
Histologic Evaluation of Soft Tissues around Dental Implant Abutments: A Narrative Review

 , , ,
, , , 
Abstract
:1. Introduction
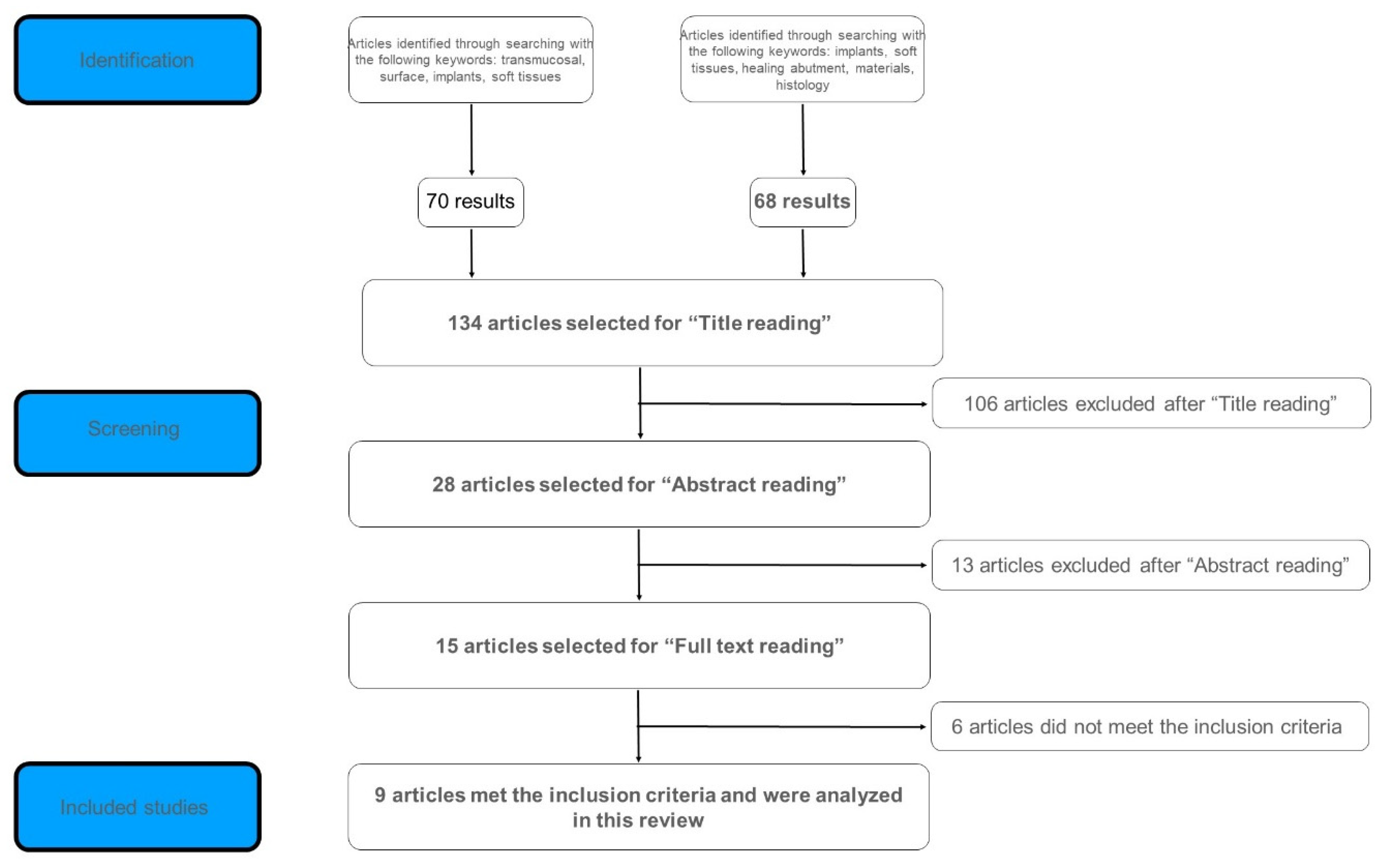
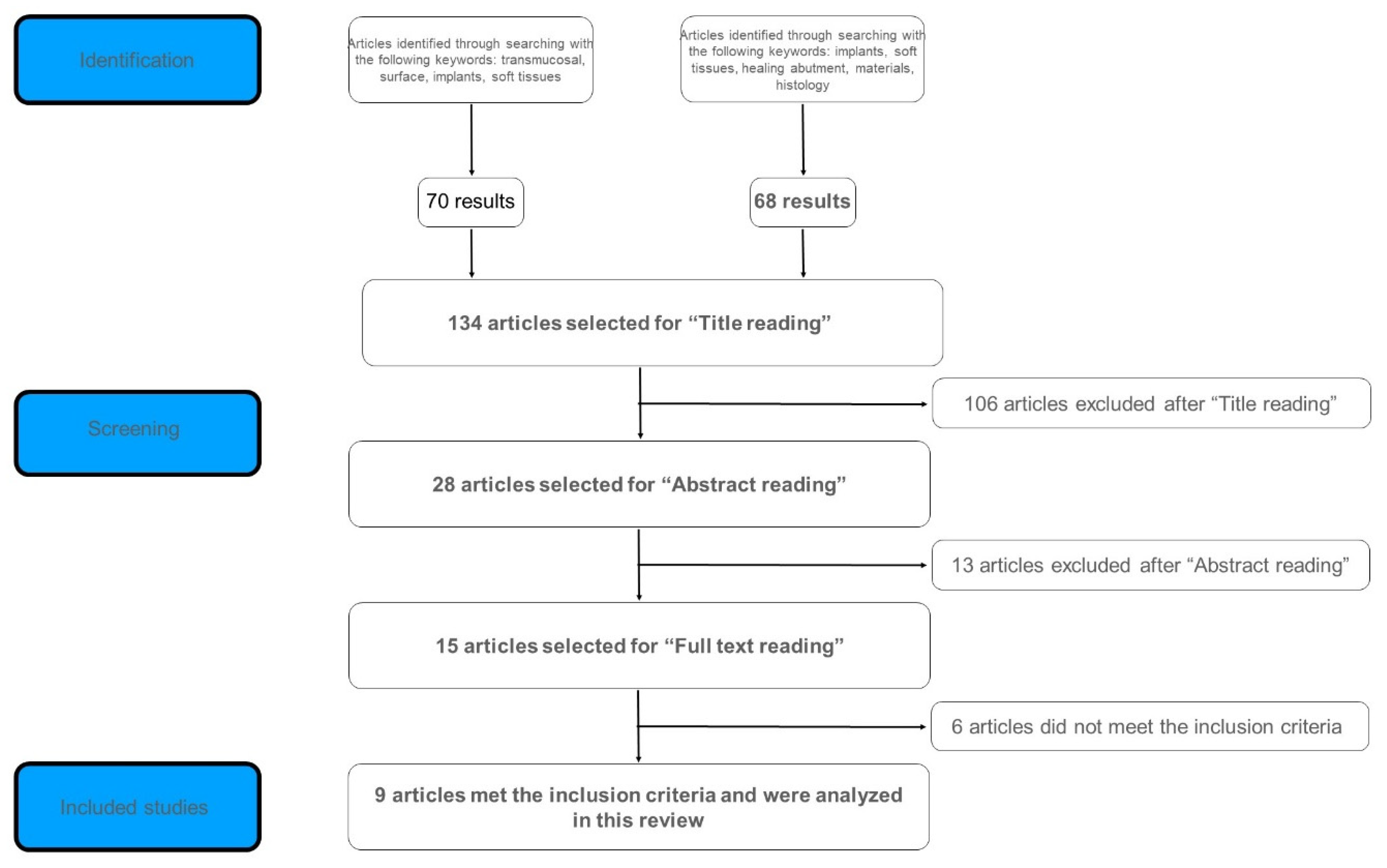
2. Materials and Methods
- -
- human studies
- -
- articles published in English
- -
- randomized clinical trials
- -
- quantitative and/or qualitative histological evaluation of peri-implant soft tissues
- -
- in vitro studies
- -
- animal studies
- -
- articles published in languages other than English
- -
- non-randomized clinical trials
- -
- book chapters
- -
- review or systematic review articles
3. Results

{kind=link}
| Reference | N° of Patients | N° of Implants/Abutments | Experimental Groups | Harvesting Procedure | Histologic Analysis | Results |
|---|---|---|---|---|---|---|
| Glauser et al. (2005) [29] | 5 | 12 titanium mini-implants | Group 1 (4) = oxidized surface Group 2 (4) = acid-etched Group 3 (4) = machined surface | Implants were harvested with a layer of surrounding hard and soft tissues Healing period: 8 weeks | Stereomicroscope/light microscope | Oxidized and acid-etched surface showed a lower epithelium height but a greater connective tissue height when compared to machined surface |
| Wennerberg et al. (2001) [30] | 15 | 30 titanium micro-implants | Control Group (15) = unmodified turned surface Test Group (15) = nanoporous TiO2 surface | Implants were harvested with a layer of surrounding hard and soft tissues. Healing period: 14 weeks | Light microscope/Transmission Electron Microscopy | The mean percentage of oral mucosa in contact with the implant transmucosal part was 72 and 48%, respectively for the test and the control group, with a statistically significant difference (p = 0.027) |
| Degidi et al. (2012) [31] | 11 | 24 implants/24 healing abutments | Control Group (12) = Standard machined, prefabricated titanium caps Test Group (12) = Acid-etched titanium caps | Gingival biopsies 5.5 mm diameter around healing cap surface Healing period: 24 weeks | Light microscope | Tissues around acid-etched titanium caps (test) showed a higher rate of restorative processes which is correlated with a higher inflammation processes observed in these tissues. |
| Schwarz et al. (2013) [32] | 30 | 18 implants/18 healing abutments | M (5) = machined modMA1 (6) = hydrophilic acid etched Ti modMA2 (7) = Ti-zirconium alloy | Healing abutments were harvested with a layer of surrounding soft tissues. Healing period: 8 weeks | Light microscope | No statistically significant differences in terms of percentage of soft tissue to abutment contact, biofilm formation, collagen fibers orientation, and the presence of inflammatory cells. |
