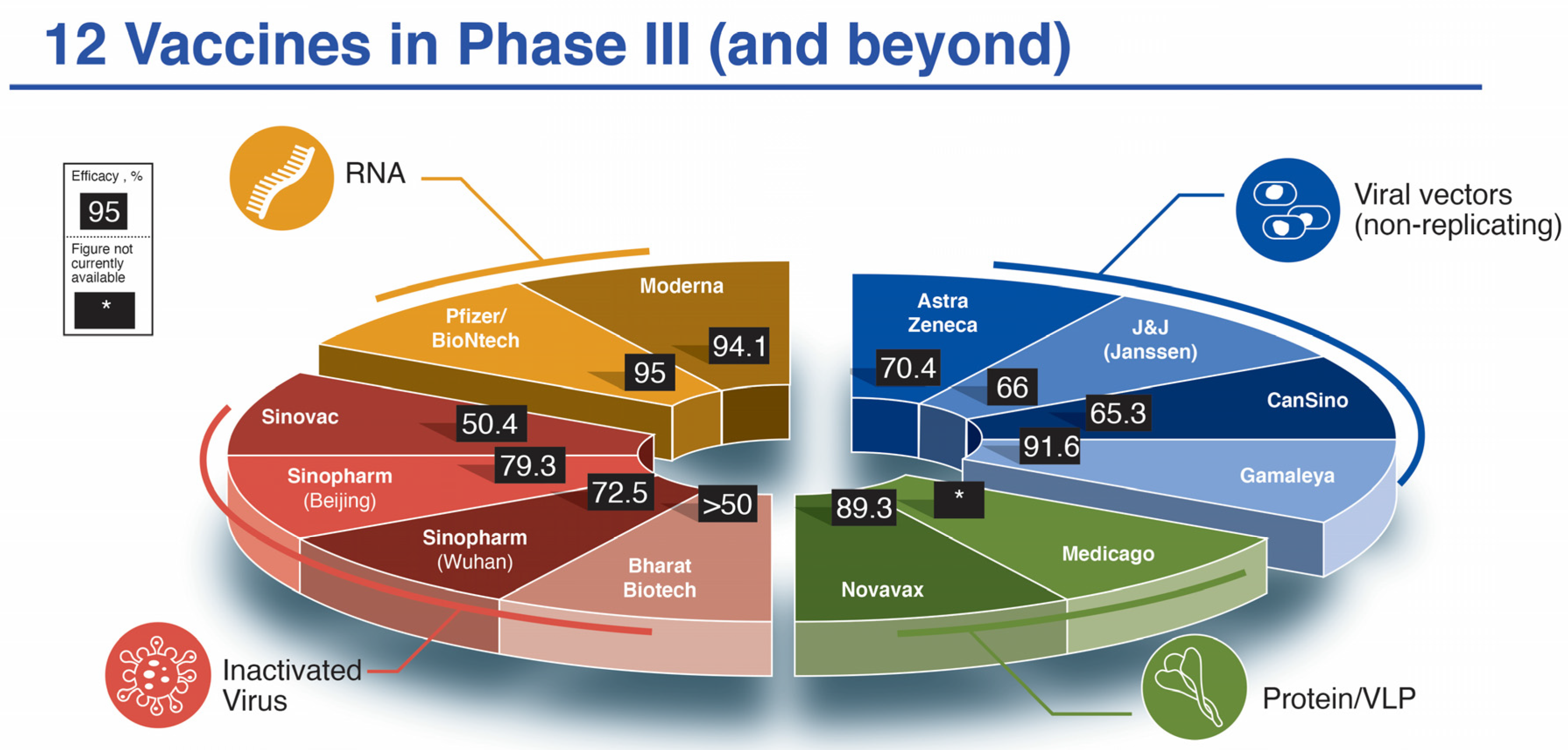
2. Overview of Twelve Vaccines Targeting COVID-19 in Phase III Clinical Trials

{kind=link}
{kind=link}
{kind=link}
| Platform [Ref.] | Name (Dose) | Phase III # Enrolled Placebo | Phase III # Enrolled Vaccine | COVID Cases Placebo (Severe) | COVID Cases Vaccine (Severe) | % Efficacy (Severe) | Projected Cost/Dose (USD) |
|---|---|---|---|---|---|---|---|
| RNA | |||||||
| Pfizer/BioNTech [16] | BNT162b2 (2 × 30 μg, 21 days apart) | 21,720 | 21,728 | 162 (9) | 8 (1) | 95 (89) | $14.70–19.50 |
| Moderna [17] | mRNA-1273 (2 × 100 μg, 28 days apart) | 15,210 | 15,210 | 185 (30) | 11 (0) | 94.1 (100) | $25–37 |
| Viral Vector | |||||||
| Astra Zeneca a [18] | AZD1222 (2 × 5×1010 vp, 28 days apart) (2.2 × 1010 vp, then 5 × 1010 28 days apart) | 4455 [1374] | 4440 [1367] | 71 [30] (10/2) | 27 [3] (0/0) | 62.1 (70.4) [90] (100) | $2–10+ |
| CanSino b | Ad5-nCoV (Convidecia) (single dose 5 × 1010 vp) | 30,000 (Pakistan) | --- | --- | 65.37 (91) | $ < 4 | |
| Gamaleya c [19] | Sputnik V (Gam-COVID-Vac) (1011 vp rAd26-S, followed by 1011 vp rAd5-S 21 days apart) | 5476 | 16,501 | 62 | 16 | 91.6 | $ < 10 |
| J&J (Janssen) d | Ad26.COV2.S (single dose 5 × 1010 vp) | 19,178 | 19,306 | 193 (34) | 66 (5) | 66 (85.4) | $2.80–9 |
| Protein/VLP | |||||||
| Novavax e | NVX-CoV2373 (2 × 5 μg + 50 μg M1 adjuvant, 21 days apart) | 15,000+ (UK) | 56 (1) | 6 (0) | 89.3 (UK) | $16 | |
| Medicago f | CoVLP (2 × 3.75 μg + AS03 GSK adjuvant, 21 days apart) | 30,000 | ---- | --- | --- | Not known | |
| Inactivated | |||||||
| Sinovac g | CoronaVac (2× alum-adjuvanted 14 days apart) | 9200 (Brazil) | 167 (31) | 85 (7) | 50.4 (Brazil) | $30 | |
| Sinopharm h (Beijing) | BBIBP-CorV (2 × 4 μg in alum adjuvant 21 days apart) | 10,000 (UAE) | ---- | --- | 79.3 (UAE) | $30–72.50 | |
| Sinopharm i (Wuhan) | Vero (2 × 5 μg in alum adjuvant 21 days apart) | 27,000 (Peru, UAE, Bahrain, Morocco, Argentina, Jordan and Pakistan) | --- | --- | 72.5% | $30–72.50 | |
| Bharat Biotech j | COVAXIN (BBV152) (2 × 6 μg in Alhydroxiquim-II adjuvant 28 days apart) | 25,800 | --- | --- | >50% | $2–3 | |
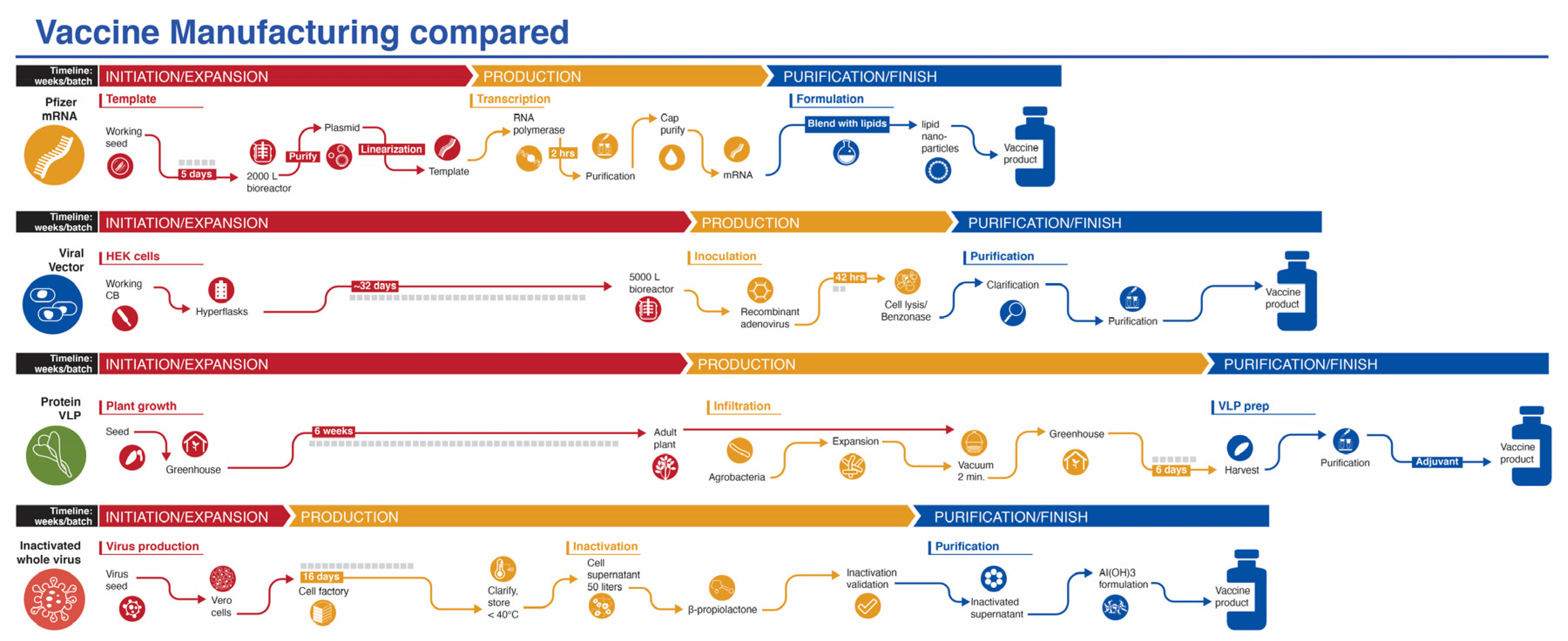
2.1. Messenger RNA (mRNA) Vaccines
