
Short versus Longer Implants in Sites without the Need for Bone Augmentation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Registration
2.2. Reporting Format
- The focused question was formulated following the PICOT format [30], where:
- Patients (P): Patients receiving fixed rehabilitations supported by implants placed in sites without bone augmentation procedures in the mandible and/or the maxilla.
- Intervention (I): dental implants with length ≤ 6 mm.
- Comparison (C): dental implants with length ≥ 8.5 mm.
- Outcome (O): implant survival rate as primary outcome, marginal bone level change, and biological and technical complication rate as secondary outcomes.
- Time (T): follow-up ≥ 1 year from prosthetic loading.
2.3. Focused Question
2.4. Information Sources and Search Strategy
2.5. Outcome Variables
- Marginal bone level change (MBLc), defined as the difference in crestal bone height between baseline and follow-up measures, considered at patient or implant level.
- Technical complication rate, considered at patient level, concerning the number of any technical complication, such as prosthesis fracture, screw loosening or fracture, implant fracture, etc., occurred until the follow-up.
- Biological complication rate, considered at patient level, concerning the number of biological complications, i.e., peri-implant mucositis and peri-implantitis, occurred until the follow-up.
2.6. Eligibility Criteria
- (a)
- RCTs comparing short (≤6 mm) implants in the test group and longer implants (≥8.5 mm) in the control group;
- (b)
- studies with a follow-up period of at least 12 months from prosthetic loading;
- (c)
- studies in which the implants were restored with a fixed prosthesis;
- (d)
- studies where both test and control implants were placed exclusively in sites without the need for bone augmentation in the mandible and/or maxilla.
- (a)
- preclinical in vitro or animal studies;
- (b)
- case reports and case series;
- (c)
- prospective and retrospective observational studies;
- (d)
- non-randomized controlled trials;
- (e)
- reviews and meta analysis;
- (f)
- studies with insufficient information for any quantitative analysis.
2.7. Population Characteristics
2.8. Study Selection and Data Extraction
2.9. Meta-Analysis
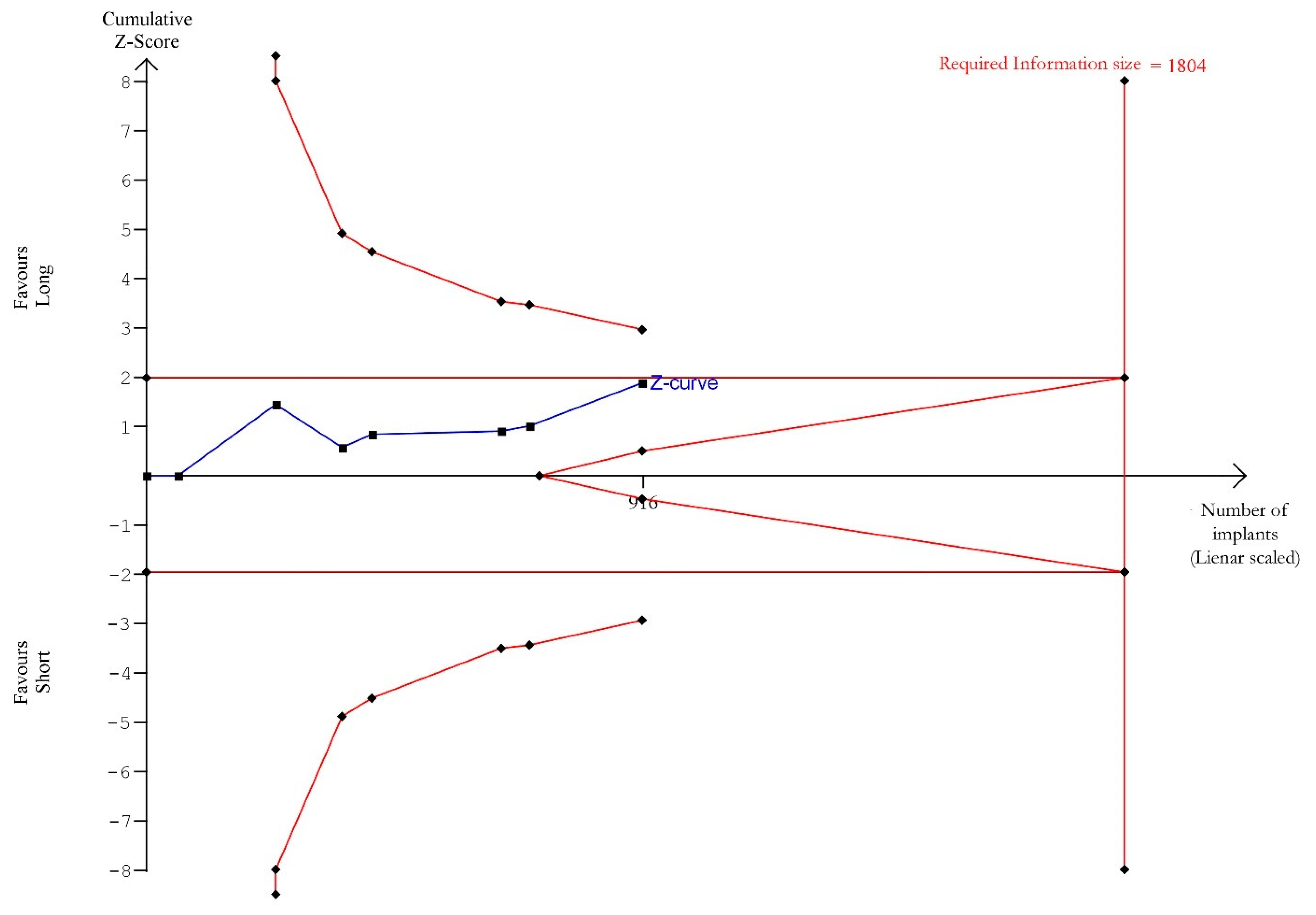
2.10. Trial Sequential Analysis
2.11. Risk of Bias and Quality of Evidence
3. Results
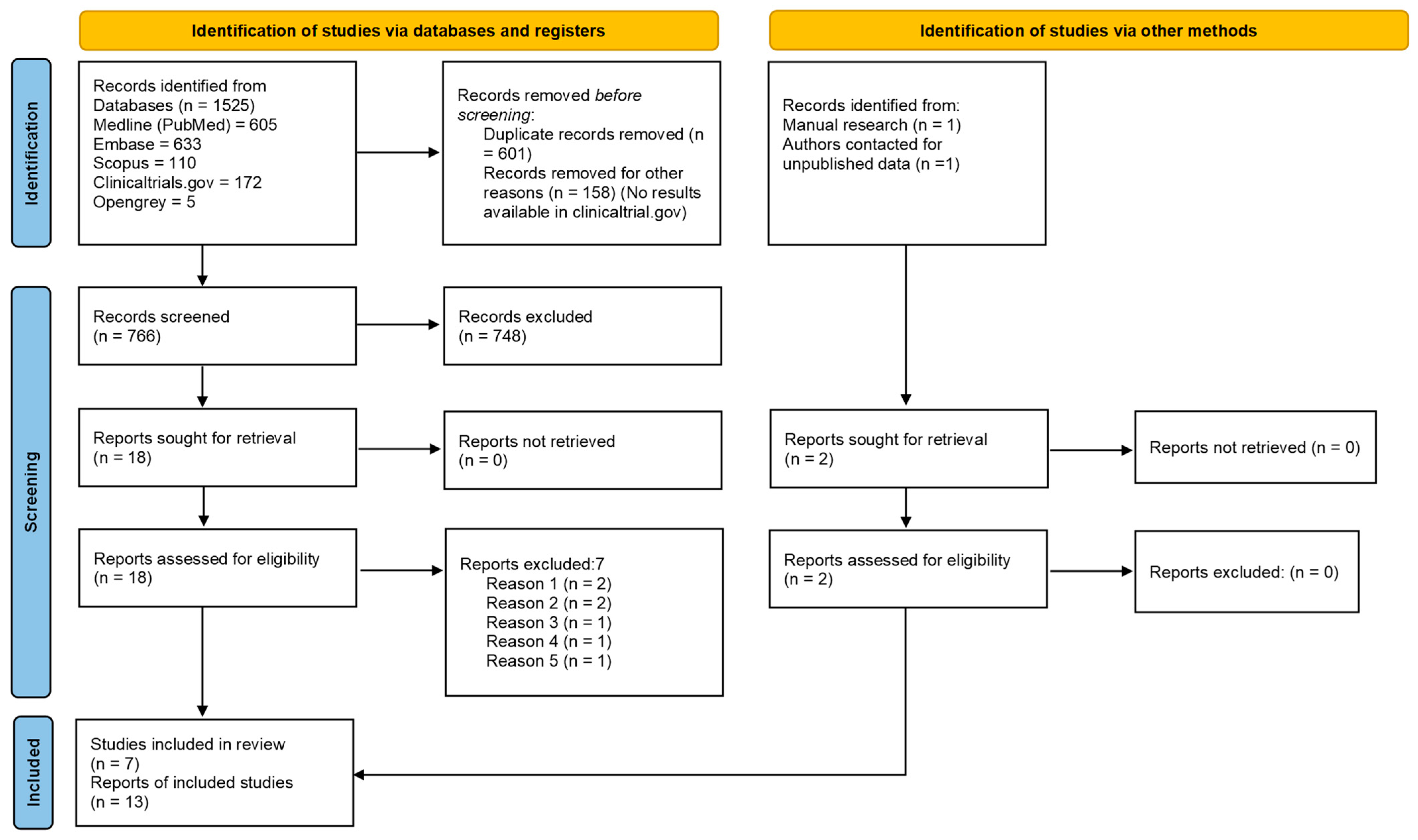
3.1. Study Selection
3.2. Characteristics of the Included Articles
3.3. Risk/Confounding Factors
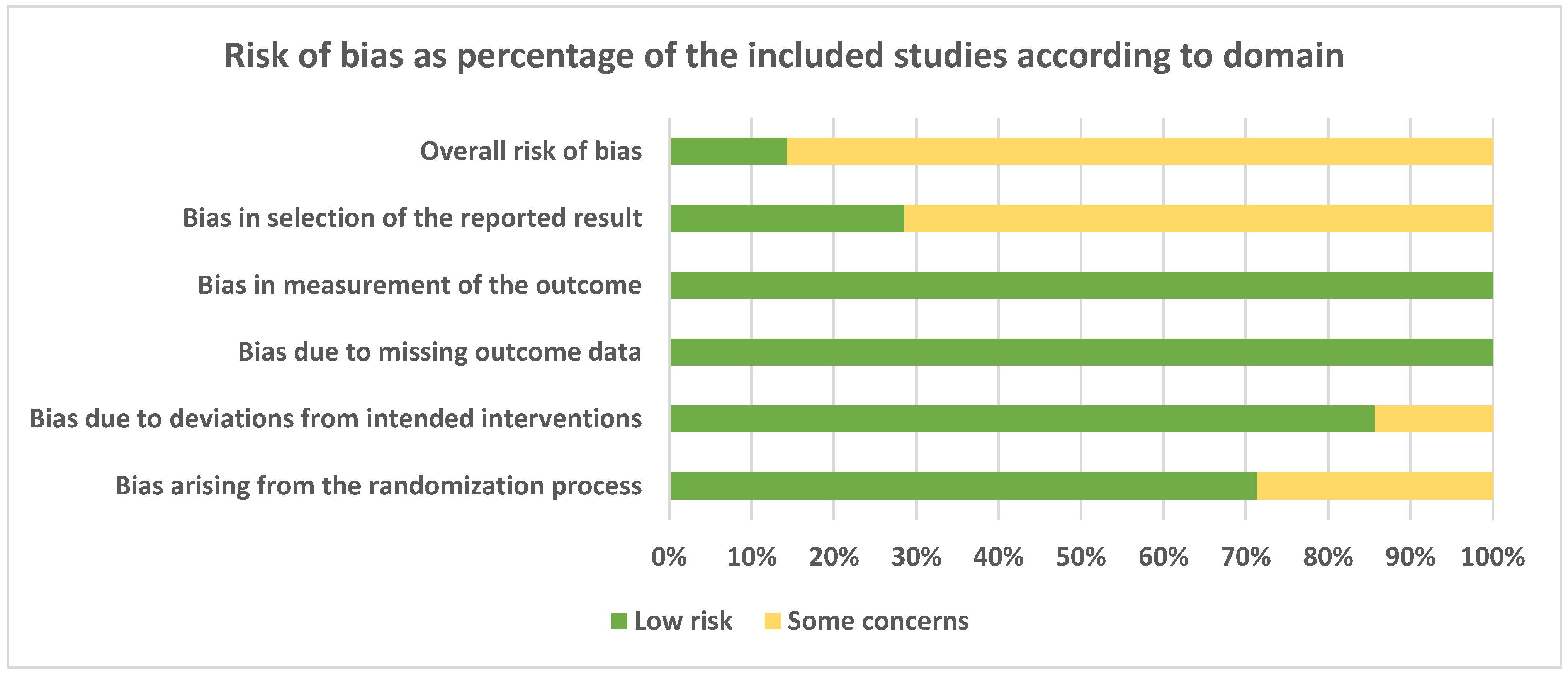
3.4. Risk of Bias and Quality of Evidence
3.5. Meta-Analysis
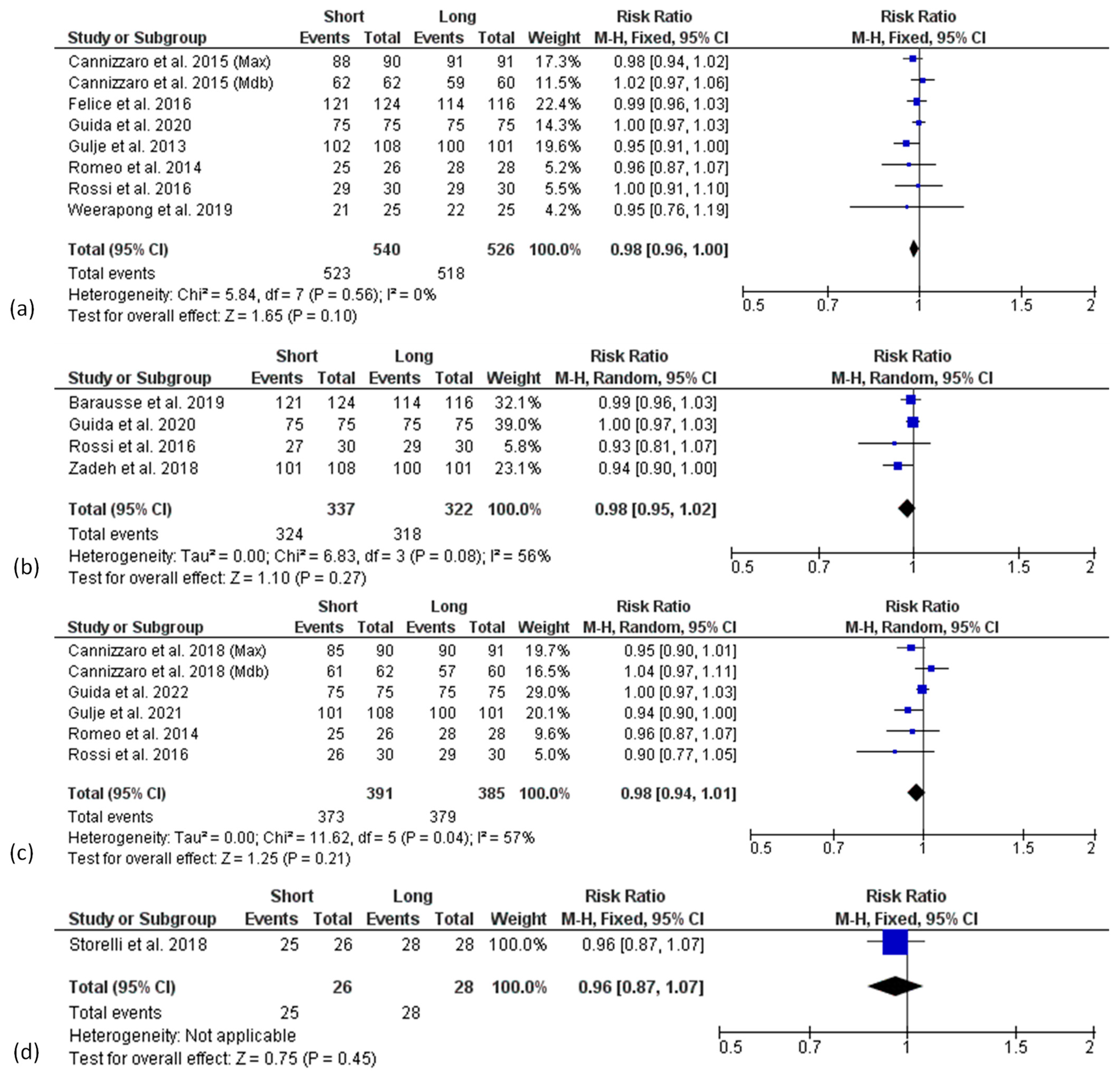
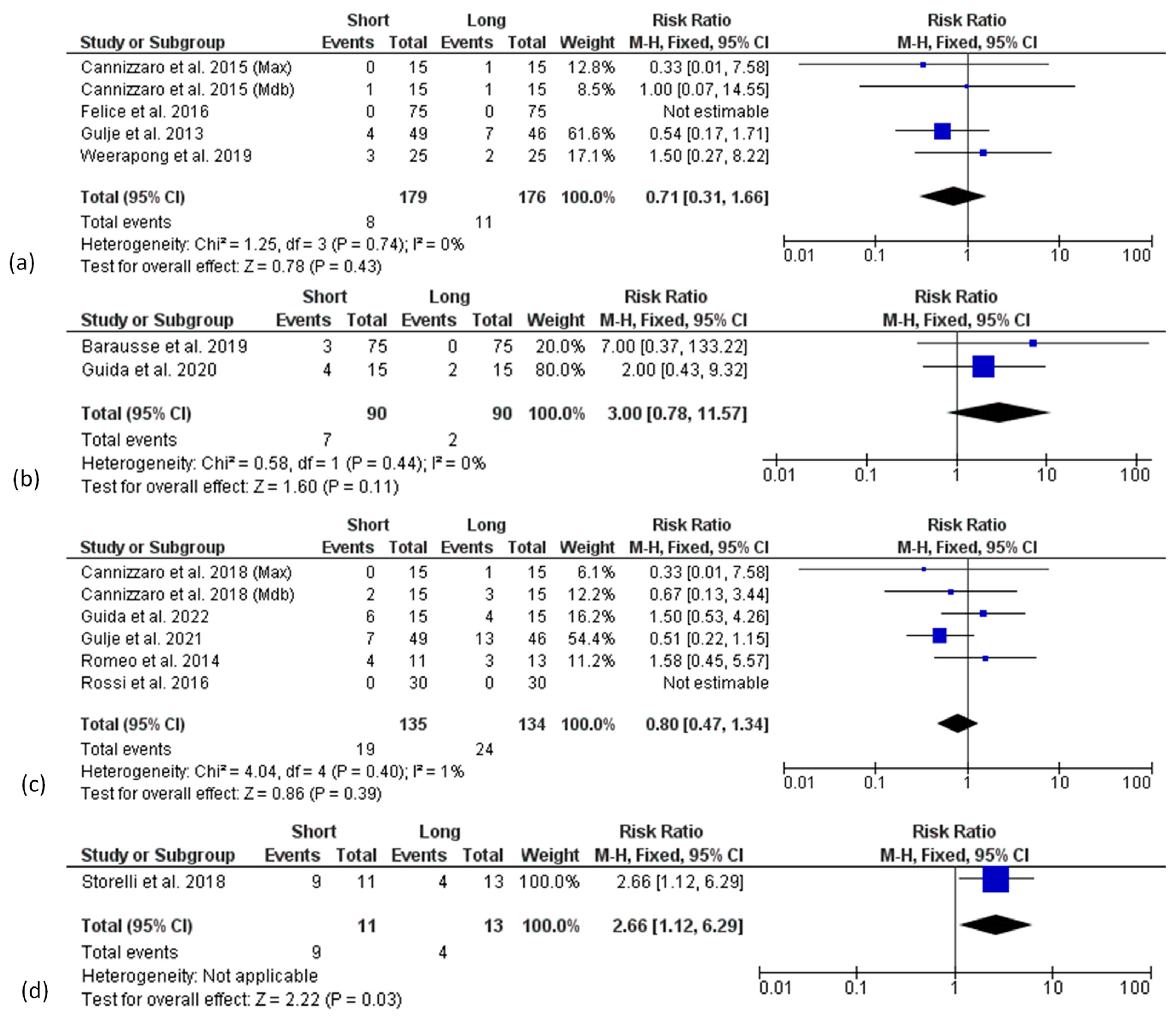
3.5.1. Survival Rate
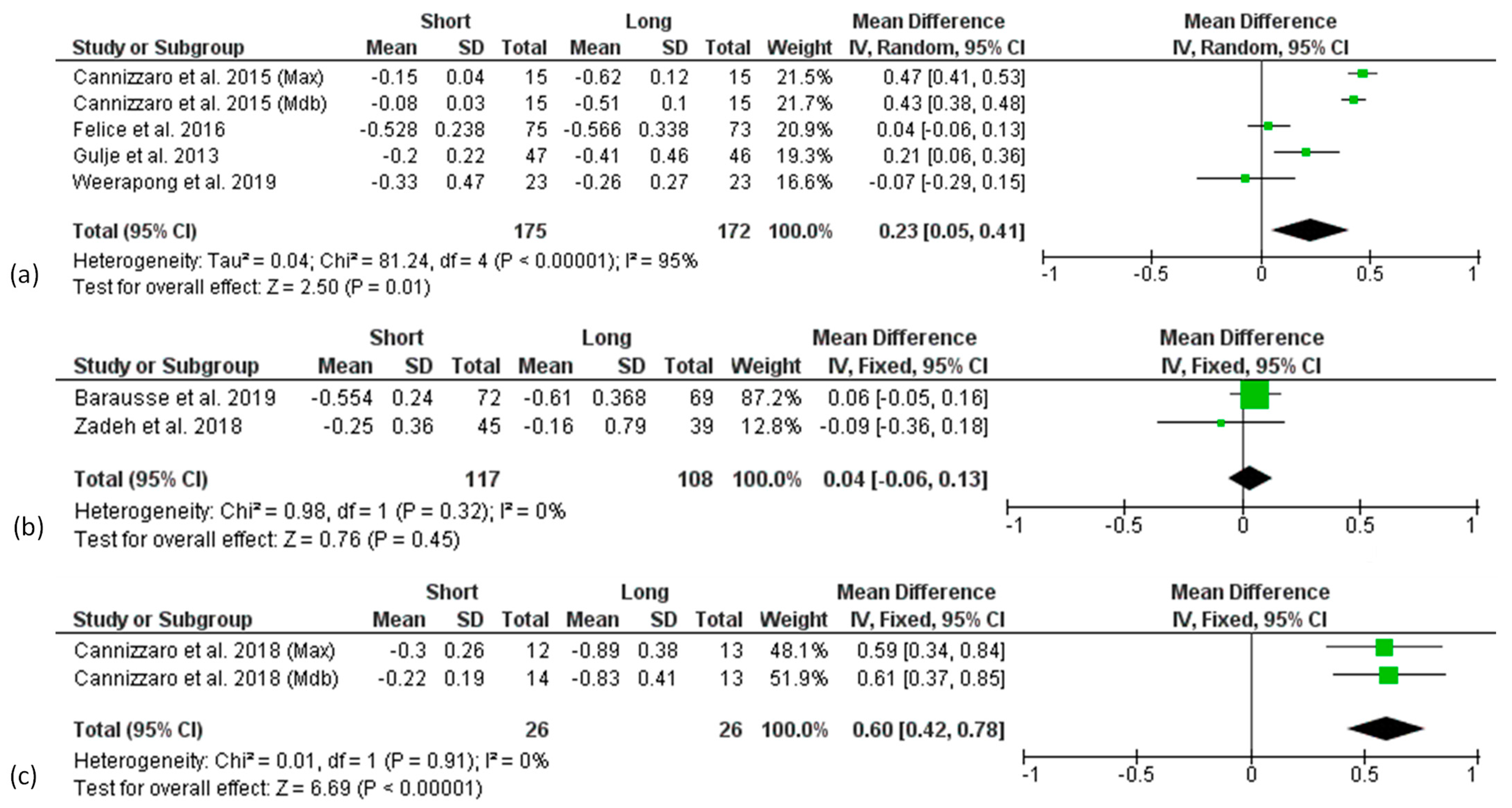
