
Discoloration Potential of Biodentine: A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
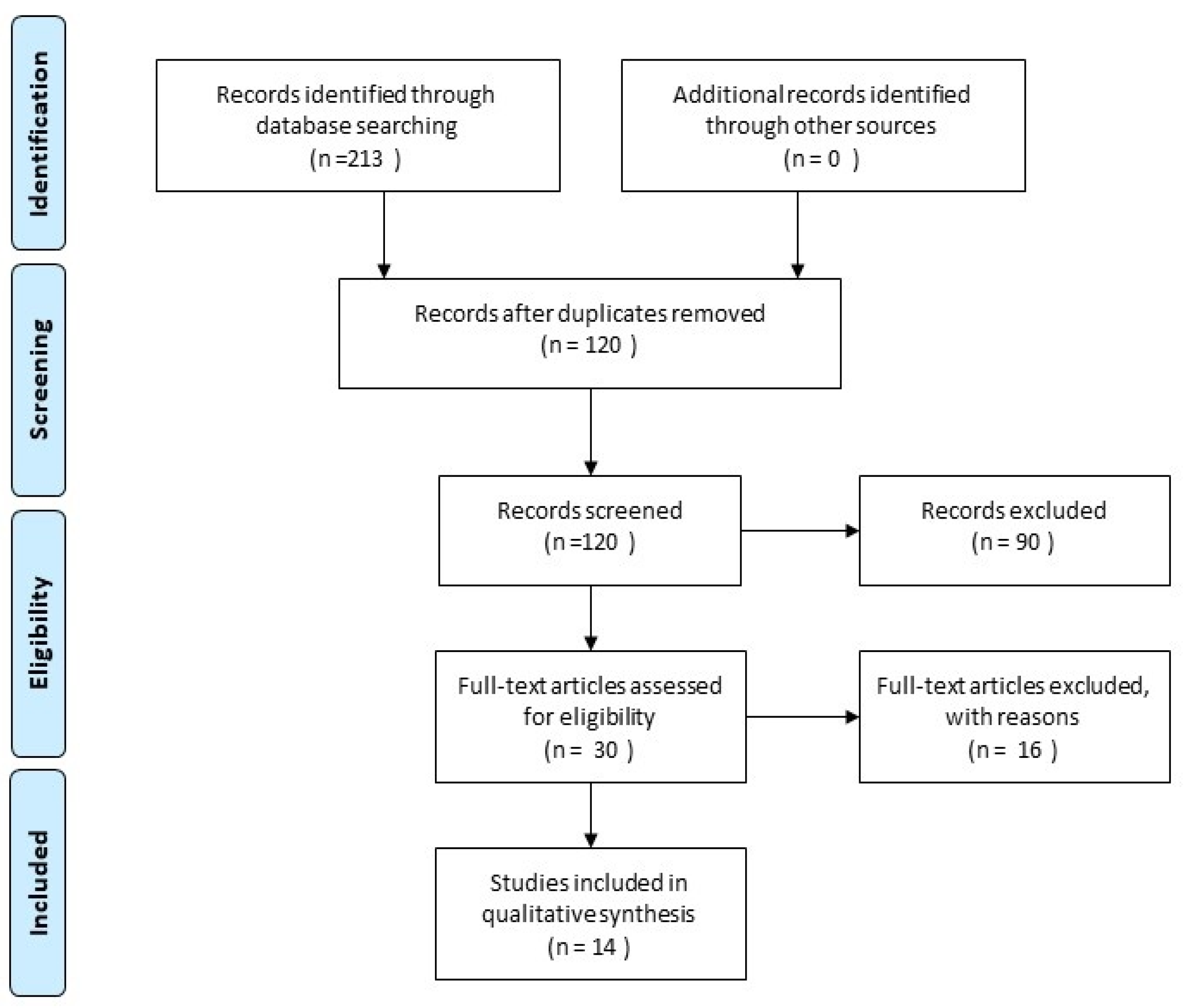
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
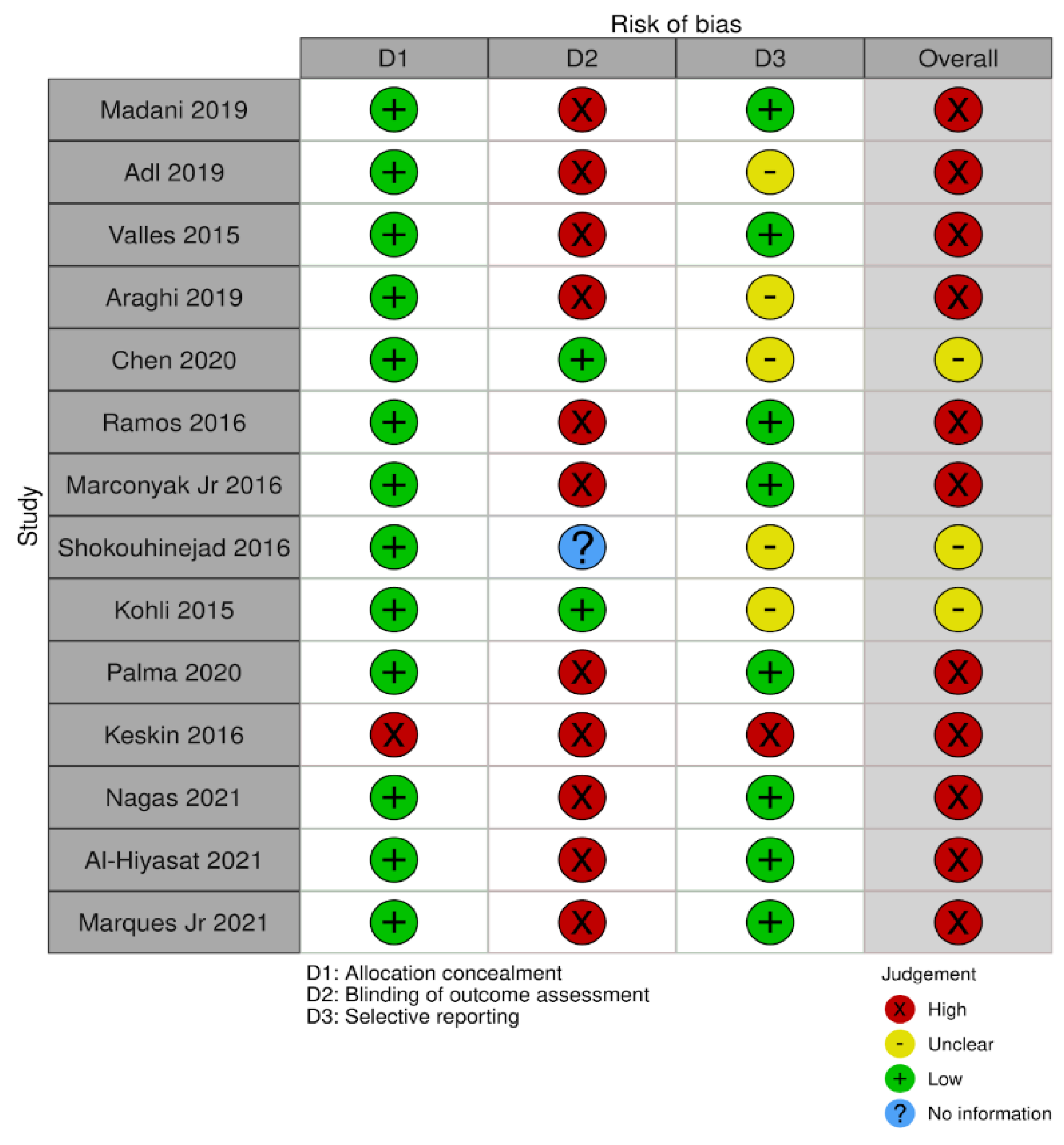
2.4. Risk of Bias Assessment
3. Results
3.1. Risk of Bias Assessment
3.2. Study Characteristics
3.3. Discoloration Potential in the Presence of Blood
3.4. Discoloration Potential in the Absence of Blood
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chugal, N.; Mallya, S.M.; Kahler, B.; Lin, L.M. Endodontic treatment outcomes. Dent. Clin. N. Am. 2017, 61, 59–80. [Google Scholar] [CrossRef] [PubMed]
- Felman, D.; Parashos, P. Coronal tooth discoloration and white mineral trioxide aggregate. J. Endod. 2013, 39, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Lenherr, P.; Allgayer, N.; Weiger, R.; Filippi, A.; Attin, T.; Krastl, G. Tooth discoloration induced by endodontic materials: A laboratory study. Int. Endod. J. 2012, 45, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Malkondu, Ö.; Kazandağ, M.K.; Kazazoğlu, E. A review on biodentine, a contemporary dentine replacement and repair material. BioMed Res. Int. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahler, B.; Rossi-Fedele, G. A review of tooth discoloration after regenerative endodontic Therapy. J. Endod. 2016, 42, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Singh, H.; Dhillon, J.S.; Batra, M.; Saini, M. MTA versus biodentine: Review of literature with a comparative analysis. J. Clin. Diagn. Res. 2017, 11, ZG01–ZG05. [Google Scholar] [CrossRef]
- Torabinejad, M.; Parirokh, M.; Dummer, P. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview - part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317. [Google Scholar] [CrossRef]
- Dawood, A.E.; Parashos, P.; Wong, R.H.; Reynolds, E.C.; Manton, D.J. Calcium silicate-based cements: Composition, properties, and clinical applications. J. Investig. Clin. Dent. 2017, 8, e12195. [Google Scholar] [CrossRef] [PubMed]
- Marciano, M.A.; Costa, R.M.; Camilleri, J.; Mondelli, R.; Guimarães, B.M.; Duarte, M.A.H. Assessment of color stability of white mineral trioxide aggregate angelus and bismuth oxide in contact with tooth structure. J. Endod. 2014, 40, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Możyńska, J.; Metlerski, M.; Lipski, M.; Nowicka, A. tooth discoloration induced by different calcium silicate–based cements: A systematic review of in vitro studies. J. Endod. 