2.2. Viral Vector-Based (Non-Replicating) Vaccines
2.3. Recombinant Protein-Based Vaccines
2.4. Inactivated Virus
3. Clinical Trial Data of Twelve Vaccines Targeting COVID-19 in Phase III Trials and Emergency Use Authorization
3.1. mRNA Vaccines—Safety/Reactogenicity and Immunogenicity/Efficacy
| Dose | N | Injection Site Pain | Headache | Fever | ||||
|---|---|---|---|---|---|---|---|---|
| Grade | Any | Any | Oral ≥ 38 °C | |||||
| Group | Placebo + Vaccine | Placebo | Vaccine | Placebo | Vaccine | Placebo | Vaccine | |
| mRNA | ||||||||
| Pfizer/BioNTech BNT162b2 (2 × 30 μg, 21 d.a.) [16,43] | Post dose 1 | ~8183 a | 12% | 78% | 27% | 35% | 0.6% | 3% |
| Post dose 2 | ~8183 a | 10% | 73% | 20% | 47% | 0% | 14% | |
| Moderna mRNA-1273 (2 × 100 μg, 28 d.a.) [17,22,44] | Post dose 1 | ~30,300 b | 17.5% | 83.7% | 26.6% | 32.7% | 0.3% | 0.8% |
| Post dose 2 | ~29,200 b | 17.0% | 88.2% | 23.4% | 58.6% | 0.3% | 15.5% | |
| Viral Vector | ||||||||
| Astra Zeneca AZD1222 (2 × 5 × 1010 vp, 28 d.a.) [18,25,26] | Post dose 1 | 964 c | 37% | 67% | 41% | 68% | 2% | 18% |
| Post dose 2 | 128 d | --- | 30.7% | --- | % | --- | 0% | |
| CanSino Ad5-nCoV (single dose 5 × 1010 vp) [28,29] | Post dose 1 | 255 e | 9% | 56% | 13% | 28% | 10% f | 16% f |
| Post dose 2 | NA | NA | NA | NA | NA | NA | NA | |
| Gamaleya Sputnik V (1011 vp Ad26 then 1011 Ad5 21 d.a.) [30] | Post dose 1 | 9 g | --- | 78% | --- | 67% | --- | 89% h |
| Post dose 2 | 20 g | --- | 40% | --- | 55% | --- | 100% h | |
| J&J (Janssen) (Ad26.COV2.S single 5 × 1010 vp) [21,49] | Post dose 1 | 673 j | 16.7% | 48.7% | 23.9% | 39.2% | 0.9% | 9.1% |
| Post dose 2 | NA | NA | NA | NA | NA | NA | NA | |
| Protein/VLP | ||||||||
| Novavax NVX-CoV2373 (2 × 5 μg+ 50 μg M1, 21 d.a.) [34] | Post dose 1 | 49 k | 13% | 38% | 31% | 23% | 0% | 0% |
| Post dose 2 | 49 k | 10% | 58% | 29% | 47% | 0% | 0% | |
| Medicago CoVLP 2 × 3.75 μg+ AS03, 21 d.a. [35] | Post dose 1 | 20 m | --- | 95% | --- | 30% | --- | 0% |
| Post dose 2 | 19 m | --- | 100% | --- | 57.9% | --- | 36.8% | |
| Inactivated | ||||||||
| Sinovac CoronaVac (2 × 3 µg + alum 14 d.a.) [36,37] | Post dose 1 | 180 p | 10% | 9.2% | 1.7% | 0.8% | 1.7% | 2.5% |
| Post dose 2 | 180 p | 3.3% | 13.6% | 0% | 0.8% | 0% | 1.7% | |
