
Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
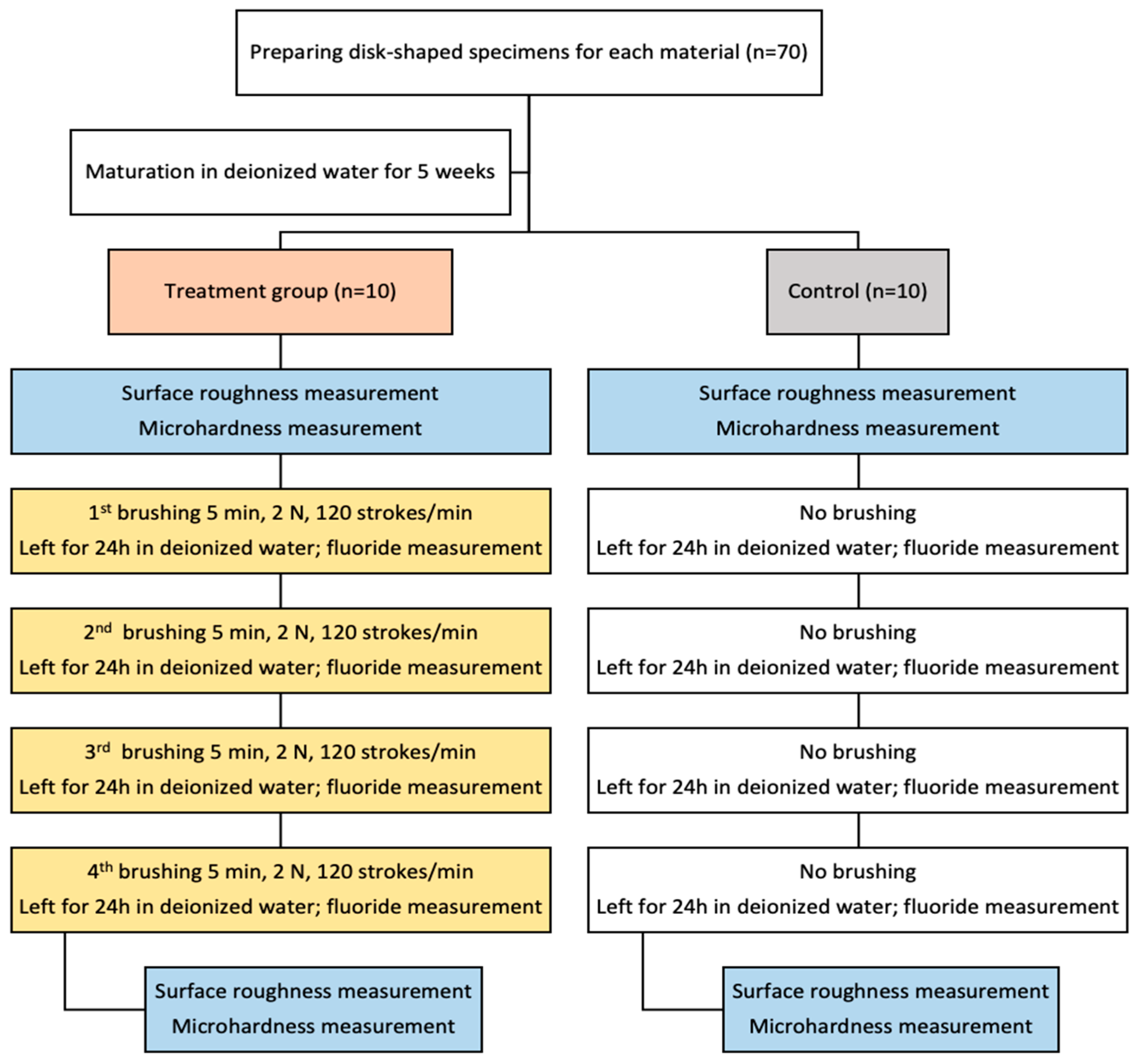
2.1. Specimen Preparation
2.2. Brushing Protocol
2.3. Fluoride Uptake Measurement
2.4. Surface Roughness Determination
2.5. Microhardness Measurement
2.6. Statistical Analysis
3. Results
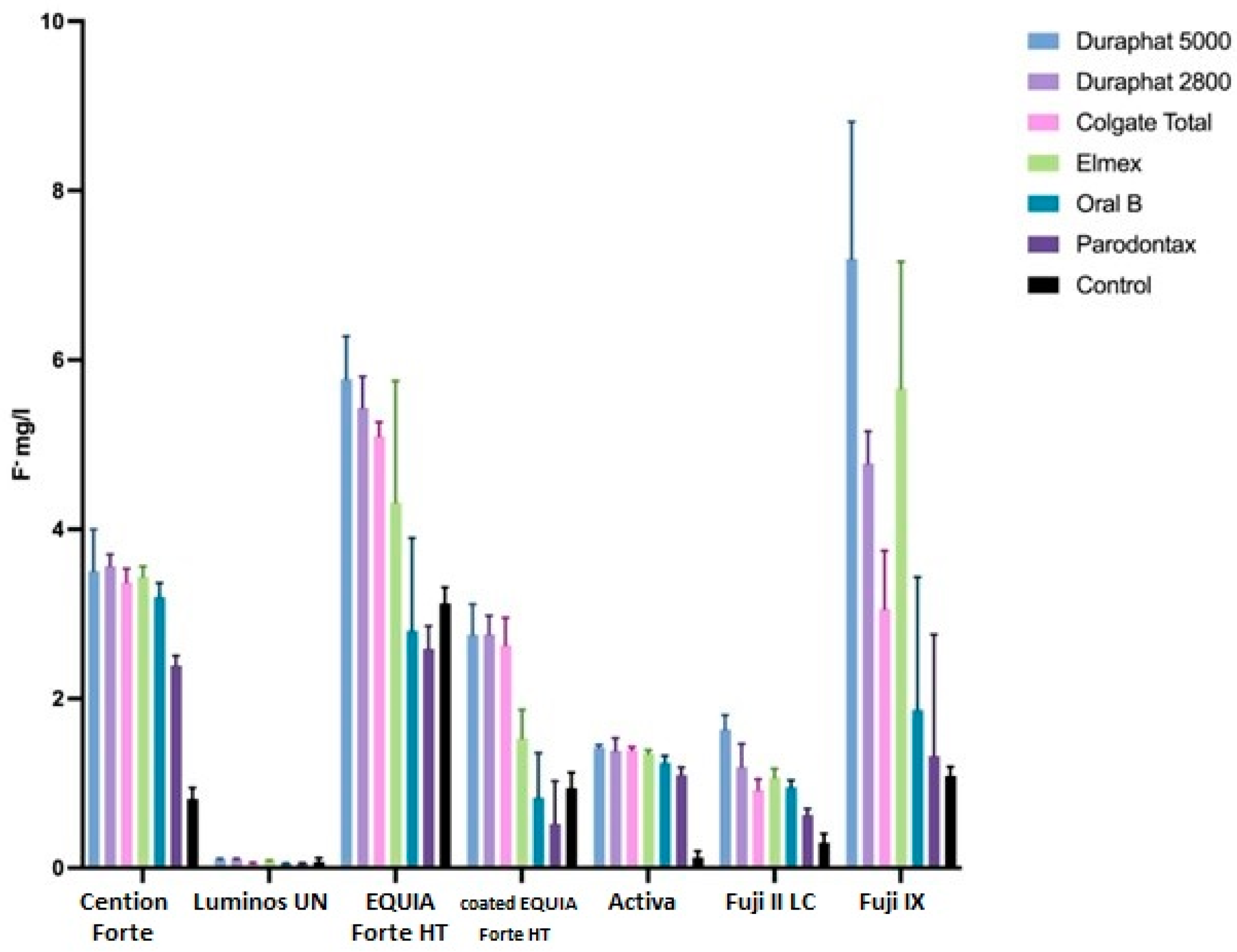
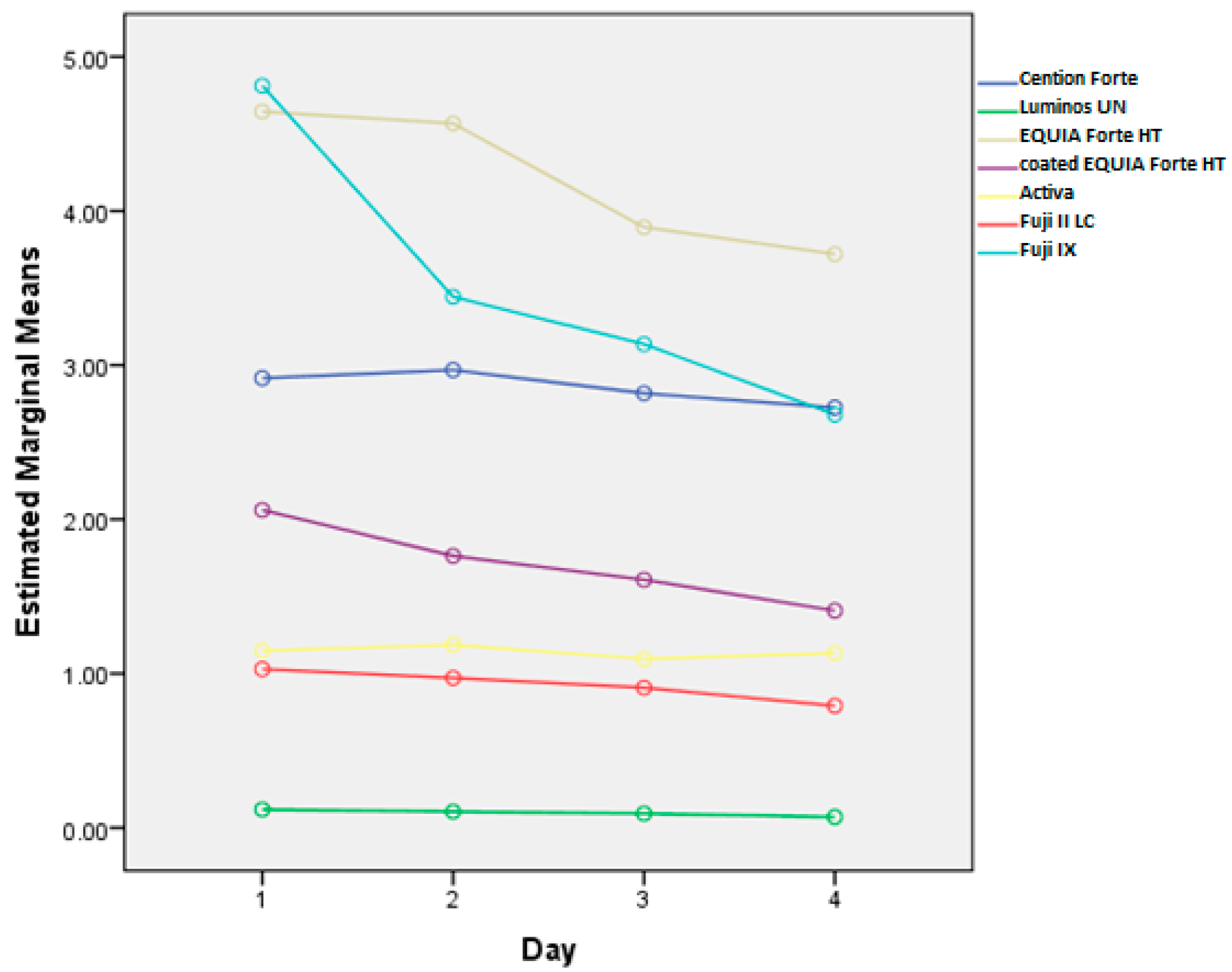
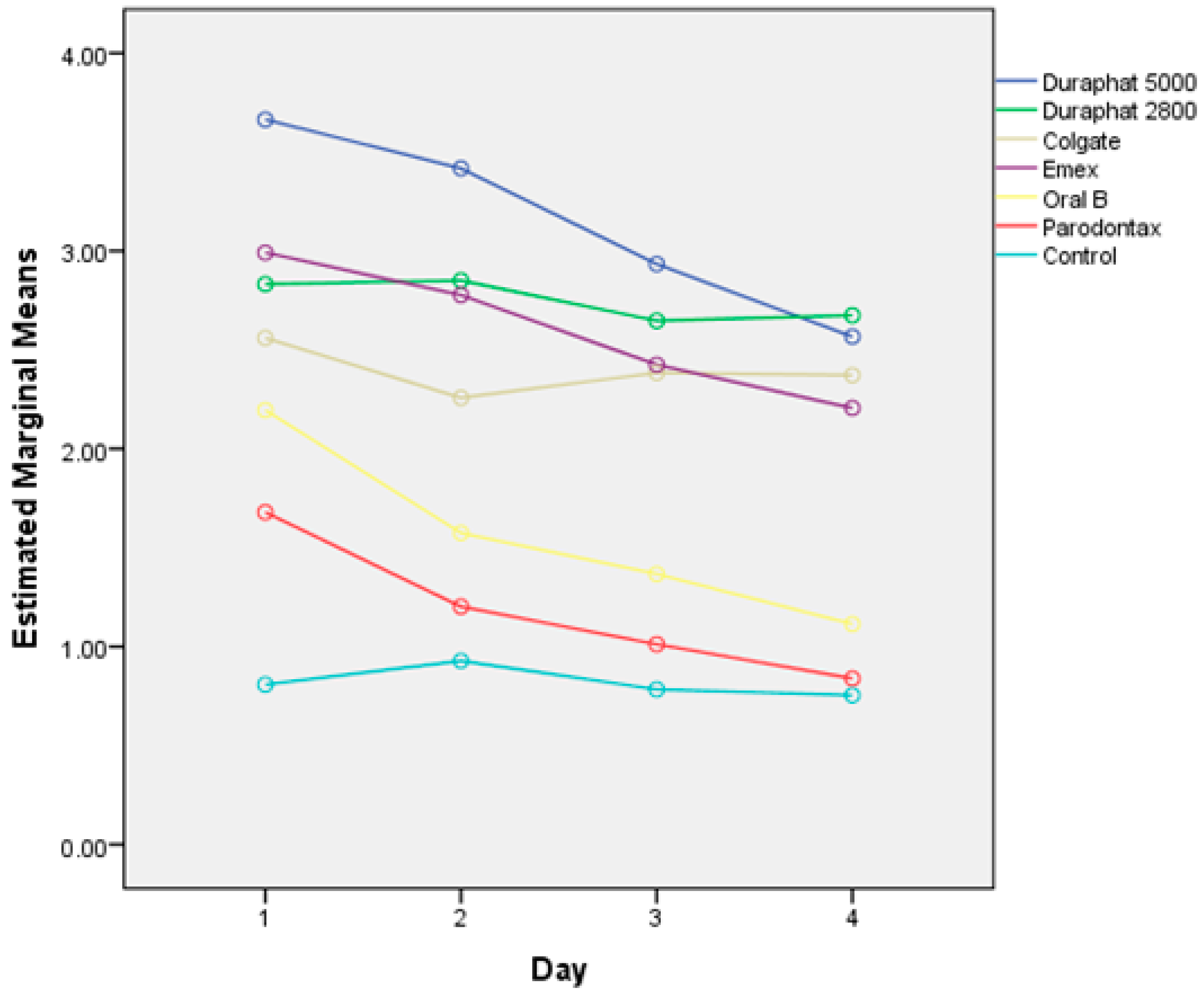
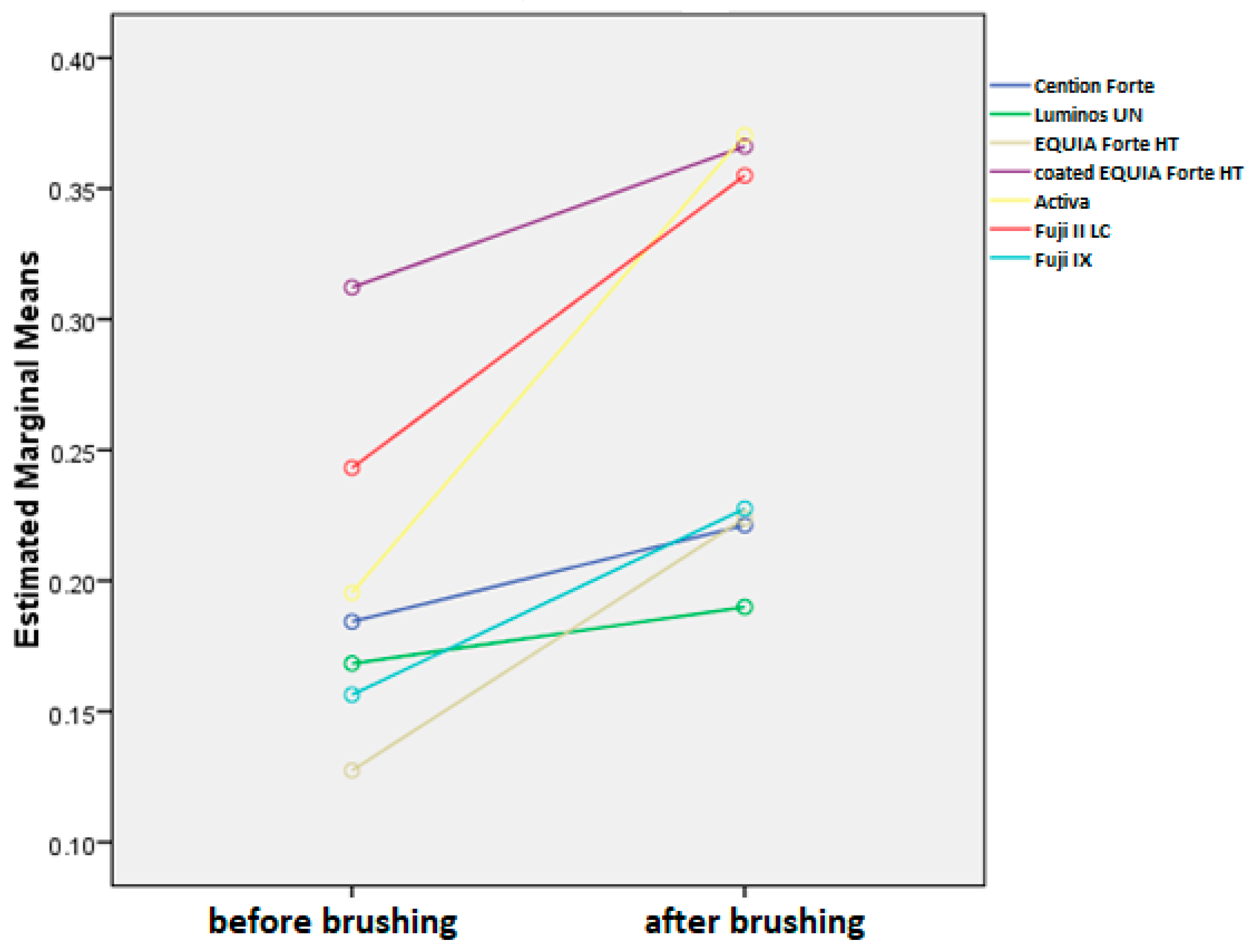
3.1. Fluoride Uptake
3.2. Surface Roughness
3.3. Microhardness Measurement Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GICs | Glass Ionomer Cements |
| NaF | Sodium Fluoride |
| SnF2 | Stannous Fluoride |
| SMFP | Sodium Monofluorophosphate |
| ppm | Parts Per Million |
| UDMA | Urethane Dimethacrylate |
| DCP | Dicalcium Phosphate |
| PEG-400 DMA | Polyethylene Glycol 400 Dimethacrylate |
| Bis-GMA | Bisphenol A Glycidyl Methacrylate |
| TEGDMA | Triethylene Glycol Dimethacrylate |
| HEMA | Hydroxyethyl Methacrylate |
| FAS | Fluoroaluminosilicate |
| RMGIC | Resin-Modified Glass Ionomer Cement |
| HV | Vickers Hardness |
| LSD | Least Significant Difference |
| SPSS | Statistical Package for the Social Sciences |