2017, 43, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Yoldaş, S.E.; Bani, M.; Atabek, D.; Bodur, H. Comparison of the potential discoloration effect of bioaggregate, biodentine, and white mineral trioxide aggregate on bovine teeth: In vitro research. J. Endod. 2016, 42, 1815–1818. [Google Scholar] [CrossRef] [PubMed]
- Junior, R.B.M.; Baroudi, K.; dos Santos, A.F.C.; Pontes, D.; Amaral, M. Tooth discoloration using calcium silicate-based cements for simulated revascularization in vitro. Braz. Dent. J. 2021, 32, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Al-Hiyasat, A.S.; Ahmad, D.M.; Khader, Y.S. The effect of different calcium silicate-based pulp capping materials on tooth discoloration: An in vitro study. BMC Oral Health 2021, 21, 330. [Google Scholar] [CrossRef]
- Nagas, E.; Ertan, A.; Eymirli, A.; Uyanik, O.; Cehreli, Z.C. Tooth discoloration induced by different calcium silicate–based cements: A two-year spectrophotometric and photographic evaluation in vitro. J. Clin. Pediatr. Dent. 2021, 45, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Chugal, N.; Lin, L.M. Alkaline materials and regenerative endodontics: A review. Materials 2017, 10, 1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camilleri, J. Color stability of white mineral trioxide aggregate in contact with hypochlorite solution. J. Endod. 2014, 40, 436–440. [Google Scholar] [CrossRef]
- Vallés, M.; Mercade, M.; Duran-Sindreu, F.; Bourdelande, J.L.; Roig, M. Color stability of white mineral trioxide aggregate. Clin. Oral Investig. 2012, 17, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Katge, F.A.; Patil, D.P. Comparative analysis of 2 calcium silicate-based cements (Biodentine and mineral trioxide aggregate) as direct pulp-capping agent in young permanent molars: A split mouth study. J. Endod. 2017, 43, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Kaup, M.; Schäfer, E.; Dammaschke, T. An in vitro study of different material properties of Biodentine compared to ProRoot MTA. Head Face Med. 2015, 11, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, T.; Baratz, A.Z.; Gutmann, J.L. In vitro investigations into the etiology of mineral trioxide tooth staining. J. Conserv. Dent. 2014, 17, 526–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvandifar, S.; Madani, Z.; Bizhani, A. Evaluation of tooth discoloration after treatment with mineral trioxide aggregate, calcium-enriched mixture, and Biodentine® in the presence and absence of blood. Dent. Res. J. 2019, 16, 377. [Google Scholar] [CrossRef]