| Sinopharm BBIBP-CorV (2 × 4 μg vp + alum, 21 d.a.) [38] | Post dose 1 or 2 q | 112 | 4% | 12% | 7% | 1% | 4% | 4% |
| Post dose 2 | --- | --- | --- | --- | --- | --- | --- | |
| Sinopharm (Wuhan) Unnamed (2 × 5 μg vp + alum, 21 d.a.) [39] | Post dose 1 | 112 r | 14.3% | 6.0% | 0% | 0% | 3.6% | 1.2% |
| Post dose 2 | 112 r | 10.7% | 9.5% | 0% | 0% | 0% | 1.2% | |
| Bharat Biotech COVAXIN (2 × 6 μg Alhydroxiquim-II 28 d.a.) [42] | Post dose 1 | 175 s | --- | 3.2% | --- | 0.5% | --- | 4.2% |
| Post dose 2 | 175 s | --- | 2.6% | --- | 1.5% | --- | 2.1% | |
| Timing | N | ELISA Titer | Virus Neutralization | γ-IFN+ CD4+ T Cells | Th1/Th2 CD4+ T cells | |||
|---|---|---|---|---|---|---|---|---|
| Units | dpd = Days Post Dose | GMT IgG | GMT = Geometric Mean Titer | %+ | Ratio of Measure | |||
| Group | P + V | Placebo | Vaccine | Placebo | Vaccine | Vaccine | Vaccine | |
| mRNA | ||||||||
| Pfizer/BioNTech BNT162b2 (2 × 30 μg, 21 d.a.) [16,43] | 21 dpd 1 | ~30 a | 0.8 | 665.7 c | 10.0 | 13.0 d | --- | --- |
| 31 dpd 2 | 360 b | 0.8 | 4931.7 a,c | 10.0 | 316.1 d | 0.08% e | 4.4 f | |
| Moderna mRNA-1273 (2 × 100 μg, 28 d.a.) [22,44] | 29 dpd 1 | ~180 g | 5.80 | 25.23 | 21.0 | 149.3 h | 0.02% j | >>1 j |
| 28 dpd 2 | ~180 g | 5.86 | 147.42 | 21.2 | 1095.8 h | 0.09% j | 28.5 j | |
| Viral Vector | ||||||||
| Astra Zeneca AZD1222 (2 × 5 × 1010 vp, 28 d.a.) [18,25,26,27] | 28 dpd 1 | 127 | 1 k | 546 k | 23.9 m, | 203.2 m | 0.06% p | 6.3 q |
| 28 dpd 2 | 112 | --- | 10,691 n | --- | 128 n | 0.097% n | --- | |
| CanSino Ad5-nCoV (single dose 5 × 1010 vp) [28,29] | 28 dpd 1 | 255 | 20 r | 571 r | 4 s | 18.3 s | 0.01% t | --- |
| NA | NA | NA | NA | NA | NA | NA | NA | |
| Gamaleya Gam-COVID-Vac (1 × 1011 vp Ad26 then Ad5 21 d.a.a) [19,30] | 21 dpd 1 | 9 | 12.5 u | 1721 u | 1.25 v,w | 4.2 v | --- x | --- x |
| 21 dpd 2 | 456 | --- | 8996 u | 1.6 v | 44.5 v | --- | --- | |
| J&J (Janssen) (Ad26.COV2.S single dose 5 × 1010 vp) [21,49] | 29 dpd 1 | ~314 | <50 | 399 y | <58 | 241 z | 0.09% α | 10 β |
| NA | NA | NA | NA | NA | NA | NA | NA | |
| Protein/VLP | ||||||||
| Novavax NVX-CoV2373 (2 × 5 μg + 50 μg M1, 21 d.a.) [34] | 21 dpd 1 | ~52 | 110 δ | 1984 δ | 20 ε | 103 ε | --- | --- |
