
Process Mining in Clinical Practice: Model Evaluations in the Central Venous Catheter Installation Training




Abstract
:1. Introduction
- RO1:
- Display major training activities in CVC installation with Pertinet modeling;
- RO2:
- Present a novel framework with fuzzy mining analysis;
- RO3:
- Perform a conformance check to understand the activity deviation with prescribed CVC training.
2. Research Background
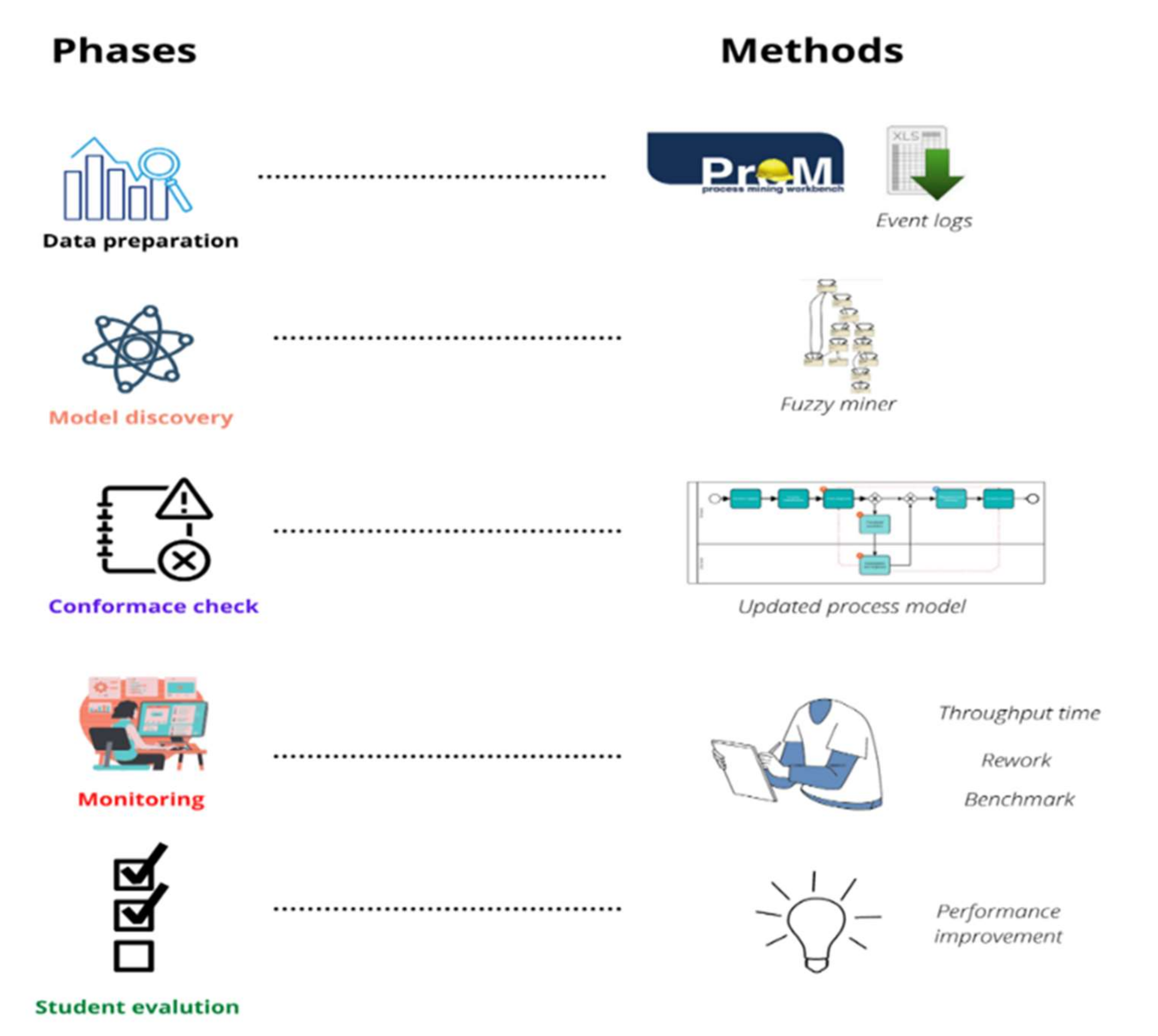
3. Methods
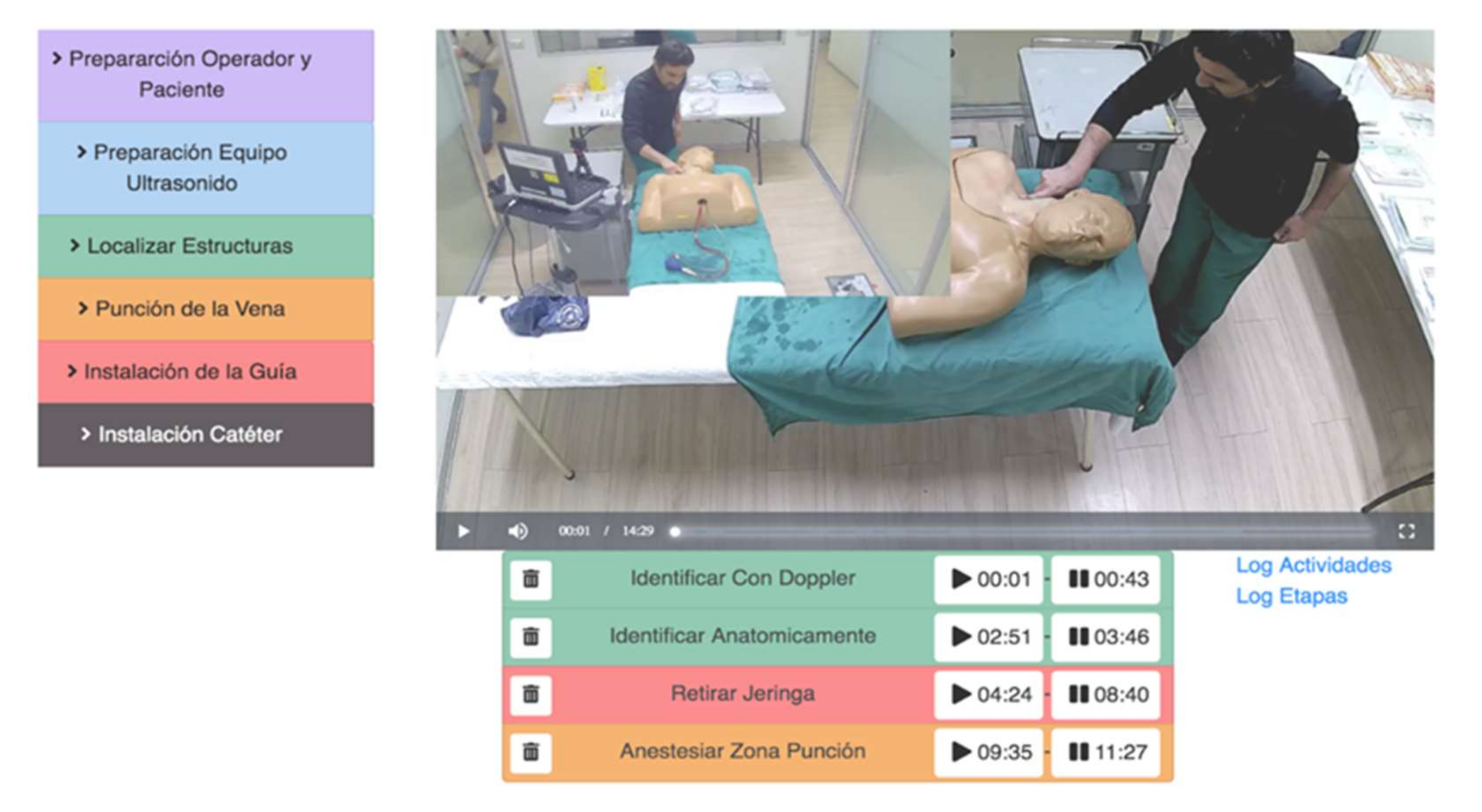
3.1. CCC19 Dataset
- Learning: Students have to learn the initial procedure;
- PRE recording: Students have to perform the first pre-test (PRE);
- Practice: Students need to practice without barriers to get a good idea of the procedure;
