
Healing of Alveolar Sockets Treated with Concentrated Growth Factors: A Split-Mouth Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Procedures
2.2. CGF Preparation
2.3. Outcome Variables
2.4. Statistical Analysis
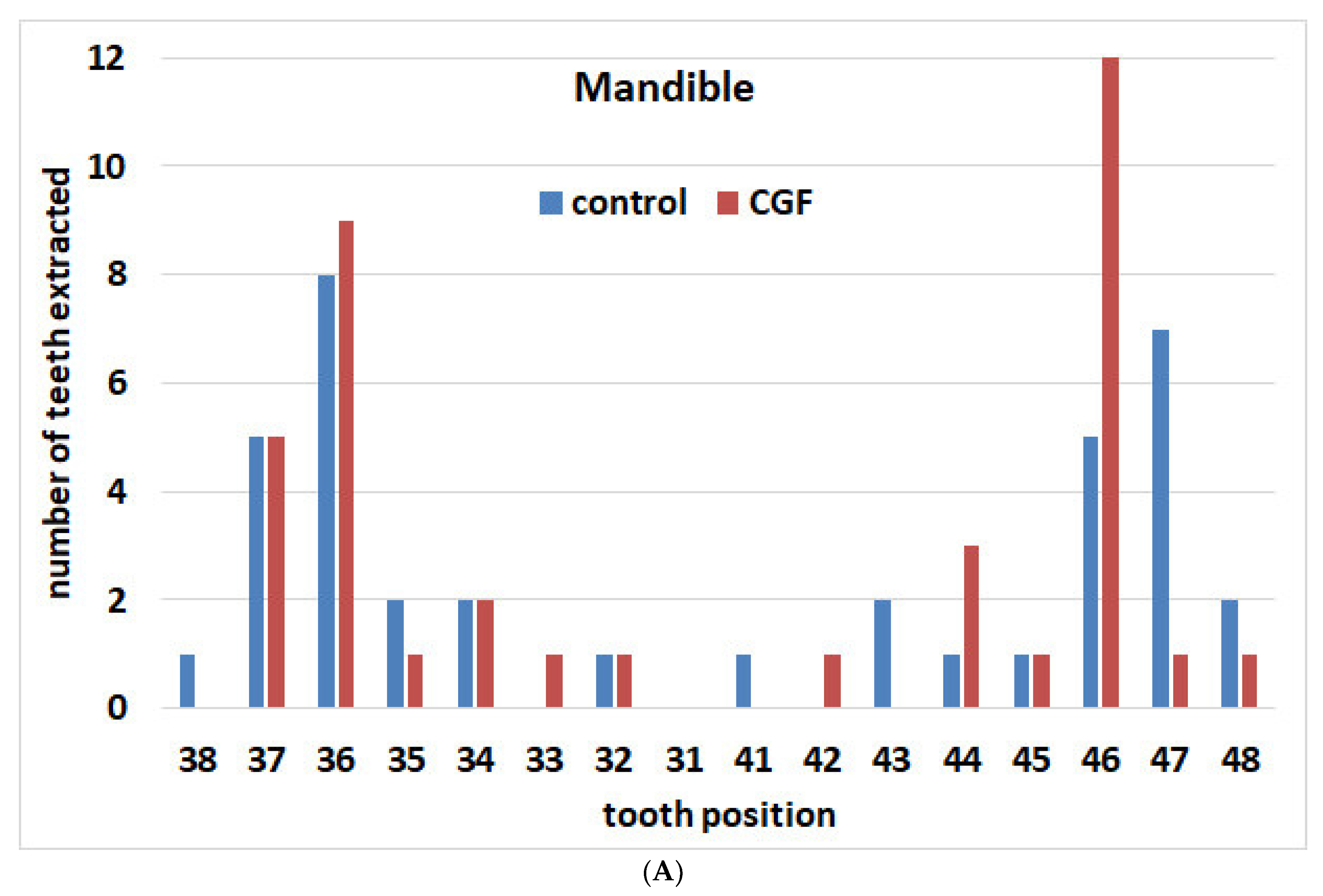
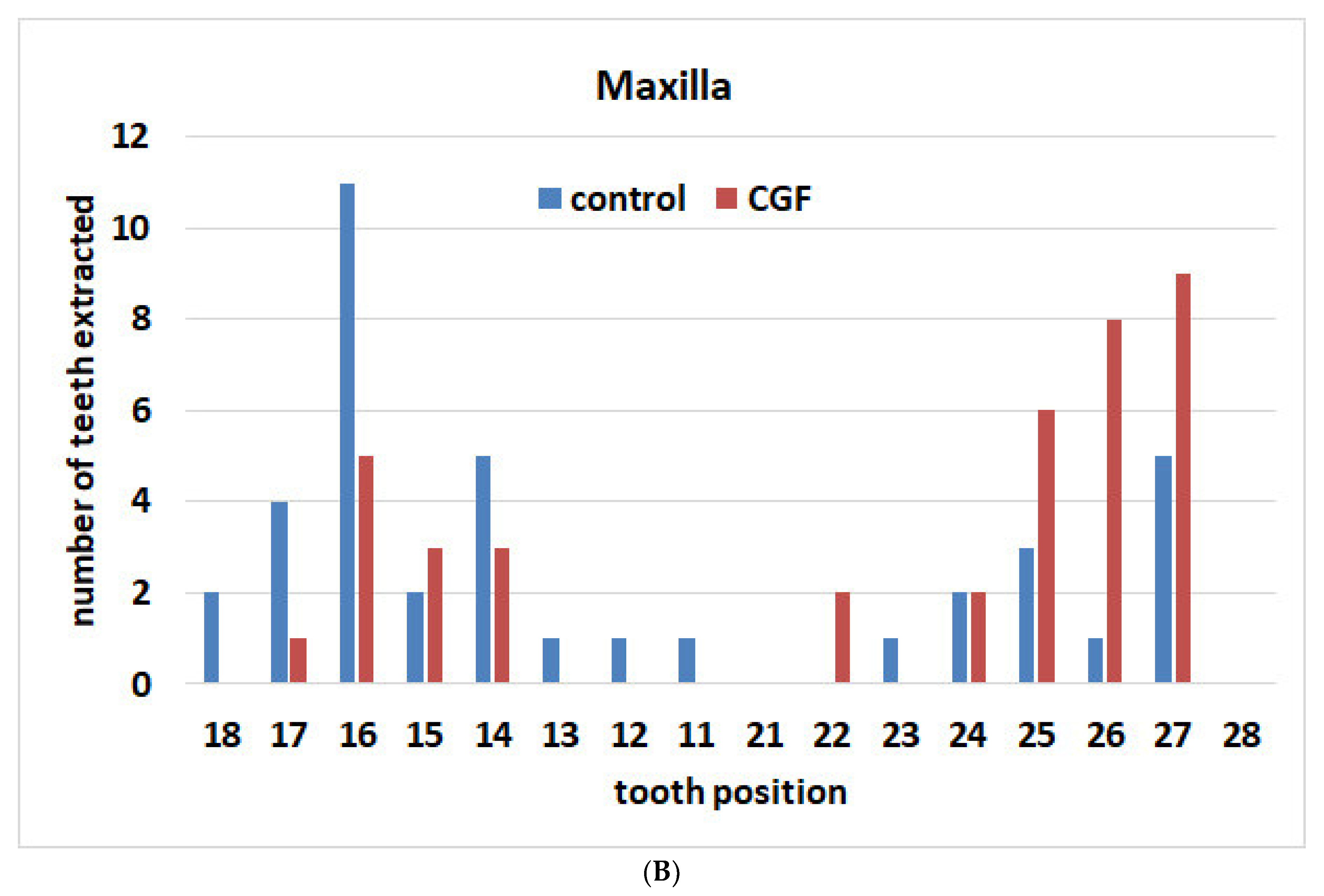
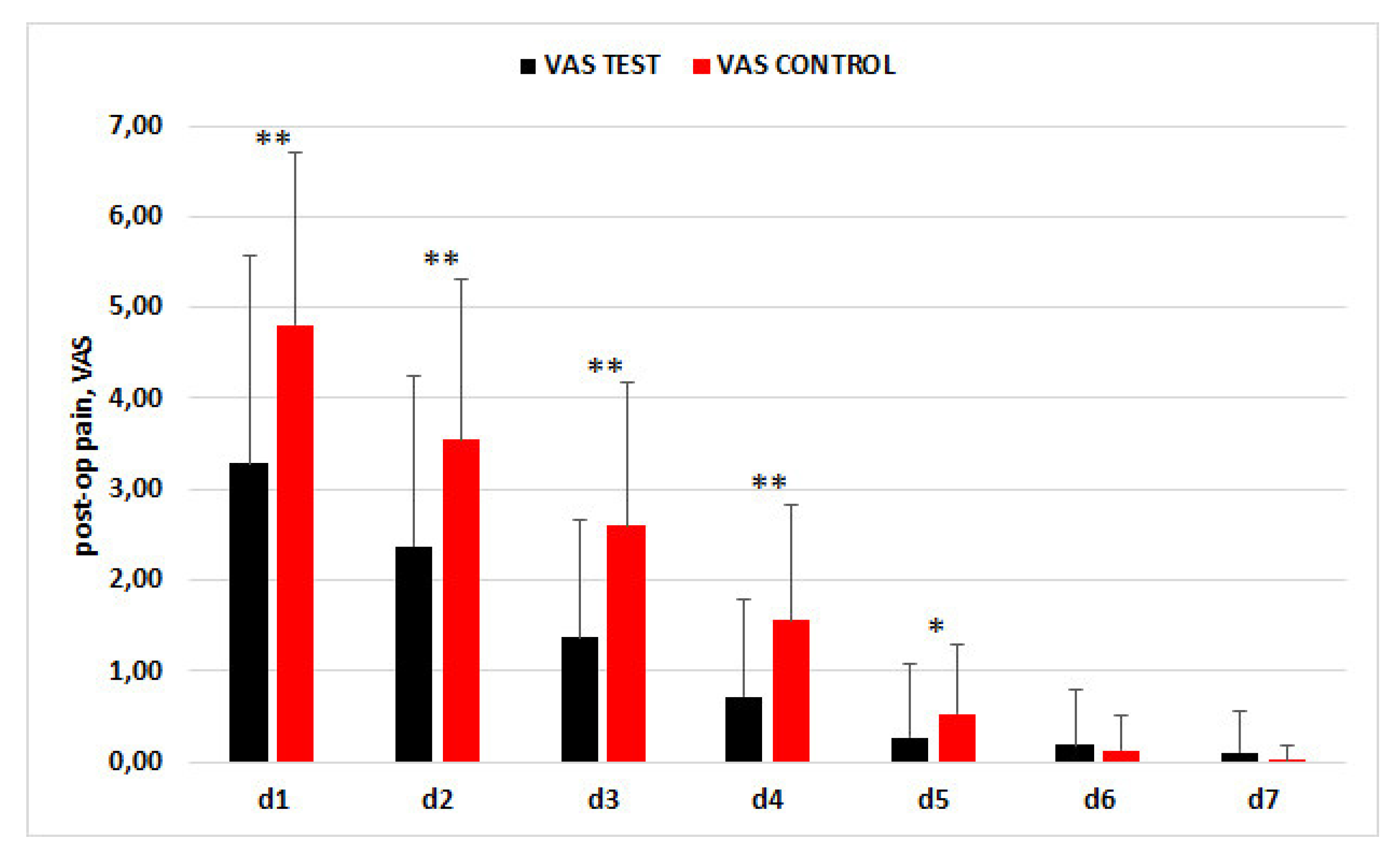
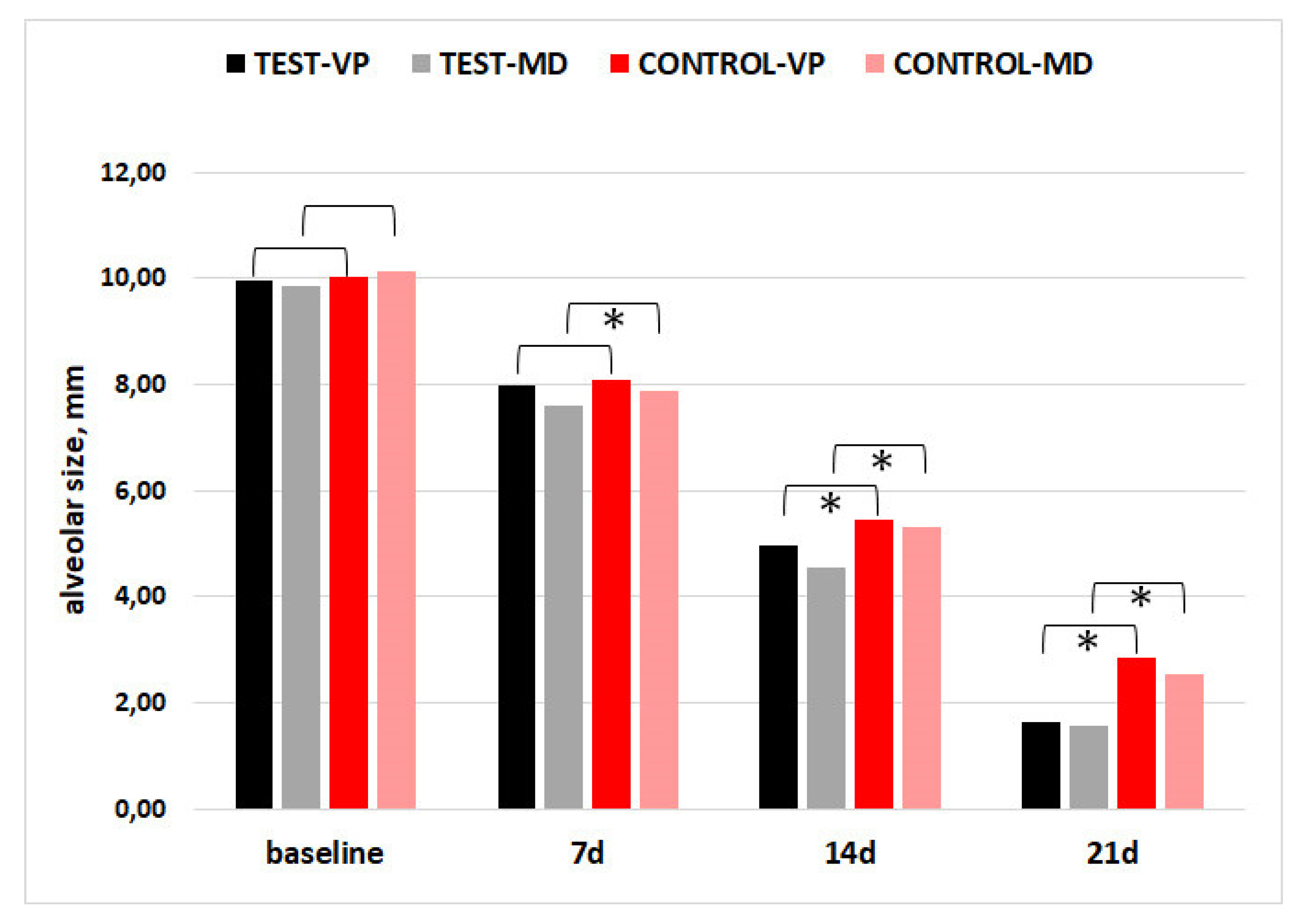
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Del Fabbro, M.; Bucchi, C.; Lolato, A.; Corbella, S.; Testori, T.; Taschieri, S. Healing of Postextraction Sockets Preserved With Autologous Platelet Concentrates. A Systematic Review and Meta-Analysis. J. Oral. Maxillofac. Surg. 2017, 75, 1601–1615. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Lorusso, F.; Postiglione, F.; Mastrangelo, F.; Petrini, M. Photobiomodulation Enhances the Healing of Postextraction Alveolar Sockets: A Randomized Clinical Trial With Histomorphometric Analysis and Immunohistochemistry. J. Oral. Maxillofac. Surg. 2020, 79, 57.e1–57.e12. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Hu, H.; Liu, Y.; Bao, C.; Wang, L. The Effect of Haemostatic Agents on Early Healing of the Extraction Socket. J. Clin. Periodontol. 2019, 46, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Couso-Queiruga, E.; Stuhr, S.; Tattan, M.; Chambrone, L.; Avila-Ortiz, G. Post-Extraction Dimensional Changes: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2021, 48, 126–144. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Francetti, L.; Weinstein, R.; Del Fabbro, M. Histomorphometric Results After Postextraction Socket Healing with Different Biomaterials: A Systematic Review of the Literature and Meta-Analysis. Int. J. Oral Maxillofac. Implant 2017, 32, 1001–1017. [Google Scholar] [CrossRef]