References
- Duckworth, R.M.; Morgan, S.N. Oral fluoride retention after use of fluoride dentifrices. Caries Res. 1991, 25, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, J.M. Fluorides in caries prevention and control: Empiricism or science. Caries Res. 2004, 38, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Buzalaf, M.A.R.; Pessan, J.P.; Honório, H.M.; Ten Cate, J.M. Mechanisms of action of fluoride for caries control. Monogr. Oral Sci. 2011, 22, 97–114. [Google Scholar] [CrossRef]
- Tokarczuk, D.; Tokarczuk, O.; Kiryk, J.; Kensy, J.; Szablińska, M.; Dyl, T.; Dobrzyński, W.; Matys, J.; Dobrzyński, M. Fluoride Release by Restorative Materials after the Application of Surface Coating Agents: A Systematic Review. Appl. Sci. 2024, 14, 4956. [Google Scholar] [CrossRef]
- Vidal, L.S.B.; Veček, N.N.; Šalinović, I.; Miletić, I.; Klarić, E.; Krmek, S.J. Short-Term Fluoride Release from Ion-Releasing Dental Materials. Acta Stomatol. Croat. 2023, 57, 229–237. [Google Scholar] [CrossRef]
- Tian, K.; Yang, B.; Yue, Y.; Liu, X.; Chu, P.K. Atomic and vibrational origins of mechanical toughness in bioactive cement during setting. Nat. Commun. 2015, 6, 8631. [Google Scholar] [CrossRef]