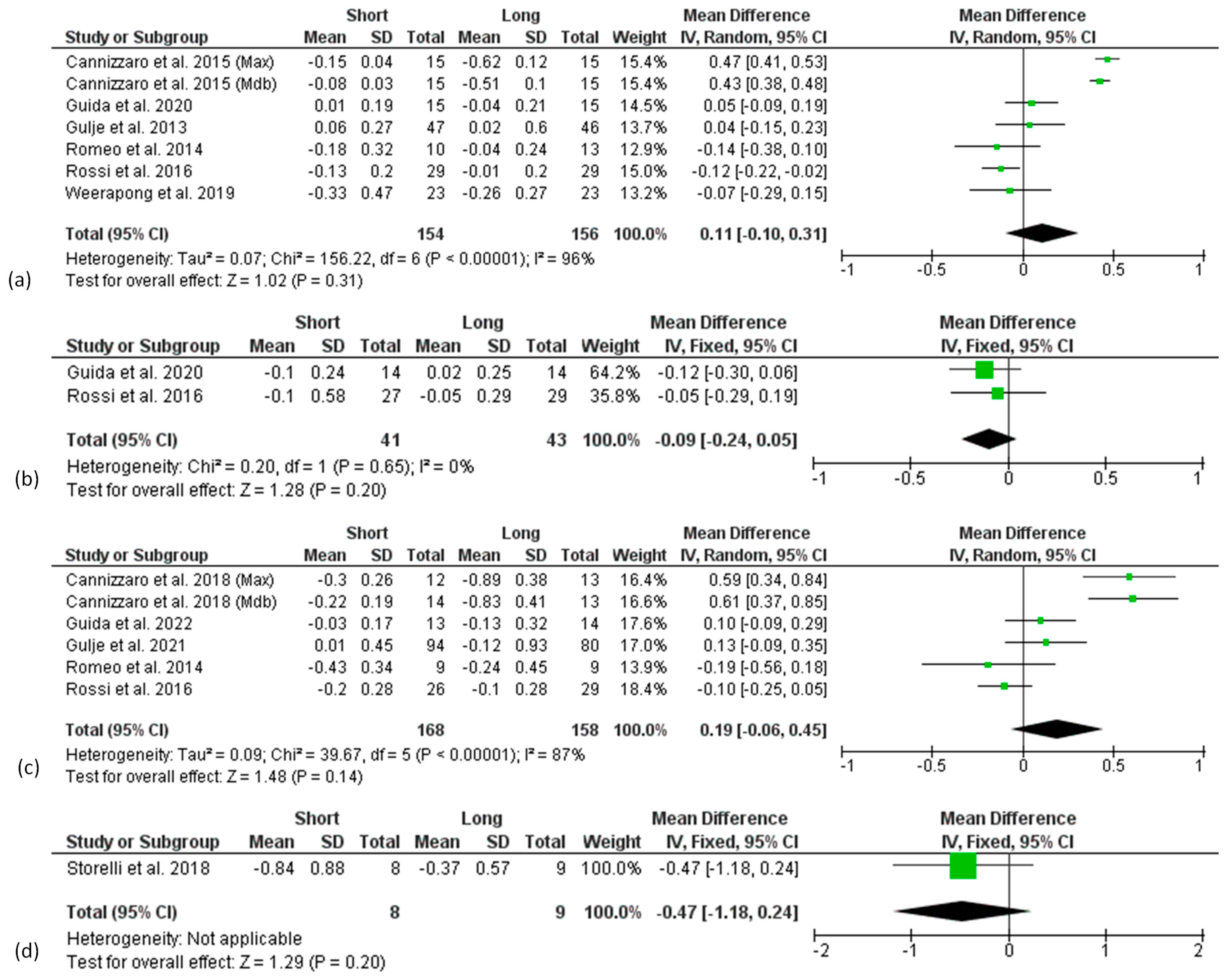
3.5.2. Peri-Implant Marginal Bone Level Change (MBLc)
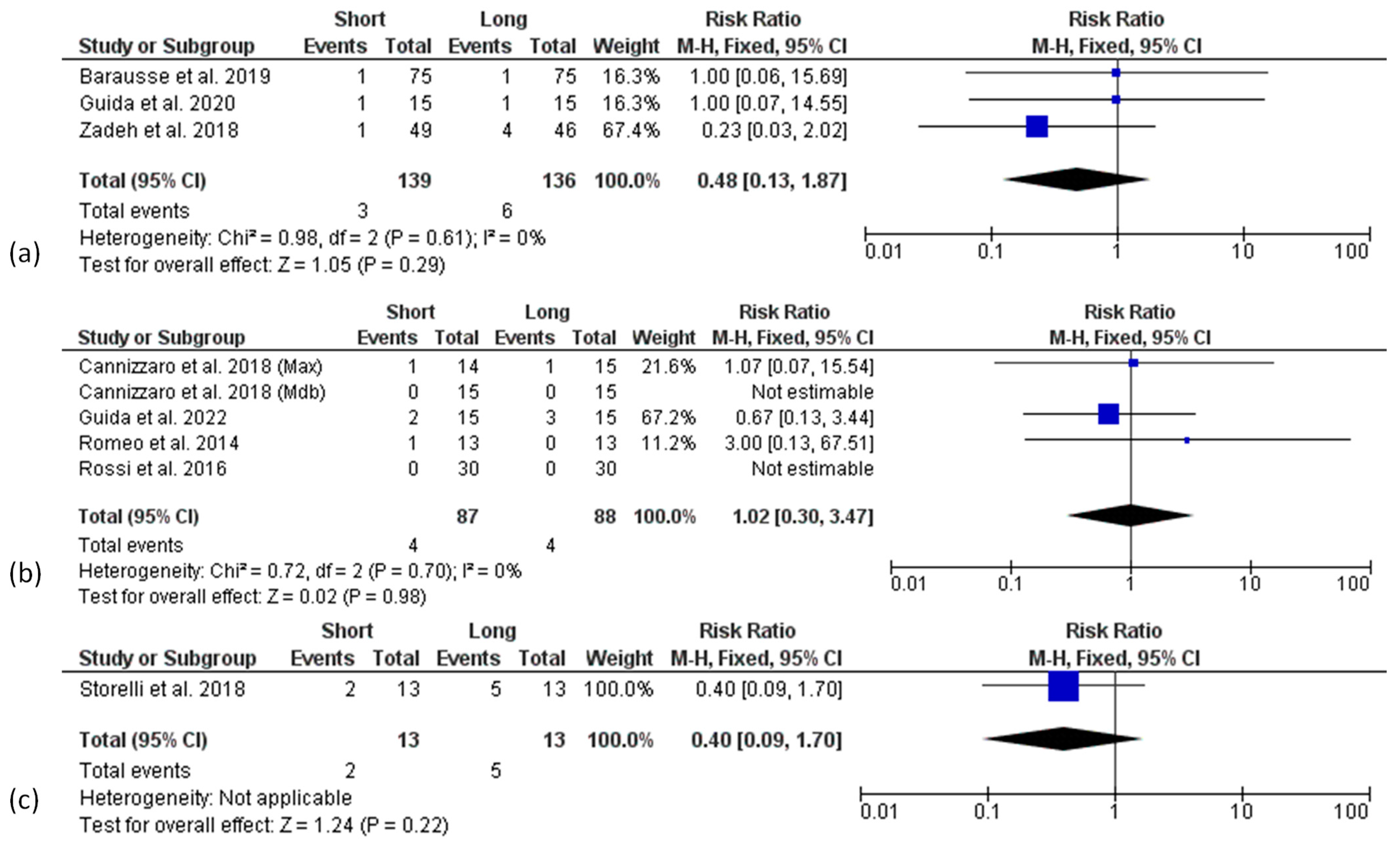
3.5.3. Biological and Technical Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Needleman, I.; Salvi, G.E.; Pjetursson, B.E. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications. Int. J. Oral Maxillofac. Implant. 2014, 29, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Rees, J.; Karasoulos, D.; Alissa, R.; Worthington, H.V.; Coulthard, P. Interventions for replacing missing teeth: Augmentation procedures of the maxillary sinus. Cochrane Database Syst. Rev. 2010, 3, CD008397. [Google Scholar]
- Fontana, F.; Maschera, E.; Rocchietta, I.; Simion, M. Clinical classification of complications in guided bone regeneration procedures by means of a nonresorbable membrane. Int. J. Periodontics Restor. Dent. 2011, 31, 265–273. [Google Scholar]
- Thoma, D.S.; Haas, R.; Tutak, M.; Garcia, A.; Schincaglia, G.P.; Hämmerle, C.H. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11–15 mm) in combination with sinus floor elevation procedures. Part 1: Demographics and patient-reported outcomes at 1 year of loading. J. Clin. Periodontol. 2015, 42, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Ravidà, A.; Wang, I.-C.; Barootchi, S.; Askar, H.; Tavelli, L.; Gargallo-Albiol, J.; Wang, H.L. Meta-analysis of randomized clinical trials comparing clinical and patient-reported outcomes between extra-short (≤6 mm) and longer (≥10 mm) implants. J. Clin. Periodontol. 2019, 46, 118–142. [Google Scholar] [CrossRef]
- Nisand, D.; Renouard, F. Short implant in limited bone volume. Periodontology 2000 2014, 66, 72–96. [Google Scholar] [CrossRef] [PubMed]
- Nisand, D.; Picard, N.; Rocchietta, I. Short implants compared to implants in vertically augmented bone: A systematic review. Clin. Oral Implant. Res. 2015, 26 (Suppl. 1), 170–179. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Donos, N.; Alcoforado, G.; Balmer, M.; Gurzawska, K.; Mardas, N.; Milinkovic, I.; Nisand, D.; Rocchietta, I.; Stavropoulos, A.; et al. Therapeutic concepts and methods for improving dental implant outcomes. Summary and consensus statements. The 4th EAO Consensus Conference 2015. Clin. Oral Implant. Res. 2015, 26 (Suppl. 1), 202–206. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI Consensus Report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implant. Res. 2018, 29, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Hingsammer, L.; Watzek, G.; Pommer, B. The influence of crown-to-implant ratio on marginal bone levels around splinted short dental implants: A radiological and clincial short term analysis. Clin. Implant Dent. Relat. Res. 2017, 19, 1090–1098. [Google Scholar] [CrossRef]