| 14 dpd 2 | ~50 | 114 δ | 63,160 δ | 20 ε | 3906 ε | 0.18% ζ | 7.5 ζ | |
| Medicago CoVLP (2 × 3.75 μg + AS03, 21 d.a.) [35] | 21 dpd 1 | 20 | 64.8 w,η | 4354 η | 5 w,θ | 29.3 θ | 0.01% λ | 2.37 λ |
| 21 dpd 2 | 19 | --- | 295,240 η | --- | 811.3 θ | 0.06% λ | 1.4 λ | |
| Inactivated | ||||||||
| Sinovac CoronaVac (2 × 3 µg + alum, 14 d.a.) [36,37] | 14 dpd 2 | 176 ξ | 81 | 1094.3 | 2.0 | 27.6 | 0.00% π | --- |
| 28 dpd 2 | 176 ξ | 80 | 1053.7 | 2.0 | 23.8 | 0.07% π | --- | |
| Sinopharm (Beijing) BBIBP-CorV 2 × 4 μg vp + alum, 21 d.a. [38] | 14 dpd 1 ς | 112 | --- | --- | 2 | 219 | --- | --- |
| 28 dpd 2 ς | 112 | --- | --- | 2 | 282 | --- | --- | |
| Sinopharm (Wuhan) Unnamed 2 × 5 μg vp + alum, 21 d.a. [39] | 14 dpd 1 σ | 56 | --- | --- | --- | --- | --- | 0.92 φ |
| 14 dpd 2 σ | 56 | 10 | 215 | 5 | 247 | 1.21 φ | ||
| Bharat Biotech COVAXIN (2 × 6 μg in Alhydroxiquim-II adjuvant, 28 d.a.) [40,41,42] | 28 dpd 1 ψ | 190 | 500 w | 2240 | 5.6 w | 12.8 | --- | --- |
| 28 dpd 2 ψ | 190 | --- | 9541 | --- | 160 | --- | 42 ω | |
3.2. Viral Vector-Based (Non-Replicating) Vaccines—Safety/Reactogenicity and Immunogenicity/Efficacy
3.3. Protein-Based Vaccines—Safety/Reactogenicity and Immunogenicity/Efficacy
3.4. Inactivated Viral Vaccines—Safety/Reactogenicity and Efficacy/Immunogenicity
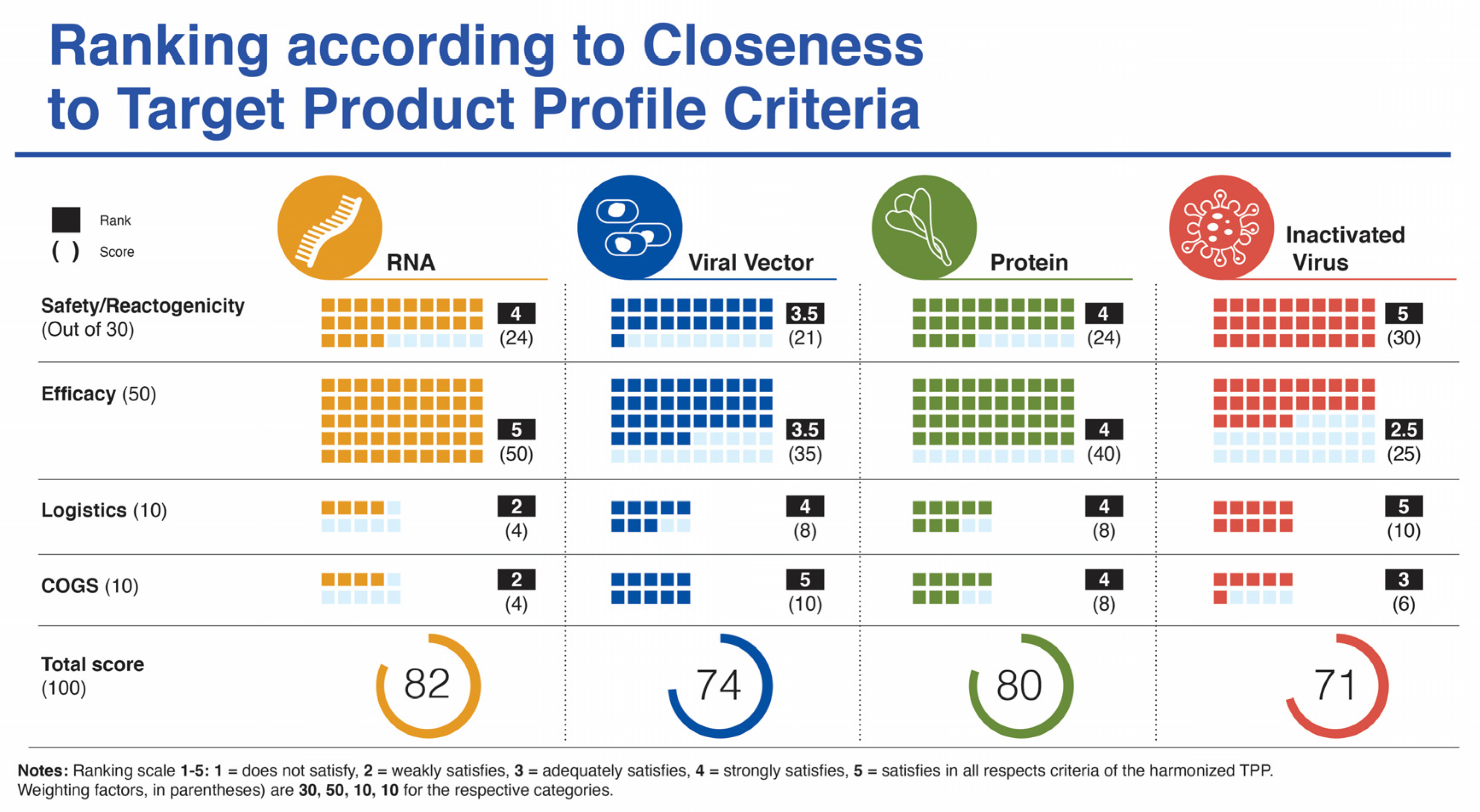
4. Comparative Analysis of Target Product Profiles
4.1. Safety/Reactogenicity—A SARS-CoV-2 Vaccine Should Provide a Clear Benefit/Risk Profile Based on 2+ Data Sets with at Least 10,000 Subjects across All Age Groups with the Dosing Regimen Intended for Licensure
4.2. Vaccine Efficacy—A SARS-CoV-2 Vaccine Should Demonstrate at Least 70% Efficacy, with Rapid Onset of Protection (<2 Weeks from Initial Dose), across All Age Groups, from Adolescents to Elderly with Appropriate Evaluation of Humoral and Cellular Immune Responses to Provide a Minimum Serological Correlate of Protection
4.3. Compliance (Relating to Dosing Regimen)—A Sars-Cov-2 Vaccine Should Be a Single Dose during an Outbreak (Optimal). A Two-Dose Regimen Is Acceptable Provided There Is a Short Interval (<28 Days) between Prime and Boost (Minimal)