- Francois, P.; Fouquet, V.; Attal, J.P.; Dursun, E. Commercially Available Fluoride-Releasing Restorative Materials: A Review and a Proposal for Classification. Materials 2020, 13, 2313. [Google Scholar] [CrossRef]
- Ilie, N. Comparative Effect of Self- or Dual-Curing on Polymerization Kinetics and Mechanical Properties in a Novel, Dental-Resin-Based Composite with Alkaline Filler. Materials 2018, 11, 108. [Google Scholar] [CrossRef]
- De Moor, R.G.; Verbeeck, R.M.; De Maeyer, E.A. Fluoride release profiles of restorative glass ionomer formulations. Dent. Mater. 1996, 12, 88–95. [Google Scholar] [CrossRef]
- Wilson, A.D.; Groffman, D.M.; Kuhn, A.T. The release of fluoride and other chemical species from glass ionomers. Biomaterials 1985, 6, 431–433. [Google Scholar] [CrossRef]
- Freedman, R.; Diefenderfer, K.E. Effects of daily fluoride exposures on fluoride release by glass ionomer-based restoratives. Oper. Dent. 2003, 28, 178–185. [Google Scholar] [PubMed]
- Forsten, L. Short- and long-term fluoride release from glass ionomers and other fluoride-containing filling materials in vitro. Scand. J. Dent. Res. 1990, 98, 179–185. [Google Scholar] [CrossRef] [PubMed]