| De Wilde et al. (2015) [33] | 13 | 25 mini-implants | Control group (13) = Commercially Pure Ti Test group (12) = Nano-hydroxyapatite coated | Implants were harvested with a layer of surrounding hard and soft tissues. Healing period: 8 weeks | Light microscope/image analysis software | No statistically significant differences in the presence of inflammatory cells nor in the expression of inflammatory mediators. |
| Garcia et al. (2016) [34] | 30 | 30 submerged titanium implants | Control group (15) = standard abutments Test group (15) = plasma-of-argon-cleaned abutments | Special punch for biopsy of soft tissues around abutment. Then abutment is disconnected and replaced with standard healing abutment Healing period: 2 weeks | Polarized light microscope | Test group: Higher area occupied by cells, no bacterial contamination, higher collagen fiber density Group control: Bacterial contamination in 40% |
| Sampatanukul et al. (2017) [35] | 10 | 15 implants/15 healing abutments | Group 1 (5) = titanium abutment Group 3 (5) = zirconia abutment Group 3 (5) = gold alloy abutment | Healing abutments were harvested with a layer of surrounding soft tissues Healing period: 8 weeks | Light microscope | The inflammatory response degree tended to be higher with the gold alloy abutment compared to the titanium abutment. Titanium and Zirconia abutments promoted better attachment percentages compared to gold alloy abutments |
| Mangano et al. (2018) [14] | 50 | 50 implants/abutments | T1 GROUP (11): Healing Abutment with Direct Metal Laser-Sintered Surface T2 GROUP (10): Healing abutment with smooth upper half and DMLS lower half T3 GROUP (19): Healing abutment with DMLS upper half and smooth lower half T4 GROUP (10): Healing abutment completely smooth | Gingival biopsies 1.5 mm wider than the healing screw thickness of average 2.1 mm (5.5 mm-3.8 mm) height of 3 mm Healing period: 4 weeks | Light microscope | Immunohistochemical analysis demonstrated the presence of adhesion molecules (integrins) between the HA and the peri-implant tissues. In HA with DMLS surface the presence of integrins is significantly greater than those found on the Machined surface. All samples were positive for inflammatory infiltrate (CD3 T lymphocytes, CD20 B Lymphocytes, CD68 Macrophages): statistically significant lower infiltrate found in HA with DMLS surface compared to smooth surface. |