4.4. Logistics (Product Stability/Storage/Supply Chain)—A SARS-CoV-2 Vaccine Should Have a Shelf Life of at Least 1 Year at −70 °C and Be Stable for at Least 1 Month at Fridge Temperature (4 °C)
4.5. COGS (Target Price/Accessibility)—A SARS CoV-2 Vaccine Should Possess Capability for Rapid Scale-Up Production and Availability of Sufficient Doses at Cost/Dose That Allows Broad Use, Including in LMIC
5. Discussion
5.1. Successes
5.2. Barriers/Hurdles
5.3. Limitations of This Analysis
5.4. Concluding Remarks
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ahn, D.G.; Shin, H.J.; Kim, M.H.; Lee, S.; Kim, H.S.; Myoung, J.; Kim, B.T.; Kim, S.J. Current Status of Epidemiology, Diagnosis, Therapeutics, and Vaccines for Novel Coronavirus Disease 2019 (COVID-19). J. Microbiol. Biotechnol. 2020, 30, 313–324. [Google Scholar] [CrossRef]
- Amanat, F.; Krammer, F. SARS-CoV-2 Vaccines: Status Report. Immunity 2020, 52, 583–589. [Google Scholar] [CrossRef]
- Callaway, E. Scores of coronavirus vaccines are in competition-how will scientists choose the best? Nature 2020. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Cohen, J. Vaccine designers take first shots at COVID-19. Science 2020, 368, 14–16. [Google Scholar] [CrossRef]
- Cyranoski, D. Profile of a killer: The complex biology powering the coronavirus pandemic. Nature 2020, 581, 22–26. [Google Scholar] [CrossRef]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical Features of 85 Fatal Cases of COVID-19 from Wuhan. A Retrospective Observational Study. Am. J. Respir. Crit. Care Med. 2020, 201, 1372–1379. [Google Scholar] [CrossRef]
- Graham, B.S. Rapid COVID-19 vaccine development. Science 2020, 368, 945–946. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Oberfeld, B.; Achanta, A.; Carpenter, K.; Chen, P.; Gilette, N.M.; Langat, P.; Said, J.T.; Schiff, A.E.; Zhou, A.S.; Barczak, A.K.; et al. SnapShot: COVID-19. Cell 2020, 181, 954. [Google Scholar] [CrossRef]
- Le, T.T.; Andreadakis, Z.; Kumar, A.; Román, G.R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Funk, C.D.; Laferrière, C.; Ardakani, A. A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic. Front. Pharmacol. 2020, 11, 937. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V.; Tukhvatullin, A.I.; Shcheblyakov, D.V.; Dzharullaeva, A.S.; Grousova, D.M.; Erokhova, A.S.; Kovyrshina, A.V.; Botikov, A.G. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, P671–P681. [Google Scholar] [CrossRef]