- O'Mullane, D.M.; Baez, R.J.; Jones, S.; Lennon, M.A.; Petersen, P.E.; Rugg-Gunn, A.J.; Whelton, H.; Whitford, G.M. Fluoride and Oral Health. Community Dent. Health 2016, 33, 69–99. [Google Scholar] [CrossRef]
- Vranić, E.; Lacević, A.; Mehmedagić, A.; Uzunović, A. Formulation ingredients for toothpastes and mouthwashes. Bosn. J. Basic Med. Sci. 2004, 4, 51–58. [Google Scholar] [CrossRef]
- World Health Organization. Fluoride Toothpaste: Application for Inclusion in the WHO Model List of Essential Medicines. 2021. Available online: https://cdn.who.int/media/docs/default-source/essential-medicines/2021-eml-expert-committee/applications-for-addition-of-new-medicines/a.14_fluoride-toothpaste.pdf?sfvrsn=4eb40f4c_4 (accessed on 15 March 2025).
- Clarkson, J.E.; Ellwood, R.P.; Chandler, R.E. A comprehensive summary of fluoride dentifrice caries clinical trials. Am. J. Dent. 1993, 6, 59–106. [Google Scholar] [PubMed]
- Pashley, D.H.; Tay, F.R. The Effect of Stannous Fluoride on the Sensitivity of Dentin. J. Dent. Res. 2004, 83, 1104–1108. [Google Scholar] [CrossRef]