- Bahat, O. Treatment planning and placement of implants in the posterior maxillae: Report of 732 consecutive Nobelpharma implants. Int. J. Oral Maxillofac. Implant. 1993, 8, 151–161. [Google Scholar] [CrossRef][Green Version]
- Pommer, B.; Frantal, S.; Willer, J.; Posch, M.; Watzek, G.; Tepper, G. Impact of dental implant length on early failure rates: A meta-analysis of observational studies. J. Clin. Periodontol. 2011, 38, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Camps-Font, O.; Burgueño-Barris, G.; Figueiredo, R.; Jung, R.E.; Gay-Escoda, C.; Valmaseda-Castellón, E. Interventions for Dental Implant Placement in Atrophic Edentulous Mandibles: Vertical Bone Augmentation and Alternative Treatments. A Meta-Analysis of Randomized Clinical Trials. J. Periodontol. 2016, 87, 1444–1457. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonça, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Sánchez, J.-L.; García-Sala-Bonmatí, F.; Martínez-González, A.; García-Dalmau, C.; Mañes-Ferrer, J.F.; Brotons-Oliver, A. Predictability of short implants (<10 mm) as a treatment option for the rehabilitation of atrophic maxillae. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e392–e402. [Google Scholar] [PubMed]
- Thoma, D.S.; Zeltner, M.; Hüsler, J.; Hämmerle, C.H.; Jung, R.E. EAO Supplement Working Group 4—EAO CC 2015 Short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral Implant. Res. 2015, 26 (Suppl. 1), 154–169. [Google Scholar] [CrossRef]
- Tong, Q.; Zhang, X.; Yu, L. Meta-analysis of Randomized Controlled Trials Comparing Clinical Outcomes Between Short Implants and Long Implants with Bone Augmentation Procedure. Int. J. Oral Maxillofac. Implant. 2017, 32, e25–e34. [Google Scholar] [CrossRef][Green Version]
- Toti, P.; Marchionni, S.; Menchini-Fabris, G.B.; Marconcini, S.; Covani, U.; Barone, A. Surgical techniques used in the rehabilitation of partially edentulous patients with atrophic posterior mandibles: A systematic review and meta-analysis of randomized controlled clinical trials. J. Cranio-Maxillo-Fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Fac. Surg. 2017, 45, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Torres-Alemany, A.; Fernández-Estevan, L.; Agustín-Panadero, R.; Montiel-Company, J.M.; Labaig-Rueda, C.; Mañes-Ferrer, J.F. Clinical Behavior of Short Dental Implants: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3271. [Google Scholar] [CrossRef]
- Palacios, J.A.V.; Garcia, J.J.; Caramês, J.M.M.; Quirynen, M.; da Silva Marques, D.N. Short implants versus bone grafting and standard-length implants placement: A systematic review. Clin. Oral Investig. 2018, 22, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Suarez, F.; Galindo-Moreno, P.; García-Nogales, A.; Fu, J.H.; Wang, H.L. A systematic review on marginal bone loss around short dental implants (<10 mm) for implant-supported fixed prostheses. Clin. Oral Implant. Res. 2014, 25, 1119–1124. [Google Scholar]
