Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature




Abstract
1. Introduction
2. Seroprevalence of IgG anti-HEV
2.1. Seroprevalence of IgG anti-HEV with Wantai HEV-IgG ELISA Assay
2.2. Meta-Analysis
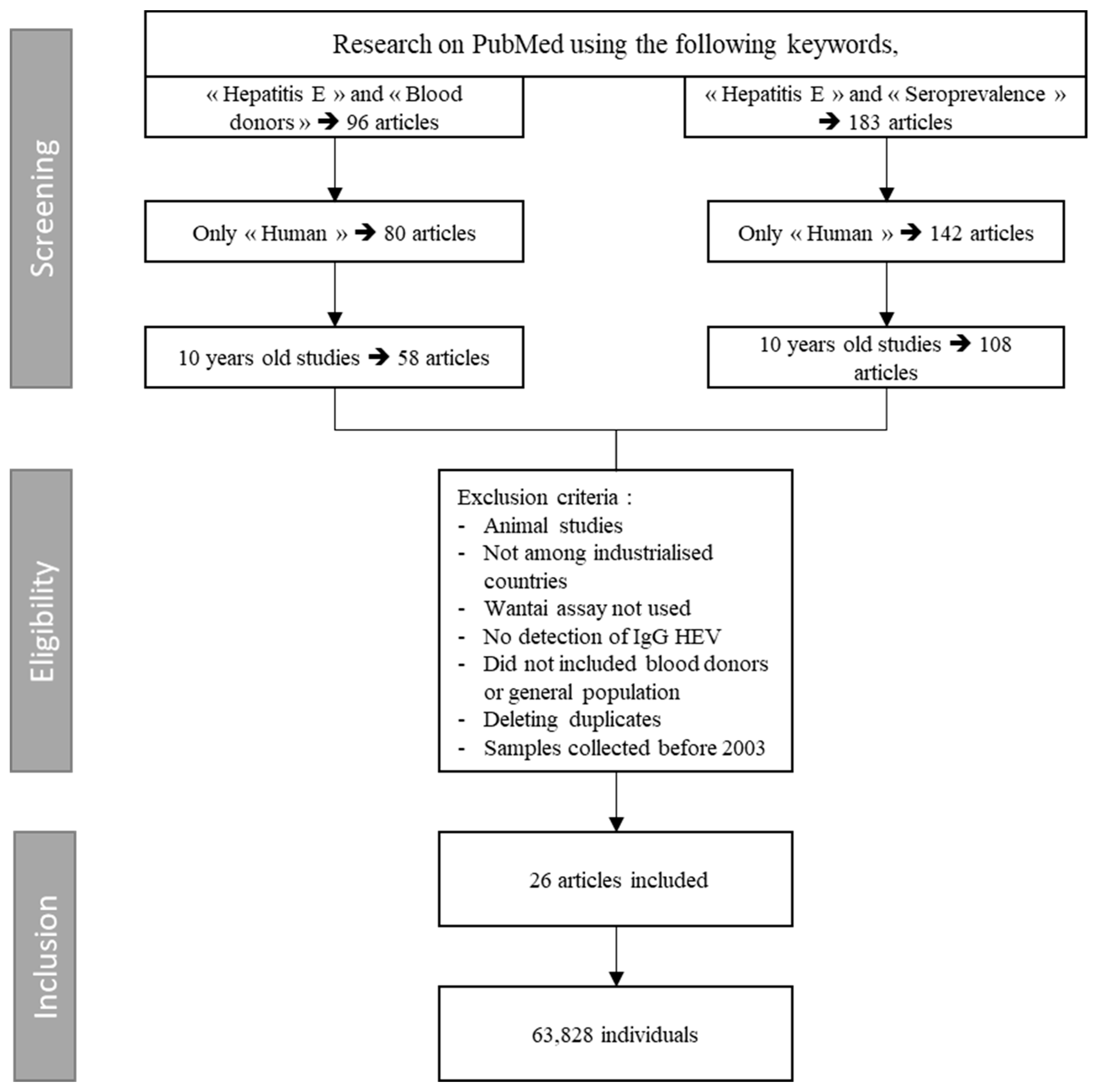
2.2.1. Literature Search, Selection Criteria, and Study Quality
2.2.2. Data Extraction
2.2.3. Statistical Analysis
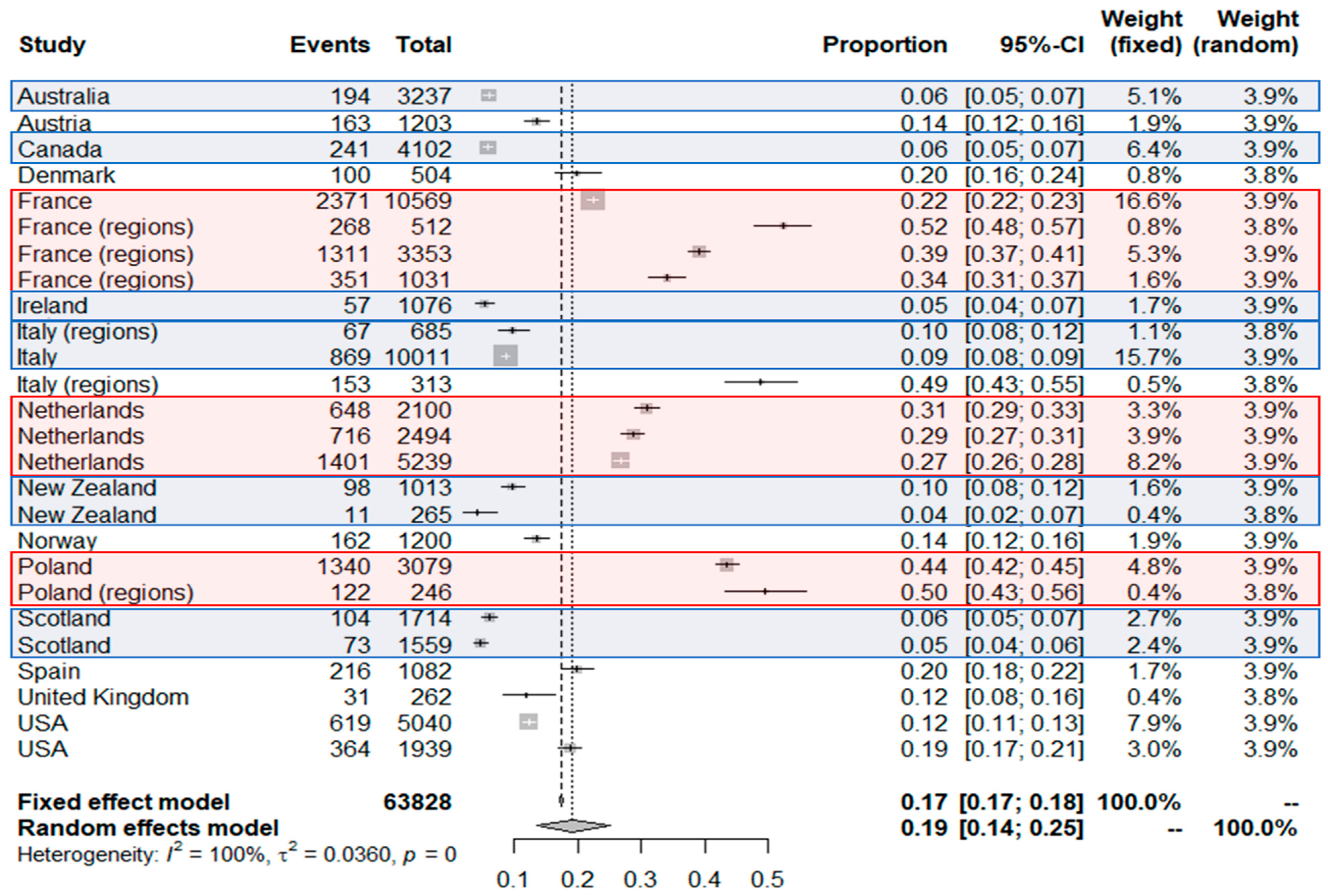
2.2.4. Results of Meta-Analysis: Human Seroprevalence of IgG anti-HEV
2.2.5. Interpretation of Meta-Analysis
2.3. High-Exposure Populations
2.4. Children
2.5. Other Seroprevalences Observed in Industrialized Countries
2.6. Characteristics Associated with Higher Seroprevalence
3. Outbreaks in High-Income Countries
3.1. Confirmed and Grouped Cases
3.2. Description of Outbreaks
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Debing, Y.; Moradpour, D.; Neyts, J.; Gouttenoire, J. Update on hepatitis e virology: Implications for clinical practice. J. Hepatol. 2016, 65, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Purcell, R.H.; Emerson, S.U. Hepatitis e: An emerging awareness of an old disease. J. Hepatol. 2008, 48, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H.R. Hepatitis e. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Dalton, H.R.; Bendall, R.; Ijaz, S.; Banks, M. Hepatitis e: An emerging infection in developed countries. Lancet Infect Dis. 2008, 8, 698–709. [Google Scholar] [CrossRef]
- Tam, A.W.; Smith, M.M.; Guerra, M.E.; Huang, C.C.; Bradley, D.W.; Fry, K.E.; Reyes, G.R. Hepatitis e virus (hev): Molecular cloning and sequencing of the full-length viral genome. Virology 1991, 185, 120–131. [Google Scholar] [CrossRef]
- Takahashi, M.; Tanaka, T.; Takahashi, H.; Hoshino, Y.; Nagashima, S.; Jirintai; Mizuo, H.; Yazaki, Y.; Takagi, T.; Azuma, M.; et al. Hepatitis e virus (hev) strains in serum samples can replicate efficiently in cultured cells despite the coexistence of hev antibodies: Characterization of hev virions in blood circulation. J. Clin. Microbiol. 2010, 48, 1112–1125. [Google Scholar] [CrossRef] [PubMed]
- Chapuy-Regaud, S.; Dubois, M.; Plisson-Chastang, C.; Bonnefois, T.; Lhomme, S.; Bertrand-Michel, J.; You, B.; Simoneau, S.; Gleizes, P.E.; Flan, B.; et al. Characterization of the lipid envelope of exosome encapsulated hev particles protected from the immune response. Biochimie 2017, 141, 70–79. [Google Scholar] [CrossRef]
- Nair, V.P.; Anang, S.; Subramani, C.; Madhvi, A.; Bakshi, K.; Srivastava, A.; Shalimar; Nayak, B.; Ranjith Kumar, C.T.; Surjit, M. Endoplasmic reticulum stress induced synthesis of a novel viral factor mediates efficient replication of genotype-1 hepatitis e virus. PLoS Pathog. 2016, 12, e1005521. [Google Scholar] [CrossRef]
- Smith, D.B. International committee on taxonomy of viruses hepeviridae study g, jameel s, emerson su, harrison tj, meng xj, okamoto h, van der poel wh, purdy ma. Consensus proposals for classification of the family hepeviridae. J. Gen. Virol. 2014, 95, 2223–2232. [Google Scholar] [CrossRef]
