
Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study

 ,
,  ,
,  ,
,  ,
,  , , ,
, , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
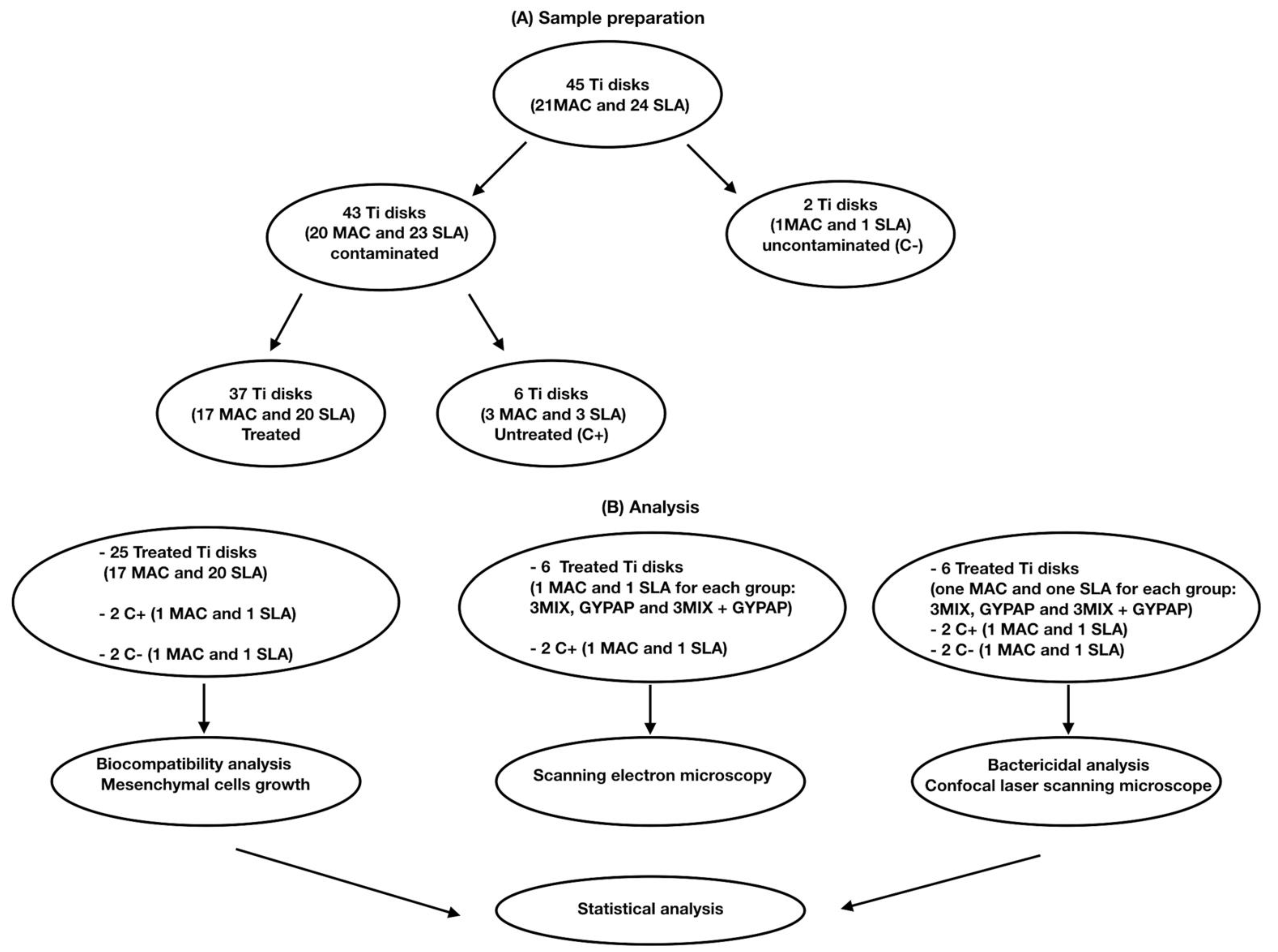
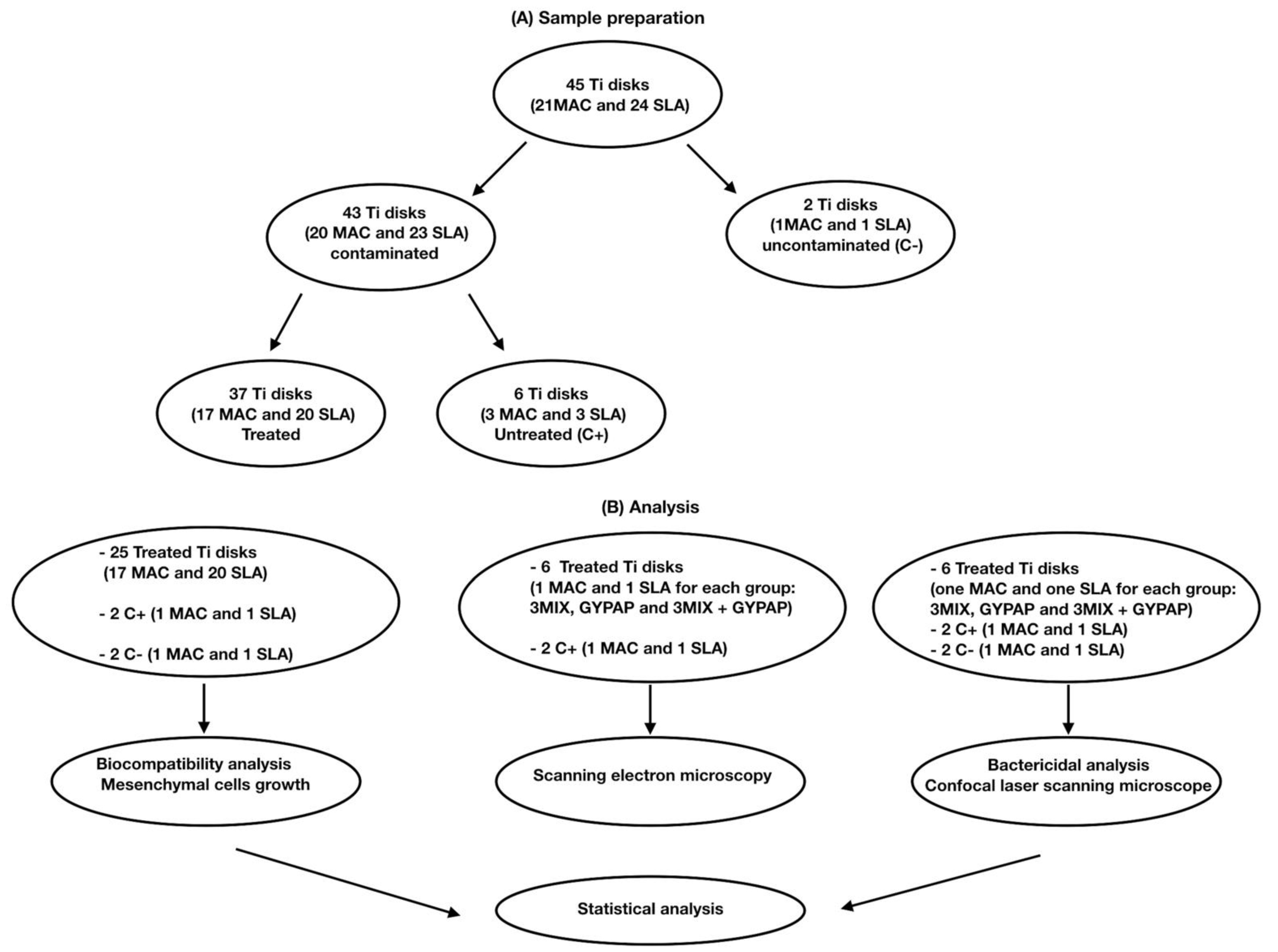
2. Materials and Methods
2.1. Saliva Collection
2.2. Biofilm Formation on Disks
2.3. Treatment Procedures
- The application of an antibiotic gel mixture with ciprofloxacin, metronidazole, and clarithromycin (3MIX) for 1 h.
- Glycine powder air polishing (GYPAP) for 1 min (AirFlow Prophylaxis Master, EMS Dental) set at medium intensity.
- The combination of the two previous procedures (3MIX + GYPAP), first the application of the antibiotic gel mixture and after glycine powder air polishing.
2.4. Mesenchymal Cells Growth on Treated Disks
2.5. Influence of Decontamination on ASCs’ Adhesion
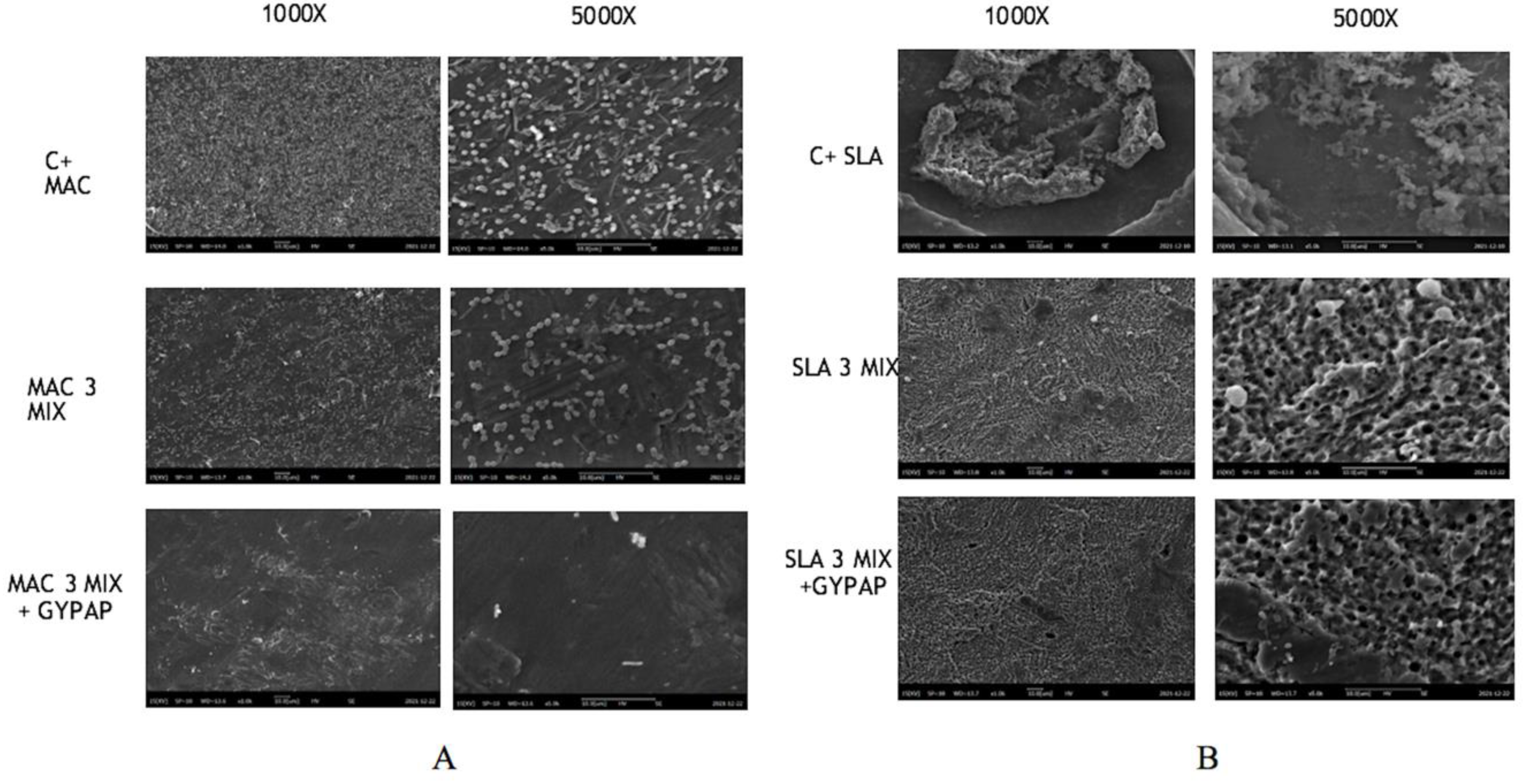
2.6. Scanning Electron Microscopy
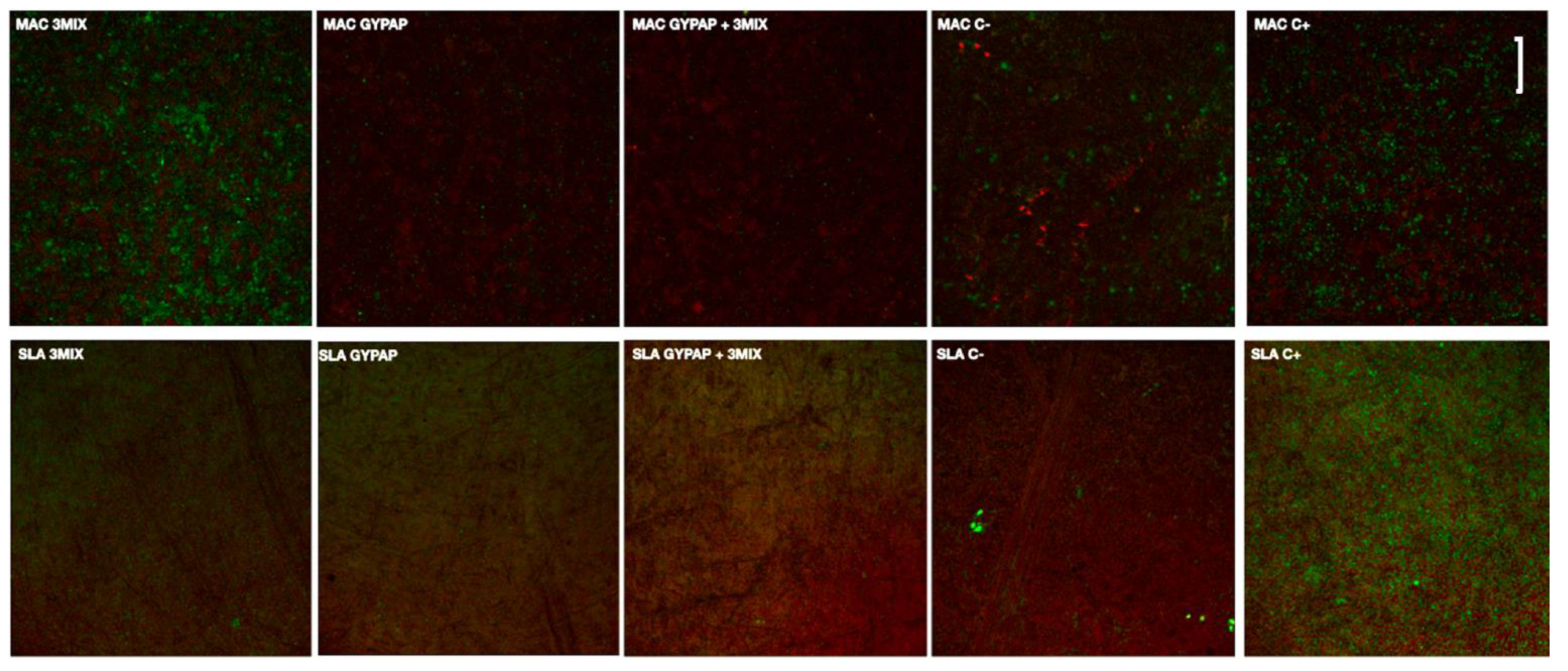
2.7. Confocal Laser Scanning Microscope (CLSM) Analysis
2.8. Statistical Analysis
3. Results
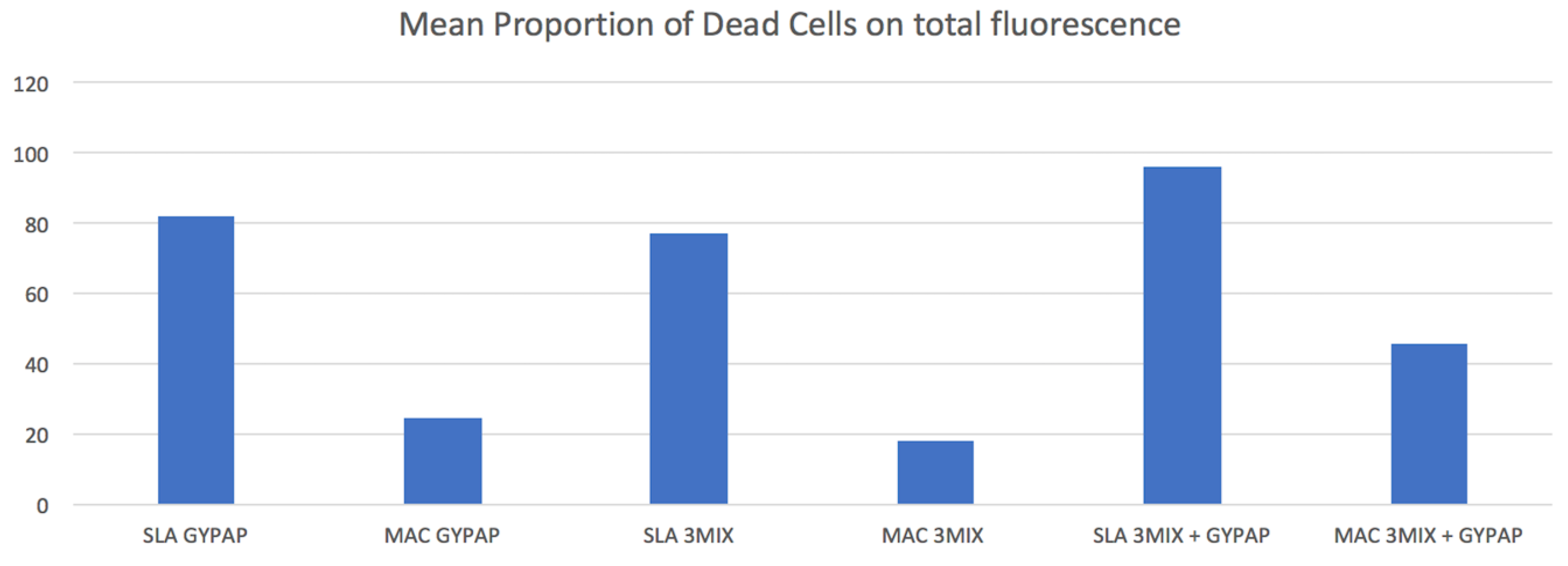
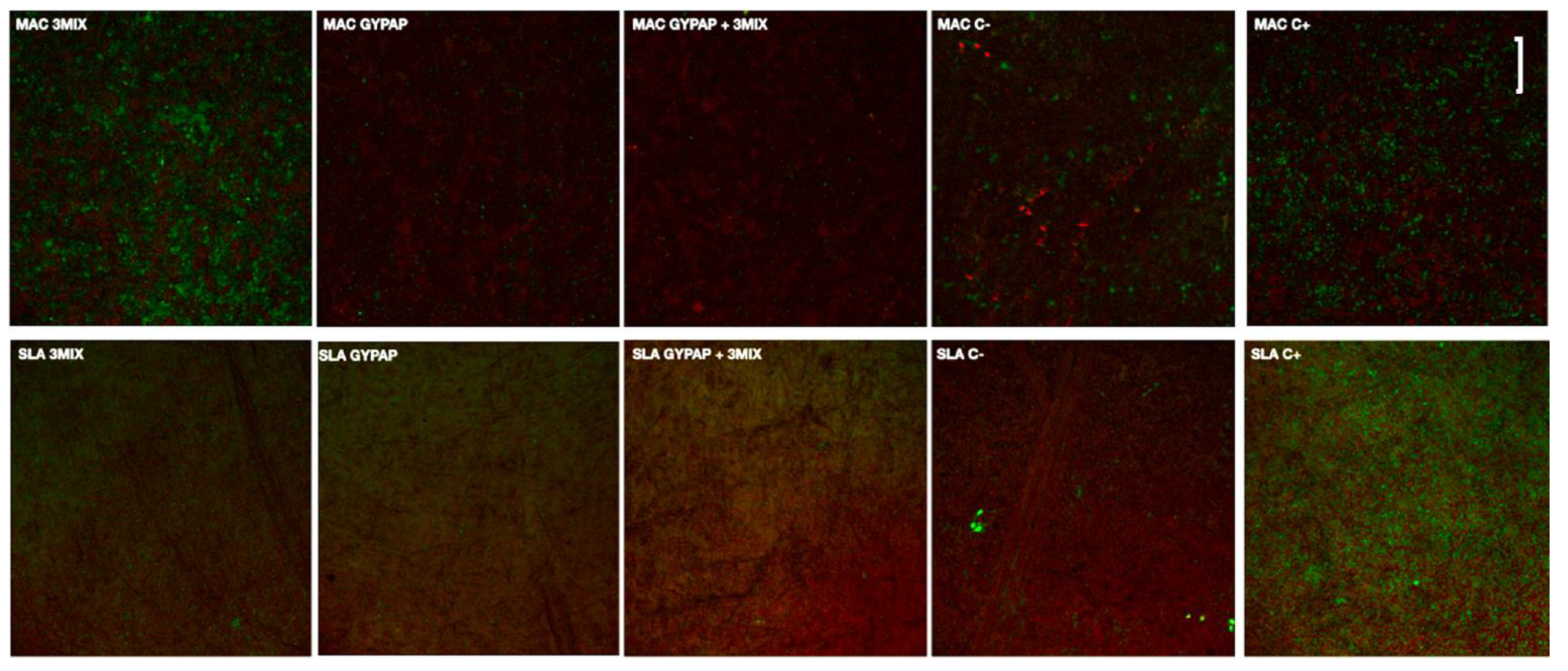
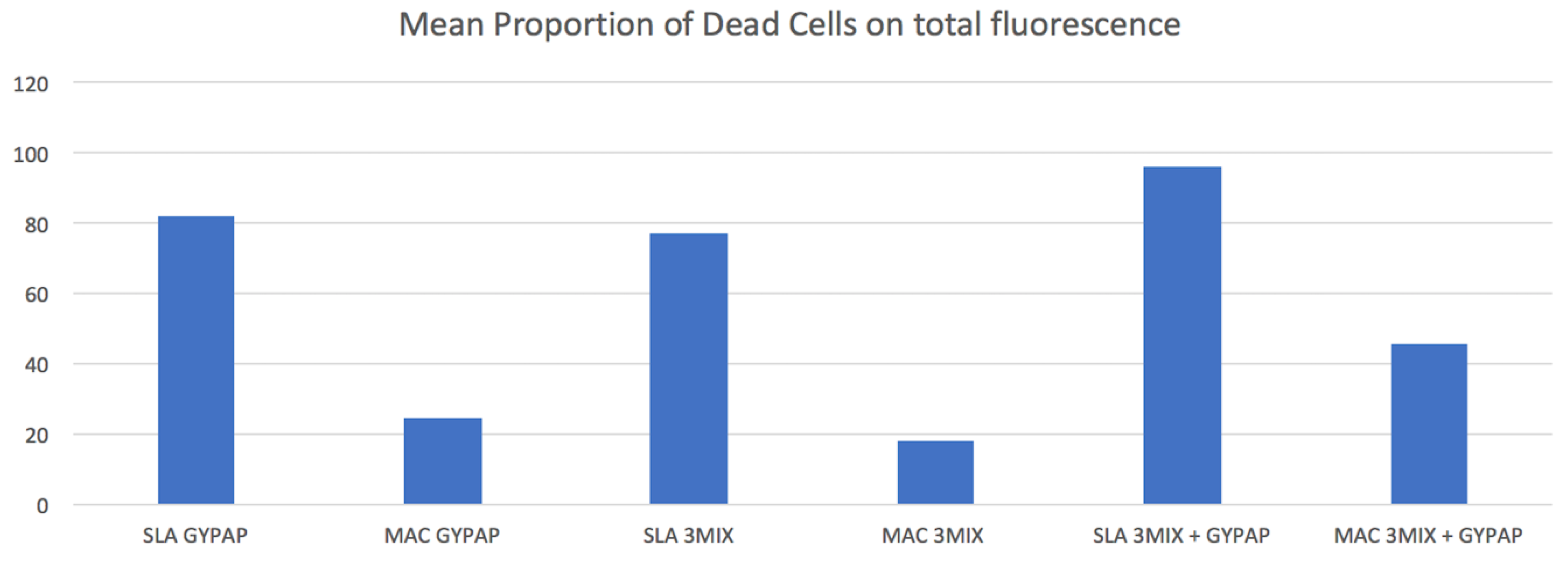
3.1. Effect of Different Decontamination Protocols on Bacterial Viability
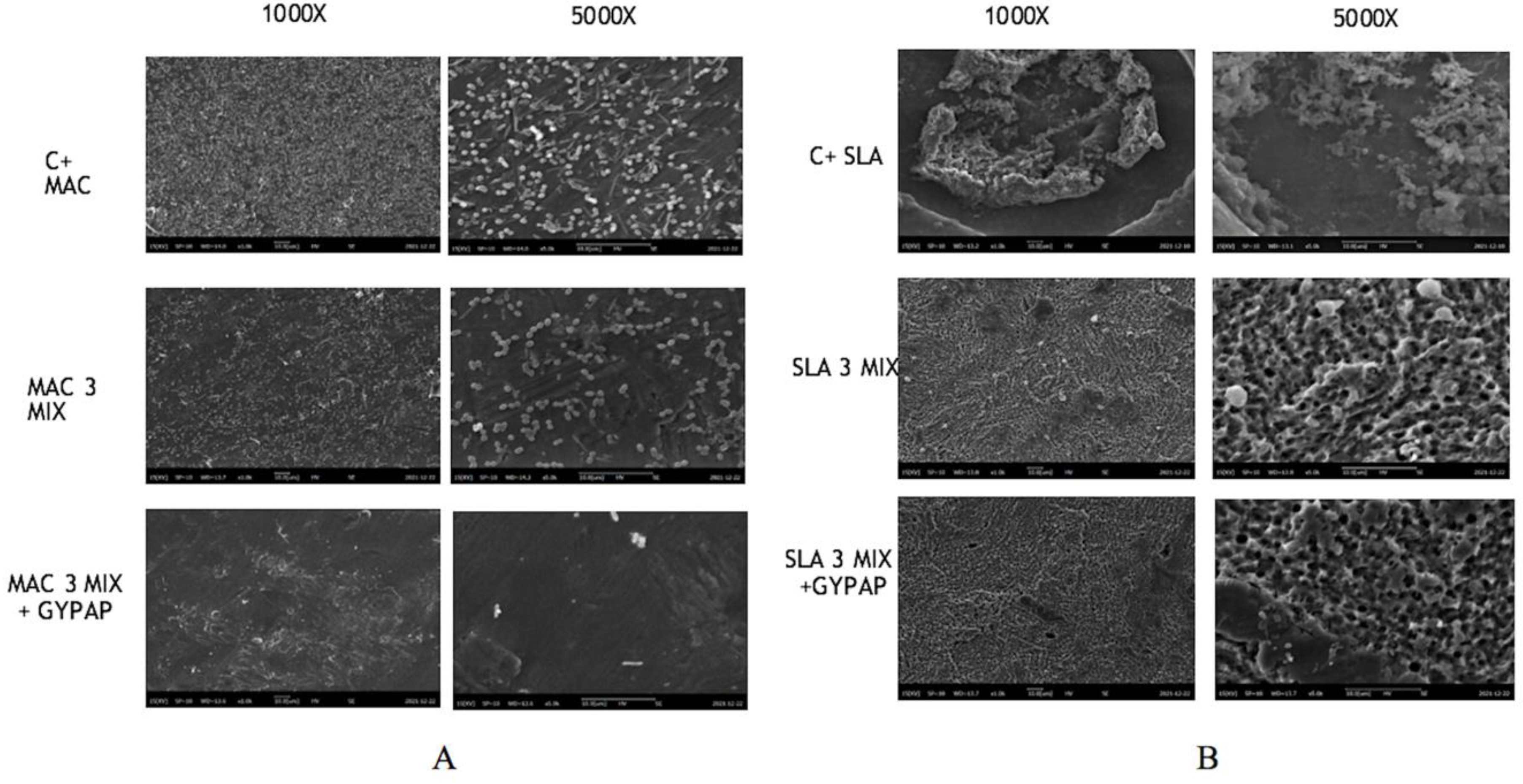
3.2. SEM Analysis
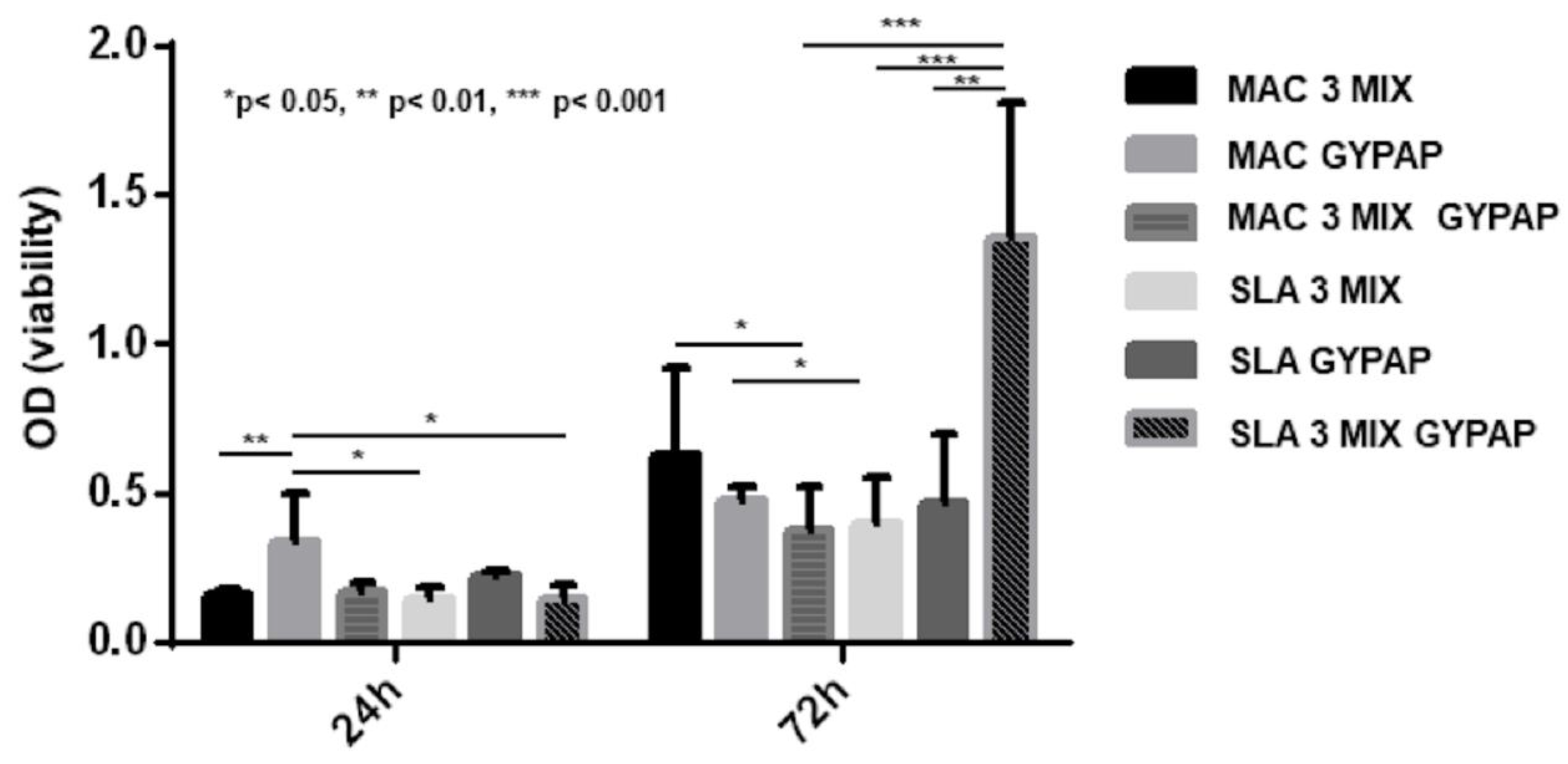
3.3. Effects of Different Decontamination Protocols on ASC Growth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implants. Res. 2012, 23, 2–21. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I) Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Troiano, G.; Lo Russo, L.; Canullo, L.; Ciavarella, D.; Lo Muzio, L.; Laino, L. Early and late implant failure of submerged versus non-submerged implant healing: A systematic review, meta-analysis and trial sequential analysis. J. Clin. Periodontol. 