- Anitua, E.; Murias-Freijo, A.; Alkhraisat, M.H.; Orive, G. Clinical, Radiographical, and Histological Outcomes of Plasma Rich in Growth Factors in Extraction Socket: A Randomized Controlled Clinical Trial. Clin. Oral Investig. 2015, 19, 589–600. [Google Scholar] [CrossRef]
- Mozzati, M.; Gallesio, G.; Di Romana, S.; Bergamasco, L.; Pol, R. Efficacy of Plasma-Rich Growth Factor in the Healing of Postextraction Sockets in Patients Affected by Insulin-Dependent Diabetes Mellitus. J. Oral Maxillofac. Surg. 2014, 72, 456–462. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S. Is Autologous Platelet Concentrate Beneficial for Post-Extraction Socket Healing? A Systematic Review. Int. J. Oral. Maxillofac. Surg. 2011, 40, 891–900. [Google Scholar] [CrossRef]
- Rodella, L.F.; Favero, G.; Boninsegna, R.; Buffoli, B.; Labanca, M.; Scarì, G.; Sacco, L.; Batani, T.; Rezzani, R. Growth factors, CD34 positive cells, and fibrin network analysis in concentrated growth factors fraction. Microsc. Res. Technol. 2011, 74, 772–777. [Google Scholar] [CrossRef]
- Landry, R.G. Effectiveness of Benzydamine HC1 in the Treatment of Periodontal Post-Surgical Patients. Ph.D. Thesis, Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 1985. [Google Scholar]