- Smith, D.B.; Simmonds, P.; Izopet, J.; Oliveira-Filho, E.F.; Ulrich, R.G.; Johne, R.; Koenig, M.; Jameel, S.; Harrison, T.J.; Meng, X.-J.; et al. Proposed reference sequences for hepatitis e virus subtypes. J. Gen. Virol. 2016, 97, 537–542. [Google Scholar] [CrossRef]
- Purdy, M.A.; Harrison, T.J.; Jameel, S.; Meng, X.J.; Okamoto, H.; Van der Poel, W.H.M.; Smith, D.B.; Ictv Report, C. Ictv virus taxonomy profile: Hepeviridae. J. Gen. Virol. 2017, 98, 2645–2646. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R. Clinical presentation of hepatitis e. Virus Res. 2011, 161, 15–22. [Google Scholar] [CrossRef]
- Echevarria, J.M. Light and darkness: Prevalence of hepatitis e virus infection among the general population. Scientifica (Cairo) 2014, 2014, 481016. [Google Scholar] [CrossRef]
- Said, B.; Ijaz, S.; Kafatos, G.; Booth, L.; Thomas, H.L.; Walsh, A.; Ramsay, M.; Morgan, D.; Hepatitis, E.I.I.T. Hepatitis e outbreak on cruise ship. Emerg. Infect. Dis. 2009, 15, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Hazeldine, S.; Banks, M.; Ijaz, S.; Bendall, R. Locally acquired hepatitis e in chronic liver disease. Lancet 2007, 369, 1260. [Google Scholar] [CrossRef]
- Colson, P.; Dhiver, C.; Gerolami, R. Hepatitis e virus as a newly identified cause of acute viral hepatitis during human immunodeficiency virus infection. Clin. Microbiol. Infect. 2008, 14, 1176–1180. [Google Scholar] [CrossRef] [PubMed]
- Abid, S.; Khan, A.H. Severe hemolysis and renal failure in glucose-6-phosphate dehydrogenase deficient patients with hepatitis e. Am. J. Gastroenterol. 2002, 97, 1544–1547. [Google Scholar] [CrossRef]
- Kamar, N.; Marion, O.; Abravanel, F.; Izopet, J.; Dalton, H.R. Extrahepatic manifestations of hepatitis e virus. Liver Int. 2016, 36, 467–472. [Google Scholar] [CrossRef]
- Hoofnagle, J.H.; Nelson, K.E.; Purcell, R.H. Hepatitis e. N. Engl. J. Med. 2012, 367, 1237–1244. [Google Scholar] [CrossRef]
- de Niet, A.; Zaaijer, H.L.; ten Berge, I.; Weegink, C.J.; Reesink, H.W.; Beuers, U. Chronic hepatitis e after solid organ transplantation. Neth. J. Med. 2012, 70, 261–266. [Google Scholar]
- Gerolami, R.; Moal, V.; Colson, P. Chronic hepatitis e with cirrhosis in a kidney-transplant recipient. N. Engl. J. Med. 2008, 358, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Te, H.S.; Drobeniuc, J.; Kamili, S.; Dong, C.; Hart, J.; Sharapov, U.M. Hepatitis e virus infection in a liver transplant recipient in the United States: A case report. Transplant Proc. 2013, 45, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Renou, C.; Lafeuillade, A.; Cadranel, J.F.; Pavio, N.; Pariente, A.; Allegre, T.; Poggi, C.; Penaranda, G.; Cordier, F.; Nicand, E. Hepatitis e virus in hiv-infected patients. AIDS 2010, 24, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Tavitian, S.; Peron, J.M.; Huynh, A.; Mansuy, J.M.; Ysebaert, L.; Huguet, F.; Vinel, J.P.; Attal, M.; Izopet, J.; Recher, C. Hepatitis e virus excretion can be prolonged in patients with hematological malignancies. J. Clin. Virol. 2010, 49, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Gauss, A.; Wenzel, J.J.; Flechtenmacher, C.; Navid, M.H.; Eisenbach, C.; Jilg, W.; Stremmel, W.; Schnitzler, P. Chronic hepatitis e virus infection in a patient with leukemia and elevated transaminases: A case report. J. Med. Case Rep. 2012, 6, 334. [Google Scholar] [CrossRef] [PubMed]
