Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies

Abstract
:
1. Introduction
- Requirements of the dentist and patient:
- ○
- High strength and toughness depending on the required indication
- ○
- High durability as dental restorative material
- ○
- Excellent optical appearance (translucency, brightness, color and fluorescence like that of natural teeth)
- ○
- Easy handling (no additional extensive treatment after the CAD/CAM process)
- ○
- Easy placement of the restoration on natural dentin
- Requirements of CAD/CAM technology:
- ○
- No chipping
- ○
- Easy processing
- ○
- Preferable: small apparatus for dental clinics
2. Materials Systems
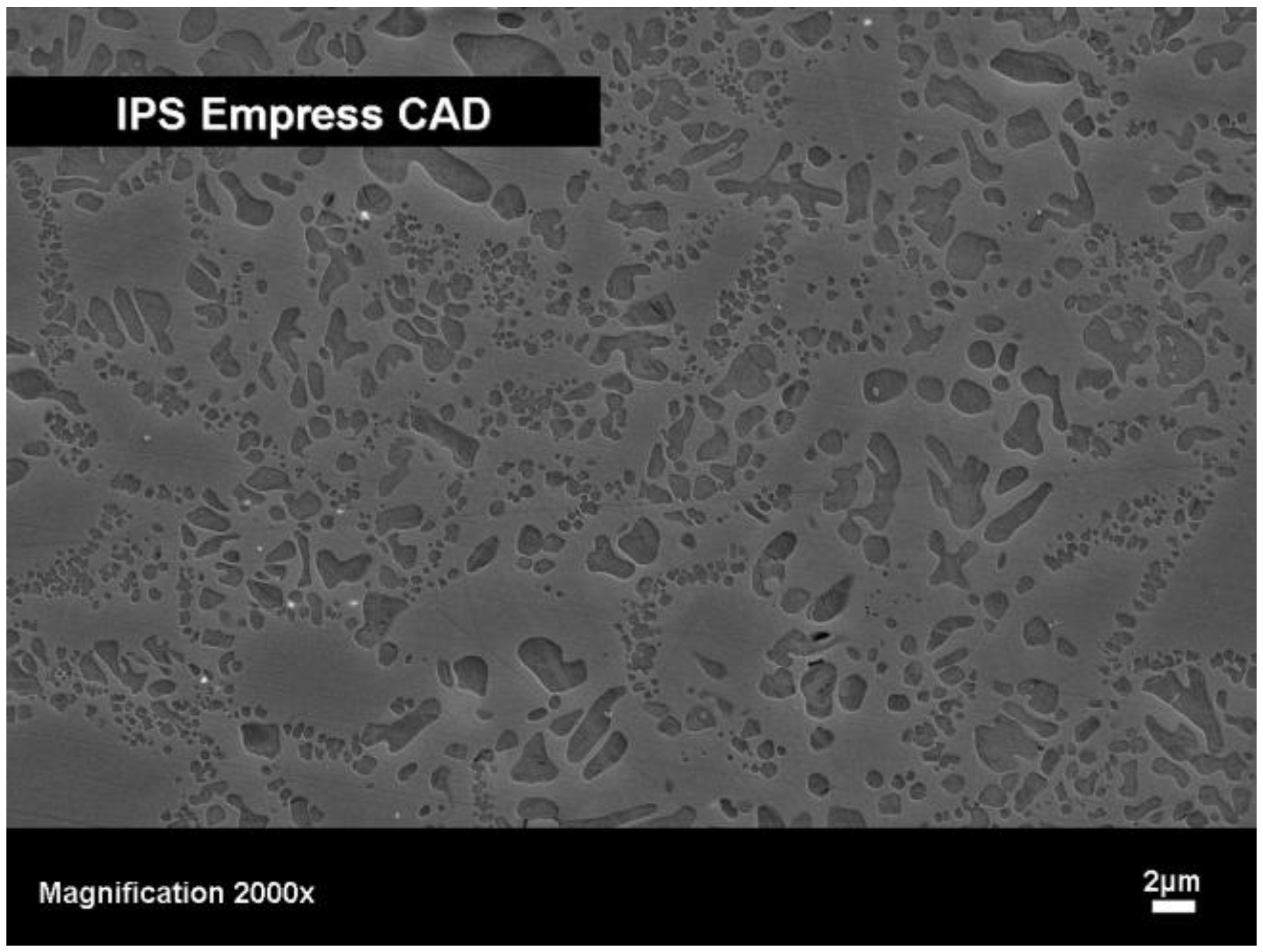