- Masse, J.-F.; Landry, R.G.; Rochette, C.; Dufour, L.; Morency, R.; D’Aoust, P. Effectiveness of Soft Laser Treatment in Periodontal Surgery. Int. Dent. J. 1993, 43, 121–127. [Google Scholar]
- Del Fabbro, M.; Corbella, S.; Taschieri, S.; Francetti, L.; Weinstein, R. Autologous Platelet Concentrate for Post-Extraction Socket Healing: A Systematic Review. Eur. J. Oral Implant 2014, 7, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Isobe, K.; Watanebe, T.; Kawabata, H.; Kitamura, Y.; Okudera, T.; Okudera, H.; Uematsu, K.; Okuda, K.; Nakata, K.; Tanaka, T.; et al. Mechanical and degradation properties of advanced platelet-rich fibrin (A-PRF), concentrated growth factors (CGF), and platelet-poor plasma-derived fibrin (PPTF). Int. J. Implant Dent. 2017, 3, 17. [Google Scholar] [CrossRef]
- Lee, H.-M.; Shen, E.-C.; Shen, J.T.; Fu, E.; Chiu, H.-C.; Hsia, Y.-J. Tensile strength, growth factor content and proliferation activities for two platelet concentrates of platelet-rich fibrin and concentrated growth factor. J. Dent. Sci. 2020, 15, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Riccitiello, F.; Tia, M.; di Lauro, A.; Sammartino, G. Influence of Leukocyte-and Platelet-Rich Fibrin (L-PRF) in the Healing of Simple Postextraction Sockets: A Split-Mouth Study. BioMed Res. Int. 2015, 2015, 369273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Kohli, M.; Gupta, N. Platelet Rich Fibrin: A Novel Approach for Osseous Regeneration. J. Maxillofac. Oral. Surg. 2012, 11, 430–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asmael, H.M.; Jamil, F.A.; Hasan, A.M. Novel Application of Platelet-Rich Fibrin as a Wound Healing Enhancement in Extraction Sockets of Patients Who Smoke. J. Craniofac. Surg. 2018, 29, e794–e797. [Google Scholar] [CrossRef]