2018, 45, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Salcetti, J.M.; Moriarty, J.D.; Cooper, L.F.; Smith, F.W.; Collins, J.G.; Socransky, S.S.; Offenbacher, S. The clinical, microbial, and host response characteristics of the failing implant. Int. J. Oral Maxillofac. Implants 1997, 12, 32–42. [Google Scholar]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Periodontol. 2018, 89, S304–S312. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Tealdo, T.; Bevilacqua, M.; Pera, F.; Pera, P. Peri-implantitis: A systematic review of recently published papers. Int. J. Prosthodont. 2014, 27, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Isidor, F. Consensus report: Implant therapy. In Proceedings of the 1st European Workshop on Periodontology; Lang, N.P., Karring, T., Eds.; Quintessence: Berlin, Germany, 1994; pp. 365–369. [Google Scholar]
- Mombelli, A.; Lang, N.P. The diagnosis and treatment of peri-implantitis. Periodontol. 2000 1998, 17, 63–76. [Google Scholar] [CrossRef]
- Canullo, L.; Signorini, L.; Pistilli, R.; Patini, R.; Pistilli, V.; Pesce, P. A prospective case series on surgical treatment of circumferential and semi-circumferential defects due to peri-implantitis. Braz. Oral. Res. 2019, 33, 72. [Google Scholar] [CrossRef] [Green Version]
- Mir-Mari, J.; Mir-Orfila, P.; Figueiredo, R.; Valmaseda-Castellon, E.; Gay-Escoda, C. Prevalence of peri-implant diseases. A cross-sectional study based on a private practice environment. J. Clin. Periodontol. 2012, 39, 490–494. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.; Faggion, C.M.; Duncan, W.J. The frequency of peri-implant diseases: A systematic review and meta-analysis. J. Periodontol. 2013, 84, 1586–1598. [Google Scholar] [CrossRef] [Green Version]