- Ramos, J.C.; Palma, P.J.; Nascimento, R.; Caramelo, F.; Messias, A.; Vinagre, A.; Santos, J.M. 1-year In Vitro Evaluation of Tooth Discoloration Induced by 2 Calcium Silicate–based Cements. J. Endod. 2016, 42, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Shokouhinejad, N.; Nekoofar, M.H.; Pirmoazen, S.; Shamshiri, A.R.; Dummer, P. Evaluation and comparison of occurrence of tooth discoloration after the application of various calcium silicate–based cements: An ex vivo study. J. Endod. 2016, 42, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Kohli, M.R.; Yamaguchi, M.; Setzer, F.C.; Karabucak, B. Spectrophotometric analysis of coronal tooth discoloration induced by various bioceramic cements and other endodontic materials. J. Endod. 2015, 41, 1862–1866. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.J.; Karabucak, B.; Steffen, J.J.; Yu, Y.-H.; Kohli, M.R. Spectrophotometric analysis of coronal tooth discoloration induced by tricalcium silicate cements in the presence of blood. J. Endod. 2020, 46, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Marques, J.A.; Santos, J.; Falacho, R.I.; Sequeira, D.; Diogo, P.; Caramelo, F.; Ramos, J.C.; Santos, J.M. Tooth discoloration after regenerative endodontic procedures with calcium silicate-based cements—An ex vivo study. Appl. Sci. 2020, 10, 5793. [Google Scholar] [CrossRef]
- Vallés, M.; Roig, M.; Duran-Sindreu, F.; Martínez, S.; Mercadé, M. Color stability of teeth restored with Biodentine: A 6-month in vitro study. J. Endod. 2015, 41, 1157–1160. [Google Scholar] [CrossRef]
- Marconyak, L.J., Jr.; Kirkpatrick, T.C.; Roberts, H.W.; Roberts, M.D.; Aparicio, A.; Himel, V.T.; Sabey, K.A. A comparison of coronal tooth discoloration elicited by Various endodontic reparative materials. J. Endod. 2016, 42, 470–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camilleri, J. Staining potential of Neo MTA Plus, MTA Plus, and Biodentine used for pulpotomy procedures. J. Endod. 2015, 41, 1139–1145. [Google Scholar] [CrossRef]