- Ustaoğlu, G.; Göller Bulut, D.; Gümüş, K.Ç. Evaluation of different platelet-rich concentrates effects on early soft tissue healing and socket preservation after tooth extraction. J. Stomatol. Oral. Maxillofac. Surg. 2019, 121, 539–544. [Google Scholar] [CrossRef]
- De Almeida Barros Mourão, C.F.; De Mello-Machado, R.C.; Javid, K.; Moraschini, V. The use of leukocyte- and platelet-rich fibrin in the management of soft tissue healing and pain in post-extraction sockets: A randomized clinical trial. J. Craniomaxillofac. Surg. 2020, 48, 452–457. [Google Scholar] [CrossRef]
- Özveri Koyuncu, B.; Işık, G.; Özden Yüce, M.; Günbay, S.; Günbay, T. Effect of concentrated growth factor (CGF) on short-term clinical outcomes after partially impacted mandibular third molar surgery: A split-mouth randomized clinical study. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 118–123. [Google Scholar] [CrossRef]
- Kamal, A.; Salman, B.; Abdul Razak, N.H.; Qabbani, A.A.; Samsudin, A.R. The Efficacy of Concentrated Growth Factor in the Healing of Alveolar Osteitis: A Clinical Study. Int. J. Dent. 2020, 2020, 9038629. [Google Scholar] [CrossRef]
- Kamal, A.; Salman, B.; Razak, N.H.A.; Samsudin, A.B.R. A Comparative Clinical Study between Concentrated Growth Factor and Low-Level Laser Therapy in the Management of Dry Socket. Eur. J. Dent. 2020, 14, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Mozzati, M.; Gallesio, G.; Tumedei, M.; Del