- Subramani, K.; Wismeijer, D. Decontamination of titanium implant surface and re-osseointegration to treat peri-implantitis: A literature review. Int. J. Oral Maxillofac. Implants 2012, 27, 1043–1054. [Google Scholar] [PubMed]
- Mussano, F.; Rovasio, S.; Schierano, G.; Baldi, I.; Carossa, S. The effect of glycine-powder airflow and hand instrumentation on peri-implant soft tissues: A split-mouth pilot study. Int. J. Prosthodont. 2013, 26, 42–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsakis, G.A.; Olmedo, D.G. Peri-implantitis is not periodontitis: Scientific discoveries shed light on microbiome- biomaterial interactions that may determine disease phenotype. Periodontol. 2000 2021, 86, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Gupta, B.; Yunker, M.; Romanos, E.B.; Malmstrom, H. Lasers use in dental implantology. Implant Dent. 2013, 22, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Mellado-Valero, A.; Buitrago-Vera, P.; Sola-Ruiz, M.F.; Ferrer-Garcia, J.C. Decontamination of dental implant surface in peri-implantitis treatment: A literature review. Med. Oral. Patol. Oral. Cir. Bucal. 2013, 18, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Charalampakis, G.; Rabe, P.; Leonhardt, A.; Dahlen, G. A follow-up study of peri-implantitis cases after treatment. J. Clin. Periodontol. 2011, 38, 864–871. [Google Scholar] [CrossRef]
- Persson, L.G.; Ericsson, I.; Berglundh, T.; Lindhe, J. Osseointegration following treatment of peri-implantitis and replacement of implant components. An experimental study in the dog. J. Clin. Periodontol. 2001, 28, 258–263. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Shibli, J.A.; Borges, A.L.S.; Tango, R.N. Influence of implantoplasty on stress distribution of exposed implants at different bone insertion levels. Braz. Oral. Res. 2017, 31, 96. [Google Scholar] [CrossRef] [Green Version]