- Yu, X.; Xu, R.; Zhang, Z.; Yang, Y.; Deng, F. A meta-analysis indicating extra-short implants (≤6 mm) as an alternative to longer implants (≥8 mm) with bone augmentation. Sci. Rep. 2021, 11, 8152. [Google Scholar] [CrossRef] [PubMed]
- Fan, T.; Li, Y.; Deng, W.-W.; Wu, T.; Zhang, W. Short Implants (5 to 8 mm) Versus Longer Implants (>8 mm) with Sinus Lifting in Atrophic Posterior Maxilla: A Meta-Analysis of RCTs. Clin. Implant Dent. Relat. Res. 2017, 19, 207–215. [Google Scholar] [CrossRef]
- Renouard, F.; Nisand, D. Impact of implant length and diameter on survival rates. Clin. Oral Implant. Res. 2006, 17 (Suppl. 2), 35–51. [Google Scholar] [CrossRef]
- Telleman, G.; Raghoebar, G.M.; Vissink, A.; den Hartog, L.; Huddleston Slater, J.J.; Meijer, H.J. A systematic review of the prognosis of short (<10 mm) dental implants placed in the partially edentulous patient. J. Clin. Periodontol. 2011, 38, 667–676. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stone, P.W. Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 2002, 15, 197–198. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, I4898. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Barausse, C.; Felice, P.; Pistilli, R.; Buti, J.; Esposito, M. Posterior jaw rehabilitation using partial prostheses supported by implants 4.0 × 4.0 mm or longer: Three-year postloading results of a multicentre randomised controlled trial. Clin. Trials Dent. 2019, 1, 25–36. [Google Scholar]
- Guida, L.; Annunziata, M.; Esposito, U.; Sirignano, M.; Torrisi, P.; Cecchinato, D. 6-mm implants for the full-arch rehabilitation of edentulous mandibles: 5-year results from a multicenter randomized controlled trial. J. Clin. Periodontol. 2022, 49. Special issue: Abstracts EuroPerio 10, accepted. [Google Scholar]
- Sahrmann, P.; Naenni, N.; Jung, R.E.; Held, U.; Truninger, T.; Hämmerle, C.H.; Attin, T.; Schmidlin, P.R. Success of 6-mm Implants with Single-Tooth Restorations: A 3-year Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 623–628. [Google Scholar] [CrossRef]
- Naenni, N.; Sahrmann, P.; Schmidlin, P.R.; Attin, T.; Wiedemeier, D.B.; Sapata, V.; Hämmerle, C.H.F.; Jung, R.E. Five-Year Survival of Short Single-Tooth Implants (6 mm): A Randomized Controlled Clinical Trial. J. Dent. Res. 2018, 97, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, P.; Schoen, P.; Naenni, N.; Jung, R.; Attin, T.; Schmidlin, P.R. Peri-implant bone density around implants of different lengths: A 3-year follow-up of a randomized clinical trial. J. Clin. Periodontol. 