Fabbro, M. Concentrated Growth Factors vs Leukocyte-and-Platelet-Rich Fibrin for Enhancing Postextraction Socket Healing. A Longitudinal Comparative Study. Appl. Sci. 2020, 10, 8256. [Google Scholar] [CrossRef]
- Torul, D.; Omezli, M.M.; Kahveci, K. Evaluation of the effects of concentrated growth factors or advanced platelet rich-fibrin on postoperative pain, edema, and trismus following lower third molar removal: A randomized controlled clinical trial. J. Stomatol. Oral. Maxillofac. Surg. 2020, 121, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Pinto, N.R.; Pereda, A.; Jiménez, P.; Corso, M.D.; Kang, B.-S.; Nally, M.; Lanata, N.; Wang, H.-L.; Quirynen, M. The impact of the centrifuge characteristics and centrifugation protocols on the cells, growth factors, and fibrin architecture of a leukocyte-and platelet-rich fibrin (L-PRF) clot and membrane. Platelets 2018, 29, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Bielecki, T.; Jimbo, R.; Barbe, G.; Del Corso, M.; Inchingolo, F.; Sammartino, G. Do the fibrin architecture and leukocyte content influence the growth factor release of platelet concentrates? An evidence-based answer comparing a pure platelet-rich plasma (P-PRP) gel and a leukocyte-and platelet-rich fibrin (L-PRF). Curr. Pharm. Biotechnol. 2012, 13, 1145–1152. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CGF | Control | p-Value | |
|---|---|---|---|
| Maxilla/mandible (n. of elements) | 39/38 | 39/38 | p = 1.00 |
| Cause of extraction (n. of elements)-Advanced caries | 44 | 47 | p = 0.86 |