- Dhaliwal, S.K.S.; Knights, J.; Albuquerque, R.F. Microbial Biofilm Decontamination on Dental Implant Surfaces: A Mini Review. Front. Cell. Infect. Microbiol. 2021, 11, 736186. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Tribst, J.P.M. Dental Materials Coatings: Effect on the Clinical Behavior. Coatings 2020, 10, 1229. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implants Res. 2009, 20, 172–184. [Google Scholar] [CrossRef]
- Mussano, F.; Genova, T.; Serra, F.G.; Carossa, M.; Munaron, L.; Carossa, S. Nano-Pore Size of Alumina Affects Osteoblastic Response. Int. J. Mol. Sci. 2018, 19, 528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayoub, H.M.; Gregory, R.L.; Tang, Q.; Lippert, F. Influence of salivary conditioning and sucrose concentration on biofilm-mediated enamel demineralization. J. Appl. Oral. Sci. 2020, 28, 20190501. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, A.; Olsson, J.; Dahlén, G. Bacterial colonization on titanium, hydroxyapatite, and amalgam surfaces in vivo. J. Dent. Res. 1995, 74, 1607–1612. [Google Scholar] [CrossRef]
- Thurnheer, T.; Belibasakis, N. Incorporation of staphylococci into titanium-grown biofilms: An in vitro “submucosal” biofilm model for peri-implantitis. Clin. Oral. Implants Res. 2016, 27, 890–895. [Google Scholar] [CrossRef] [Green Version]
- Roehling, S.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Braissant, O.; Woelfler, H.; Waltimo, T.; Kniha, H.; Gahlert, M.J. In Vitro Biofilm Formation on Titanium and Zirconia Implant Surfaces. J. Periodontol. 2017, 88, 298–307. [Google Scholar] [CrossRef]