2017, 44, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Sluka, B.; Naenni, N.; Jung, R.E.; Attin, T.; Schmidlin, P.R.; Sahrmann, P. Changes of radiopacity around implants of different lengths: Five-year follow-up data of a randomized clinical trial. Clin. Oral Implant. Res. 2020, 31, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Della Vecchia, M.P.; Leles, C.R.; Cunha, T.R.; Ribeiro, A.B.; Sorgini, D.B.; Muglia, V.A.; Reis, A.C.; Albuquerque, R.F., Jr.; de Souza, R.F. Mini-Implants for Mandibular Overdentures: Cost-Effectiveness Analysis alongside a Randomized Trial. JDR Clin. Transl. Res. 2018, 3, 47–56. [Google Scholar] [CrossRef]
- Esposito, M.; Barausse, C.; Pistilli, R.; Checchi, V.; Diazzi, M.; Gatto, M.R.; Felice, P. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: Four-month post-loading data from a randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 221–230. [Google Scholar]
- Al-Hashedi, A.A.; Taiyeb-Ali, T.B.; Yunus, N. Outcomes of placing short implants in the posterior mandible: A preliminary randomized controlled trial. Aust. Dent. J. 2016, 61, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, G.; Felice, P.; Buti, J.; Leone, M.; Ferri, V.; Esposito, M. Immediate loading of fixed cross-arch prostheses supported by flapless-placed supershort or long implants: 1-year results from a randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 27–36. [Google Scholar] [PubMed]
- Cannizzaro, G.; Felice, P.; Ippolito, D.R.; Velasco-Ortega, E.; Esposito, M. Immediate loading of fixed cross-arch prostheses supported by flapless-placed 5 mm or 11.5 mm long implants: 5-year results from a randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 295–306. [Google Scholar]
- Rossi, F.; Botticelli, D.; Cesaretti, G.; De Santis, E.; Storelli, S.; Lang, N.P. Use of short implants (6 mm) in a single-tooth replacement: A 5-year follow-up prospective randomized controlled multicenter clinical study. Clin. Oral Implant. Res. 2016, 27, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Romeo, E.; Storelli, S.; Casano, G.; Scanferla, M.; Botticelli, D. Six-mm versus 10-mm long implants in the rehabilitation of posterior edentulous jaws: A 5-year follow-up of a randomised controlled trial. Eur. J. Oral Implantol. 2014, 7, 371–381. [Google Scholar]
- Guljé, F.; Abrahamsson, I.; Chen, S.; Stanford, C.; Zadeh, H.; Palmer, R. Implants of 6 mm vs. 11 mm lengths in the posterior maxilla and mandible: A 1-year multicenter randomized controlled trial. Clin. Oral Implant. Res. 2013, 24, 1325–1331. [Google Scholar] [CrossRef] [PubMed]
- Guljé, F.L.; Meijer, H.J.A.; Abrahamsson, I.; Barwacz, C.A.; Chen, S.; Palmer, P.J.; Zadeh, H.; Stanford, C.M. Comparison of 6-mm and 11-mm dental implants in the posterior region supporting fixed dental prostheses: 5-year results of an open multicenter randomized controlled trial. Clin. Oral Implant. Res. 2021, 32, 15–22. [Google Scholar] [CrossRef]