- Voysey, M.; Costa Clemens, S.A.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.J.; Baillie, V.; Barnabas, S.L.; Bhorat, Q.E. Single Dose Administration, and the Influence of the Timing of the Booster Dose on Immunogenicity and Efficacy Of ChAdOx1 nCoV-19 (AZD1222) Vaccine. Lancet 2021. Available online: https://ssrn.com/abstract=3777268 (accessed on 9 February 2021). [CrossRef]
- Janssen. COVID-19 Vaccine Ad26.COV2.S VAC31518 (JNJ-78436735) Sponsor Briefing Document Vaccines and Related Biological Products Advisory Committee 26 February 2021. Available online: https://www.fda.gov/media/146219/download (accessed on 26 February 2021).
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Editorial. Messengers of hope. Nat. Biotechnol. 2021, 39, 1. [Google Scholar] [CrossRef] [PubMed]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Zhu, F.C.; Guan, X.H.; Li, Y.H.; Huang, J.Y.; Jiang, T.; Hou, L.H.; Li, J.X.; Yang, B.F.; Wang, L.; Wang, W.J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V.; Tukhvatullin, A.I.; Shcheblyakov, D.V.; Dzharullaeva, A.S.; Grousova, D.M.; Erokhova, A.S.; Kovyrshina, A.V.; Botikov, A.G.; et al. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: Two open, non-randomised phase 1/2 studies from Russia. Lancet 2020, 396, 887–897. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1-2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Ledford, H. Oxford COVID-vaccine paper highlights lingering unknowns about results. Nature 2020, 588, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H.; et al. Phase 1-2 Trial of a SARS-CoV-2 Recombinant Spike Protein Nanoparticle Vaccine. N. Engl. J. Med. 2020, 383, 2320–2332. [Google Scholar] [CrossRef]
- Ward, B.J.; Gobeil, P.; Seguin, A.; Atkins, J.; Boulay, I.; Charbonneau, P.-Y.; Couture, M.; D’Aoust, M.-A.; Dhaliwall, J.; Finkle, C. Phase 1 trial of a Candidate Recombinant Virus-Like Particle Vaccine for Covid-19 Disease Produced in Plants. Medrxiv Prepr. Serv. Health Sci. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.11.04.20226282v1 (accessed on 9 February 2021).