- Canullo, L.; Genova, T.; Wang, H.L.; Carossa, S.; Mussano, F. Plasma of Argon Increases Cell Attachment and Bacterial Decontamination on Different Implant Surfaces. Int. J. Oral Maxillofac. Implants. 2017, 32, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- Canullo, L.; Genova, T.; Tallarico, M.; Gautier, G.; Mussano, F.; Botticelli, D. Plasma of Argon Affects the Earliest Biological Response of Different Implant Surfaces: An In Vitro Comparative Study. J. Dent. Res. 2016, 95, 566. [Google Scholar] [CrossRef]
- Mandras, N.; Alovisi, M.; Roana, J.; Crosasso, P.; Luganini, A.; Pasqualini, D.; Genta, E.; Arpicco, S.; Banche, G.; Cuffini, A.; et al. Evaluation of the Bactericidal Activity of a Hyaluronic Acid-Vehicled Clarithromycin Antibiotic Mixture by Confocal Laser Scanning Microscopy. Appl. Sci. 2020, 10, 761. [Google Scholar] [CrossRef]
- Mussano, F.; Genova, T.; Corsalini, M.; Schierano, G.; Pettini, F.; Di Venere, D.; Carossa, S. Cytokine, Chemokine, and Growth Factor Profile Characterization of Undifferentiated and Osteoinduced Human Adipose-Derived Stem Cells. Stem. Cells Int. 2017, 2017, 6202783. [Google Scholar] [CrossRef]
- Menini, M.; Delucchi, F.; Bagnasco, F.; Pera, F.; Di Tullio, N.; Pesce, P. Efficacy of air-polishing devices without removal of implant-supported full-arch prostheses. Int. J. Oral. Implantol. 2021, 14, 401–416. [Google Scholar]
- Grande, F.; Mochi Zamperoli, E.; Pozzan, M.C.; Tesini, F.; Catapano, S. Qualitative Evaluation of the Effects of Professional Oral Hygiene Instruments on Prosthetic Ceramic Surfaces. Materials 2021, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Becker, K.; Renvert, S. Efficacy of air polishing for the non-surgical treatment of peri-implant diseases: A systematic review. J. Clin. Periodontol. 