- POST recording: Finally, they need to conduct the final post-test (POST) to make sure of the acquisition of enough knowledge.
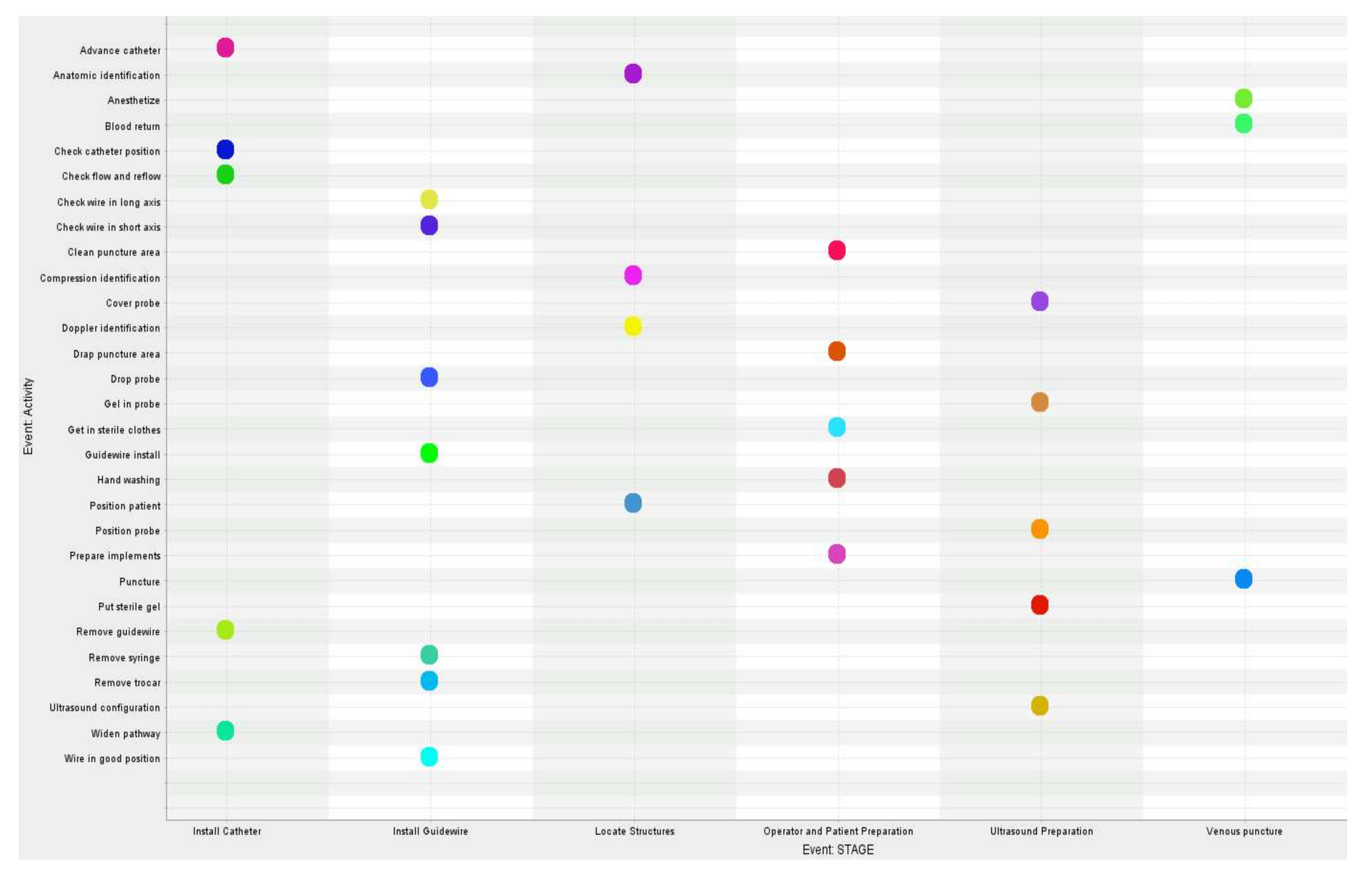
3.2. Process Stages
3.3. Model Preparation
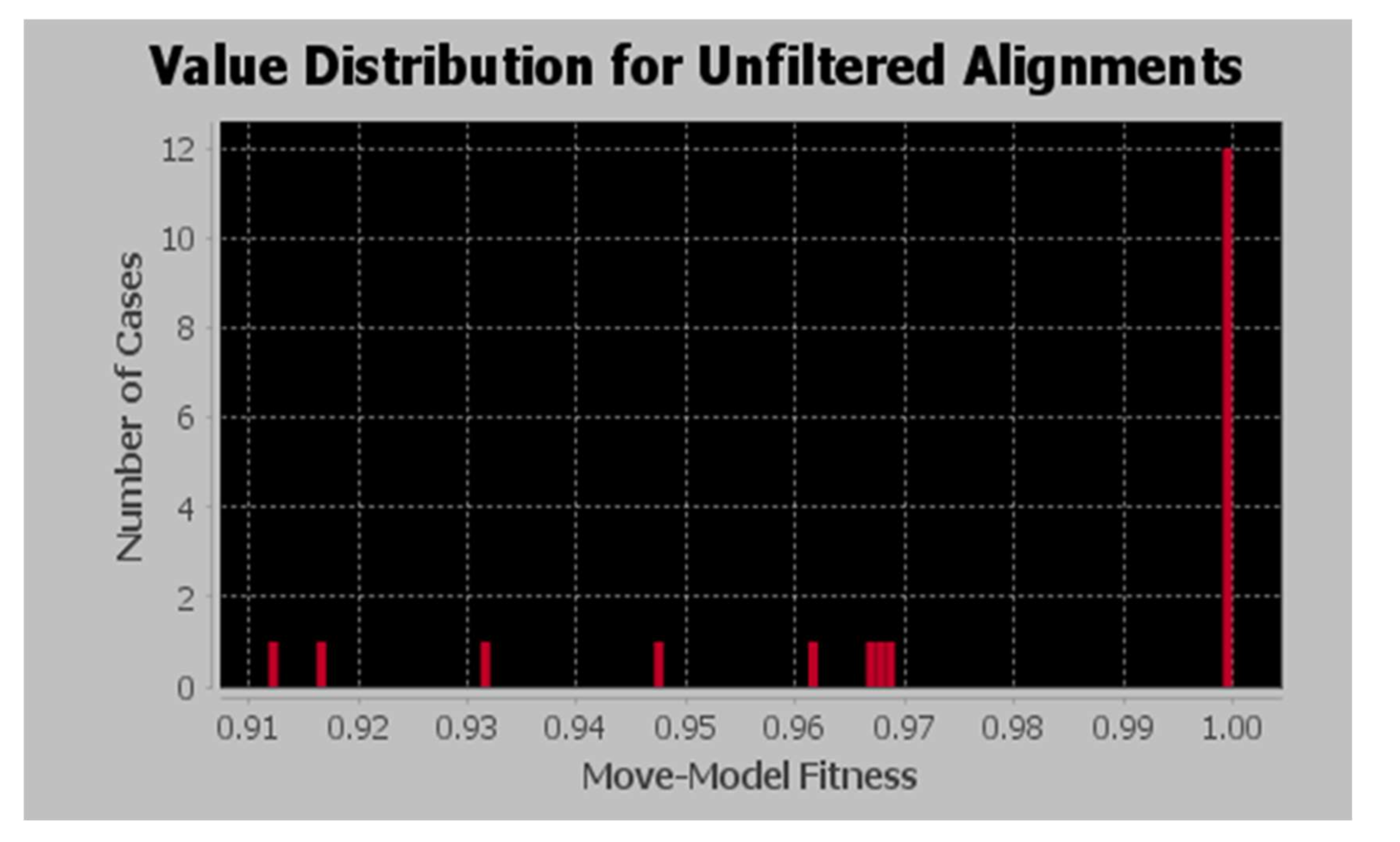
3.4. Model Fitness Calculation
3.5. Model Analysis
4. Results
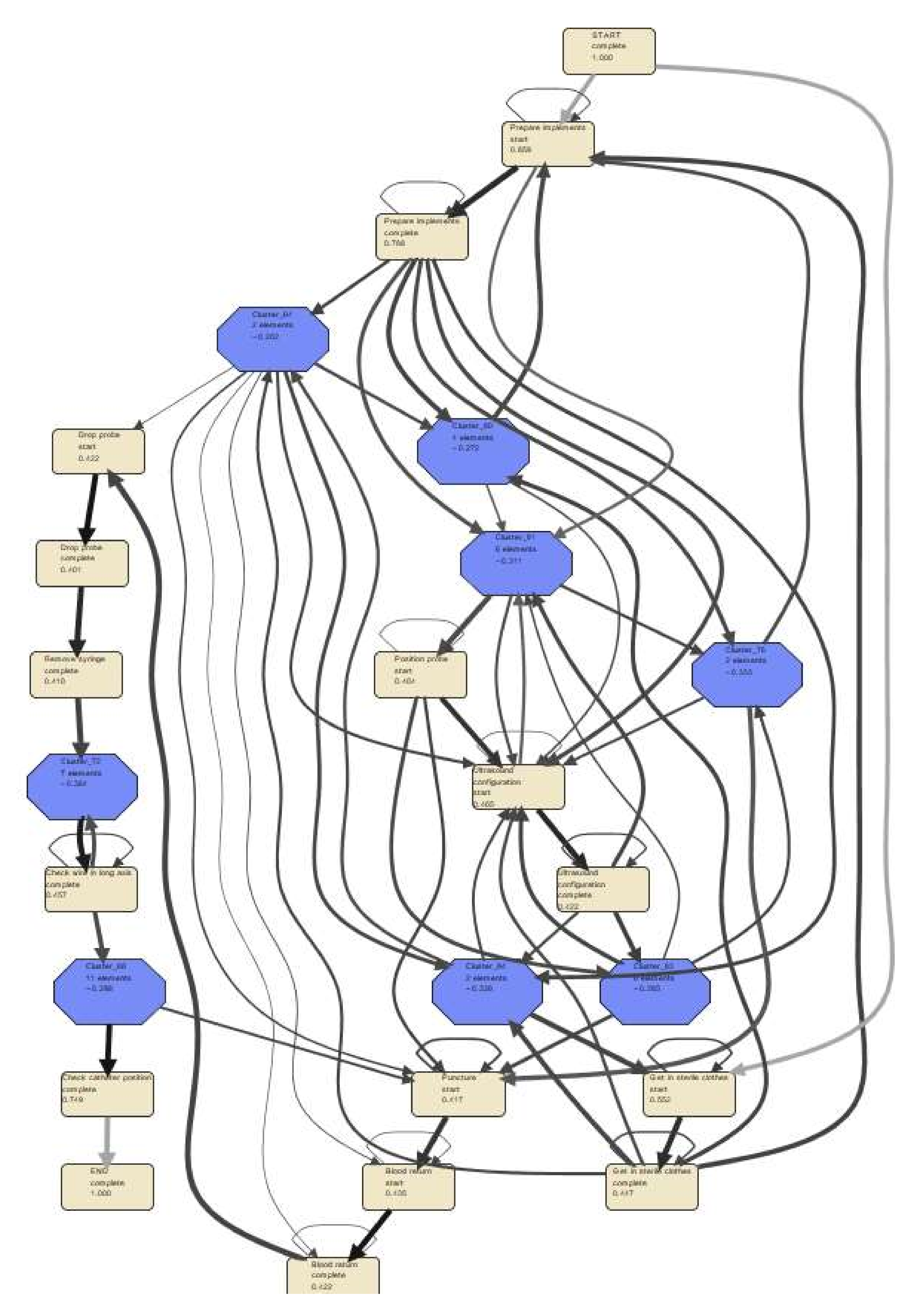
4.1. Process Discovery with Fuzzy Modeling
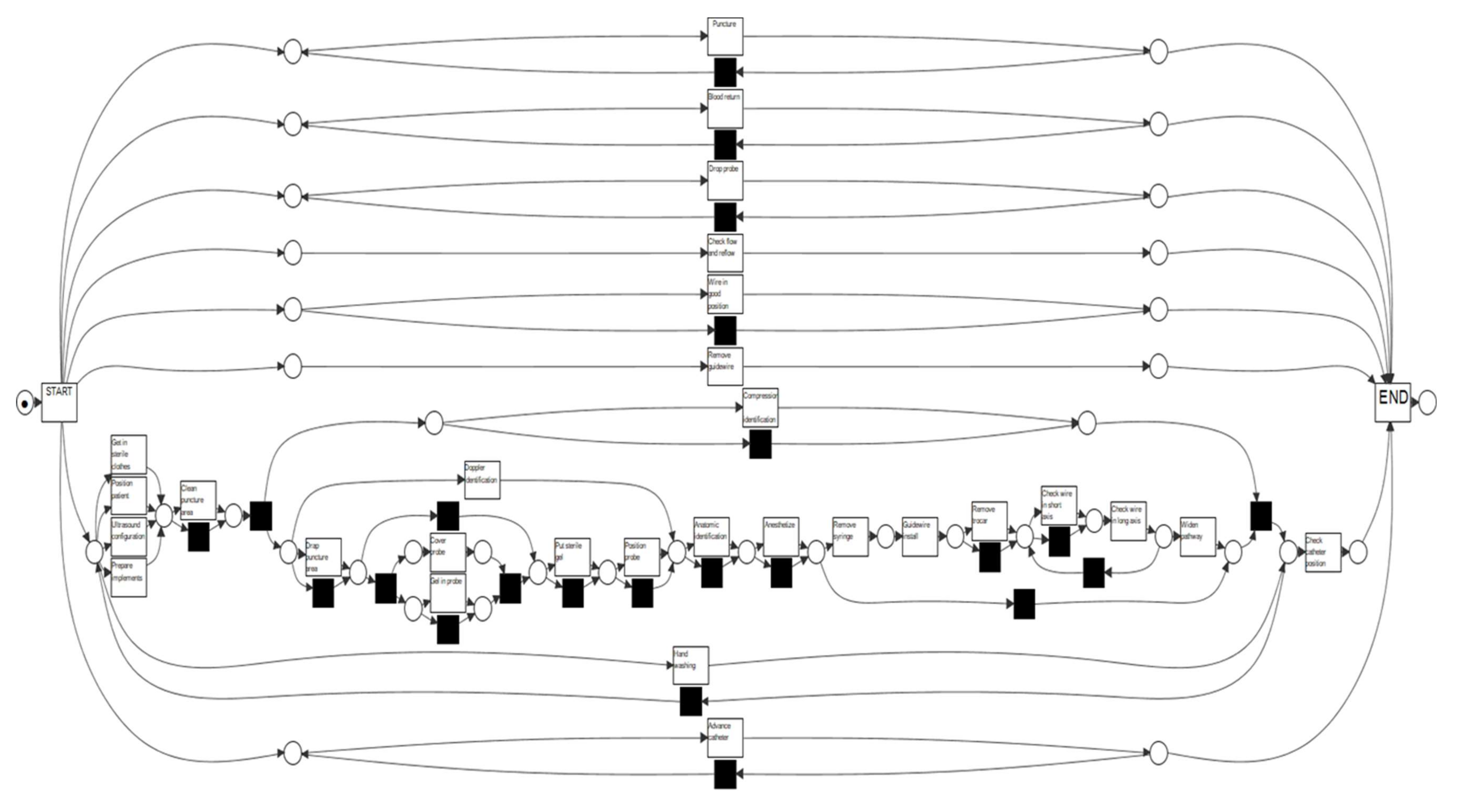
4.2. Petri Net (P-Net) Modeling of Student Activities
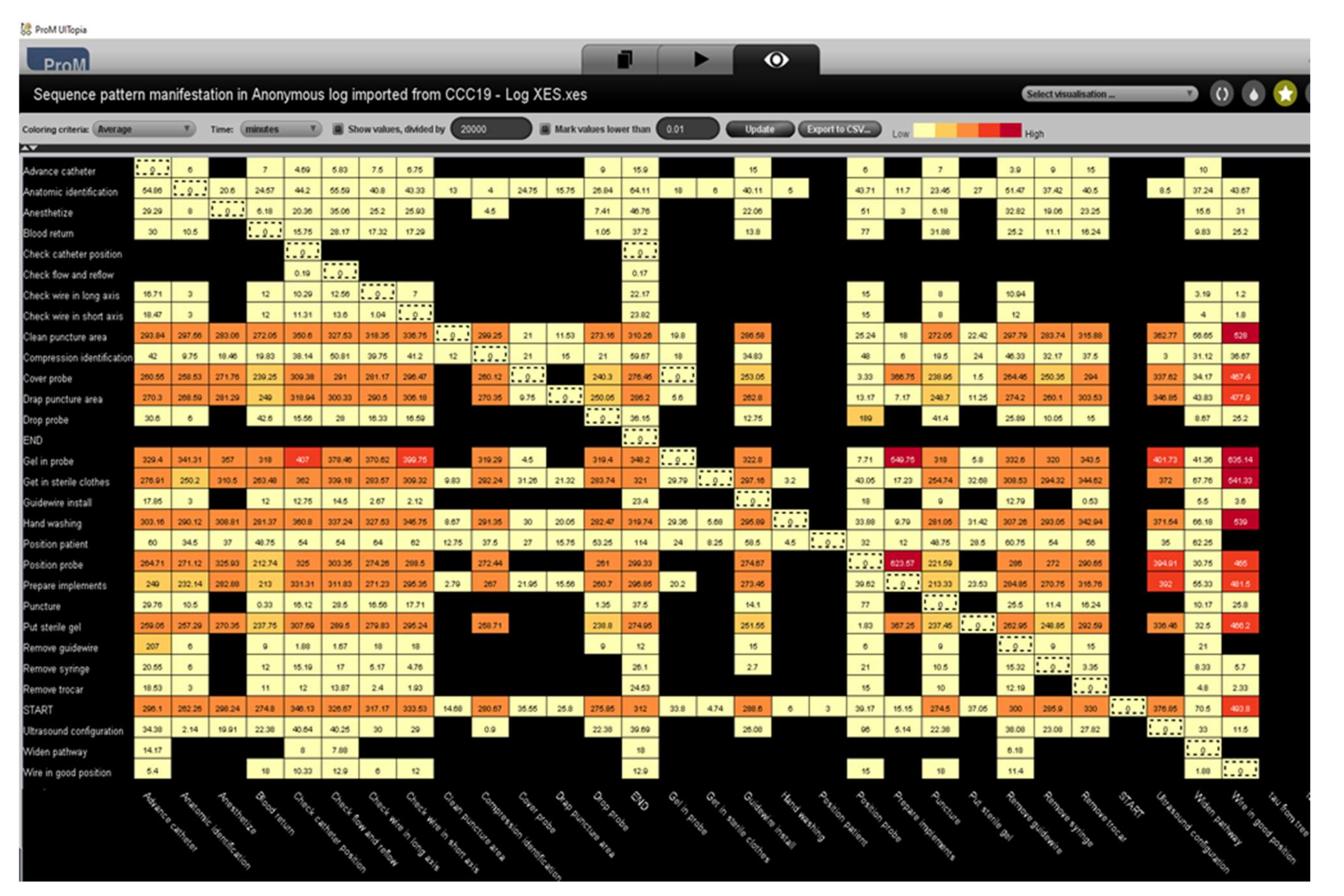
4.3. Conformance Check
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jug, R.; Jiang, X.S.; Bean, S.M. Giving and Receiving Effective Feedback: A Review Article and How-To Guide. Arch. Pathol. Lab. Med. 2019, 143, 