| Canullo et al. (2021) [28] | 36 | 36 implants | MAC (smooth-surface-machined) 9-1 drop out, 8 SAMPLES UTM (Ultrathin threaded microsurface) 9 Plasma-MAC (MAC plasma-of-argon-activated) 9 Plasma-UTM (UTM plasma-of-argon-activated) 9 | Gingival biopsies with a 5 mm wide punch. Peri-implant collar of tissue of about 1.3 mm removed with the abutment. Healing period: 8 weeks | Polarized light microscope | MAC surfaces showed to have the ability to improve soft tissues morphogenesis. Moreover, plasma of argon treatment showed a positive effect especially on the connective tissue portion of thin tissues, increasing the ratio between the thickness of connective compartment and epithelium. Approximately 2/3 of MAC and UTM cases showed a moderate or severe grade of inflammation, compared to PLASMA-MAC and PLASMA-UTM surfaces, which exhibited a moderate/severe inflammation only in 1/3 of the cases. Erythematous/exudative process (indicator of inflammation) was absent in PLASMA-MAC group and was observed in all the other groups. The significant performance of plasma groups in terms of soft tissues behavior is visible in case of thin preoperative biotype (less than 2 mm), while it is not in case of thick preoperative biotype (more than 2 mm). |
4. Discussion
- connective tissue height
- percentage of the oral mucosa in contact with the implant transmucosal portion
- biofilm formation and bacterial contamination
- collagen fibers’ orientation and density
- presence of inflammatory cells
- expression of inflammatory mediators and inflammatory infiltrate (CD3 T lymphocytes, CD20 B lymphocytes, CD68 macrophages)
- evaluation of the attachment to the abutment’s surface through the measurement of integrins expression.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.-I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implant. Res. 2008, 19, 635–641. [Google Scholar] [CrossRef]
- Berglundh, T.; Abrahamsson, I.; Welander, M.; Lang, N.P.; Lindhe, J. Morphogenesis of the peri-implant mucosa: An experimental study in dogs. Clin. Oral Implant. Res. 2007, 18, 1–8. [Google Scholar] [CrossRef]
- Cochran, D.L.; Hermann, J.S.; Schenk, R.K.; Higginbottom, F.L.; Buser, D. Biologic Width Around Titanium Implants. A Histometric Analysis of the Implanto-Gingival Junction Around Unloaded and Loaded Nonsubmerged Implants in the Canine Mandible. J. Periodontol. 1997, 68, 186–197. [Google Scholar] [CrossRef]