- Guida, L.; Annunziata, M.; Esposito, U.; Sirignano, M.; Torrisi, P.; Cecchinato, D. 6-mm-short and 11-mm-long implants compared in the full-arch rehabilitation of the edentulous mandible: A 3-year multicenter randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 64–73. [Google Scholar] [CrossRef]
- Weerapong, K.; Sirimongkolwattana, S.; Sastraruji, T.; Khongkhunthian, P. Comparative Study of Immediate Loading on Short Dental Implants and Conventional Dental Implants in the Posterior Mandible: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 141–149. [Google Scholar] [CrossRef]
- Felice, P.; Checchi, L.; Barausse, C.; Pistilli, R.; Sammartino, G.; Masi, I.; Ippolito, D.R.; Esposito, M. Posterior jaws rehabilitated with partial prostheses supported by 4.0 × 4.0 mm or by longer implants: One-year post-loading results from a multicenter randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 35–45. [Google Scholar]
- Zadeh, H.H.; Guljé, F.; Palmer, P.J.; Abrahamsson, I.; Chen, S.; Mahallati, R.; Stanford, C.M. Marginal bone level and survival of short and standard-length implants after 3 years: An Open Multi-Center Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2018, 29, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Storelli, S.; Abbà, A.; Scanferla, M.; Botticelli, D.; Romeo, E. 6 mm vs. 10 mm-long implants in the rehabilitation of posterior jaws: A 10-year follow-up of a randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 283–292. [Google Scholar]
- Weber, H.-P.; Morton, D.; Gallucci, G.O.; Roccuzzo, M.; Cordaro, L.; Grutter, L. Consensus statements and recommended clinical procedures regarding loading protocols. Int. J. Oral Maxillofac. Implant. 2009, 24, 180–183. [Google Scholar]
- Chen, S.T.; Beagle, J.; Jensen, S.S.; Chiapasco, M.; Darby, I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int. J. Oral Maxillofac. Implant. 2009, 24, 272–278. [Google Scholar]
- Friberg, B.; Jemt, T.; Lekholm, U. Early failures in 4641 consecutively placed Brånemark dental implants: A study from stage 1 surgery to the connection of completed prostheses. Int. J. Oral Maxillofac. Implant. 1991, 6, 142–146. [Google Scholar]
- Aljateeli, M.; Wang, H.-L. Implant microdesigns and their impact on osseointegration. Implant Dent. 2013, 22, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, M.; Guida, L. The Effect of Titanium Surface Modifications on Dental Implant Osseointegration. Front. Oral Biol. 2015, 17, 62–77. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search String |
|---|---|
| PubMed (MEDLINE) | (“dental implants” [MeSH Terms] OR “dental implantation” [MeSH Terms]) AND (short OR shorter OR long OR longer OR length) AND (randomized controlled trials) |