- Geng, Y.; Zhang, H.; Huang, W.; T, J.H.; Geng, K.; Li, Z.; Wang, Y. Persistent hepatitis e virus genotype 4 infection in a child with acute lymphoblastic leukemia. Hepat. Mon. 2014, 14, e15618. [Google Scholar] [CrossRef]
- Kamar, N.; Selves, J.; Mansuy, J.-M.; Ouezzani, L.; Péron, J.-M.; Guitard, J.; Cointault, O.; Esposito, L.; Abravanel, F.; Danjoux, M.; et al. Hepatitis e virus and chronic hepatitis in organ-transplant recipients. N. Engl. J. Med. 2008, 358, 811–817. [Google Scholar] [CrossRef]
- Péron, J.-M.; Mansuy, J.-M.; Récher, C.; Bureau, C.; Poirson, H.; Alric, L.; Izopet, J.; Vinel, J.-P. Prolonged hepatitis e in an immunocompromised patient. J. Gastroenterol. Hepatol. 2006, 21, 1223–1224. [Google Scholar] [CrossRef]
- Dalton, H.R.; Bendall, R.P.; Keane, F.E.; Tedder, R.S.; Ijaz, S. Persistent carriage of hepatitis e virus in patients with hiv infection. N. Engl. J. Med. 2009, 361, 1025–1027. [Google Scholar] [CrossRef]
- Behrendt, P.; Steinmann, E.; Manns, M.P.; Wedemeyer, H. The impact of hepatitis e in the liver transplant setting. J. Hepatol. 2014, 61, 1418–1429. [Google Scholar] [CrossRef]
- Tamura, A.; Shimizu, Y.K.; Tanaka, T.; Kuroda, K.; Arakawa, Y.; Takahashi, K.; Mishiro, S.; Shimizu, K.; Moriyama, M. Persistent infection of hepatitis e virus transmitted by blood transfusion in a patient with t-cell lymphoma. Hepatol. Res. 2007, 37, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.C.; Flower, R.L.; Seed, C.R.; Stramer, S.L.; Faddy, H.M. A comparative study of assay performance of commercial hepatitis e virus enzyme-linked immunosorbent assay kits in Australian blood donor samples. J. Blood Transfus. 2016, 2016, 9647675. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Jeong, S.H.; Kim, J.W.; Woo, B.H.; Lee, D.H.; Kim, H.Y.; Ahn, S. Seroprevalence of anti-hepatitis e virus (hev) in a korean population: Comparison of two commercial anti-hev assays. BMC Infect. Dis. 2012, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, J.J.; Preiss, J.; Schemmerer, M.; Huber, B.; Jilg, W. Test performance characteristics of anti-hev igg assays strongly influence hepatitis e seroprevalence estimates. J. Infect. Dis. 2013, 207, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Du, H.; Wang, Y. Comparison of two diagnostic reagents to detect anti-hepatitis e virus igg antibodies. Chin. J. Zoon. 2008, 24, 1087–1089. [Google Scholar]
- Beijing Wantai Biological Pharmacy Enterprise Co., Ltd. Wantai HEV-IgM ELISA. Available online: http://wantaibio.company.weiku.com/item/HEV-IgM-Elisa-kit-18043455.html (accessed on 3 December 2018).