244–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laidlaw, A.; Aiton, J.; Struthers, J.; Guild, S. Developing research skills in medical students: AMEE Guide No. 69. Med. Teach. 2012, 34, 754–771. [Google Scholar] [CrossRef] [PubMed]
- Butler-Henderson, K.; Dalton, L.; Probst, Y.; Maunder, K.; Merolli, M. A meta-synthesis of competency standards suggest allied health are not preparing for a digital health future. Int. J. Med. Inform. 2020, 144, 104296. [Google Scholar] [CrossRef] [PubMed]
- Landry, S.; Beaulieu, M.; Roy, J. Strategy deployment in healthcare services: A case study approach. Technol. Forecast. Soc. Chang. 2016, 113, 429–437. [Google Scholar] [CrossRef]
- Alexandrou, E.; Spencer, T.R.; Frost, S.A.; Mifflin, N.; Davidson, P.M.; Hillman, K.M. Central venous catheter placement by advanced practice nurses demonstrates low procedural complication and infection rates–A report from 13 years of service*. Crit. Care Med. 2014, 42, 536–543. [Google Scholar] [CrossRef] [Green Version]
- Lynagh, M.; Burton, R.; Sanson-Fisher, R. A systematic review of medical skills laboratory training: Where to from here? Med. Educ. 2007, 41, 879–887. [Google Scholar] [CrossRef]
- Hatala, R.; Cook, D.A.; Zendejas, B.; Hamstra, S.J.; Brydges, R. Feedback for simulation-based procedural skills training: A meta-analysis and critical narrative synthesis. Adv. Health Sci. Educ. Theory Pract. 2014, 19, 251–272. [Google Scholar] [CrossRef]
- Strand, I.; Nåden, D.; Slettebø, Å. Students Learning in a Skills Laboratory. Vård Nord. 2009, 29, 18–22. [Google Scholar] [CrossRef] [Green Version]