| Clinicaltrials.gov | Condition or disease: dental implants OR dental implantation Other terms: short OR shorter OR long OR longer OR length |
| Embase | (‘dental implants’/exp OR ‘dental implants’ OR ‘dental implantation’/exp OR ‘dental implantation’) AND (short OR shorter OR long OR longer OR ‘length’/exp OR length) AND randomized AND controlled AND trial |
| Scopus | (‘dental AND implants’/exp OR ‘dental AND implants’ OR ‘dental AND implantation’/exp OR ‘dental AND implantation’) AND (short OR shorter OR long OR longer OR ‘length’/exp OR length) AND (randomized AND controlled AND trial) |
| Open grey (assimilated by Dans Easy) | (“dental implants” OR “dental implantation”) AND (short OR shorter OR long OR longer OR length) AND (randomized controlled trials) |
| Study | Reason for Exclusion |
|---|---|
| Sahrmann et al., 2016 [36] | Sinus floor elevation with Summer’s technique allowed (reason 1) |
| Naenni et al., 2018 [37] | Sinus floor elevation with Summer’s technique allowed (reason 1) |
| Sahrmann et al., 2017 [38] | Only rx bone density analysis (reason 2) |
| Sluka et al., 2020 [39] | Only rx bone radiopacity analysis (reason 2) |
| Della Vecchia et al., 2018 [40] | Mini implants for overdentures (reason 3) |
| Esposito et al., 2015 [41] | Follow up <12 months (reason 4) |
| Al-Hashedi et al., 2016 [42] | <8.5 mm implants in the control group (reason 5) |
| Study/Studies | Study Design | Follow Up (Years) | Max, Mdb | Test Implant Length | Control Implant Length | Patients 1/Implants | Age (Mean) Age (Range) Gender (M/F) | Implant Surface (Name, Company) | Implant Location | Prosthetic Rehabilitation | Prosthetic Loading | Post-Extraction Implants Included | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Test | Control | Test | Control | |||||||||||
| Gulje et al., 2013 [47], Zadeh et al., 2018 [52]; Gulje et al., 2021 [48] | RCT, parallel group | 1, 3, 5 | Max + Mdb pooled | 6 mm | 11 mm | 49/108 | 46/101 | 54.8 26–69 21/28 | 54.1 34–70 27/19 | Blasted fluoride-modified (OsseoSpeed, Astra Tech Implant System, Dentsply Sirona) | Premolar and molar | 2–3 unit splinted crowns (screw-retained) | Early (6 w) | No |
| Romeo et al., 2014 [46]; Storelli et al., 2018 [53] | RCT, parallel group | 5, 10 | Max + Mdb pooled | 6 mm | 10 mm | 11/26 | 13/28 | 50 37–75 6/5 | 56 32–75 6/7 | Sand blasted large grit acid etched (SLA, Straumann) | Premolar and molar | 2–3 unit splinted crowns (cemented) | Early (8 w) | No |
| Cannizzaro et al., 2015 [43]; 2018 [44] | RCT, parallel group | 1, 5 | Max, Mdb | 5 mm | 11.5 mm | Max 15/91 Mdb 15/60 | Max 15/90 Mdb 15/62 | Max 58.9 44–78 7/8 Mdb 62.9 47–80 8/7 | Max 58.5 43–72 9/6 Mdb 58.8 38–72 7/8 | Dual acid-etched (NanoTite, Biomet 3I) | Anterior and posterior | FA prostheses with distal cantilever (screw-retained) | Immediate (<1 w) | Yes |