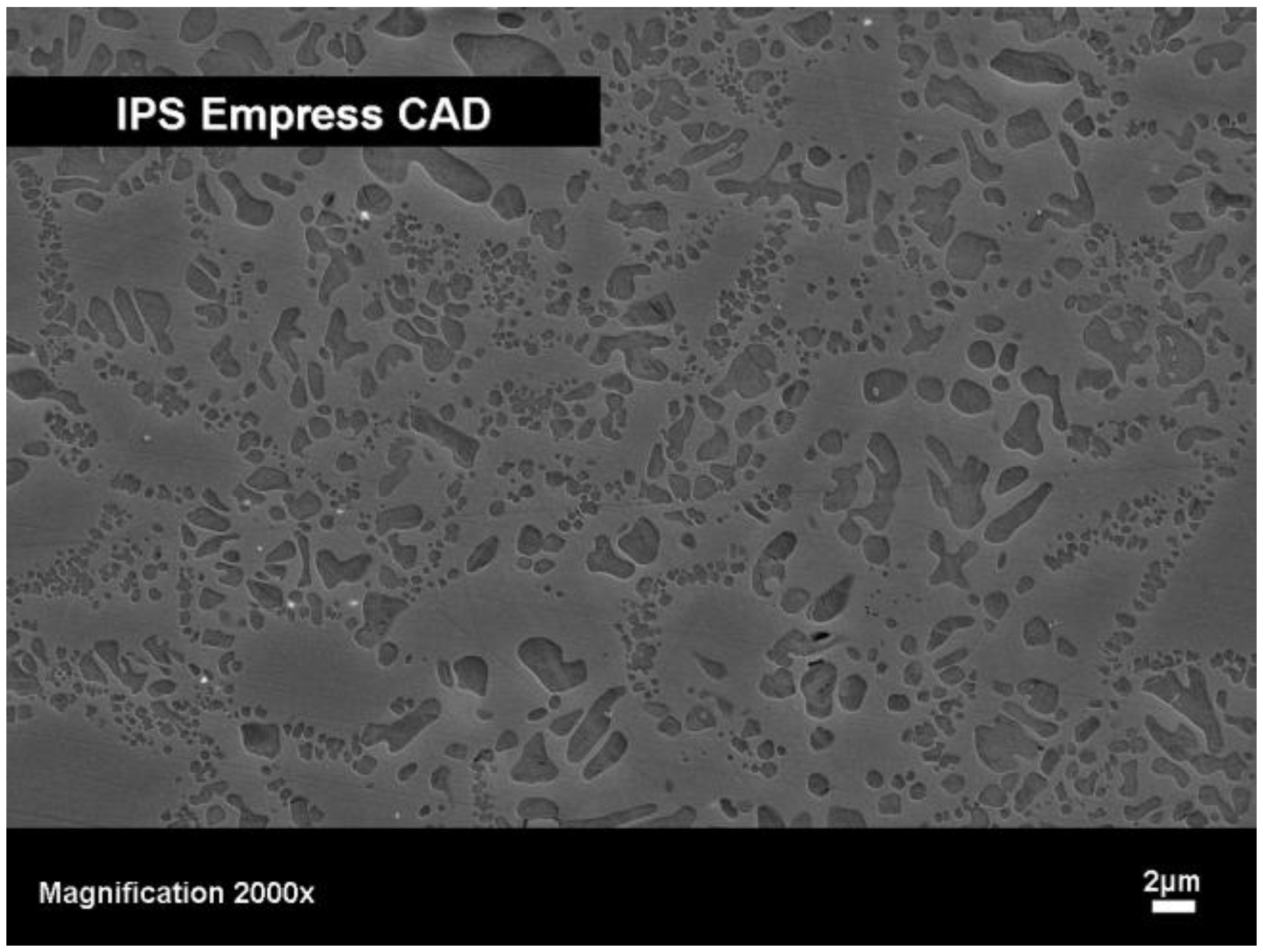
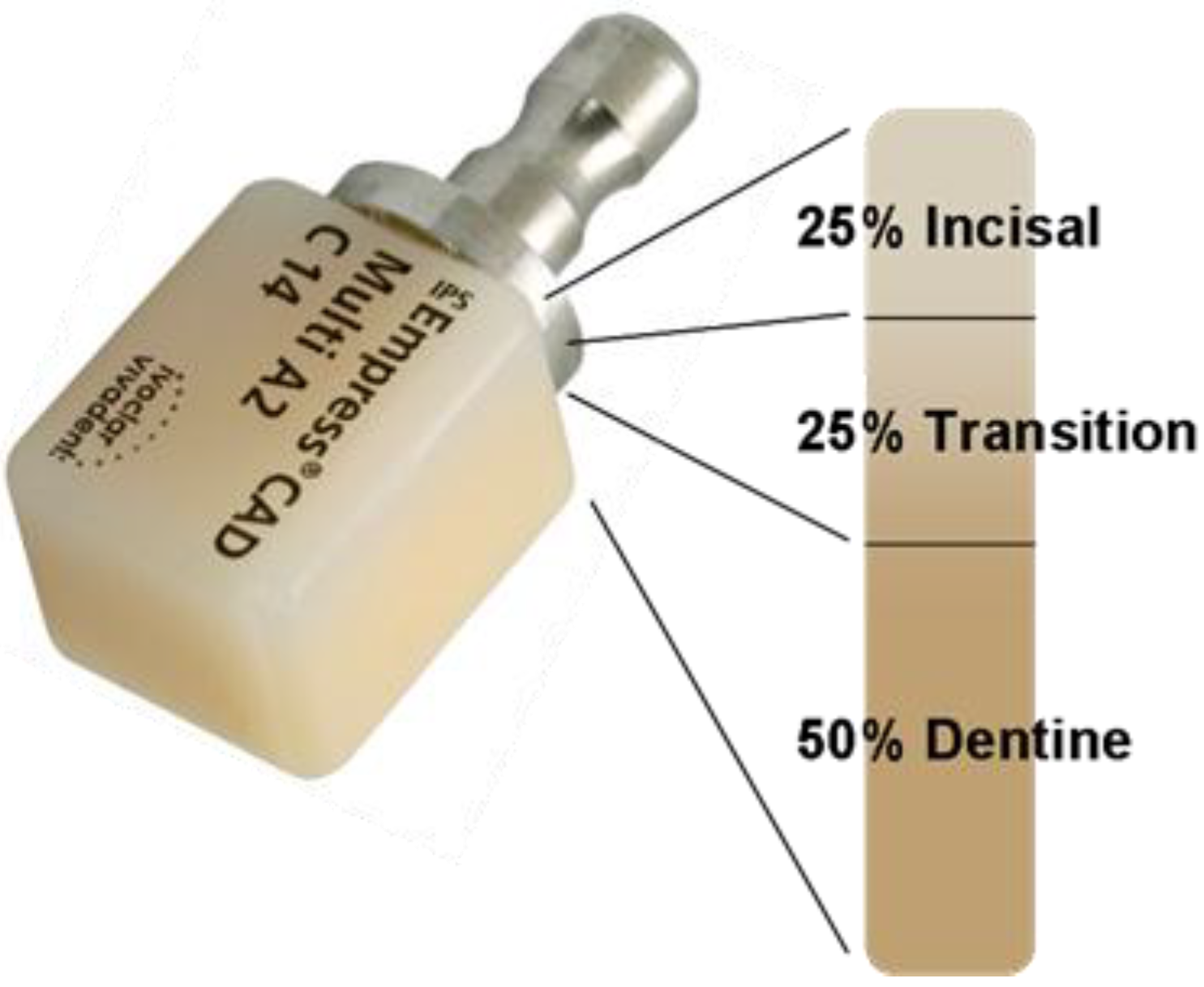
2.1. Type I: Leucite-based glass-ceramics
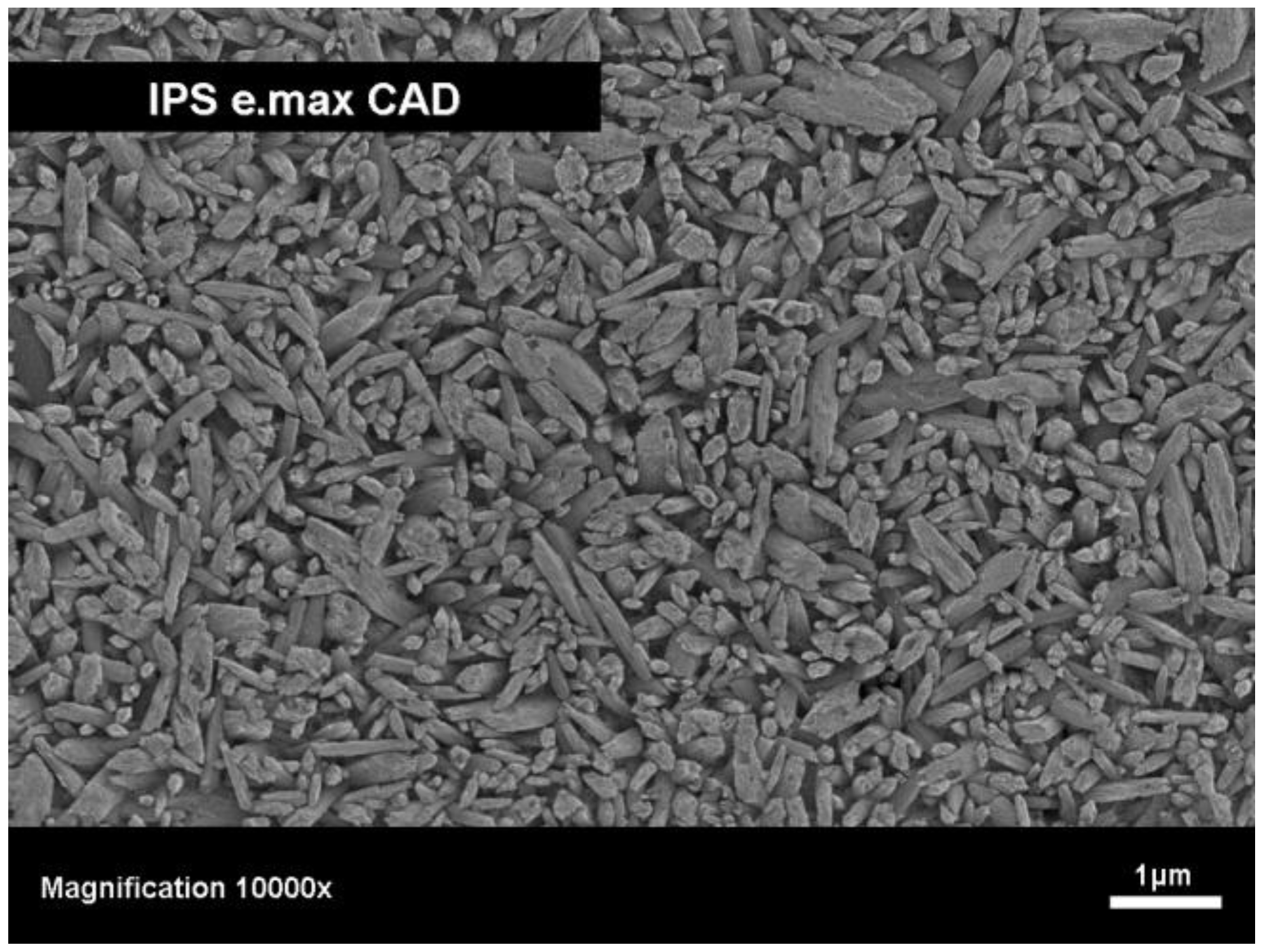
2.2. Type II: Lithium disilicate-based glass-ceramics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties | IPS Empress® CAD | IPS e.max® CAD | |
|---|---|---|---|
| Biaxial flexural strength | MPa | 160 | 300–420 |
| Fracture toughness, KIC | MPa m1/2 | 1.3 | 2.0–2.5 |
| Hardness | MPa | 6200 | 5700–5900 |
| Elastic modulus | GPa | 62 | 90–100 |
| CTE(100–500 °C) | 10-6 K-1 | 17.0–18.0 | 10.2–10.7 |
| Chemical durability (weigth loss in 4% acidic acid) | μg cm-2 | 25 | 30–50 |
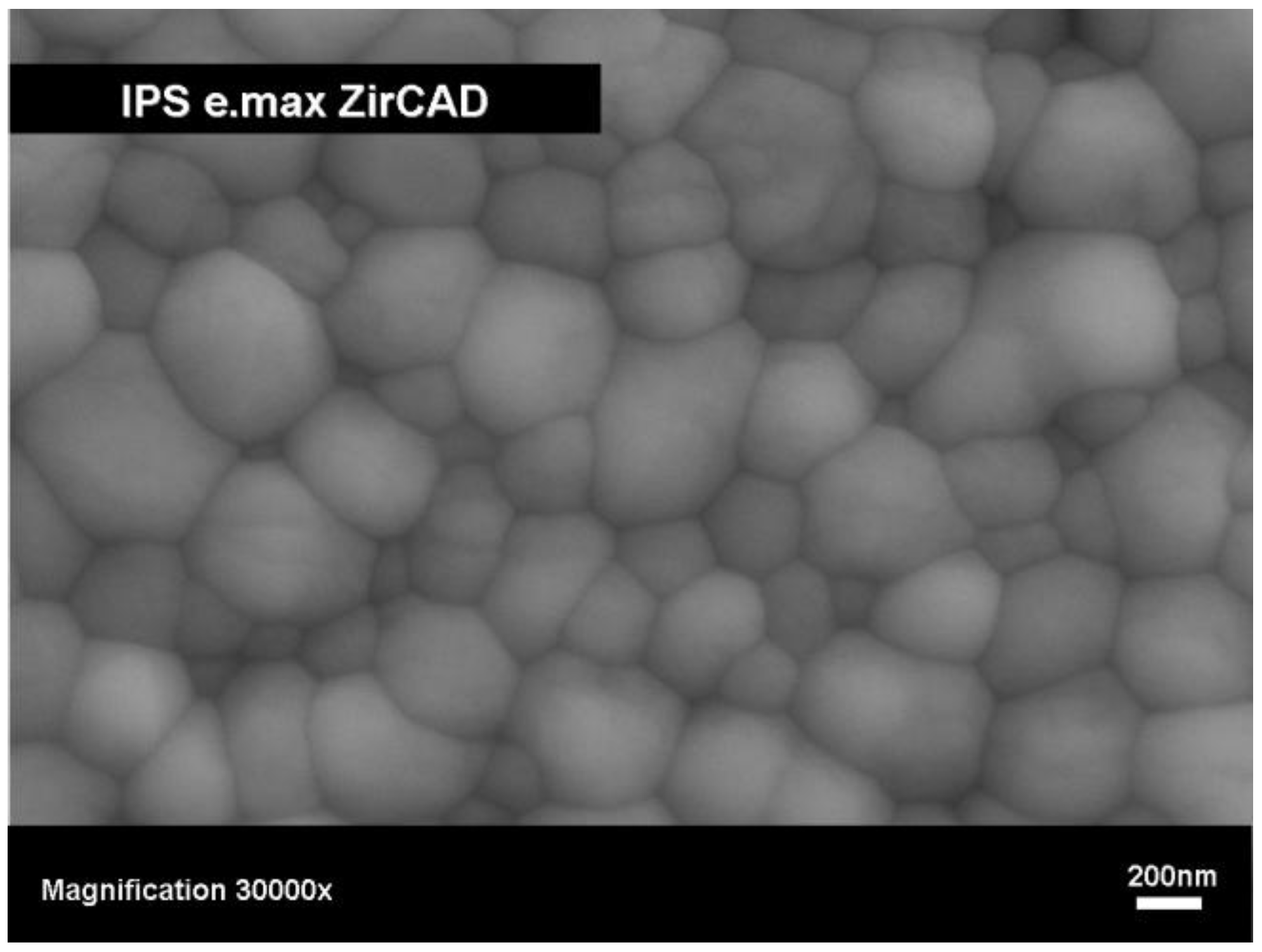