- Rossi-Tamisier, M.; Moal, V.; Gerolami, R.; Colson, P. Discrepancy between anti-hepatitis e virus immunoglobulin g prevalence assessed by two assays in kidney and liver transplant recipients. J. Clin. Virol. 2013, 56, 62–64. [Google Scholar] [CrossRef]
- Hartl, J.; Otto, B.; Madden, R.G.; Webb, G.; Woolson, K.L.; Kriston, L.; Vettorazzi, E.; Lohse, A.W.; Dalton, H.R.; Pischke, S. Hepatitis e seroprevalence in europe: A meta-analysis. Viruses 2016, 8, 211. [Google Scholar] [CrossRef]
- Christensen, P.B.; Engle, R.E.; Hjort, C.; Homburg, K.M.; Vach, W.; Georgsen, J.; Purcell, R.H. Time trend of the prevalence of hepatitis e antibodies among farmers and blood donors: A potential zoonosis in Denmark. Clin. Infect Dis. 2008, 47, 1026–1031. [Google Scholar] [CrossRef]
- Mansuy, J.M.; Bendall, R.; Legrand-Abravanel, F.; Saune, K.; Miedouge, M.; Ellis, V.; Rech, H.; Destruel, F.; Kamar, N.; Dalton, H.R.; et al. Hepatitis e virus antibodies in blood donors, France. Emerg. Infect. Dis. 2011, 17, 2309–2312. [Google Scholar] [CrossRef]
- Holm, D.K.; Moessner, B.K.; Engle, R.E.; Zaaijer, H.L.; Georgsen, J.; Purcell, R.H.; Christensen, P.B. Declining prevalence of hepatitis e antibodies among danish blood donors. Transfusion 2015, 55, 1662–1667. [Google Scholar] [CrossRef]
- Sauleda, S.; Ong, E.; Bes, M.; Janssen, A.; Cory, R.; Babizki, M.; Shin, T.; Lindquist, A.; Hoang, A.; Vang, L.; et al. Seroprevalence of hepatitis e virus (hev) and detection of hev rna with a transcription-mediated amplification assay in blood donors from Catalonia (Spain). Transfusion 2015, 55, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Nemecek, V.; Butovicova, P.; Maly, M.; Dite, P.; Vertatova, M.; Vodickova, I.; Kriz, B. The prevalence of antibodies against hepatitis e virus in the Czech Republic: Serological survey. Epidemiol. Mikrobiol. Imunol. 2017, 66, 3–7. [Google Scholar] [PubMed]
- Strakova, P.; Kriz, B.; Rudolf, I.; Hubalek, Z. Seroprevalence study of hepatitis e virus infection in two districts of the Czech Republic. Epidemiol. Mikrobiol. Imunol. 2014, 63, 92–94. [Google Scholar] [PubMed]
- Mansuy, J.M.; Gallian, P.; Dimeglio, C.; Saune, K.; Arnaud, C.; Pelletier, B.; Morel, P.; Legrand, D.; Tiberghien, P.; Izopet, J. A nationwide survey of hepatitis e viral infection in French blood donors. Hepatology 2016, 63, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Boutrouille, A.; Bakkali-Kassimi, L.; Cruciere, C.; Pavio, N. Prevalence of anti-hepatitis e virus antibodies in French blood donors. J. Clin. Microbiol. 2007, 45, 2009–2010. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.; Harte, D.; Sutherland, M.; Croucher, D.; Fouche, L.; Flanagan, P.; Williamson, D. Prevalence of hepatitis e virus antibodies and infection in New Zealand blood donors. N. Z. Med. J. 2018, 131, 38–43. [Google Scholar] [PubMed]
- Zafrullah, M.; Zhang, X.; Tran, C.; Nguyen, M.; Kamili, S.; Purdy, M.A.; Stramer, S.L. Disparities in detection of antibodies against hepatitis e virus in US blood donor samples using commercial assays. Transfusion 2018, 58, 1254–1263. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in r with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Barendregt, J.J.; Doi, S.A.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-analysis of prevalence. J. Epidemiol. Community Health 2013, 67, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Fellows, H.J.; Gane, E.J.; Wong, P.; Gerred, S.; Schroeder, B.; Croxson, M.C.; Garkavenko, O. Hepatitis e in New Zealand. J. Gastroenterol. Hepatol. 2007, 22, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Bura, M.; Lagiedo, M.; Michalak, M.; Sikora, J.; Mozer-Lisewska, I. Hepatitis e virus igg seroprevalence in hiv patients and blood donors, west-central Poland. Int. J. Infect. Dis. 2017, 61, 20–22. [Google Scholar] [CrossRef]
- Lucarelli, C.; Spada, E.; Taliani, G.; Chionne, P.; Madonna, E.; Marcantonio, C.; Pezzotti, P.; Bruni, R.; La Rosa, G.; Pisani, G.; et al. High prevalence of anti-hepatitis e virus antibodies among blood donors in central Italy, February to March 2014. Euro Surveill. 2016, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Grabarczyk, P.; Sulkowska, E.; Gdowska, J.; Kopacz, A.; Liszewski, G.; Kubicka-Russel, D.; Baylis, S.A.; Corman, V.M.; Nocen, E.; Piotrowski, D.; et al. Molecular and serological infection marker screening in blood donors indicates high endemicity of hepatitis e virus in Poland. Transfusion 2018, 58, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Mansuy, J.M.; Saune, K.; Rech, H.; Abravanel, F.; Mengelle, C.; S, L.H.; Destruel, F.; Kamar, N.; Izopet, J. Seroprevalence in blood donors reveals widespread, multi-source exposure to hepatitis e virus, southern France, October 2011. Euro Surveill. 2015, 20, 27–34. [Google Scholar] [CrossRef]
- Izopet, J.; Labrique, A.B.; Basnyat, B.; Dalton, H.R.; Kmush, B.; Heaney, C.D.; Nelson, K.E.; Ahmed, Z.B.; Zaman, K.; Mansuy, J.M.; et al. Hepatitis e virus seroprevalence in three hyperendemic areas: Nepal, Bangladesh and southwest France. J. Clin. Virol. 2015, 70, 39–42. [Google Scholar] [CrossRef]
- Mooij, S.H.; Hogema, B.M.; Tulen, A.D.; van Pelt, W.; Franz, E.; Zaaijer, H.L.; Molier, M.; Hofhuis, A. Risk factors for hepatitis e virus seropositivity in Dutch blood donors. BMC Infect. Dis. 2018, 18, 173. [Google Scholar] [CrossRef]