| Rossi et al., 2016 [45] | RCT, mixed 2 | 5 | Max + Mdb pooled | 6 mm | 10 mm | NC/30 | NC/30 | 48.8 NR 16/14 | 47.7 NR 16/14 | Sand blasted large grit acid etched (SLA, Straumann) | Premolar and molar | SCs (retention NC) | Early (7 w) | No |
| Felice et al., 2016 [51]; Barausse et al., 2019 [34] | RCT, parallel group | 1, 3 | Max + Mdb pooled | 4 mm | ≥8.5 mm | 75/124 | 75/116 | 53.7 27–76 30/45 | 55.5 25–86 36/39 | Sand-blasted acid-etched (SA2, TwinKon, Global D) | Premolar and molar | SCs and 2–3 unit splinted crowns (screw retained) | Conventional (4 m) | Yes |
| Weerapong et al., 2019 [50] | RCT, parallel group | 1 | Mdb | 6 mm | 10 mm | 25/25 | 25/25 | 50.5 20–61 9/14 | 51.4 22–64 7/16 | NR (PW+ Dental Implant System) | Molar | SCs (cemented) | Immediate (<1 w) | Yes |
| Guida et al., 2020 [49]; Guida et al., 2022 [35] | RCT, parallel group | 1, 3, 5 | Mdb | 6 mm | 11 mm | 15/75 | 15/75 | 63 NR 5/10 | 61 NR 12/3 | Blasted fluoride-modified (OsseoSpeed, Astra Tech Implant System, Dentsply Sirona) | Interforaminal | FA prostheses with distal cantilever (screw-retained) | Conventional (3 m) | No |
| Certainty Assessment | № of Implants | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Short Implants | Long Implants | Relative (95% CI) | Absolute (95% CI) | ||
| Survival Rate (Implant Level) (Follow-Up: Range 1 to 10 Years) | ||||||||||||
| 8 | Randomised trials | Not serious | Not serious | Not serious | Serious a | None | 518/540 (95.9%) | 515/526 (97.9%) | RR 0.98 (0.96 to 1.00) | 20 fewer per 1.000 (from 39 fewer to 0 fewer) | ⊕⊕⊕◯ Moderate | CRITICAL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guida, L.; Bressan, E.; Cecoro, G.; Volpe, A.D.; Del Fabbro, M.; Annunziata, M. Short versus Longer Implants in Sites without the Need for Bone Augmentation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Materials 2022, 15, 3138. https://doi.org/10.3390/ma15093138
Guida L, Bressan E, Cecoro G, Volpe AD, Del Fabbro M, Annunziata M. Short versus Longer Implants in Sites without the Need for Bone Augmentation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Materials. 2022; 15(9):3138. https://doi.org/10.3390/ma15093138
Chicago/Turabian StyleGuida, Luigi, Eriberto Bressan, Gennaro Cecoro, Armando Davide Volpe, Massimo Del Fabbro, and Marco Annunziata. 2022. "Short versus Longer Implants in Sites without the Need for Bone Augmentation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Materials 15, no. 9: 3138. https://doi.org/10.3390/ma15093138
APA StyleGuida, L., Bressan, E., Cecoro, G., Volpe, A. D., Del Fabbro, M., & Annunziata, M. (2022). Short versus Longer Implants in Sites without the Need for Bone Augmentation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Materials, 15(9), 3138. https://doi.org/10.3390/ma15093138