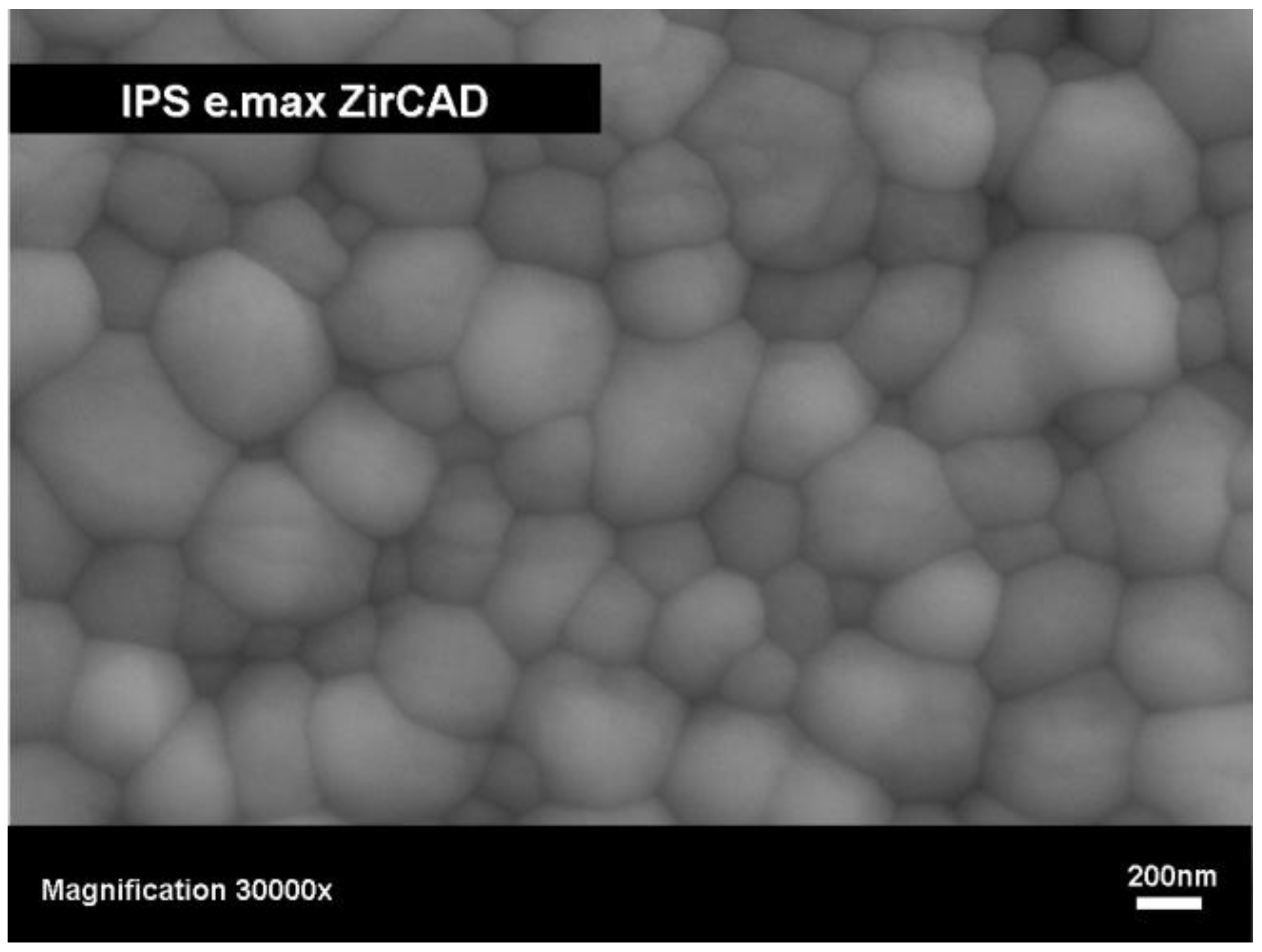
2.3. Type III: Yttrium-stabilized zirconium oxide-based ceramic

| Presintered ZrO2 | Final dense sintered ZrO2 | ||||
|---|---|---|---|---|---|
| Properties | Properties | ||||
| Density | g cm-3 | 3.09–3.21 | Density | g cm-3 | >6.0 |
| Porosity | % | 47.3–49.3 | Porosity | % | <0.5 |
| Biaxial flexural strength | MPa | 50–90 | Biaxial flexural strength | MPa | >900 |
| ZrO2 | wt % | 87.0–95.0 | Fracture toughness, KIC | MPa m1/2 | 5.5 |
| Y2O3 | wt % | 4.0–6.0 | Hardness HV10 | MPa | 13000 |
| HfO2 | wt % | 1.0–5.0 | CTE(100–400°C) | 10-6 K-1 | 10.75 |
| Al2O3 | wt % | 0.1–1.0 | CTE(100–500°C) | 10-6 K-1 | 10.8 |
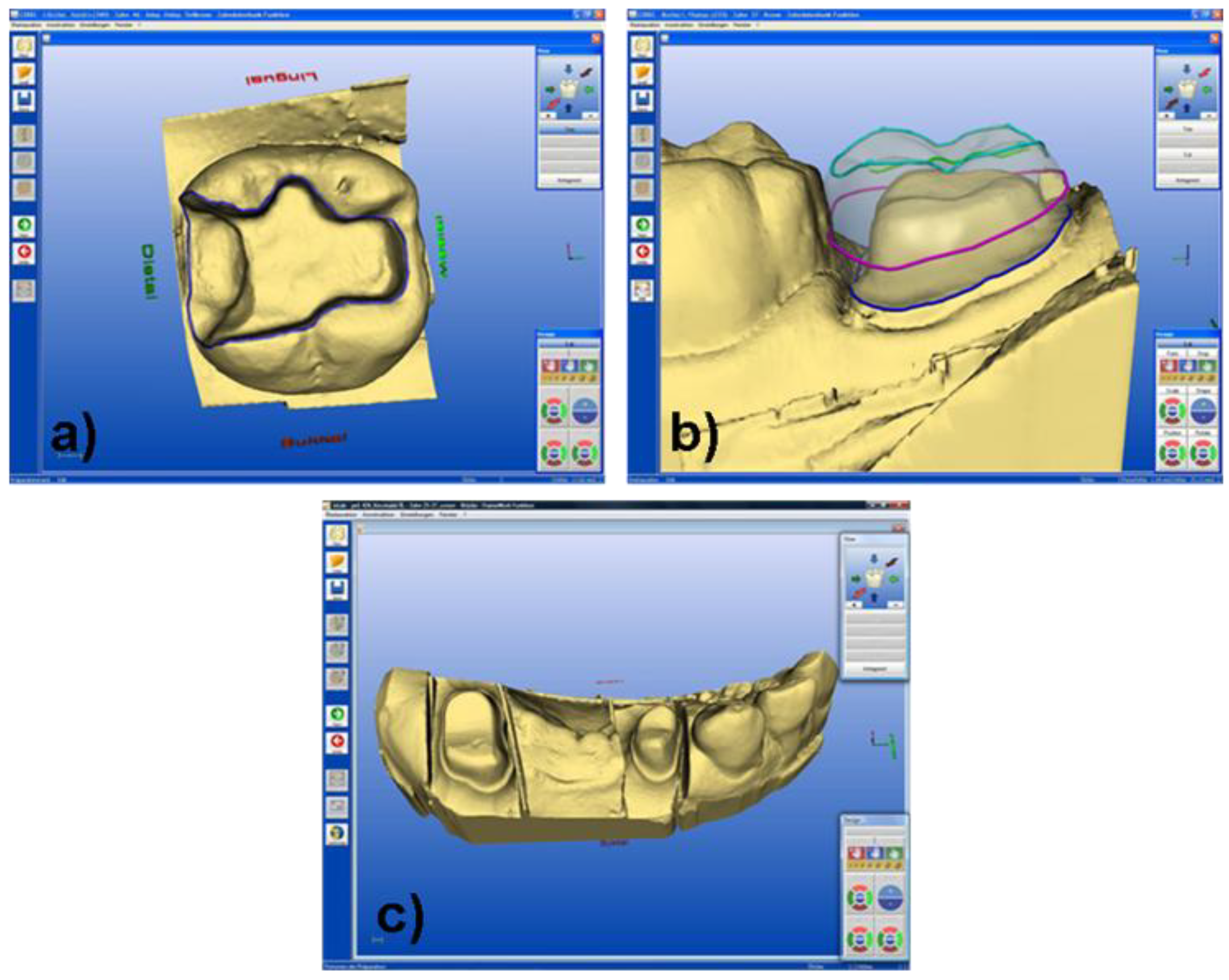