- Ralhan, S.; Bhogal, P.; Bhatnagar, G.; Young, J.; Green, M. Effective teaching skills—How to become a better medical educator. BMJ 2012, 344, e765. [Google Scholar] [CrossRef]
- Nimavat, N.; Singh, S.; Fichadiya, N.; Sharma, P.; Patel, N.; Kumar, M.; Chauhan, G.; Pandit, N. Online Medical Education in India-Different Challenges and Probable Solutions in the Age of COVID-19. Adv. Med. Educ. Pract. 2021, 12, 237–243. [Google Scholar] [CrossRef]
- Neumuth, D.; Loebe, F.; Herre, H.; Neumuth, T. Modeling surgical processes: A four-level translational approach. Artif. Intell. Med. 2011, 51, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Brzychczy, E.; Napieraj, A.; Sukiennik, M. Modeling of processes with use of process mining techniques. Sci. Pap. Silesian Univ. Technol. Organ. Manag. Ser. 2018, 2018, 23–36. [Google Scholar] [CrossRef]
- Lira, R.; Salas-Morales, J.; de la Fuente, R.; Fuentes, R.; Sepúlveda, M.; Arias, M.; Herskovic, V.; Munoz-Gama, J. Tailored Process Feedback Through Process Mining for Surgical Procedures in Medical Training: The Central Venous Catheter Case. Lect. Notes Bus. Inf. Process. 2019, 342, 163–174. [Google Scholar] [CrossRef]
- Meyer, J.; Reimold, J.; Wehmschulte, C. Conformance Checking Challenge 2019: Analysis of Central Venous Catheter Installation with MEHRWERK ProcessMining. Available online: https://icpmconference.org/2019/wp-content/uploads/sites/6/2019/09/ICPM2019_paper_84.pdf (accessed on 28 February 2022).