- Van Gageldonk-Lafeber, A.B.; van der Hoek, W.; Borlee, F.; Heederik, D.J.; Mooi, S.H.; Maassen, C.B.; Yzermans, C.J.; Rockx, B.; Smit, L.A.; Reimerink, J.H. Hepatitis e virus seroprevalence among the general population in a livestock-dense area in The Netherlands: A cross-sectional population-based serological survey. BMC Infect. Dis. 2017, 17, 21. [Google Scholar] [CrossRef]
- Slot, E.; Hogema, B.M.; Riezebos-Brilman, A.; Kok, T.M.; Molier, M.; Zaaijer, H.L. Silent hepatitis e virus infection in Dutch blood donors, 2011 to 2012. Euro Surveill. 2013, 18, 20550. [Google Scholar] [CrossRef]
- Xu, C.; Wang, R.Y.; Schechterly, C.A.; Ge, S.; Shih, J.W.; Xia, N.S.; Luban, N.L.; Alter, H.J. An assessment of hepatitis e virus (hev) in US blood donors and recipients: No detectable hev rna in 1939 donors tested and no evidence for hev transmission to 362 prospectively followed recipients. Transfusion 2013, 53, 2505–2511. [Google Scholar] [CrossRef] [PubMed]
- Lange, H.; Overbo, J.; Borgen, K.; Dudman, S.; Hoddevik, G.; Urdahl, A.M.; Vold, L.; Sjurseth, S.K. Hepatitis e in norway: Seroprevalence in humans and swine. Epidemiol. Infect. 2017, 145, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Hofmann, M.; Danzer, M.; Hofer, K.; Kaar, J.; Gabriel, C. Seroprevalence and incidence of hepatitis e in blood donors in upper Austria. PLoS ONE 2015, 10, e0119576. [Google Scholar] [CrossRef] [PubMed]
- Beale, M.A.; Tettmar, K.; Szypulska, R.; Tedder, R.S.; Ijaz, S. Is there evidence of recent hepatitis e virus infection in english and north welsh blood donors? Vox Sang. 2011, 100, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Galli, C.; Fomiatti, L.; Tagliacarne, C.; Velati, C.; Zanetti, A.R.; Castaldi, S.; Romano, L. Seroprevalence of hepatitis e virus among blood donors in northern Italy (Sondrio, Lombardy) determined by three different assays. Blood Transfus 2017, 15, 502–505. [Google Scholar] [PubMed]
- Spada, E.; Pupella, S.; Pisani, G.; Bruni, R.; Chionne, P.; Madonna, E.; Villano, U.; Simeoni, M.; Fabi, S.; Marano, G.; et al. A nationwide retrospective study on prevalence of hepatitis e virus infection in Italian blood donors. Blood Transfus 2018, 1–9. [Google Scholar] [CrossRef]
- Thom, K.; Gilhooly, P.; McGowan, K.; Malloy, K.; Jarvis, L.M.; Crossan, C.; Scobie, L.; Blatchford, O.; Smith-Palmer, A.; Donnelly, M.C.; et al. Hepatitis e virus (hev) in scotland: Evidence of recent increase in viral circulation in humans. Euro Surveill. 2018, 23, 12. [Google Scholar] [CrossRef]
- Shrestha, A.C.; Seed, C.R.; Flower, R.L.; Rooks, K.M.; Keller, A.J.; Harley, R.J.; Chan, H.T.; Holmberg, J.A.; Faddy, H.M. Hepatitis e virus and implications for blood supply safety, Australia. Emerg. Infect. Dis. 2014, 20, 1940–1942. [Google Scholar] [CrossRef]
- Fearon, M.A.; O’Brien, S.F.; Delage, G.; Scalia, V.; Bernier, F.; Bigham, M.; Weger, S.; Prabhu, S.; Andonov, A. Hepatitis e in Canadian blood donors. Transfusion 2017, 57, 1420–1425. [Google Scholar] [CrossRef]
- O’Riordan, J.; Boland, F.; Williams, P.; Donnellan, J.; Hogema, B.M.; Ijaz, S.; Murphy, W.G. Hepatitis e virus infection in the Irish blood donor population. Transfusion 2016, 56, 2868–2876. [Google Scholar] [CrossRef]
- Cleland, A.; Smith, L.; Crossan, C.; Blatchford, O.; Dalton, H.R.; Scobie, L.; Petrik, J. Hepatitis e virus in Scottish blood donors. Vox Sang. 2013, 105, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, A.; Tefanova, V.; Reshetnjak, I.; Kuznetsova, T.; Geller, J.; Lundkvist, A.; Janson, M.; Neare, K.; Velstrom, K.; Jokelainen, P.; et al. Hepatitis e virus in domestic pigs, wild boars, pig farm workers, and hunters in Estonia. Food Environ. Virol. 2015, 7, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, A.; Chaussade, H.; Rigaud, E.; Rodriguez, J.; Berthault, C.; Boue, F.; Tognon, M.; Touze, A.; Garcia-Bonnet, N.; Choutet, P.; et al. High hepatitis e virus seroprevalence in forestry workers and in wild boars in France. J. Clin. Microbiol. 2012, 50, 2888–2893. [Google Scholar] [CrossRef] [PubMed]
- Krumbholz, A.; Joel, S.; Dremsek, P.; Neubert, A.; Johne, R.; Durrwald, R.; Walther, M.; Muller, T.H.; Kuhnel, D.; Lange, J.; et al. Seroprevalence of hepatitis e virus (hev) in humans living in high pig density areas of Germany. Med. Microbiol. Immunol. 2014, 203, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.; Mesquita, J.R.; Pereira, S.S.; Oliveira, R.M.; Abreu-Silva, J.; Rodrigues, A.; Myrmel, M.; Stene-Johansen, K.; Overbo, J.; Goncalves, G.; et al. Prevalence of hepatitis e virus antibodies in workers occupationally exposed to swine in Portugal. Med. Microbiol. Immunol. 2017, 206, 77–81. [Google Scholar] [CrossRef]
- Meng, X.J.; Wiseman, B.; Elvinger, F.; Guenette, D.K.; Toth, T.E.; Engle, R.E.; Emerson, S.U.; Purcell, R.H. Prevalence of antibodies to hepatitis e virus in veterinarians working with swine and in normal blood donors in the United States and other countries. J. Clin. Microbiol. 2002, 40, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Chaussade, H.; Rigaud, E.; Allix, A.; Carpentier, A.; Touze, A.; Delzescaux, D.; Choutet, P.; Garcia-Bonnet, N.; Coursaget, P. Hepatitis e virus seroprevalence and risk factors for individuals in working contact with animals. J. Clin. Virol. 2013, 58, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Dremsek, P.; Wenzel, J.J.; Johne, R.; Ziller, M.; Hofmann, J.; Groschup, M.H.; Werdermann, S.; Mohn, U.; Dorn, S.; Motz, M.; et al. Seroprevalence study in forestry workers from eastern Germany using novel genotype 3- and rat hepatitis e virus-specific immunoglobulin g elisas. Med. Microbiol. Immunol. 2012, 201, 189–200. [Google Scholar] [CrossRef]
