
Assessment of Abdominal Constrictor’s Forces for Informing Computational Models of Orthostatic Hypotension



Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OH | Orthostatic Hypotension |
References
- Joseph, A.; Wanono, R.; Flamant, M.; Vidal-Petiot, E. Orthostatic hypotension: A Review. Néphrologie Thérapeutique 2017, 13. [Google Scholar] [CrossRef]
- Freeman, R.; Abuzinadah, A.R.; Gibbons, C.; Jones, P.; Miglis, M.G.; Sinn, D.I. Orthostatic hypotension. J. Am. Coll. Cardiol. 2018, 72, 1294–1309. [Google Scholar] [CrossRef]
- Gibbons, C.H.; Schmidt, P.; Biaggioni, I.; Frazier-Mills, C.; Freeman, R.; Isaacson, S.; Karabin, B.; Kuritzky, L.; Lew, M.; Low, P.; et al. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. J. Neurol. 2017, 264, 1567–1582. [Google Scholar] [CrossRef] [PubMed]
- Lanier, J.B.; Mote, M.B.; Clay, E.C. Evaluation and management of orthostatic hypotension. Am. Fam. Physician 2011, 84, 527–536. [Google Scholar]
- Farrell, M.C.; Shibao, C.A. Morbidity and mortality in orthostatic hypotension. Auton. Neurosci. 2020, 229, 102717. [Google Scholar] [CrossRef]
- Mol, A.; Bui Hoang, P.T.; Sharmin, S.; Reijnierse, E.M.; van Wezel, R.J.; Meskers, C.G.; Maier, A.B. Orthostatic hypotension and falls in older adults: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2019, 20, 589–597. [Google Scholar] [CrossRef]
- Arnold, A.C.; Raj, S.R. Orthostatic hypotension: A practical approach to investigation and Management. Can. J. Cardiol. 2017, 33, 1725–1728. [Google Scholar] [CrossRef]
- Jameson, J.L.; Kasper, D.L.; Longo, D.L.; Fauci, A.S.; Hauser, S.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Biaggioni, I. Orthostatic hypotension in the hypertensive patient. Am. J. Hypertens. 2018, 31, 1255–1259. [Google Scholar] [CrossRef] [PubMed]
- Eschlböck, S.; Wenning, G.; Fanciulli, A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J. Neural Transm. 2017, 124, 1567–1605. [Google Scholar] [CrossRef] [PubMed]
- Ringer, M.; Lappin, S. Orthostatic Hypotension; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Chelimsky, G.; Chelimsky, T. Non-pharmacologic management of orthostatic hypotension. Auton. Neurosci. 2020, 229, 102732. [Google Scholar] [CrossRef]
- Park, J.W.; Okamoto, L.E.; Shibao, C.A.; Biaggioni, I. Pharmacologic treatment of orthostatic hypotension. Auton. Neurosci. 2020, 229, 102721. [Google Scholar] [CrossRef]