- Lira, R.; Salas-Morales, J.; Leiva, L.; de la Fuente, R.; Fuentes, R.; Delfino, A.; Nazal, C.H.; Sepúlveda, M.; Arias, M.; Herskovic, V.; et al. Process-Oriented Feedback through Process Mining for Surgical Procedures in Medical Training: The Ultrasound-Guided Central Venous Catheter Placement Case. Int. J. Environ. Res. Public Health 2019, 16, 1877. [Google Scholar] [CrossRef] [Green Version]
- Thimbleby, H. Technology and the Future of Healthcare. J. Public Health Res. 2013, 2, 28. [Google Scholar] [CrossRef] [Green Version]
- Bergman, B.; Neuhauser, D.; Provost, L. Five main processes in healthcare: A citizen perspective. BMJ Qual. Saf. 2011, 20 (Suppl. 1), i41. [Google Scholar] [CrossRef] [Green Version]
- Munoz-Gama, J.; Martin, N.; Fernandez-Llatas, C.; Johnson, O.A.; Sepúlveda, M.; Helm, E.; Galvez-Yanjari, V.; Rojas, E.; Martinez-Millana, A.; Aloini, D.; et al. Process mining for healthcare: Characteristics and challenges. J. Biomed. Inform. 2022, 127, 103994. [Google Scholar] [CrossRef]
- Ali, O.; Ishak, M.K.; Bhatti, M.K.L.; Khan, I.; Kim, K.I. A Comprehensive Review of Internet of Things: Technology Stack, Middlewares, and Fog/Edge Computing Interface. Sensors 2022, 22, 995. [Google Scholar] [CrossRef]
- Farahani, B.; Firouzi, F.; Chang, V.; Badaroglu, M.; Constant, N.; Mankodiya, K. Towards fog-driven IoT eHealth: Promises and challenges of IoT in medicine and healthcare. Futur. Gener. Comput. Syst. 2018, 78, 659–676. [Google Scholar] [CrossRef] [Green Version]
- Ibarra-Esquer, J.E.; González-Navarro, F.F.; Flores-Rios, B.L.; Burtseva, L.; Astorga-Vargas, M.A. Tracking the evolution of the internet of things concept across different application domains. Sensors 2017, 17, 1379. [Google Scholar] [CrossRef]
- Pal, S.; Hitchens, M.; Rabehaja, T.; Mukhopadhyay, S. Security requirements for the internet of things: A systematic approach. Sensors 2020, 20, 5897. [Google Scholar] [CrossRef] [PubMed]
- Rojas, E.; Munoz-Gama, J.; Sepúlveda, M.; Capurro, D. Process mining in healthcare: A literature review. J. Biomed. Inform. 2016, 61, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Gatta, R.; Vallati, M.; Fernandez-Llatas, C.; Martinez-Millana, A.; Orini, S.; Sacchi, L.; Castellano, M. What Role Can Process Mining Play in Recurrent Clinical Guidelines Issues? A Position Paper. Int. J. Environ. Res. Public Health 2020, 17, 6616. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Gama, J.; Galvez, V.; de la Fuente, R.; Sepúlveda, M.; Fuentes, R. Interactive Process Mining for Medical Training. In Interactive Process Mining in Healthcare; Springer: Cham, Switzerland, 2021; pp. 233–242. [Google Scholar] [CrossRef]
- Mahajan, V.; Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications. J. Mark. Res. 1976, 13, 317. [Google Scholar] [CrossRef]
- R’Bigui, H.; Cho, C. The state-of-the-art of business process mining challenges. Int. J. Bus. Process. Integr. Manag. 2017, 8, 285–303. [Google Scholar] [CrossRef]
- Prom611|ProM Tools. Available online: https://www.promtools.org/doku.php?id=prom611 (accessed on 26 April 2022).