- Kantala, T.; Kinnunen, P.M.; Oristo, S.; Jokelainen, P.; Vapalahti, O.; Maunula, L. Hepatitis e virus antibodies in Finnish veterinarians. Zoon. Public Health 2017, 64, 232–238. [Google Scholar] [CrossRef]
- De Sabato, L.; Di Bartolo, I.; Montomoli, E.; Trombetta, C.; Ruggeri, F.M.; Ostanello, F. Retrospective study evaluating seroprevalence of hepatitis e virus in blood donors and in swine veterinarians in Italy (2004). Zoon. Public Health 2017, 64, 308–312. [Google Scholar] [CrossRef]
- Krumbholz, A.; Mohn, U.; Lange, J.; Motz, M.; Wenzel, J.J.; Jilg, W.; Walther, M.; Straube, E.; Wutzler, P.; Zell, R. Prevalence of hepatitis e virus-specific antibodies in humans with occupational exposure to pigs. Med. Microbiol. Immunol. 2012, 201, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Riveiro-Barciela, M.; Rodriguez-Frias, F.; Buti, M. Hepatitis e: Scale of the problem in Spain. Gastroenterol. Hepatol. 2012, 35, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.; Tokarska-Rodak, M.; Plewik, D.; Pańczuk, A.; Szepeluk, A.; Krajewska, M. The serological surveillance of hepatitis e virus among hunters and foresters in eastern Poland. Pol. J. Microbiol. 2017, 66, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Kuniholm, M.H.; Purcell, R.H.; McQuillan, G.M.; Engle, R.E.; Wasley, A.; Nelson, K.E. Epidemiology of hepatitis e virus in the United States: Results from the third national health and nutrition examination survey, 1988–1994. J. Infect. Dis. 2009, 200, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Buti, M.; Plans, P.; Dominguez, A.; Jardi, R.; Rodriguez Frias, F.; Esteban, R.; Salleras, L.; Plasencia, A. Prevalence of hepatitis e virus infection in children in the northeast of Spain. Clin. Vaccine Immunol. 2008, 15, 732–734. [Google Scholar] [CrossRef] [PubMed]
- Bayhan, G.I.; Demioren, K.; Guducuoglu, H. Epidemiology of hepatitis e virus in children in the province of van, Turkey. Turk. Pediatr. Ars. 2016, 51, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Potemkin, I.A.; Lopatukhina, M.A.; Gadzhieva, O.A.; Prokhorova, E.L.; Diyarrassuba, A.; Isaeva, O.A.; Kozhanova, T.V.; Ivanova, O.E.; Silenova, O.V.; Setdikova, N.; et al. Prevalence of hepatitis e markers in children. Zh. Mikrobiol. Epidemiol. Immunobiol. 2015, 2, 38–46. [Google Scholar]
- Oliveira, R.; Mesquita, J.R.; Pereira, S.; Abreu-Silva, J.; Teixeira, J.; Nascimento, M.S.J. Seroprevalence of hepatitis e virus antibodies in Portuguese children. Pediatr. Infect. Dis. J. 2017, 36, 623–626. [Google Scholar] [CrossRef]
- Faber, M.S.; Wenzel, J.J.; Jilg, W.; Thamm, M.; Hohle, M.; Stark, K. Hepatitis e virus seroprevalence among adults, Germany. Emerg. Infect. Dis. 2012, 18, 1654–1657. [Google Scholar] [CrossRef]
- Verhoef, L.; Koopmans, M.; Duizer, E.; Bakker, J.; Reimerink, J.; Van Pelt, W. Seroprevalence of hepatitis e antibodies and risk profile of hev seropositivity in The Netherlands, 2006–2007. Epidemiol. Infect. 2012, 140, 1838–1847. [Google Scholar] [CrossRef]
- Van Hoecke, F.; Van Maerken, T.; De Boulle, M.; Geerts, A.; Vlierberghe, V.; Colle, I.; Padalko, H.E. Hepatitis e seroprevalence in east and west Flanders, Belgium. Acta Gastroenterol. Belg. 2012, 75, 322–324. [Google Scholar]
- Faber, M.; Willrich, N.; Schemmerer, M.; Rauh, C.; Kuhnert, R.; Stark, K.; Wenzel, J.J. Hepatitis e virus seroprevalence, seroincidence and seroreversion in the German adult population. J. Viral. Hepat. 2018, 25, 752–758. [Google Scholar] [CrossRef]
- Pittaras, T.; Valsami, S.; Mavrouli, M.; Kapsimali, V.; Tsakris, A.; Politou, M. Seroprevalence of hepatitis e virus in blood donors in Greece. Vox Sang. 2014, 106, 387. [Google Scholar] [CrossRef]
- Haagsman, A.; Reuter, G.; Duizer, E.; Nagy, G.; Herremans, T.; Koopmans, M.; Szucs, G. Seroepidemiology of hepatitis e virus in patients with non-a, non-b, non-c hepatitis in Hungary. J. Med. Virol. 2007, 79, 927–930. [Google Scholar] [CrossRef]
- Hickey, C.; Spillane, D.; Benson, J.; Levis, J.; Fanning, L.J.; Cryan, B.; Prentice, M.B. Hepatitis e virus (hev) infection in Ireland. Ir. Med. J. 2016, 109, 451. [Google Scholar] [PubMed]
- Mor, O.; Bassal, R.; Michaeli, M.; Wax, M.; Ram, D.; Cohen-Ezra, O.; Cohen, D.; Mendelson, E.; Ben-Ari, Z.; Shohat, T. Prevalence of hepatitis e virus antibodies, Israel, 2009–2010. Emerg. Infect. Dis. 2015, 21, 692–694. [Google Scholar] [CrossRef]
- Ricco, G.; Bonino, F.; Lanza, M.; Scatena, F.; Alfieri, C.M.; Messa, P.; Marchisio, E.; Mascolo, G.; Romano, L.; Galli, C.; et al. New immunoassays for total, iga and igm antibodies against hepatitis e virus: Prevalence in Italian blood donors and patients with chronic liver or kidney diseases. Dig. Liver Dis. 2016, 48, 536–541. [Google Scholar] [CrossRef]