- Marinho, V.C.; Higgins, J.P.; Logan, S.; Sheiham, A. Fluoride Toothpaste for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2003, 2016, CD002278. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Bruun, C.; Thylstrup, A. Sodium Monofluorophosphate: A Review of the Literature. J. Clin. Dent. 1994, 5, 1–7. [Google Scholar] [PubMed]
- Moda, M.D.; Dos Santos, P.H.; Pini, N.I.P.; Furini, L.N.; Briso, A.L.F.; Assmann, A.; Fagundes, T.C. Effects of Different Toothpastes on the Nanomechanical Properties and Chemical Composition of Resin-Modified Glass Ionomer Cement and Composite Resin Restorations. Dent. J. 2023, 11, 173. [Google Scholar] [CrossRef]
- Gururaj, M.; Shetty, R.; Nayak, M.; Shetty, S.; Kumar, C.V. Fluoride releasing and uptake capacities of esthetic restorations. J. Contemp. Dent. Pract. 2013, 14, 887–891. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Sidhu, S.K.; Czarnecka, B. Fluoride exchange by glass-ionomer dental cements and its clinical effects: A review. Biomater. Investig. Dent. 2023, 10, 2244982. [Google Scholar] [CrossRef] [PubMed]
- ISO 11609:2010; Dentistry—Dentifrices—Requirements, Test Methods and Marking. International Organization for Standardization: Geneva, Switzerland, 2010.