- Buser, D.; Weber, H.P.; Donath, K.; Fiorellini, J.P.; Paquette, D.W.; Williams, R.C. Soft Tissue Reactions to Non-Submerged Unloaded Titanium Implants in Beagle Dogs. J. Periodontol. 1992, 63, 225–235. [Google Scholar] [CrossRef]
- Ivanovski, S.; Lee, R. Comparison of peri-implant and periodontal marginal soft tissues in health and disease. Periodontology 2000 2018, 76, 116–130. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Wennström, J.; Lindhe, J. The peri-implant hard and soft tissues at different implant systems. A comparative study in the dog. Clin. Oral Implant. Res. 1996, 7, 212–219. [Google Scholar] [CrossRef]
- Listgarten, M.A.; Lang, N.P.; Schroeder, H.E.; Schroeder, A. Periodontal tissues and their counterparts around endosseous implants. Clin. Oral Implant. Res. 1991, 2, 1–19. [Google Scholar] [CrossRef]
- Berglundh, T.; Lindhe, J.; Ericsson, I.; Marinello, C.P.; Liljenberg, B.; Thornsen, P. The soft tissue barrier at implants and teeth. Clin. Oral Implants Res. 1991, 2, 81–90. [Google Scholar] [CrossRef]
- Gould, T.; Westbury, L.; Brunette, D. Ultrastructural study of the attachment of human gingiva to titanium in vivo. J. Prosthet. Dent. 1984, 52, 418–420. [Google Scholar] [CrossRef]
- Rompen, E.; Domken, O.; Degidi, M.; Pontes, A.E.F.; Piattelli, A. The effect of material characteristics, of surface topography and of implant components and connections on soft tissue integration: A literature review. Clin. Oral Implant. Res. 2006, 17, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Jepsen, S.; Stadlinger, B.; Terheyden, H. Peri-implantitis and its prevention. Clin. Oral Implant. Res. 2019, 30, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Mangano, F.G.; Shibli, J.A.; Roth, L.A.; Addazio, G.D.; Piattelli, A.; Iezzi, G. Immunohistochemical Evaluation of Peri-Implant Soft Tissues around Machined and Direct Metal Laser Sintered (DMLS) Healing Abutments in Humans. Int. J. Environ. Res. Public Health 2018, 15, 1611. [Google Scholar] [CrossRef] [Green Version]
- Gulati, K.; Moon, H.-J.; Kumar, P.S.; Han, P.; Ivanovski, S. Anodized anisotropic titanium surfaces for enhanced guidance of gingival fibroblasts. Mater. Sci. Eng. C 2020, 112, 110860. [Google Scholar] [CrossRef] [PubMed]
- Ferraris, S.; Warchomicka, F.; Iranshahi, F.; Rimondini, L.; Cochis, A.; Spriano, S. Electron Beam Structuring of Ti6Al4V: New Insights on the Metal Surface Properties Influencing the Bacterial Adhesion. Materials 2020, 13, 409. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.-W.; Kim, J.-G.; Kim, M.-K.; Ansari, S.; Moshaverinia, A.; Choi, S.-H.; Ryu, J.-J. Effect of laser-dimpled titanium surfaces on attachment of epithelial-like cells and fibroblasts. J. Adv. Prosthodont. 2015, 7, 138–145. [Google Scholar] [CrossRef]