2015, 42, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.S.; Shih, K.S.; Lai, C.H.; Takeuchi, Y.; Chen, Y.W. Surface property alterations and osteoblast attachment to contaminated titanium surfaces after different surface treatments: An in vitro study. Clin. Implant Dent. Relat. Res. 2018, 20, 583–591. [Google Scholar] [CrossRef]
- Mombelli, A. Microbiology and antimicrobial therapy of peri-implantitis. Periodontol. 2000 2002, 28, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Penarrocha-Oltra, D.; Covani, U.; Rossetti, P.H. Microbiologic and clinical findings of implants in healthy condition and with peri-implantitis. Oral Maxillofac. Surg. 2015, 30, 834–842. [Google Scholar] [CrossRef]
- Serino, G.; Ström, C. Peri-implantitis in partially edentulous patients: Association with inadequate plaque control. Clin. Oral. Implants Res. 2009, 20, 169–174. [Google Scholar] [CrossRef]
- Pesce, P.; Canullo, L.; Grusovin, M.G.; de Bruyn, H.; Cosyn, J.; Pera, P. Systematic review of some prosthetic risk factors for periimplantitis. J. Prosthet. Dent. 2015, 114, 346–350. [Google Scholar] [CrossRef]
- Subramani, K.; Jung, R.E.; Molenberg, A.; Hämmerle, C.H. Biofilm on dental implants: A review of the literature. Int. J. Oral. Maxillofac. Implants 2009, 24, 616–626. [Google Scholar]
- Menini, M.; Pesce, P.; Bagnasco, F.; Carossa, M.; Mussano, F.; Pera, F. Evaluation of internal and external hexagon connections in immediately loaded full-arch rehabilitations: A within-person randomised split-mouth controlled trial. Int. J. Oral. Implantol. 