- Gandolfi, M.G.; Chersoni, S.; Acquaviva, G.L.; Piana, G.; Prati, C.; Mongiorgi, R. Fluoride release and absorption at different pH from glass-ionomer cements. Dent. Mater. 2006, 22, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Hadley, P.C.; Bilington, R.W.; Pearson, G.J. Effect of monovalent ions in glass ionomer on their uptake and re-release. Biomaterials 1999, 20, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.M.; Huang, G.F.; Chang, H.H.; Wang, Y.L.; Guo, M.K. A continuous flow system for assessing fluoride release/uptake of fluoride-containing restorative materials. Dent. Mater. 2004, 20, 740–749. [Google Scholar] [CrossRef]
- Markovic, D.L.J.; Petrovic, B.B.; Peric, T.O. Fluoride content and recharge ability of five glass-ionomer dental materials. BMC Oral. Health 2008, 8, 21. [Google Scholar] [CrossRef]
- Wiegand, A.; Buchalla, W.; Attin, T. Review on fluoride-releasing restorative materials—Fluoride release and uptake characteristics, antibacterial activity, and influence on caries formation. Dent. Mater. 2007, 23, 343–362. [Google Scholar] [CrossRef]
- Creanor, S.L.; Carruthers, L.H.; Saunders, W.P.; Strang, R.; Foye, R.H. Fluoride uptake and release characteristics of glass ionomer cements. Caries Res. 1994, 28, 322–328. [Google Scholar] [CrossRef]
- Preston, A.J.; Mair, L.H.; Agalamanyi, E.A.; Higham, S.M. Fluoride release from aesthetic dental materials. J. Oral. Rehabil. 1999, 26, 123–129. [Google Scholar] [CrossRef]
- Arbabzadeh-Zavareh, F.; Gibbs, T.; Meyers, I.A.; Bouzari, M.; Mortazavi, S.; Walsh, L.J. Recharge pattern of contemporary glass ionomer restoratives. Dent. Res. J. 2012, 9, 139–145. [Google Scholar] [CrossRef]
- Hatibovic-Kofman, S.; Koch, G.; Eksrand, J. Glass ionomer materials as rechargeable fluoride-release system. Int. J. Paediatr. Dent. 1997, 7, 65–73. [Google Scholar] [CrossRef]
- Behrend, B.; Geurtsen, W. Long-term effects of four extraction media on the fluoride release from four polyacid-modified composite resins (compomers) and one resin-modified glass-ionomer cement. J. Biomed. Mater. Res. 2001, 58, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Brenes-Alvarado, A.; Cury, J.A. Fluoride Release from Glass Ionomer Cement and Resin-modified Glass Ionomer Cement Materials under Conditions Mimicking the Caries Process. Oper. Dent. 2021, 46, 457–466. [Google Scholar] [CrossRef]
- Rao, A.; Rao, A.; Sudha, P. Fluoride rechargability of a non-resin auto-cured glass ionomer cement from a fluoridated dentifrice: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2011, 29, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Czarnecka, B.; Nicholson, J.W. Maturation affects fluoride uptake by glass-ionomer dental cements. Dent. Mater. 2012, 28, e1–e5. [Google Scholar] [CrossRef]
- Bueno, L.S.; Borges, A.F.S.; Navarro, M.F.L.; Nicholson, J.W.; Hill, R.G.; Sidhu, S.K. Determination of chemical species of fluoride during uptake mechanism of glass-ionomer cements with NMR spectroscopy. Dent. Mater. 2021, 37, 1176–1182. [Google Scholar] [CrossRef]
- Cabral, M.F.C.; Martinho, R.L.d.M.; Guedes-Neto, M.V.; Rebelo, M.A.B.; Pontes, D.G.; Cohen-Carneiro, F. Do conventional glass ionomer cements release more fluoride than resin-modified glass ionomer cements? Restor. Dent. Endod. 2015, 40, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Neti, B.; Sayana, G.; Muddala, L.; Mantena, S.R.; Yarram, A.; Gvd, H. Fluoride releasing restorative materials: A review. Int. J. Dent. Mater. 2020, 2, 19–23. [Google Scholar] [CrossRef]
- Moshaverinia, M.; de Almeida Queiroz Ferreira, L.; Smidt, G.; Shah, K.C.; Ansari, S.; Moshaverinia, A. Evaluation of mechanical, optical, and fluoride-releasing properties of a translucent bulk fill glass hybrid restorative dental material. J. Esthet. Restor. Dent. 2024, 36, 503–510. [Google Scholar] [CrossRef]
- Moshaverinia, M.; Navas, A.; Jahedmanesh, N.; Shah, K.C.; Moshaverinia, A.; Ansari, S. Comparative evaluation of the physical properties of a reinforced glass ionomer dental restorative material. J. Prosthet. Dent. 2019, 122, 154–159. [Google Scholar] [CrossRef]
- GC America. EQUIA Forte Bulk Fill, Fluoride Releasing, Glass Hybrid Restorative System. Available online: https://www.gcamerica.com/products/operatory/EQUIA_Forte/ (accessed on 18 November 2024).