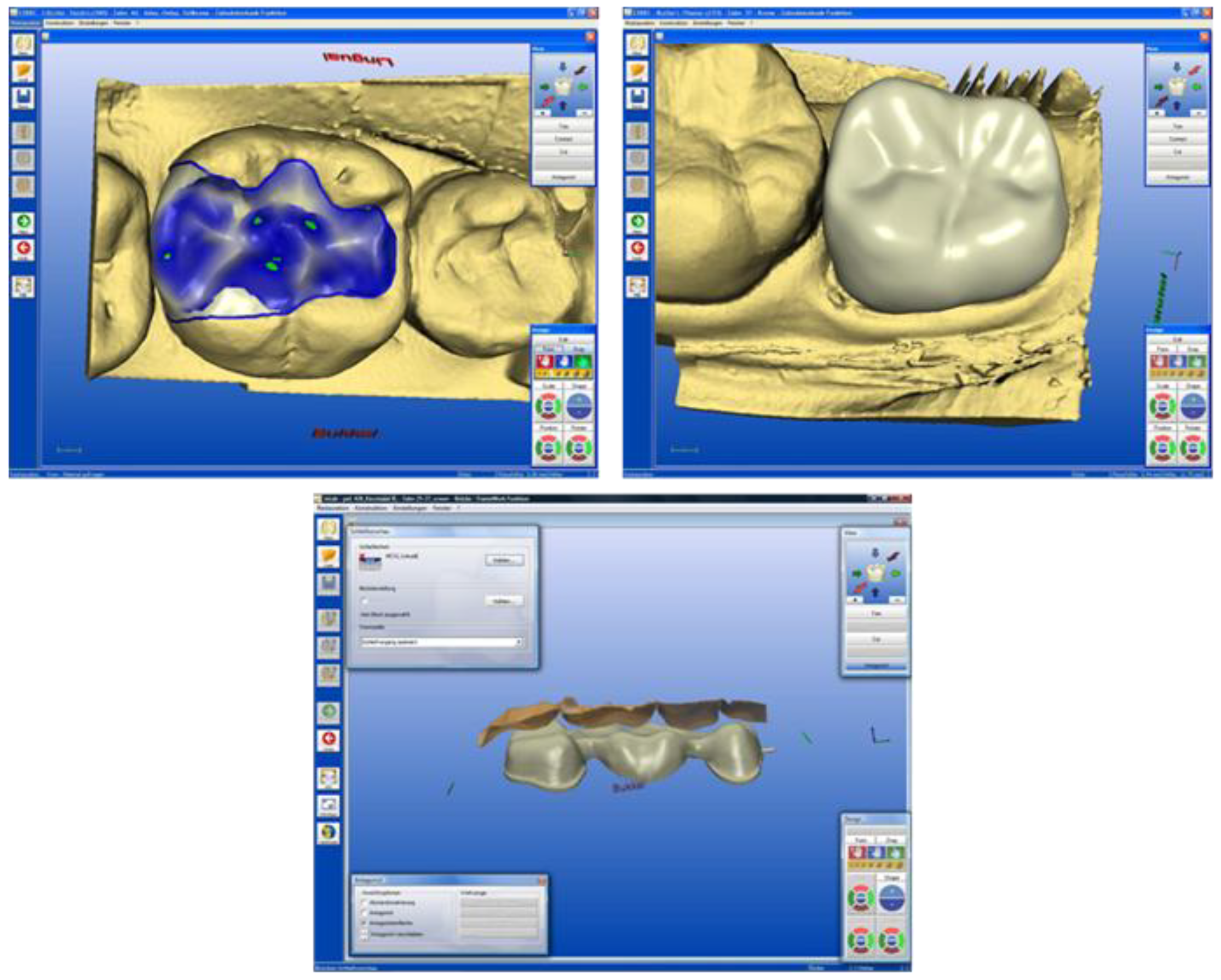
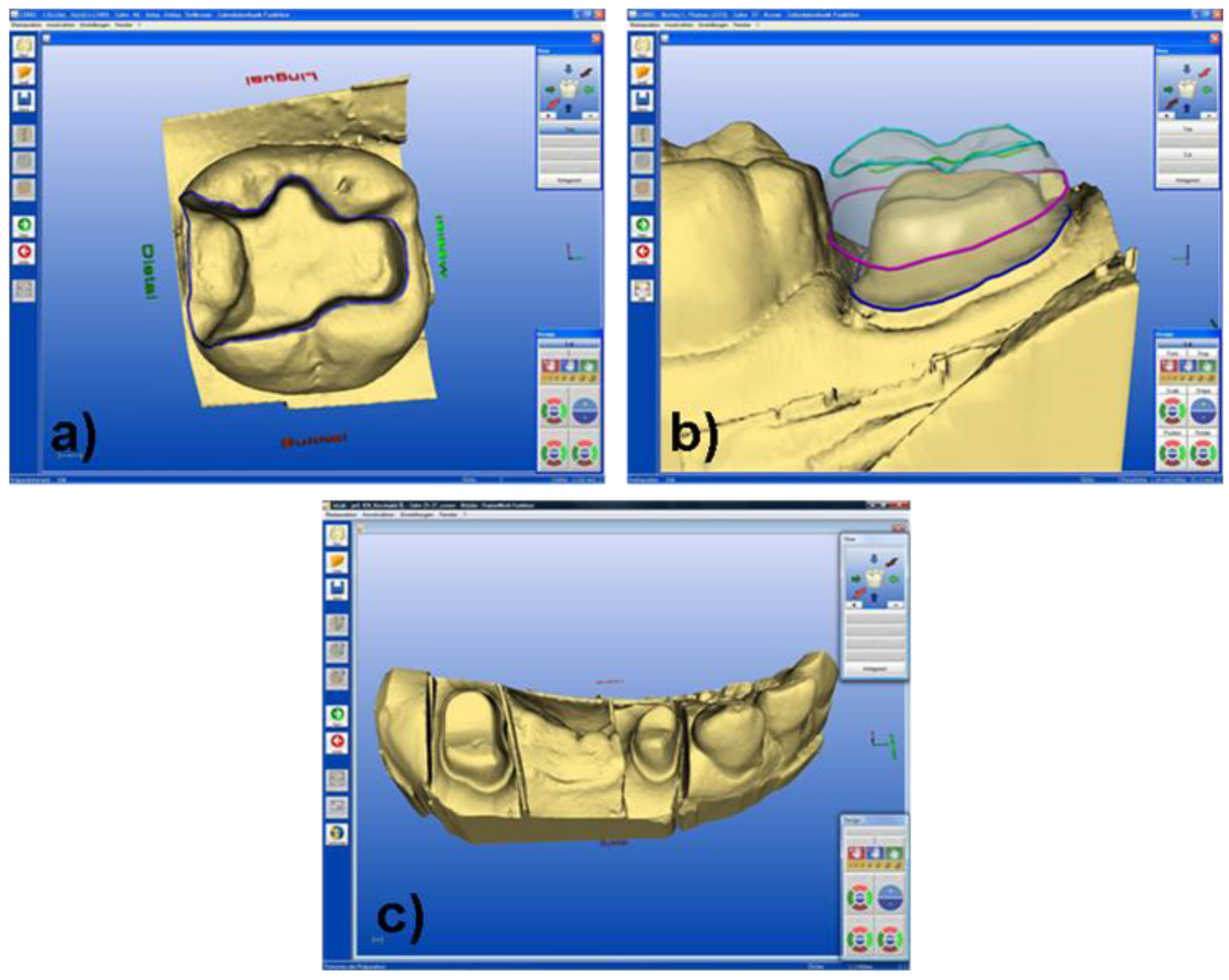
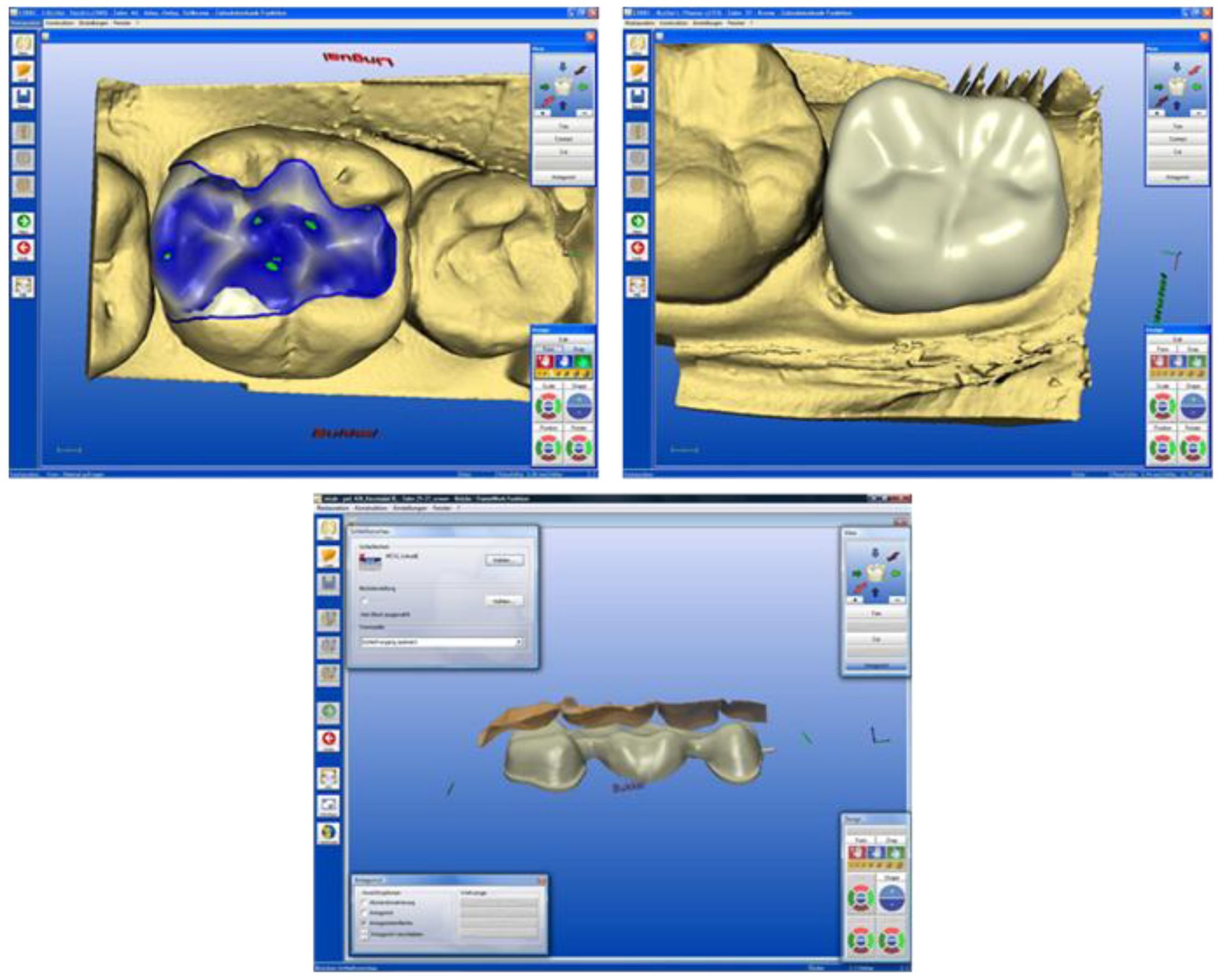
3. Machining Systems using CAD/CAM Technology
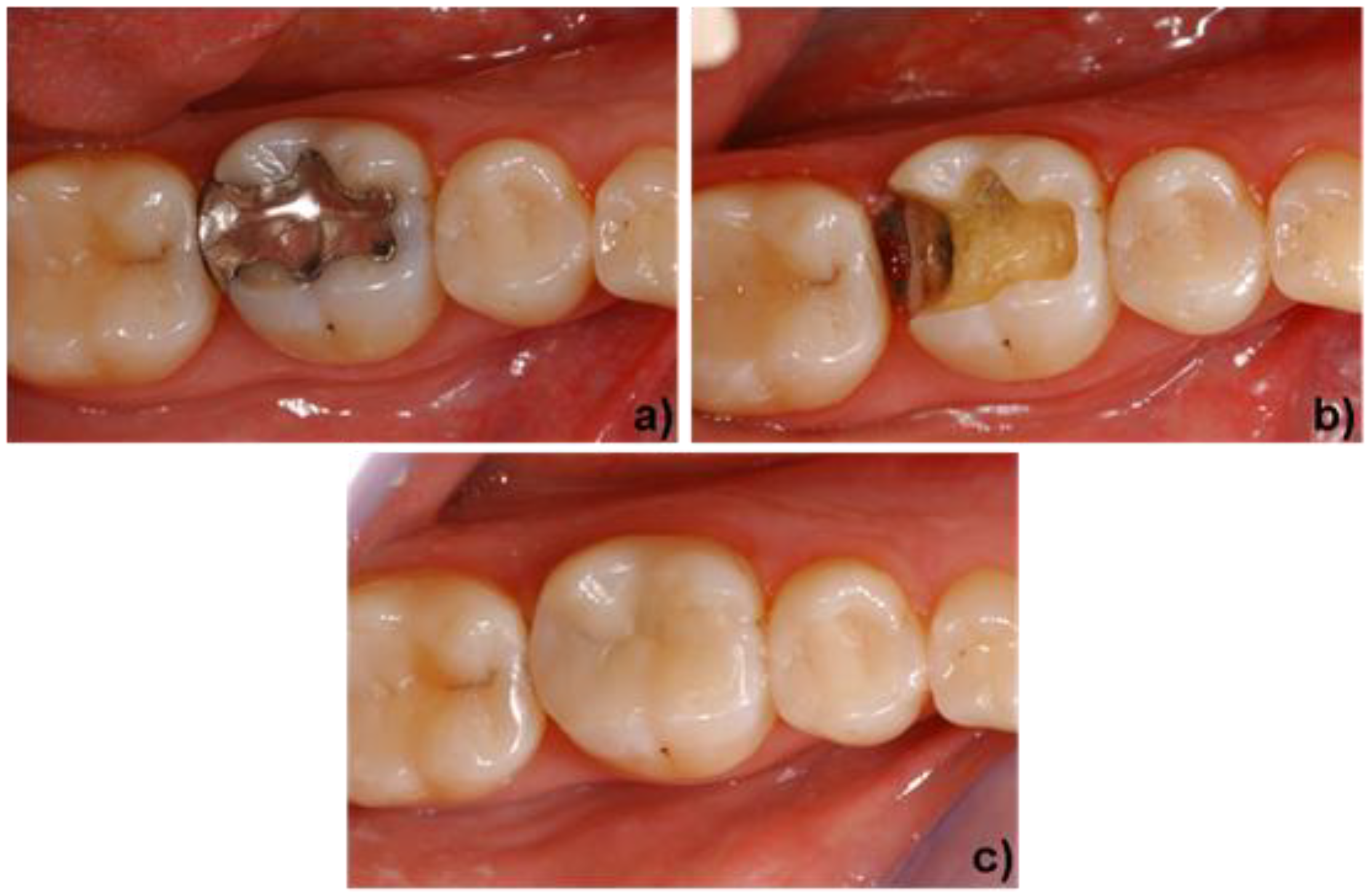
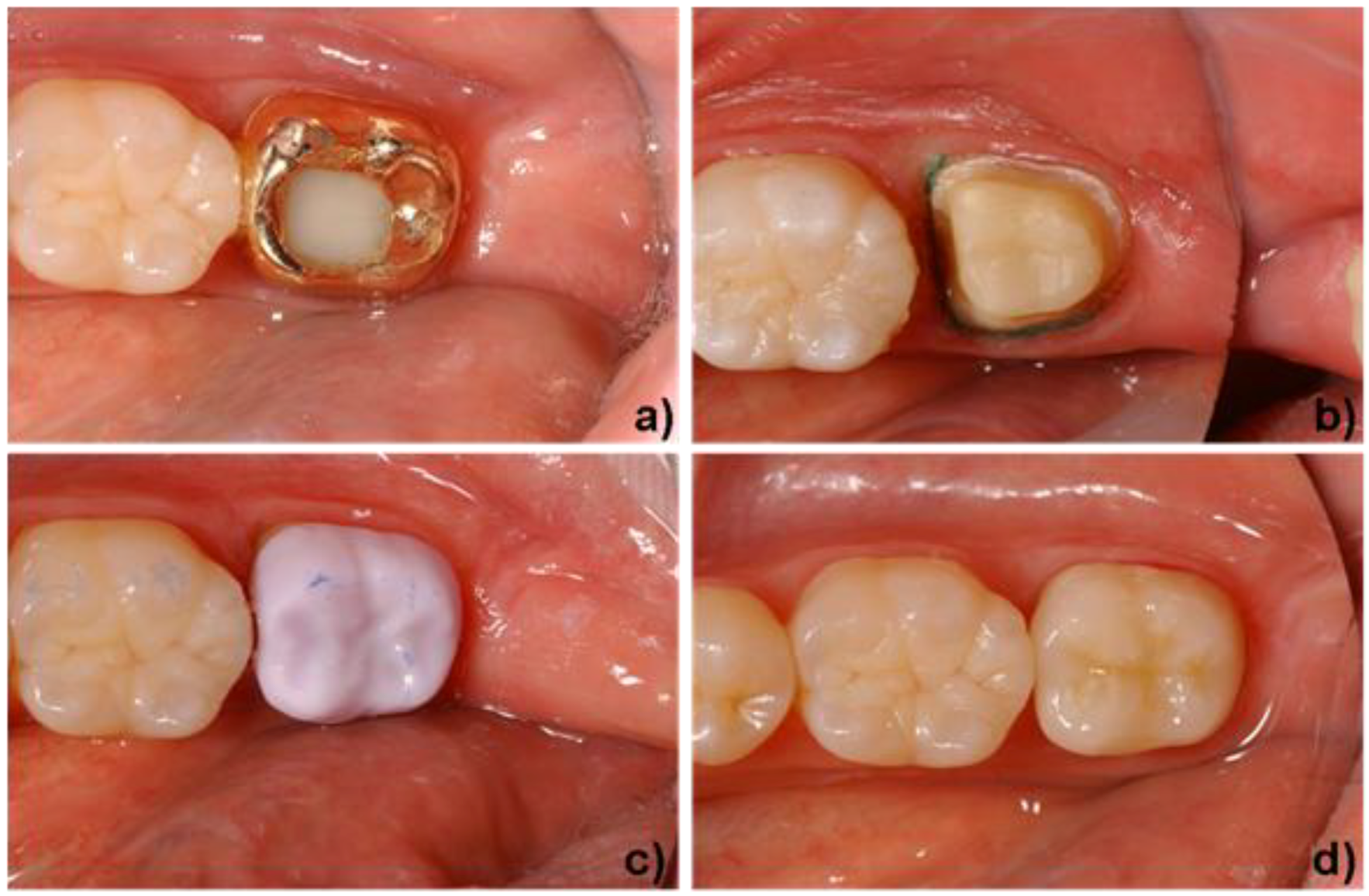
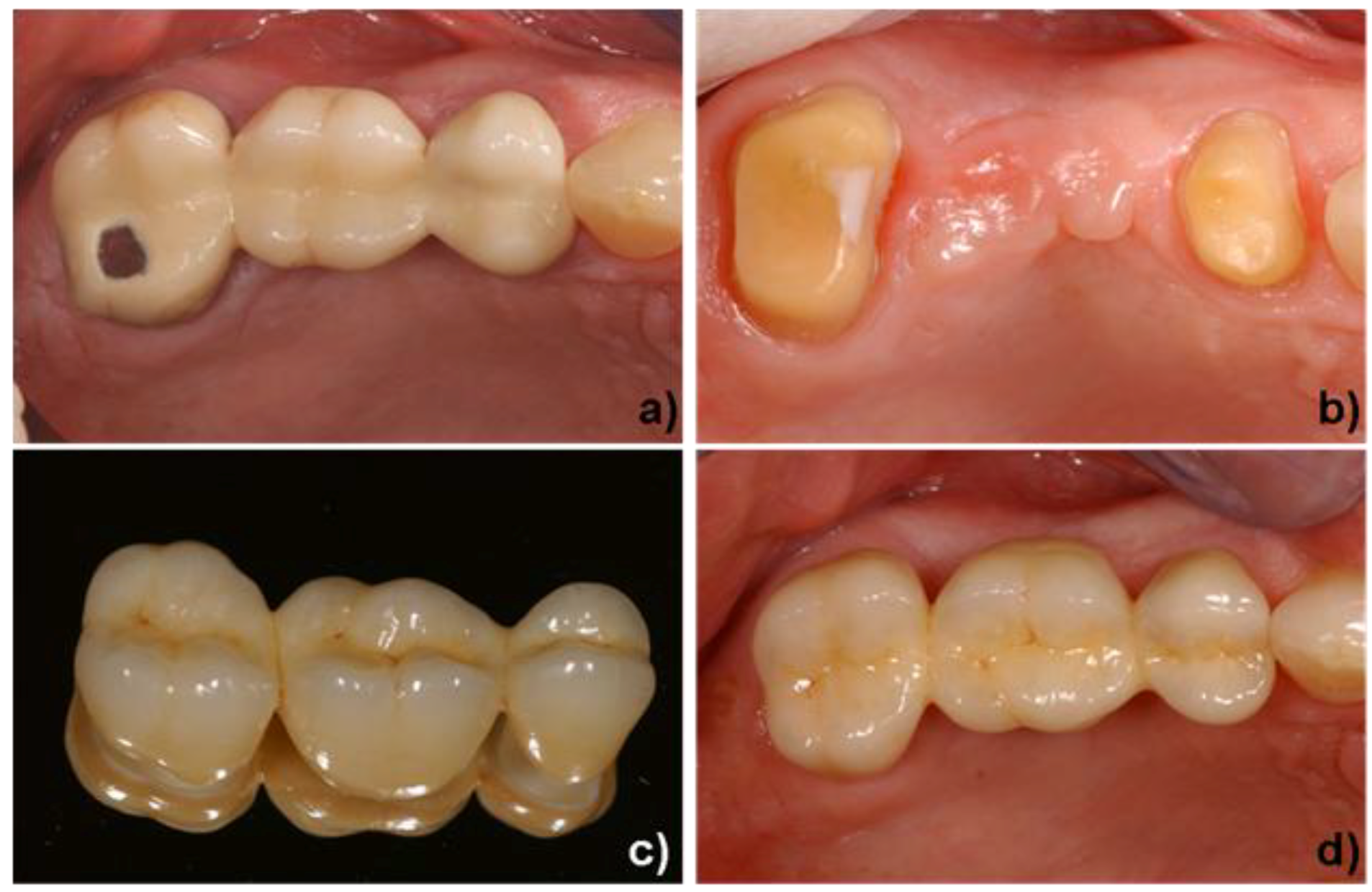
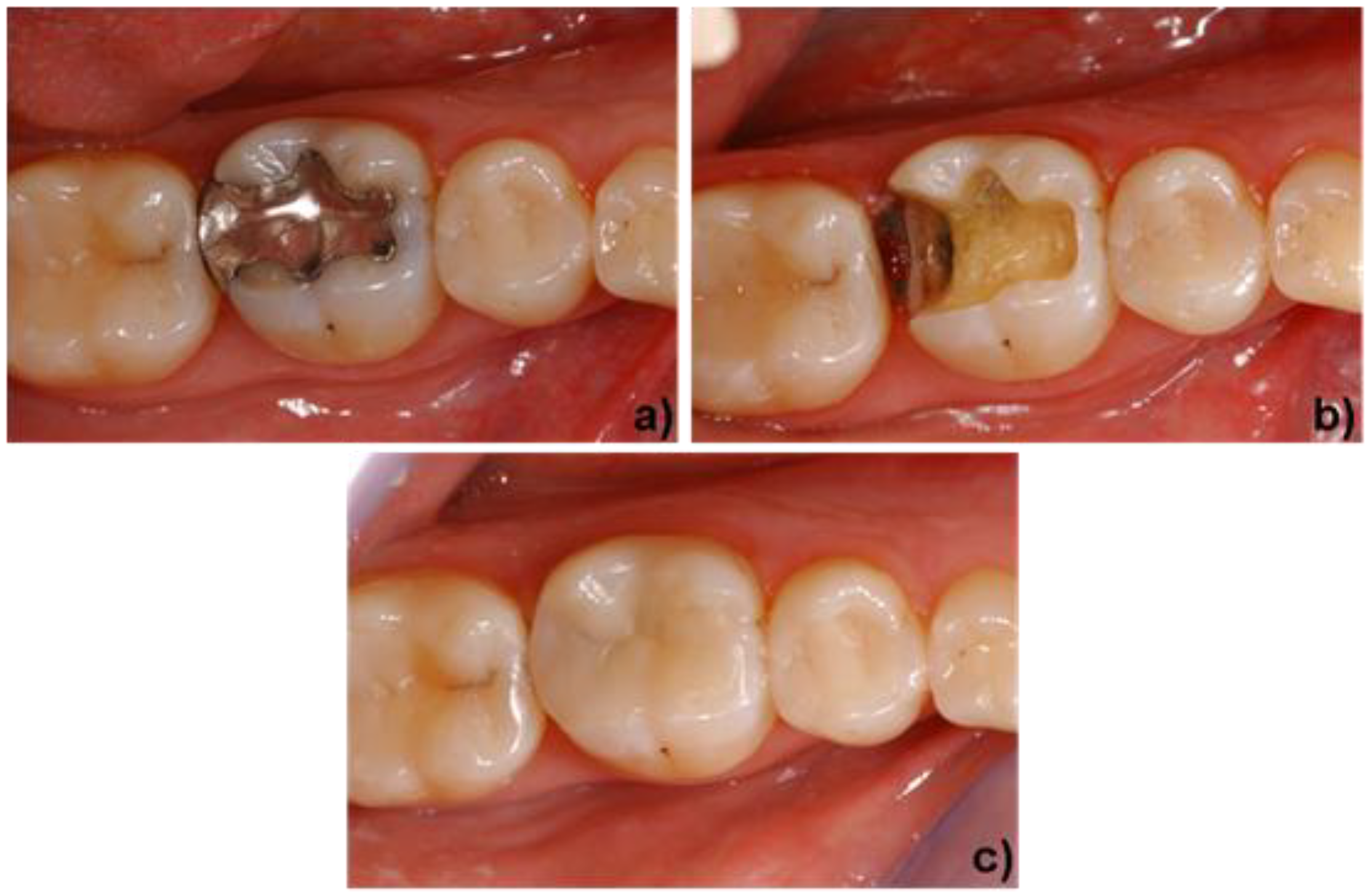
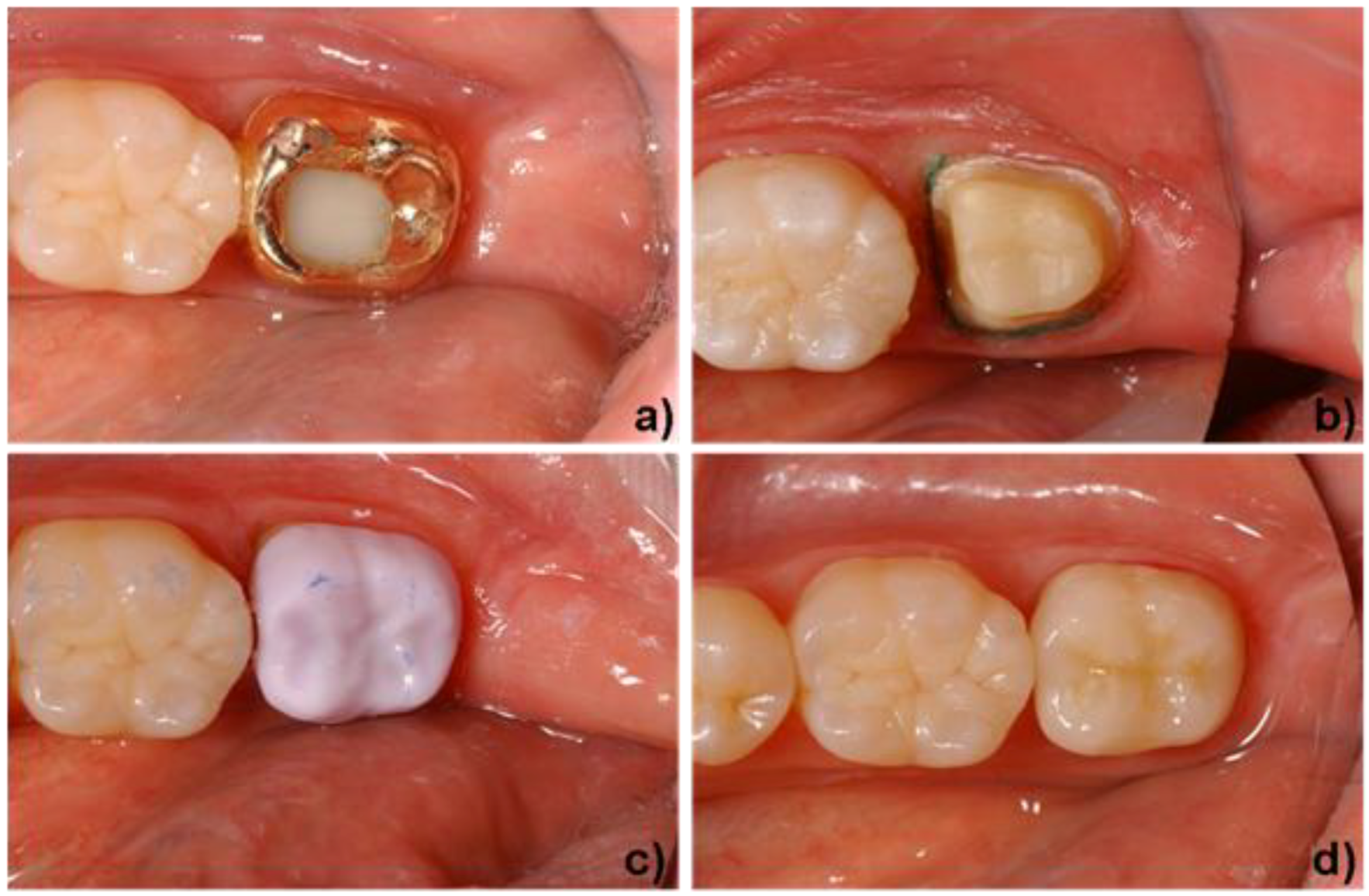
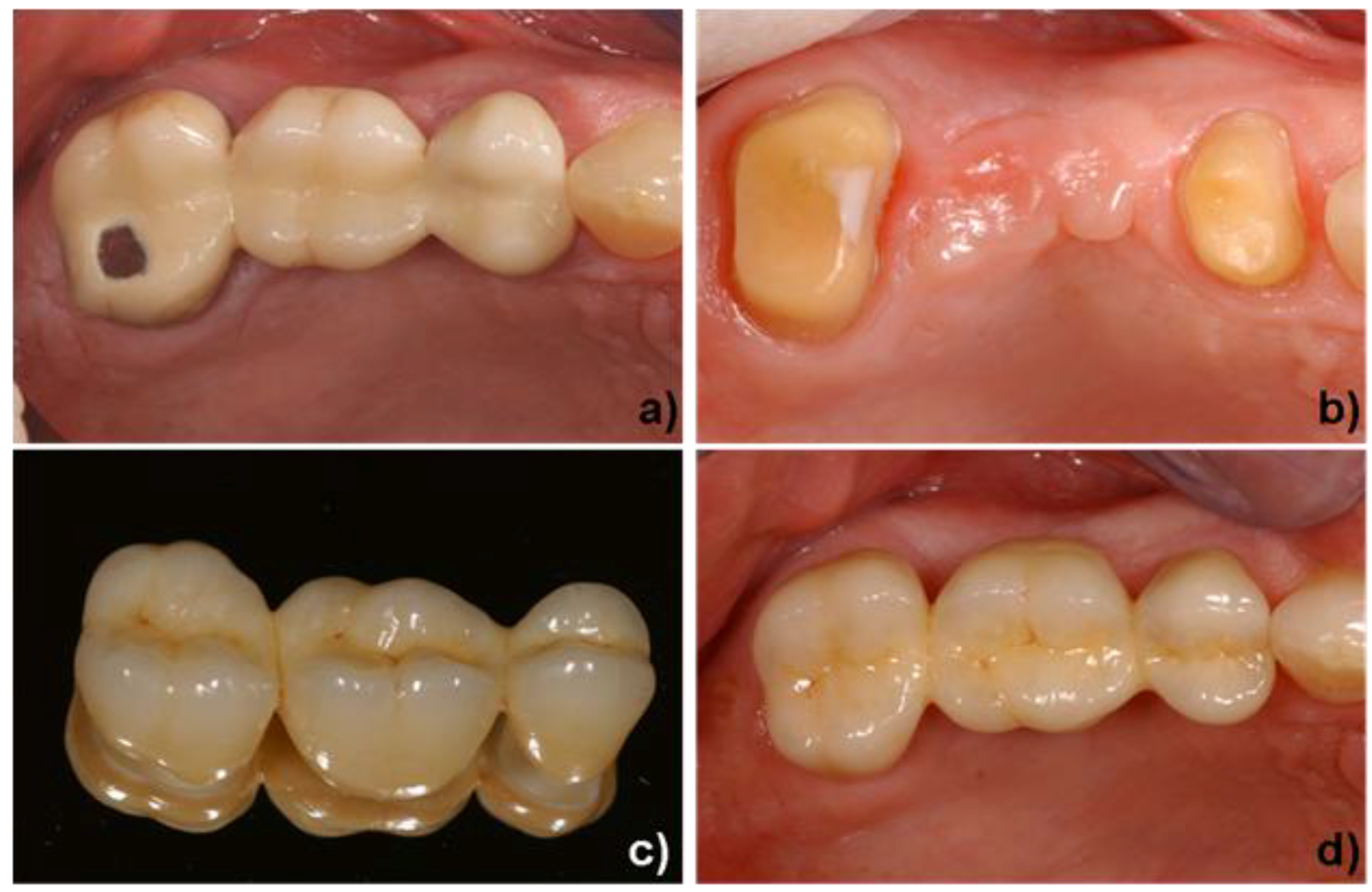
4. Clinical Application
Acknowledgements
References and notes
- Kirsten, H. Die Jacketkrone; Hermann Meusser Verlag: Berlin, Germany, 1929. [Google Scholar]
- Southan, D.E. Die Porzellan-Jacketkrone. In Dental-Keramik Vorträge und Diskussionen; Internationalen Keramik Symposium; Mc Lean, J.W., Ed.; Quintessenz Verlag: Berlin, Germany, 1984; pp. 276–280. [Google Scholar]