| -Periodontal disease | 29 | 27 | |
| -Tooth fracture | 4 | 3 | |
| Alveolar size VP/L at baseline, mean ± SD (mm) | 9.95 ± 2.52 | 10.03 ± 2.66 | p = 0.61 |
| Alveolar size MD at baseline, mean ± SD (mm) | 9.87 ± 3.38 | 10.14 ± 3.49 | p = 0.10 |
| Intraoperative complications (number) | 5 | 3 | p = 0.22 |
| Postoperative complications (number) | 0 | 1 | p = 0.50 |
| Healing index at 1 week (score) | 5.01 ± 1.30 | 6.65 ± 1.41 | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mozzati, M.; Tumedei, M.; Gallesio, G.; Menicucci, G.; Manzella, C.; Testori, T.; Fabbro, M.D. Healing of Alveolar Sockets Treated with Concentrated Growth Factors: A Split-Mouth Study. Materials 2022, 15, 4859. https://doi.org/10.3390/ma15144859
Mozzati M, Tumedei M, Gallesio G, Menicucci G, Manzella C, Testori T, Fabbro MD. Healing of Alveolar Sockets Treated with Concentrated Growth Factors: A Split-Mouth Study. Materials. 2022; 15(14):4859. https://doi.org/10.3390/ma15144859
Chicago/Turabian StyleMozzati, Marco, Margherita Tumedei, Giorgia Gallesio, Giulio Menicucci, Carlo Manzella, Tiziano Testori, and Massimo Del Fabbro. 2022. "Healing of Alveolar Sockets Treated with Concentrated Growth Factors: A Split-Mouth Study" Materials 15, no. 14: 4859. https://doi.org/10.3390/ma15144859
APA StyleMozzati, M., Tumedei, M., Gallesio, G., Menicucci, G., Manzella, C., Testori, T., & Fabbro, M. D. (2022). Healing of Alveolar Sockets Treated with Concentrated Growth Factors: A Split-Mouth Study. Materials, 15(14), 4859. https://doi.org/10.3390/ma15144859