- Bogarín, A.; Cerezo, R.; Romero, C. Discovering learning processes using Inductive Miner: A case study with Learning Management Systems (LMSs). Psicothema 2018, 30, 322–329. [Google Scholar] [CrossRef]
- Song, M.; Günther, C.W.; Van Der Aalst, W.M.P. Trace Clustering in Process Mining. In Proceedings of the International Conference on Business Process Management, Ulm, Germany, 8–10 September 2009; Springer: Berlin/Heidelberg, Germany, 2009; Volume 17, pp. 109–120. [Google Scholar] [CrossRef]
- Munoz-Gama, J. Conformance checking and its challenges. Lect. Notes Bus. Inf. Process. 2016, 270, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Battineni, G.; Chintalapudi, N.; Amenta, F. Model discovery, and replay fitness validation using inductive mining techniques in medical training of CVC surgery. Appl. Comput. Informat 2020, ahead-of-print. [Google Scholar] [CrossRef]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Q. 2005, 83, 691. [Google Scholar] [CrossRef] [Green Version]
- Kelly, E.; Richards, J.B. Medical education: Giving feedback to doctors in training. BMJ 2019, 366, l4523. [Google Scholar] [CrossRef]
- Palepu, G.; Deven, J.; Subrahmanyam, M.; Mohan, S. Impact of ultrasonography on central venous catheter insertion in intensive care. Indian J. Radiol. Imaging 2009, 19, 191. [Google Scholar] [CrossRef] [PubMed]
- Geyer-Klingeberg, J.; Nakladal, J.; Badakhshan, P.; Somasundaram, I. Medical Training Analytics through Process Mining: The Case of Central Venous Catheters Surgeries Conformance Checking Challenge 2019 *. Available online: https://www.thoracic.org/patients/patient-resources/resources/central-venous-catheter.pdf (accessed on 26 April 2022).
- Wang, Y.; Zacharewicz, G.; Traoré, M.K.; Chen, D. An integrative approach to simulation model discovery: Combining system theory, process mining and fuzzy logic. J. Intell. Fuzzy Syst. 2018, 34, 477–490. [Google Scholar] [CrossRef] [Green Version]
- Zeigler, B.P.; Praehofer, H.; Kim, T.G. Theory of Modeling and Simulation Handbook of Simulator-Based Training Creating Computer Simulation Systems: An introduction to the High Level Architecture. Practice 2000, 100, 91–92. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Activities | Occurrences (Absolute) | Occurrence (Relative) |
|---|---|---|
| Prepare implements | 126 | 9.039% |
| Get in sterile clothes | 74 | 5.308% |
| Ultrasound configuration | 66 | 4.735% |
| Check wire in the long axis | 62 | 4.448% |
| Advance catheter | 60 | 4.304% |
| Puncture | 60 | 4.304% |
| Blood return | 58 | 4.161% |
| Drop probe | 56 | 4.017% |
| Guidewire install | 56 | 4.017% |
| Check wire in short axis | 54 | 3.874% |
| Remove syringe | 52 | 3.73% |
| Anatomic identification | 50 | 3.587% |
| Position probe | 50 | 3.587% |
| Remove trocar | 48 | 3.443% |
| Hand washing | 44 | 3.156% |
| Put sterile gel | 44 | 3.156% |
| Remove guidewire | 42 | 3.013% |
| Compression identification | 42 | 3.013% |
| Widen pathway | 42 | 3.013% |
| Drap puncture area | 40 | 2.869% |
| Cover probe | 40 | 2.869% |
| Clean puncture area | 38 | 2.726% |
| Check flow and reflow | 38 | 2.726% |
| Anaesthetize | 38 | 2.726% |
| Gel in probe | 38 | 2.726% |
| Check catheter position | 34 | 2.439% |
| Wire in a good position | 20 | 1.435% |
| Position patient | 12 | 0.861% |
| Doppler identification | 10 | 0.717% |
| Activities | Total Log (Absolute) | Accurately Fitting Logs | Model Moves (In All Traces) |
|---|---|---|---|
| Gel in probe | 20 | 15 | 5 |
| Check catheter position | 20 | 16 | 4 |
| Anaesthetize | 20 | 17 | 3 |
| Check wire in the long axis | 30 | 28 | 2 |
| Compression identification | 20 | 18 | 2 |
| Widen pathway | 20 | 18 | 2 |
| Check flow and reflow | 20 | 18 | 2 |
| Position probe | 27 | 25 | 2 |
| Anatomic identification | 26 | 25 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battineni, G.; Chintalapudi, N.; Zacharewicz, G. Process Mining in Clinical Practice: Model Evaluations in the Central Venous Catheter Installation Training. Algorithms 2022, 15, 153. https://doi.org/10.3390/a15050153
Battineni G, Chintalapudi N, Zacharewicz G. Process Mining in Clinical Practice: Model Evaluations in the Central Venous Catheter Installation Training. Algorithms. 2022; 15(5):153. https://doi.org/10.3390/a15050153
Chicago/Turabian StyleBattineni, Gopi, Nalini Chintalapudi, and Gregory Zacharewicz. 2022. "Process Mining in Clinical Practice: Model Evaluations in the Central Venous Catheter Installation Training" Algorithms 15, no. 5: 153. https://doi.org/10.3390/a15050153
APA StyleBattineni, G., Chintalapudi, N., & Zacharewicz, G. (2022). Process Mining in Clinical Practice: Model Evaluations in the Central Venous Catheter Installation Training. Algorithms, 15(5), 153. https://doi.org/10.3390/a15050153