2019, 12, 169–179. [Google Scholar]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Mombelli, A.; Feloutzis, A.; Brägger, U.; Lang, N.P. Treatment of peri-implantitis by local delivery of tetracycline. Clinical, microbiological and radiological results. Clin. Oral. Implants Res. 2001, 12, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Lessem, J.; Lindahl, C.; Svensson, M. Treatment of incipient peri-implant infections using topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement. J. Int. Acad. Periodontol. 2004, 6, 154–159. [Google Scholar]
- Renvert, S.; Lessem, J.; Dahlen, G.; Lindahl, C.; Svensson, M. Topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement of incipient peri-implant infections: A randomized clinical trial. J. Clin. Periodont. 2006, 33, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral. Implants Res. 2014, 25, 279–287. [Google Scholar] [CrossRef]
- Hoshino, E.; Kurihara-Ando, N.; Sato, I.; Uematsu, H.; Sato, M.; Kota, K.; Iwaku, M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int. J. Endod. 1996, 29, 125–130. [Google Scholar] [CrossRef]
- Ding, R.Y.; Cheung, G.S.P.; Chen, J.; Yin, X.Z.; Wang, Q.Q.; Zhang, C.F. Pulp Revascularization of Immature Teeth with Apical Periodontitis: A Clinical Study. J. Endod. 2009, 35, 745–749. [Google Scholar] [CrossRef]
- Amsden, G.W. Advanced-generation macrolides: Tissue-directed antibiotics. Int. J. Antimicrob. Agents 2001, 18, 11–15. [Google Scholar] [CrossRef]
- Cuffini, A.M.; Tullio, V.; Mandras, N.; Roana, J.; Scalas, D.; Banche, G.; Carlone, N.A. Clarithromycin mediated the expression of polymorphonuclear granulocyte response against streptococcus pneumoniae strains with different patterns of susceptibility and resistance to penicillin and clarithromycin. Int. J. Tissue React. 2002, 24, 37–44. [Google Scholar]