- Alali, A.Q.; Abdal-Hay, A.; Gulati, K.; Ivanovski, S.; Fournier, B.P.J.; Lee, R.S.B. Influence of Bioinspired Lithium-Doped Titanium Implants on Gingival Fibroblast Bioactivity and Biofilm Adhesion. Nanomaterials 2021, 11, 2799. [Google Scholar] [CrossRef]
- Akiyama, Y.; Iwasa, F.; Hotta, Y.; Matsumoto, T.; Oshima, Y.; Baba, K. Effects of surface roughness of ceria-stabilized zirconia/alumina nanocomposite on the morphology and function of human gingival fibroblasts. Dent. Mater. J. 2021, 40, 472–480. [Google Scholar] [CrossRef]
- Rossi, S.; Tirri, T.; Paldan, H.; Kuntsi-Vaattovaara, H.; Tulamo, R.; Närhi, T. Peri-implant tissue response to TiO2 surface modified implants. Clin. Oral Implant. Res. 2008, 19, 348–355. [Google Scholar] [CrossRef]
- Paldan, H.; Areva, S.; Tirri, T.; Peltola, T.; Lindholm, T.C.; Lassila, L.; Pelliniemi, L.J.; Happonen, R.-P.; Närhi, T.O. Soft tissue attachment on sol–gel-treated titanium implants in vivo. J. Mater. Sci. Mater. Med. 2008, 19, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Wieland, M.; Schwartz, Z.; Zhao, G.; Rupp, F.; Geis-Gerstorfer, J.; Schedle, A.; Broggini, N.; Bornstein, M.M.; Buser, D.; et al. Potential of chemically modified hydrophilic surface characteristics to support tissue integration of titanium dental implants. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 88, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Guy, S.; McQuade, M.; Scheidt, M.; McPherson, J.; Rossmann, J.; Van Dyke, T. In Vitro Attachment of Human Gingival Fibroblasts to Endosseous Implant Materials. J. Periodontol. 1993, 64, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Ruano, R.; Jaeger, R.G.; Jaeger, M.M. Effect of a Ceramic and a Non-Ceramic Hydroxyapatite on Cell Growth and Procollagen Synthesis of Cultured Human Gingival Fibroblasts. J. Periodontol. 2000, 71, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidra, A.S.; Rungruanganunt, P. Clinical Outcomes of Implant Abutments in the Anterior Region: A Systematic Review. J. Esthet. Restor. Dent. 2013, 25, 159–176. [Google Scholar] [CrossRef]
- Chai, W.; Moharamzadeh, K.; Brook, I.; Van Noort, R. A review of histomorphometric analysis techniques for assessing implant-soft tissue interface. Biotech. Histochem. 2011, 86, 242–254. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Canullo, L.; Cochran, D.; De Bruyn, H. “Peri-Implantitis”: A Complication of a Foreign Body or a Man-Made “Disease”. Facts and Fiction. Clin. Implant Dent. Relat. Res. 2016, 18, 840–849. [Google Scholar] [CrossRef]