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 181–192. [Google Scholar] [CrossRef]
- Palacios, R.; Patiño, E.G.; de Oliveira Piorelli, R.; Conde, M.; Batista, A.P.; Zeng, G.; Xin, Q.; Kallas, E.G.; Flores, J.; Ockenhouse, C.F.; et al. Double-Blind, Randomized, Placebo-Controlled Phase III Clinical Trial to Evaluate the Efficacy and Safety of treating Healthcare Professionals with the Adsorbed COVID-19 (Inactivated) Vaccine Manufactured by Sinovac—PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 853. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Xia, S.; Duan, K.; Zhang, Y.; Zhao, D.; Zhang, H.; Xie, Z.; Li, X.; Peng, C.; Zhang, Y.; Zhang, W.; et al. Effect of an Inactivated Vaccine Against SARS-CoV-2 on Safety and Immunogenicity Outcomes: Interim Analysis of 2 Randomized Clinical Trials. JAMA 2020, 324, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Ganneru, B.; Jogdand, H.; Daram, V.K.; Molugu, N.R.; Prasad, S.D.; Kannappa, S.V.; Ella, K.M.; Ravikrishnan, R.; Awasthi, A.; Jose, J. Evaluation of Safety and Immunogenicity of an Adjuvanted, TH-1 Skewed, Whole Virion Inactivated SARS-CoV-2 Vaccine-BBV152. iScience 2020. [Google Scholar] [CrossRef]
- Ella, R.; Mohan, K.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.K.; Ganneru, B.; Sapkal, G.; Yadav, P.; Panda, S. Safety and immunogenicity trial of an inactivated SARS-CoV-2 vaccine-BBV152: A phase 1, double-blind, randomised control trial. Medrxiv Prepr. Serv. Health Sci. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.12.11.20210419v1 (accessed on 9 February 2021).
- Ella, R.; Reddy, S.; Jogdand, H.; Sarangi, V.; Ganneru, B.; Prasad, S.; Das, D.; Raju, D.; Praturi, U.; Sapkal, G.; et al. Safety and immunogenicity clinical trial of an inactivated SARS-CoV-2 vaccine, BBV152 (a phase 2, double-blind, randomised controlled trial) and the persistence of immune responses from a phase 1 follow-up report. Medrxiv Prepr. Serv. Health Sci. 2020. [Google Scholar] [CrossRef]
- Pfizer. Pfizer-Biontech COVID-19 Vaccine (BNT162, PF-07302048) Vaccines and Related Biological Products Advisory Committee Briefing Document. 2020. Available online: https://www.fda.gov/media/144246/download (accessed on 9 February 2021).
- Moderna. MRNA-1273 Vaccines and Related Biological Products Advisory Committee Meeting Presentation 17 December 2020. 2020. Available online: https://www.fda.gov/media/144452/download (accessed on 9 February 2021).
- Monograph. Prevnar® 13, © Wyeth Canada, 21 December 2009. 2009. Available online: https://pdf.hres.ca/dpd_pm/00052583.PDF (accessed on 9 February 2021).
- Monograph. SHINGRIX Herpes Zoster Vaccine (Non-Live Recombinant, AS01B Adjuvanted) 13 October 2017. 2017. Available online: https://pdf.hres.ca/dpd_pm/00056533.PDF (accessed on 9 February 2021).
- Monograph. GARDASIL® 9 [Human Papillomavirus 9-Valent Vaccine, Recombinant] 5 February 2015. 2015. Available online: https://pdf.hres.ca/dpd_pm/00058026.PDF (accessed on 9 February 2021).
- Monograph. FLUVIRAL (2020–2021) Trivalent Influenza Vaccine (Split Virion, Inactivated) 6 February 2014. 2009. Available online: https://pdf.hres.ca/dpd_pm/00057995.PDF (accessed on 9 February 2021).
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I. Safety and immunogenicity of the Ad26. COV2. S COVID-19 vaccine candidate: Interim results of a phase 1/2a, double-blind, randomized, placebo-controlled trial. Medrxiv Prepr. Serv. Health Sci. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.09.23.20199604v1 (accessed on 26 February 2021).
- Shimabukuro, T.T. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine—United States, 14–23 December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7002e1.htm (accessed on 9 February 2021).