- Gibbons, C.H.; Freeman, R. Delayed orthostatic hypotension. Auton. Neurosci. 2020, 229, 102724. [Google Scholar] [CrossRef]
- Chisholm, P.; Anpalahan, M. Orthostatic hypotension: Pathophysiology, assessment, treatment and the paradox of supine hypertension. Intern. Med. J. 2017, 47, 370–379. [Google Scholar] [CrossRef]
- Low, P.A.; Tomalia, V.A. Orthostatic hypotension: Mechanisms, causes, management. J. Clin. Neurol. 2015, 11, 220. [Google Scholar] [CrossRef] [PubMed]
- Smit, A.A.; Halliwill, J.R.; Low, P.A.; Wieling, W. Pathophysiological basis of orthostatic hypotension in autonomic failure. J. Physiol. 1999, 519, 1–10. [Google Scholar] [CrossRef]
- Bradley, J.; Davis, K. Orthostatic hypotension. Am. Fam. Physician 2003, 68, 2393–2398. [Google Scholar] [PubMed]
- Smit, A.A.; Wieling, W.; Fujimura, J.; Denq, J.C.; Opfer-Gehrking, T.; Akarriou, M.; Karemaker, J.M.; Low, P.A. Use of lower abdominal compression to combat orthostatic hypotension in patients with autonomic dysfunction. Clin. Auton. Res. 2004, 14. [Google Scholar] [CrossRef]
- Baudenbacher, F.; Biaggioni, I.; Harder, R.; Diedrich, A.; Okamoto, L. Compression Device, System, and Method for Decreasing Abdominal Venous Pooling. U.S. Patent No. 10179083, 15 January 2019. [Google Scholar]
- Okamoto, L.E.; Diedrich, A.; Baudenbacher, F.J.; Harder, R.; Whitfield, J.S.; Iqbal, F.; Gamboa, A.; Shibao, C.A.; Black, B.K.; Raj, S.R.; et al. Efficacy of servo-controlled splanchnic venous compression in the treatment of orthostatic hypotension. Hypertension 2016, 68, 418–426. [Google Scholar] [CrossRef]
- Cutsforth-Gregory, J.K.; Low, P.A. Neurogenic orthostatic hypotension inparkinson disease: A Primer. Neurol. Ther. 2019, 8, 307–324. [Google Scholar] [CrossRef] [PubMed]
- Palma, J.A.; Kaufmann, H. Orthostatic hypotension in parkinson disease. Clin. Geriatr. Med. 2020, 36, 53–67. [Google Scholar] [CrossRef]
- Fanciulli, A.; Goebel, G.; Metzler, B.; Sprenger, F.; Poewe, W.; Wenning, G.K.; Seppi, K. Elastic abdominal binders attenuate orthostatic hypotension in parkinson’s disease. Mov. Disord. Clin. Pract. 2015, 3, 156–160. [Google Scholar] [CrossRef]
- Mar, P.L.; Raj, S.R. Orthostatic hypotension for the cardiologist. Curr. Opin. Cardiol. 2018, 33, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Rivasi, G.; Rafanelli, M.; Mossello, E.; Brignole, M.; Ungar, A. Drug-related orthostatic hypotension: Beyond anti-hypertensive medications. Drugs Aging 2020, 37, 725–738. [Google Scholar] [CrossRef]