- Takeda, H.; Matsubayashi, K.; Sakata, H.; Sato, S.; Kato, T.; Hino, S.; Tadokoro, K.; Ikeda, H. A nationwide survey for prevalence of hepatitis e virus antibody in qualified blood donors in Japan. Vox Sang. 2010, 99, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Tamura, K.; Hoshino, Y.; Nagashima, S.; Yazaki, Y.; Mizuo, H.; Iwamoto, S.; Okayama, M.; Nakamura, Y.; Kajii, E.; et al. A nationwide survey of hepatitis e virus infection in the general population of Japan. J. Med. Virol. 2010, 82, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Bura, M.; Bukowska, A.; Bura, A.; Michalak, M.; Mozer-Lisewska, I. Hepatitis e virus antibodies in hiv-infected patients and blood donors from western Poland—A preliminary report. Adv. Clin. Exp. Med. 2017, 26, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Queiros, L.; Condeco, J.; Tender, A.; Mateus, M.; Teixeira, A.; Pascoal, H. The seroprevalence for hepatitis e viral antibodies in the northern region of Portugal (among the donor population). Acta Med. Port. 1997, 10, 447–453. [Google Scholar] [PubMed]
- Mateos, M.L.; Camarero, C.; Lasa, E.; Teruel, J.L.; Mir, N.; Baquero, F. Hepatitis e virus: Relevance in blood donors and risk groups. Vox Sang. 1999, 76, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Echevarria, J.M.; Fogeda, M.; Avellon, A. Epidemiology of hepatitis e virus infection in Spain. Enferm. Infecc. Microbiol. Clin. 2015, 33, 281–286. [Google Scholar] [PubMed]
- Fogeda, M.; Avellon, A.; Echevarria, J.M. Prevalence of specific antibody to hepatitis e virus in the general population of the community of Madrid, Spain. J. Med. Virol. 2012, 84, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, A.; Kenfak-Foguena, A.; Andre, C.; Canellini, G.; Burgisser, P.; Moradpour, D.; Darling, K.E.; Cavassini, M. Hepatitis e virus seroprevalence among blood donors in southwest Switzerland. PLoS ONE 2011, 6, e21150. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Stableforth, W.; Thurairajah, P.; Hazeldine, S.; Remnarace, R.; Usama, W.; Farrington, L.; Hamad, N.; Sieberhagen, C.; Ellis, V.; et al. Autochthonous hepatitis e in southwest england: Natural history, complications and seasonal variation, and hepatitis e virus igg seroprevalence in blood donors, the elderly and patients with chronic liver disease. Eur. J. Gastroenterol. Hepatol. 2008, 20, 784–790. [Google Scholar] [CrossRef]
- Teshale, E.H.; Denniston, M.M.; Drobeniuc, J.; Kamili, S.; Teo, C.G.; Holmberg, S.D. Decline in hepatitis e virus antibody prevalence in the United States from 1988–1994 to 2009–2010. J. Infect. Dis. 2015, 211, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Stramer, S.L.; Moritz, E.D.; Foster, G.A.; Ong, E.; Linnen, J.M.; Hogema, B.M.; Mak, M.; Chia, C.P.; Dodd, R.Y. Hepatitis e virus: Seroprevalence and frequency of viral rna detection among US blood donors. Transfusion 2016, 56, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, E.J.; Couturier, E.; Faber, M.; Said, B.; Ijaz, S.; Tavoschi, L.; Takkinen, J.; Adlhoch, C. Hepatitis e virus infection in europe: Surveillance and descriptive epidemiology of confirmed cases, 2005 to 2015. Euro Surveill. 2016, 22. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Hepatitis E in the EU/EEA, 2005–2015 Baseline Assessment of Testing, Diagnosis, Surveillance and Epidemiology; European Center for Disease Prevention and Control: Stockholm, Sweden, 2017.
- Rivero-Juarez, A.; Frias, M.; Martinez-Peinado, A.; Risalde, M.A.; Rodriguez-Cano, D.; Camacho, A.; Garcia-Bocanegra, I.; Cuenca-Lopez, F.; Gomez-Villamandos, J.C.; Rivero, A. Familial hepatitis e outbreak linked to wild boar meat consumption. Zoon. Public Health 2017, 64, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Guillois, Y.; Abravanel, F.; Miura, T.; Pavio, N.; Vaillant, V.; Lhomme, S.; Le Guyader, F.S.; Rose, N.; Le Saux, J.C.; King, L.A.; et al. High proportion of asymptomatic infections in an outbreak of hepatitis e associated with a spit-roasted piglet, France, 2013. Clin. Infect. Dis. 2016, 62, 351–357. [Google Scholar] [CrossRef]
- Garbuglia, A.R.; Scognamiglio, P.; Petrosillo, N.; Mastroianni, C.M.; Sordillo, P.; Gentile, D.; La Scala, P.; Girardi, E.; Capobianchi, M.R. Hepatitis e virus genotype 4 outbreak, Italy, 2011. Emerg. Infect. Dis. 2013, 19, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Trmal, J.; Pavlik, I.; Vasickova, P.; Matejickova, L.; Simunkova, L.; Luks, S.; Pazderkova, J. Outbreaks of viral hepatitis e in the Czech Republic? Epidemiol. Mikrobiol. Imunol. 2012, 61, 15–20. [Google Scholar] [PubMed]
- Yapa, C.M.; Furlong, C.; Rosewell, A.; Ward, K.A.; Adamson, S.; Shadbolt, C.; Kok, J.; Tracy, S.L.; Bowden, S.; Smedley, E.J.; et al. First reported outbreak of locally acquired hepatitis e virus infection in Australia. Med. J. Aust. 2016, 204, 274. [Google Scholar] [CrossRef] [PubMed]
- Ishida, S.; Matsuura, K.; Yoshizumi, S.; Miyoshi, M.; Sugisawa, T.; Tanida, M.; Okano, M. Hepatitis e outbreak at a nursing home for aged people in Hokkaido, Japan, between February and March 2016. J. Clin. Virol. 2018, 101, 23–28. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country | Population | Assay | Number of Samples | Seroprevalence anti-HEV IgG (%) | Reference |
|---|---|---|---|---|---|
| Denmark | BD | Wantai | 504 | 19.80 | [41] |
| NIH | 10.70 | ||||
| Spain | BD | Wantai | 9998 | 19.96 | [42] |
| Mikrogen | 10.72 | ||||
| Czech Republic | GP | Mikrogen | 1715 | 6.70 | [43] |
| Diagnostic Bioprobes | 230 | 5.70 | [44] | ||
| France | BD | Wantai | 10,569 | 22.4 | [45] |
| Genelabs Diagnostics | 1998 | 3.20 | [46] | ||
| New Zealand | BD | Wantai | 1013 | 9.70 | [47] |
| MP Diagnostics | 8.10 | ||||
| USA | BD | Wantai | 5040 | 12.28 | [48] |
| DSI | 11.29 | ||||
| MP Diagnostics | 10.65 |