- Canullo, L.; Annunziata, M.; Pesce, P.; Tommasato, G.; Nastri, L.; Guida, L. Influence of abutment material and modifications on peri-implant soft-tissue attachment: A systematic review and meta-analysis of histological animal studies. J. Prosthet. Dent. 2021, 125, 426–436. [Google Scholar] [CrossRef]
- Glauser, R.; Schupbach, P.; Gottlow, J.; Dds, C.H.F.H. Periimplant Soft Tissue Barrier at Experimental One-Piece Mini-implants with Different Surface Topography in Humans: A Light-Microscopic Overview and Histometric Analysis. Clin. Implant Dent. Relat. Res. 2005, 7, s44–s51. [Google Scholar] [CrossRef]
- Wennerberg, A.; Fröjd, V.; Olsson, M.; Nannmark, U.; Emanuelsson, L.; Johansson, P.; Josefsson, Y.; Kangasniemi, I.; Peltola, T.; Tirri, T.; et al. Nanoporous TiO2 Thin Film on Titanium Oral Implants for Enhanced Human Soft Tissue Adhesion: A Light and Electron Microscopy Study. Clin. Implant Dent. Relat. Res. 2011, 13, 184–196. [Google Scholar] [CrossRef]
- Degidi, M.; Artese, L.; Piattelli, A.; Scarano, A.; Shibli, J.A.; Piccirilli, M.; Perrotti, V.; Iezzi, G. Histological and immunohistochemical evaluation of the peri-implant soft tissues around machined and acid-etched titanium healing abutments: A prospective randomised study. Clin. Oral Investig. 2012, 16, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Mihatovic, I.; Becker, J.; Bormann, K.H.; Keeve, P.L.; Friedmann, A. Histological evaluation of different abutments in the posterior maxilla and mandible: An experimental study in humans. J. Clin. Periodontol. 2013, 40, 807–815. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, E.A.; Jimbo, R.; Wennerberg, A.; Naito, Y.; Coucke, P.; Bryington, M.S.; Vandeweghe, S.; De Bruyn, H. The Soft Tissue Immunologic Response to Hydroxyapatite-Coated Transmucosal Implant Surfaces: A Study in Humans. Clin. Implant Dent. Relat. Res. 2015, 17, e65–e74. [Google Scholar] [CrossRef] [PubMed]
- Garcia, B.; Camacho, F.; Penarrocha, D.; Tallarico, M.; Perez, S.; Canullo, L. Influence of Plasma Cleaning procedure on the interaction between soft tissue and abutments: A randomized controlled histologic study. Clin. Oral Implant. Res. 2017, 28, 1269–1277. [Google Scholar] [CrossRef]