- Palma, J.A.; Kaufmann, H. Management of orthostatic hypotension. Contin. Lifelong Learn. Neurol. 2020, 26, 154–177. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.J.; Singer, W.; Sandroni, P.; Sletten, D.M.; Gehrking, T.L.; Gehrking, J.A.; Low, P.; Basford, J.R. Effects of patient-controlled abdominal compression on standing systolic blood pressure in adults with orthostatic hypotension. Arch. Phys. Med. Rehabil. 2015, 96, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Magkas, N.; Tsioufis, C.; Thomopoulos, C.; Dilaveris, P.; Georgiopoulos, G.; Sanidas, E.; Papademetriou, V.; Tousoulis, D. Orthostatic hypotension: From pathophysiology to clinical applications and therapeutic considerations. J. Clin. Hypertens. 2019, 21, 546–554. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Sall, F.S.; Sailley, R.; Capellier, G.; Khoury, A. Reliability of manikin-based studies: An evaluation of manikin characteristics and their impact on measurements of ventilatory variables. Anaesthesia 2015, 70, 915–921. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
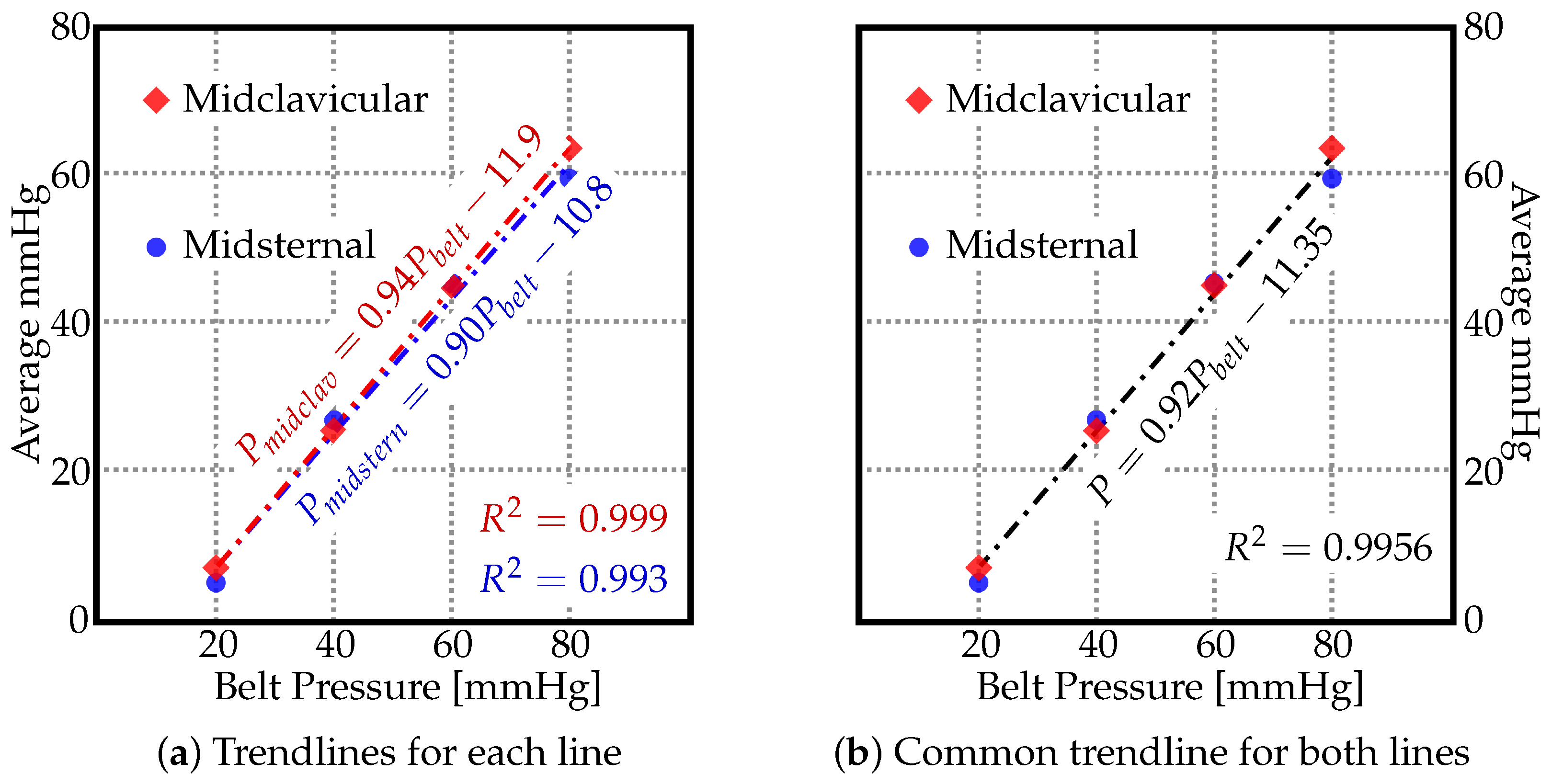
| Midsternal Line | Midclavicular Line | ||||
|---|---|---|---|---|---|
| Belt Pressure (mmHG) | Calculated | Measured (mmHG) | Error % | Measured (mmHG) | Error % |
| 20 | 7.05 | 5.6 | 20.57 | 6.8 | 3.55 |
| 40 | 25.45 | 26.6 | 4.52 | 25.8 | 1.38 |
| 60 | 43.85 | 45 | 2.62 | 44.8 | 2.17 |
| 80 | 62.25 | 59.4 | 4.58 | 63.2 | 1.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed, F.; Jose, R.; Devine, T.; Coletti, C.; Toma, M. Assessment of Abdominal Constrictor’s Forces for Informing Computational Models of Orthostatic Hypotension. Materials 2022, 15, 3116. https://doi.org/10.3390/ma15093116
Syed F, Jose R, Devine T, Coletti C, Toma M. Assessment of Abdominal Constrictor’s Forces for Informing Computational Models of Orthostatic Hypotension. Materials. 2022; 15(9):3116. https://doi.org/10.3390/ma15093116
Chicago/Turabian StyleSyed, Faiz, Rejath Jose, Timothy Devine, Chris Coletti, and Milan Toma. 2022. "Assessment of Abdominal Constrictor’s Forces for Informing Computational Models of Orthostatic Hypotension" Materials 15, no. 9: 3116. https://doi.org/10.3390/ma15093116
APA StyleSyed, F., Jose, R., Devine, T., Coletti, C., & Toma, M. (2022). Assessment of Abdominal Constrictor’s Forces for Informing Computational Models of Orthostatic Hypotension. Materials, 15(9), 3116. https://doi.org/10.3390/ma15093116