- Hoffmann-Axelthelm, W. Geschichte der Zahnheilkunde; Quintessenz Verlag: Berlin, Germany, 1974; pp. 311–333. [Google Scholar]
- Gehre, G. Zahnärztliche Werkstoffe und ihre Verarbeitung. Band 1. Grundlagen und Verarbeitung; Eichner, K., Kappert, H.F., Eds.; Georg Thieme Verlag: Stuttgart, New York, NY, USA, 2005; pp. 362–364. [Google Scholar]
- Kerschbaum, T. Überlebenszeiten von Kronen und Brückenzahnersatz heute. Zahnärztl. Mitt. 1986, 76, 2315–2320. [Google Scholar] [PubMed]
- Kerschbaum, T.; Erpenstein, H. Galvano-keramische Einzelkronen haben sich klinisch bewährt. Zahnärztl. Mitt. 1997, 87, 28–33. [Google Scholar]
- Weinstein, M.; Katz, S.; Weinstein, A.B. Fused Procelain-To-Metal Teeth. U.S. Patent 3,052,982, 1962. [Google Scholar]
- McLean, J.W. Dental Porcelains. In Dental Materials Research; Dickson, G., Cassels, J.M., Eds.; NBS Publication 354; National Bureau of Standards: Washington, DC, USA, 1972. [Google Scholar]
- Wohlwend, A.; Schärer, P. Die empress-technik—ein neues Verfahren zur Herstellung von vollkeramischen Kronen, Inlays und Facetten. Quintessenz Zahntech 1990, 16, 966–978. [Google Scholar]
- Höland, W.; Frank, M. IPS Empress Glaskeramik. In Metallfreie Restaurationen aus Presskeramik; Haller, B., Bischoff, H., Eds.; Quintessenz Verlag: Berlin, Germany, 1993; pp. 147–160. [Google Scholar]
- Mörmann, W.H.; Jans, H.; Brandestini, M.; Ferru, A.; Lutz, F. Computer machined adhesive porcelain inlays: margin adaptation after fatigue stress. J. Dent. Res. 1986, 65. Abstr. 339. [Google Scholar] [PubMed]
- Duret, F. CAD/CAM in dentistry. J. Am. Dent Assoc. 1988, 117, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Rekow, E.D. Prostheses by computer. N.Y. State Dental J. 1988, 54, 21–22. [Google Scholar]
- Höland, W.; Frank, M.; Rheinberger, V.M. Surface Crystallization of Leucite in Glass. J. Non-Cryst. Solids 1995, 180, 292–307. [Google Scholar] [CrossRef]
- Schweiger, M. Materials Properties of IPS Empress. In Presented at Scientific Meeting, Hohenems, Austria, 2006.