- Mandras, N.; Roana, J.; Allizond, V.; Pasqualini, D.; Crosasso, P.; Burlando, M.; Banche, G.; Denisova, T.; Berutti, E.; Cuffini, A. Antibacterial Efficacy and Drug-Induced Tooth Discolouration of Antibiotic Combinations for Endodontic Regenerative Procedures. Int. J. Immunopathol. Pharmacol. 2013, 26, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Burrell, R.C.; Walters, J.D. Distribution of systemic clarithromycin to gingiva. J. Periodontol. 2008, 79, 1712–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Schlee, M.; Wagner, W.; Covani, U.; Montegrotto Group for the Study of Peri-implant Disease. International Brainstorming Meeting on Etiologic and Risk Factors of Peri-implantitis, Montegrotto (Padua, Italy), August 2014. Int. J. Oral Maxillofac. Implants. 2015, 30, 1093–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alovisi, M.; Carossa, M.; Mandras, N.; Roana, J.; Costalonga, M.; Cavallo, L.; Pira, E.; Putzu, M.G.; Bosio, D.; Roato, I.; et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials 2022, 15, 4850. https://doi.org/10.3390/ma15144850
Alovisi M, Carossa M, Mandras N, Roana J, Costalonga M, Cavallo L, Pira E, Putzu MG, Bosio D, Roato I, et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials. 2022; 15(14):4850. https://doi.org/10.3390/ma15144850
Chicago/Turabian StyleAlovisi, Mario, Massimo Carossa, Narcisa Mandras, Janira Roana, Massimo Costalonga, Lorenza Cavallo, Enrico Pira, Maria Grazia Putzu, Davide Bosio, Ilaria Roato, and et al. 2022. "Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study" Materials 15, no. 14: 4850. https://doi.org/10.3390/ma15144850
APA StyleAlovisi, M., Carossa, M., Mandras, N., Roana, J., Costalonga, M., Cavallo, L., Pira, E., Putzu, M. G., Bosio, D., Roato, I., Mussano, F., & Scotti, N. (2022). Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials, 15(14), 4850. https://doi.org/10.3390/ma15144850