- Sampatanukul, T.; Serichetaphongse, P.; Pimkhaokham, A. Histological evaluations and inflammatory responses of different dental implant abutment materials: A human histology pilot study. Clin. Implant Dent. Relat. Res. 2018, 20, 160–169. [Google Scholar] [CrossRef]
- Löe, H.; Silness, J. Periodontal Disease in Pregnancy, I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Cosyn, J.; De Rouck, T. Aesthetic outcome of single-tooth implant restorations following early implant placement and guided bone regeneration: Crown and soft tissue dimensions compared with contralateral teeth. Clin. Oral Implant. Res. 2009, 20, 1063–1069. [Google Scholar] [CrossRef]
- Gulati, K.; Ivanovski, S. Dental implants modified with drug releasing titania nanotubes: Therapeutic potential and developmental challenges. Expert Opin. Drug Deliv. 2017, 14, 1009–1024. [Google Scholar] [CrossRef]
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Race to invade: Understanding soft tissue integration at the transmucosal region of titanium dental implants. Dent. Mater. 2021, 37, 816–831. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Sanz-Martín, I.; de Albornoz, A.C.; Figuero, E.; Sanz, M. Biological effect of the abutment material on the stability of peri-implant marginal bone levels: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 124–144. [Google Scholar] [CrossRef] [Green Version]
- Furuhashi, A.; Ayukawa, Y.; Atsuta, I.; Rakhmatia, Y.; Koyano, K. Soft Tissue Interface with Various Kinds of Implant Abutment Materials. J. Clin. Med. 2021, 10, 2386. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cinquini, C.; Marchio, V.; Di Donna, E.; Alfonsi, F.; Derchi, G.; Nisi, M.; Barone, A. Histologic Evaluation of Soft Tissues around Dental Implant Abutments: A Narrative Review. Materials 2022, 15, 3811. https://doi.org/10.3390/ma15113811
Cinquini C, Marchio V, Di Donna E, Alfonsi F, Derchi G, Nisi M, Barone A. Histologic Evaluation of Soft Tissues around Dental Implant Abutments: A Narrative Review. Materials. 2022; 15(11):3811. https://doi.org/10.3390/ma15113811
Chicago/Turabian StyleCinquini, Chiara, Vincenzo Marchio, Edouard Di Donna, Fortunato Alfonsi, Giacomo Derchi, Marco Nisi, and Antonio Barone. 2022. "Histologic Evaluation of Soft Tissues around Dental Implant Abutments: A Narrative Review" Materials 15, no. 11: 3811. https://doi.org/10.3390/ma15113811
APA StyleCinquini, C., Marchio, V., Di Donna, E., Alfonsi, F., Derchi, G., Nisi, M., & Barone, A. (2022). Histologic Evaluation of Soft Tissues around Dental Implant Abutments: A Narrative Review. Materials, 15(11), 3811. https://doi.org/10.3390/ma15113811