- Bühler, P.; Völkel, T.; Scientific documentation of IPS Empress CAD, Ivoclar Vivadent AG, Schaan, Principality of Liechtenstein. 2006.
- Schweiger, M.; Höland, W.; Frank, M.; Drescher, H.; Rheinberger, V.M. IPS Empress 2, a new pressable high strength glass-ceramic for esthetic all ceramic restoration. Quint. Dent. Technol. 1999, 22, 143–152. [Google Scholar]
- Höland, W.; Schweiger, M.; Frank, M.; Rheinberger, V.M. A comparison of the microstructure and properties of the IPS Empress 2 and the IPS Empress glass-ceramic. J. Biomed. Mater. Res. Part B 2000, 53, 297–303. [Google Scholar] [CrossRef]
- Sorensen, J.A.; Cruz, M.; Mito, W.T.; Merrideth, H.; Raffeiner, O. Empress 2 all-ceramic bridge clinical trails. IADR Abstract 902, Symposia Behavioral Sciences & Health Services Research. J. Dent. Res. 1999, 78. [Google Scholar] [PubMed]
- Pospiech, P.; Rountree, P.; Unsöld, F.; Rammelsberg, P. In vitro-investigations on the fracture strength of all-ceramic posterior bridges of Empress II. J. Dent. Res. 1999, 78, 307. [Google Scholar]
- Apel, E.; van’t Hoen, C.; Rheinberger, V.; Höland, W. Influence of ZrO2 on the crystallization and properties of lithium disilicate glass-ceramics derived from a multi-component system. J. Eur. Ceram. Soc. 2007, 27, 1571–1577. [Google Scholar] [CrossRef]
- Höland, W.; Rheinberger, V.; Apel, E.; van’t Hoen, C. Principles and Phenomena of bioengineering with glass-ceramics for dental restoration. J. Eur. Ceram. Soc. 2007, 27, 1521–1526. [Google Scholar] [CrossRef]
- Höland, W.; Apel, E.; van’t Hoen, C.; Rheinberger, V. Studies of crystal phase formations in high-strength lithium disilicate glass-ceramics. J. Non-Cryst. Solids 2006, 352, 4041–4050. [Google Scholar] [CrossRef]
- Höland, W.; Rheinberger, V.; van’t Hoen, C. P2O5 as an effective nucleating agent of lithium disilicate glass-ceramics. J. Inorg. Phophorus Chem. 2005, 19, 36–41. [Google Scholar]
- Ritzberger, C.; Rheinberger, V.; Höland, W.; Apel, E. Hochfeste Glaskeramik, 80. In Presented at Glastechnische Tagung & 8th International Conference “Advances in Fusion and Processing of Glass”, Dresden, Germany, 2006.
- Schweiger, M. Zirkonoxid—hochfeste und bruchzähe Strukturkeramik. Ästhetische Zahnmedizin 2004, 5, 248–257. [Google Scholar]
- Rothbrust, F. IPS e.max ZirCAD; Internal report Ivoclar Vivadent AG: Principality of Liechtenstein, 2006; pp. 17–25. [Google Scholar]
- Höland, W.; Rheinberger, V.; Apel, E.; Ritzberger, C.; Rothbrust, F.; Kappert, H.; Krumeich, F.; Nesper, R. Future perspectives of biomaterials for dental restoration. J. Eur. Ceram. Soc. 2009, 29, 1291–1298. [Google Scholar] [CrossRef]
- Höland, W.; Schweiger, M.; Watzke, R.; Peschke, A.; Kappert, H.F. Ceramics as biomaterials for dental restoration. Expert Rev. Med. Devices 2008, 5, 729–745. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.; Mito, W.T. Rational and clinical technique for esthetic restorations of endodontically treated teeth with the Cosmo Post and IPS Empress Post system. Quint. Dent. Technol. 1998, 21, 81–90. [Google Scholar]
- Wohlwend, A.; Studer, S.; Schärer, P. Das Zirkondioxidabutment - ein neues vollkeramisches Konzept zur ästhetischen Verbesserung der Suprastrukturen in der Implantologie. Quintessenz Zahntech. 1996, 22, 364. [Google Scholar]
- Rühle, M.; Evans, A.G. High toughness ceramics and ceramic composites. Prog. Mat. Sci. 1989, 33, 85–167. [Google Scholar] [CrossRef]
- Deville, S.; Guénin, G.; Chevalier, J. Martensitic transformation in zirconia part I. Nanometer scale prediction and measurement of transformation induced relief. Acta Mater. 2004, 52, 5697–5707. [Google Scholar]
- Deville, S.; Guénin, G.; Chevalier, J. Martensitic transformation in zirconia part II. Martensite growth. Acta Mater. 2004, 52, 5709–5721. [Google Scholar]
- Lange, F.F. Transformation Toughening. J. Mat. Sci. 1982, 17, 247–254. [Google Scholar] [CrossRef]
- Lange, F.F. Transformation-Toughened ZrO2: Correlations between grain size control and composition in the system ZrO2-Y2O3. J. Am. Ceram. Soc. 1986, 69, 240–242. [Google Scholar] [CrossRef]
- Mörmann, W.H. State of the Art of CAD/CAM Restorations; 20 Years of Cerec; Quintessenz-Verlag: Berlin, Germany, 2006. [Google Scholar]
- Mörmann, W.H.; Brandestini, M. Chairside computer-aided direct ceramic inlays. Quintessence Int. 1989, 20, 329. [Google Scholar] [PubMed]
- Mehl, A.; Gloger, W.; Hickel, R. Fully anatomic CAD/CAM-fabrication of tooth restorations with a new precise 3D-scanning system. J. Dent. Res. 2000, 79. Abstr. 3091. [Google Scholar] [PubMed]
- Mörmann, W.H. 20 Jahre keramische CEREC CAD/CAM restaurationen. technischer stand und klinische bewährung. Zahnärztl. Mit. 2006, 96, 58–65. [Google Scholar]
- Reich, S.; Wichmann, M. Unterschiede zwischen den CEREC-3D-Software-Versionen 1000 und 15000. Int. J. Comp. Dent. 2004, 7, 47–60. [Google Scholar]
- Sailer, I.; Pjetursson, B.E.; Zwahlen, M.; Hämmerle, C.H. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 Years. Part II: fixed dental prostheses. Clin. Oral Implants Res. 2007, 18, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Att, W.; Grigoriadou, M.; Strub, J.R. ZrO2 three unit fixed partial dentures: comparison of failure load before and after exposure to a mastication simulator. J. Oral Rehabil. 2007, 34, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Vult von Steyern, P.; Ebberson, S.; Holmgren, J.; Haag, P.; Nilner, K. Fracture strength of two oxide ceramic crown systems after cyclic pre-loading and thermocycling. J. Oral Rehabil. 2006, 33, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Tinschert, J.; Natt, G.; Mautsch, W.; Augthun, M.; Spiekermann, H. Fracture resistance of lithium disilicate-, alumina- and zirconia-based three unit fixed partial dentures: a laboratory study. Int. J. Prosthodont. 2001, 14, 231–238. [Google Scholar] [PubMed]
- Blatz, M.B. Long therm clinical success of all-ceramic posterior restorations. Quintessence Int. 2002, 33, 415–426. [Google Scholar] [PubMed]
- Sailer, I.; Feher, A.; Filser, F.; Gauckler, L.J.; Luthy, H.; Hämmerle, C.H. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. [Google Scholar] [PubMed]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ritzberger, C.; Apel, E.; Höland, W.; Peschke, A.; Rheinberger, V.M. Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies. Materials 2010, 3, 3700-3713. https://doi.org/10.3390/ma3063700
Ritzberger C, Apel E, Höland W, Peschke A, Rheinberger VM. Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies. Materials. 2010; 3(6):3700-3713. https://doi.org/10.3390/ma3063700
Chicago/Turabian StyleRitzberger, Christian, Elke Apel, Wolfram Höland, Arnd Peschke, and Volker M. Rheinberger. 2010. "Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies" Materials 3, no. 6: 3700-3713. https://doi.org/10.3390/ma3063700
APA StyleRitzberger, C., Apel, E., Höland, W., Peschke, A., & Rheinberger, V. M. (2010). Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies. Materials, 3(6), 3700-3713. https://doi.org/10.3390/ma3063700