- Ruengrungsom, C.; Burrow, M.F.; Parashos, P.; Palamara, J.E.A. Evaluation of F, Ca, and P release and microhardness of eleven ion-leaching restorative materials and the recharge efficacy using a new Ca/P containing fluoride varnish. J. Dent. 2020, 102, 103474. [Google Scholar] [CrossRef]
- Neelakantan, P.; John, S.; Anand, S.; Sureshbabu, N.; Subbarao, C. Fluoride release from a new glass-ionomer cement. Oper. Dent. 2011, 36, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Burgess, J.O. Compressive strength, fluoride release, and recharge of fluoride-releasing materials. Biomaterials 2003, 24, 2451–2461. [Google Scholar] [CrossRef]
- Wang, L.; Buzalaf, M.; Atta, M.T. Effect of one-bottle adhesive systems on the fluoride release of a resin-modified glass ionomer. J. Appl. Oral. Sci. 2004, 12, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Mousavinasab, S.M.; Meyers, I. Fluoride release by glass ionomer cements, compomer and giomer. Dent. Res. J. 2009, 6, 75–81. [Google Scholar] [PubMed]
- Zafar, M.S.; Ahmed, N. Therapeutic roles of fluoride released from restorative dental materials. Fluoride 2015, 48, 184–194. [Google Scholar]
- Gui, Y.; Zhao, X.; Li, S.; Tang, L.; Gong, X. Fluoride release and recharge properties of six restorative materials. Zhonghua Kou Qiang Yi Xue Za Zhi 2015, 50, 28–32. [Google Scholar] [PubMed]
- Nicholson, J.W.; Czarnecka, B. The release of ions by compomers under neutral and acidic conditions. J. Oral. Rehabil. 2004, 31, 665–670. [Google Scholar] [CrossRef]
- Williams, J.A.; Briggs, E.; Billington, R.W.; Pearson, G.J. The effects of adding fluoride compounds to a fluoride-free glass ionomer cement on subsequent fluoride and sodium release. Biomaterials 2003, 24, 1301–1308. [Google Scholar] [CrossRef]
- Naoum, S.; Ellakwa, A.; Martin, F.; Swain, M. Fluoride release, recharge and mechanical property stability of various fluoride-containing resin composites. Oper. Dent. 2011, 36, 422–432. [Google Scholar] [CrossRef]
- Weidlich, P.; Miranda, L.A.; Maltz, M.; Samuel, S.M. Fluoride release and uptake from glass ionomer cements and composite resins. Braz. Dent. J. 2000, 11, 89–96. [Google Scholar] [PubMed]
- Faller, R.V.; Noble, W.H. Protection From Dental Erosion: All Fluorides are Not Equal. Compend. Contin. Educ. Dent. 2018, 39, e13–e17. [Google Scholar] [PubMed]
- American Dental Association. Fluoride: Topical and Systemic Supplements. Available online: https://www.ada.org/resources/ada-library/oral-health-topics/fluoride-topical-and-systemic-supplements (accessed on 11 November 2024).