- Shimabukuro, T.T. Allergic Reactions including anaphylaxis after receipt of the first dose of Moderna COVID-19 vaccine—United States, 21 December 2020–10 January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef]
- de Vrieze, J. Pfizer’s vaccine raises allergy concerns. Science 2021, 371, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, J. Complement activation-related pseudoallergy: A stress reaction in blood triggered by nanomedicines and biologicals. Mol. Immunol. 2014, 61, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and T(H)1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Dolgin, E. Search for better COVID vaccines confounded by existing rollouts. Nature 2021, 589, 340–341. [Google Scholar] [CrossRef]
- Hervé, C.; Laupèze, B.; Del Giudice, G.; Didierlaurent, A.M.; Tavares Da Silva, F. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines 2019, 4, 39. [Google Scholar] [CrossRef]
- Bottazzi, M.E.; Strych, U.; Hotez, P.J.; Corry, D.B. Coronavirus vaccine-associated lung immunopathology-what is the significance? Microbes Infect. 2020, 22, 403–404. [Google Scholar] [CrossRef]
- Vasilakos, J.P.; Tomai, M.A. The use of Toll-like receptor 7/8 agonists as vaccine adjuvants. Expert Rev. Vaccines 2013, 12, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Monograph. ENGERIX-B Hepatitis B Vaccine (Recombinant) 6 November 1987. 1987. Available online: https://pdf.hres.ca/dpd_pm/00058559.PDF (accessed on 9 February 2021).
- Monograph. AREPANRIX™ H1N1 AS03-Adjuvanted H1N1 Pandemic Influenza Vaccine Emulsion for Injection, 20 April 2010. 2010. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/dhp-mps/alt_formats/pdf/prodpharma/legislation/interimorders-arretesurgence/prodinfo-vaccin-eng.pdf (accessed on 9 February 2021).
- Sedita, J.; Perrella, S.; Morio, M.; Berbari, M.; Hsu, J.S.; Saxon, E.; Jarrahian, C.; Rein-Weston, A.; Zehrung, D. Cost of goods sold and total cost of delivery for oral and parenteral vaccine packaging formats. Vaccine 2018, 36, 1700–1709. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168. [Google Scholar] [CrossRef]
- Wyllie, D.; Mulchandani, R.; Jones, H.E.; Taylor-Phillips, S.; Brooks, T.; Charlett, A.; Ades, A.E.; Makin, A.; Oliver, I.; Moore, P.; et al. SARS-CoV-2 responsive T cell numbers are associated with protection from COVID-19: A prospective cohort study in keyworkers. Medrxiv Prepr. Serv. Health Sci. 2020. [Google Scholar] [CrossRef]
- Romero-Steiner, S.; Frasch, C.; Concepcion, N.; Goldblatt, D.; Käyhty, H.; Väkeväinen, M.; Laferriere, C.; Wauters, D.; Nahm, M.H.; Schinsky, M.F.; et al. Multilaboratory evaluation of a viability assay for measurement of opsonophagocytic antibodies specific to the capsular polysaccharides of Streptococcus pneumoniae. Clin. Diagn. Lab. Immunol. 2003, 10, 1019–1024. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kupferschmidt, K. Fast-spreading U.K. virus variant raises alarms. Science 2021, 371, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmidt, K. Viral evolution may herald new pandemic phase. Science 2021, 371, 108–109. [Google Scholar] [CrossRef]
- Kupferschmidt, K. Vaccinemakers ponder how to adapt to virus variants. Science 2021, 371, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmidt, K. Vaccine 2.0: Moderna and Other Companies Plan Tweaks that Would Protect against New Coronavirus Mutations. Science 2021. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: What new variants are emerging and how are they being investigated? BMJ 2021, 372, n158. [Google Scholar] [CrossRef]
- Xie, X.; Zou, J.; Fontes-Garfias, C.R.; Xia, H.; Swanson, K.A.; Cutler, M.; Cooper, D.; Menachery, V.D.; Weaver, S.; Dormitzer, P.R.; et al. Neutralization of N501Y mutant SARS-CoV-2 by BNT162b2 vaccine-elicited sera. Biorxiv Prepr. Serv. Biol. 2021. [Google Scholar] [CrossRef]
- Muik, A.; Wallisch, A.K.; Sänger, B.; Swanson, K.A.; Mühl, J.; Chen, W.; Cai, H.; Maurus, D.; Sarkar, R.; Türeci, Ö.; et al. Neutralization of SARS-CoV-2 lineage B.1.1.7 pseudovirus by BNT162b2 vaccine-elicited human sera. Science 2021. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Liu, Y.; Liu, J.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Xia, H.; Swanson, K.A.; Cutler, M.; Cooper, D.; et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K, and N501Y variants by BNT162b2 vaccine-elicited sera. Biorxiv Prepr. Serv. Biol. 2021. [Google Scholar] [CrossRef]
- Mallapaty, S. Israel is first to see COVID-infection drop from vaccines. Nature 2021, 590, 197. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Funk, C.D.; Laferrière, C.; Ardakani, A. Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective. Viruses 2021, 13, 418. https://doi.org/10.3390/v13030418
Funk CD, Laferrière C, Ardakani A. Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective. Viruses. 2021; 13(3):418. https://doi.org/10.3390/v13030418
Chicago/Turabian StyleFunk, Colin D., Craig Laferrière, and Ali Ardakani. 2021. "Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective" Viruses 13, no. 3: 418. https://doi.org/10.3390/v13030418
APA StyleFunk, C. D., Laferrière, C., & Ardakani, A. (2021). Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective. Viruses, 13(3), 418. https://doi.org/10.3390/v13030418