| Country | Population | Number of Samples | Positive Samples | Seroprevalence anti-HEV IgG (%) | Reference |
|---|---|---|---|---|---|
| France (regions) | BD | 512 | 268 | 52.5 | [40] |
| Poland (regions) | BD | 246 | 122 | 49.6 | [54] |
| Italy (regions) | BD | 313 | 153 | 49 | [55] |
| Poland | BD | 3079 | 1340 | 43.52 | [56] |
| France (regions) | BD | 3353 | 1311 | 39.1 | [57] |
| France (regions) | BD | 1031 | 351 | 34 | [58] |
| Netherlands | BD | 2100 | 648 | 31 | [59] |
| GP | 2494 | 716 | 28.7 | [60] | |
| BD | 5239 | 1401 | 27 | [61] | |
| France | BD | 10,569 | 2371 | 22.4 | [45] |
| Spain | BD | 1082 | 216 | 19.96 | [42] |
| Denmark | BD | 504 | 100 | 19.8 | [41] |
| USA | BD | 1939 | 364 | 18.8 | [62] |
| Norway | BD | 1200 | 162 | 14 | [63] |
| Austria | BD | 1203 | 163 | 13.55 | [64] |
| USA | BD | 5040 | 619 | 12.28 | [48] |
| UK | BD | 262 | 31 | 12 | [65] |
| Italy (regions) | BD | 685 | 67 | 9.8 | [66] |
| New Zealand | BD | 1013 | 98 | 9.7 | [47] |
| Italy | BD | 10,011 | 869 | 8.7 | [67] |
| Scotland | BD | 1714 | 104 | 6.1 | [68] |
| Australia | BD | 3237 | 194 | 5.99 | [69] |
| Canada | BD | 4102 | 241 | 5.9 | [70] |
| Ireland | BD | 1076 | 57 | 5.3 | [71] |
| Scotland | BD | 1559 | 73 | 4.7 | [72] |
| New Zealand | BD | 265 | 11 | 4.2 | [53] |
| Country | Population | Assay | Number of Samples | Seroprevalence anti-HEV IgG (%) | p | OR [CI95] | References |
|---|---|---|---|---|---|---|---|
| Estonia | H | Mikrogen | 144 | 4.2 | 0.02 | 3.54 [1.07; 12.69] | [73] |
| PFW | 67 | 13.4 | |||||
| Germany | BD | Mikrogen | 301 | 11 | 0.0076 | 1.77 [1.15; 2.794] | [79] |
| FW | 563 | 18 | |||||
| GP | 106 | 28.3 | 0.02 | 2.14 [1.06; 4.41] | [82] | ||
| PFW | 116 | 15.5 | |||||
| Norway | BD | Wantai | 1200 | 14 | NS, p > 0.05 | [63] | |
| V | 163 | 13 | |||||
| FaW | 79 | 30 | 0.00028 | 2.68 [1.54; 4.53] | |||
| Portugal | GP | Mikrogen | 804 | 19.9 | 0.01 | 1.78 [1.12; 2.79] | [76] |
| PFW | 114 | 30.4 | |||||
| Spain | GP | ND | 325 | 7.3 | 0.002 | 2.89 [1.42; 5.82] | [83] |
| PFW | 101 | 19 | |||||
| Finland | GP | Axiom | 52 | 5.8 | NS, p > 0.05 | [80] | |
| V | 333 | 10.2 | |||||
| USA | BD | In-house assay | 400 | 18 | 0.005 | 1.60 [1.14; 2.26] | [77] |
| PFW | 468 | 26 | |||||
| France | FW | MP Diagnostics | 593 | 31.2 | / | / | [74] |
| GP | 322 | 26 | 0.007 | 1.61 [1.13; 2.30] | [78] | ||
| FW | 306 | 36.4 | |||||
| PFW | 231 | 43.8 | 0.0000017 | 2.19 [1.51; 3.21] | |||
| Italy | BD | BioChain Institute | 170 | 8.82 | 0.0007 | 3.30 [1.53; 8.15] | [81] |
| V | 83 | 9.64 | |||||
| Poland | H | ND | 210 | 3.81 | / | / | [84] |
| Country | Population | Assay | Number of Samples | Seroprevalence anti-HEV IgG (%) | Reference |
|---|---|---|---|---|---|
| USA | CH | ND | 18,695 | <5 | [85] |
| Spain | CH | Biokit | 1249 | 4.6 | [86] |
| Turkey | CH | Diagnostic Bioprobes | 408 | 4.2 | [87] |
| Russia | CH | ND | 3122 | 1.4 | [88] |
| Portugal | CH | Mikrogen | 352 | 1.1 | [89] |
| Country | Population | Assay | Number of Samples | HEV IgG (%) | Reference |
|---|---|---|---|---|---|
| Belgium | P | Strip immunoassay | 100 | 14 | [92] |
| Germany | GP | Mikrogen | 4422 | 16.8 | [90] |
| Germany | GP | 7075 | 15.3 | [93] | |
| Greece | BD | Adaltis | 265 | 9.43 | [94] |
| Hungary | P | In-house assay | 246 | 10.5 | [95] |
| Ireland | BD | ND | 198 | 8 | [96] |
| Israel | BD | Diagnostic system | 729 | 10.6 | [97] |
| Italy | BD | In-house assay | 199 | 7 | [98] |
| Japan | BD | In-house assay | 12,600 | 3.4 | [99] |
| Japan | GP | In-house assay | 22,027 | 5.3 | [100] |
| Netherlands | GP | ND | 7072 | 1.9 | [91] |
| Poland | BD | Euroimmun | 105 | 3.8 | [101] |
| Portugal | BD | Abbott | 1473 | 2.5 | [102] |
| Spain | BD | 563 | 2.8 | [103] | |
| Spain | GP | ND | NA | 10 | [104] |
| Spain | GP | Bioprobes | 2305 | 2.17 | [105] |
| Switzerland | BD | MP Diagnostics | 550 | 4.9 | [106] |
| UK | BD | ND | 500 | 16 | [107] |
| UK | PCLD | ND | 126 | 13 | |
| UK | OP | ND | 336 | 25 | |
| USA | GP | Diagnostic system | 5966 | 10.2 | [108] |
| USA | GP | 7885 | 6 | ||
| USA | BD | MP Diagnostics | 4499 | 9.5 | [109] |
| Country | Number of Persons | Year | Cause | Virus | Reference |
|---|---|---|---|---|---|
| Spain | 8 | 2015 | Wild boar meat consumption | Genotype 3 | [112] |
| Australia | 17 | 2014 | Pork products in a restaurant | Genotype 3 | [116] |
| France | 17 | 2013 | Wedding spit-roasted piglet | ND | [113] |
| Italy | 5 | 2011 | Not identified | Genotype 4 | [114] |
| Czech Republic | 13 | Not found in the reference | Not identified | ND | [115] |
| 8 | Infection in farm pigs | ND | |||
| UK | 4 | 2008 | foodborne source on a cruise ship | ND | [14] |
| Japan | 29 | 2016 | Not identified | Genotype 3 | [117] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capai, L.; Falchi, A.; Charrel, R. Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature. Viruses 2019, 11, 84. https://doi.org/10.3390/v11010084
Capai L, Falchi A, Charrel R. Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature. Viruses. 2019; 11(1):84. https://doi.org/10.3390/v11010084
Chicago/Turabian StyleCapai, Lisandru, Alessandra Falchi, and Rémi Charrel. 2019. "Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature" Viruses 11, no. 1: 84. https://doi.org/10.3390/v11010084
APA StyleCapai, L., Falchi, A., & Charrel, R. (2019). Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature. Viruses, 11(1), 84. https://doi.org/10.3390/v11010084