- Hove, L.H.; Holme, B.; Young, A.; Tveit, A.B. The erosion-inhibiting effect of TiF4, SnF2, and NaF solutions on pellicle-covered enamel in vitro. Acta Odontol. Scand. 2007, 65, 259–264. [Google Scholar] [CrossRef]
- Hove, L.H.; Holme, B.; Young, A.; Tveit, A.B. The protective effect of TiF4, SnF2 and NaF against erosion-like lesions in situ. Caries Res. 2008, 42, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Şişmanoğlu, S.; Gümüştaş, B.; Yıldırım-Bilmez, Z. Effect of Polishing Systems on Fluoride Release and Surface Roughness of Different Restorative Materials. Odovtos Int. J. Dent. Sci. 2020, 22, 81–92. [Google Scholar] [CrossRef]
- Jamwal, N.; Rao, A.; Shenoy, R.; Pai, M.; Ks, A.; Br, A. Effect of whitening toothpaste on surface roughness and microhardness of human teeth: A systematic review and meta-analysis. F1000Reseach 2022, 11, 22. [Google Scholar] [CrossRef]
- Dionysopoulos, D.; Tolidis, K.; Sfeikos, T.; Karanasiou, C.; Parisi, X. Evaluation of Surface Microhardness and Abrasion Resistance of Two Dental Glass Ionomer Cement Materials after Radiant Heat Treatment. Adv. Mater. Sci. Eng. 2017, 2017, 5824562. [Google Scholar] [CrossRef]
- Carvalho, L.F.; Alves, L.M.M.; Bergamo, E.T.P.; Benalcazar Jalkh, E.B.; Campos, T.M.B.; Zahoui, A.; Fermino, E.S.; Magalhães, A.C.; Silva, T.L.; Coelho, P.G.; et al. Influence of abrasive dentifrices on polymeric reconstructive material properties after simulated toothbrushing. Biomater. Investig. Dent. 2023, 10, 2268670. [Google Scholar] [CrossRef] [PubMed]
- Kelić, M.; Kilić, D.; Kelić, K.; Šutej, I.; Par, M.; Peroš, K.; Tarle, Z. The Fluoride Ion Release from Ion-Releasing Dental Materials after Surface Loading by Topical Treatment with Sodium Fluoride Gel. J. Funct. Biomater. 2023, 14, 102. [Google Scholar] [CrossRef]
- Yıldız, M.; Bayindir, Y.Z. Fluoride release from conventional glass-ionomer cements and polyacid-modified composite resins. Fluoride 2004, 37, 38–42. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Commercial Name | Type of the Material | Composition | Manufacturer | Lot No. |
|---|---|---|---|---|
| Cention Forte | Alkasite (resin composite with reactive glass fillers) | Urethane Dimethacrylate (UDMA), Dicalcium Phosphate (DCP), Aromatic aliphatic-UDMA, Polyethylene Glycol 400 Dimethacrylate (PEG-400 DMA), Barium aluminium silicate glass, | Ivoclar Vivadent, Schaan, Liechtenstein | Z005MC |
| Luminos UN | Fluoride-containing nano hybrid composite | Bisphenol A Glycidyl Methacrylate/Triethylene Glycol Dimethacrylate (Bis-GMA/TEGDMA) resin, multifunctional filler (including micronized fluoroboroaluminosilicate glass) | UnoDent Ltd., Witham, United Kingdom | 20250225 |
| EQUIA Forte HT, without coat | Glass hybrid | Powder: fluoroaluminosilicate glass, polyacrylic acid, iron oxide Liquid: polybasic carboxylic acid, water | GC Corporation, Tokyo, Japan | 230310B |
| EQUIA Forte HT, with coat | Glass hybrid, covered with resin-based coat | Coat: silica fillers, multifunctional monomers. Powder and liquid same as EQUIA Forte HT. | GC Corporation, Tokyo, Japan | 230310B |
| ACTIVA-BioACTIVE-Restorative | Bioactive composite | Diurethane dimethacrylate (UDMA) and other methacrylate-based monomers, polyacrylic acid/maleic acid copolymer, silanated bioactive glass and calcium, silanated silica, sodium fluoride, aluminoflurosilicate ionomer glass, and water | Pulpodent, Watertown, MA, USA | 160209 |
| Fuji II LC | Resin-modified glass ionomer material | Fluroaluminisilicate glass/ Liquid distilled water, polyacrylic acid, Hydroxyethyl Methacrylate (HEMA), UDMA | GC Corporation, Tokyo, Japan | 230105A |
| Fuji IX GP Extra (Fuji IX) | Conventional glass ionomer material | Liquid: Distilled water, Polyacrylic acid Powder: Fluoroaluminosilicate glass (FAS) | GC Corporation, Tokyo, Japan | 240402A |
| Toothpaste | Manufacturer | Declared Fluoride | Declared ppm F− |
|---|---|---|---|
| Duraphat 5000 | Colgate-Palmolive, Mortagne, France | Sodium fluoride | 5000 |
| Duraphat 2800 | Colgate-Palmolive, Mortagne, France | Sodium fluoride | 2800 |
| Colgate Total | Palmolive, NY, USA | Sodium fluoride | 1450 |
| Oral B Gum & Enamel | Procter & Gamble, Schwalbach TS, Germany | Stannous fluoride, Sodium fluoride | 1100 350 |
| Elmex Sensitive professional | GABA InternationalAG, Therwil, Switzerland | Sodium monofluorophosphate | 1450 |
| Parodontax Classic | Haleon Medical Devices, Dungarvan Co., Waterford, Ireland | No declared fluoride | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banic Vidal, L.S.; Šalinović, I.; Veček, N.N.; Ivica, A.; Miletić, I.; Jukić Krmek, S. Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes. Materials 2025, 18, 2152. https://doi.org/10.3390/ma18092152
Banic Vidal LS, Šalinović I, Veček NN, Ivica A, Miletić I, Jukić Krmek S. Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes. Materials. 2025; 18(9):2152. https://doi.org/10.3390/ma18092152
Chicago/Turabian StyleBanic Vidal, Llubitza Slaviza, Ivan Šalinović, Nikolina Nika Veček, Anja Ivica, Ivana Miletić, and Silvana Jukić Krmek. 2025. "Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes" Materials 18, no. 9: 2152. https://doi.org/10.3390/ma18092152
APA StyleBanic Vidal, L. S., Šalinović, I., Veček, N. N., Ivica, A., Miletić, I., & Jukić Krmek, S. (2025). Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes. Materials, 18(9), 2152. https://doi.org/10.3390/ma18092152