- Vallés, M.; Mercade, M.; Duran-Sindreu, F.; Bourdelande, J.L.; Roig, M. Influence of light and oxygen on the color stability of five calcium silicate–based materials. J. Endod. 2013, 39, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-H.; Shin, Y.-S.; Lee, H.-S.; Kim, S.-O.; Shin, Y.; Jung, I.-Y.; Song, J.S. Color changes of teeth after treatment with various mineral trioxide aggregate–based materials: An ex vivo study. J. Endod. 2015, 41, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Parinyaprom, N.; Nirunsittirat, A.; Chuveera, P.; Na Lampang, S.; Srisuwan, T.; Sastraruji, T.; Bua-on, P.; Simprasert, S.; Khoipanich, I.; Sutharaphan, T.; et al. Outcomes of direct pulpcapping by using either ProRoot mineral trioxide aggregateor Biodentine in permanent teeth with carious pulpexposure in 6- to 18-year-old patients: A randomizedcontrolled trial. J. Endod. 2018, 44, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Abuelniel, G.M.; Duggal, M.S.; Kabel, N. A comparison of MTA and Biodentine as medicaments for pulpotomy in trau-matized anterior immature permanent teeth: A randomized clinical trial. Dent. Traumatol. 2020, 36, 400–410. [Google Scholar] [CrossRef]
- Linu, S.; Lekshmi, M.; Varunkumar, V.; Joseph, V.S. Treatment outcome following direct pulp capping using bioceramic materials in mature permanent teeth with carious exposure: A pilot retrospective study. J. Endod. 2017, 43, 1635–1639. [Google Scholar] [CrossRef] [PubMed]
- Aly, M.M.; Taha, S.E.E.; El Sayed, M.A.; Youssef, R.; Omar, H.M. Clinical and radiographic evaluation of Biodentine and Mineral Trioxide Aggregate in revascularization of non-vital immature permanent anterior teeth (randomized clinical study). Int. J. Paediatr. Dent. 2019, 29, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Haikal, L.; dos Santos, B.F.; Vu, D.-D.; Braniste, M.; Dabbagh, B. Biodentine pulpotomies on permanent traumatized teeth with complicated crown fractures. J. Endod. 2020, 46, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- Uesrichai, N.; Nirunsittirat, A.; Chuveera, P.; Srisuwan, T.; Sastraruji, T.; Chompu-Inwai, P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: A noninferiority randomized controlled trial. Int. Endod. J. 2019, 52, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane, 2021. Available online: www.training.cochrane.org/handbook (accessed on 21 July 2021).
- Keskin, C.; Sarıyılmaz, E. Tooth discoloration induced by calcium silicate-based materials in contact with blood. Int. J. Clin. Dent. 2016, 9, 47–51. [Google Scholar]
- Godiny, M.; Araghi, S.; Khavid, A.; Saeidipour, M. In vitro evaluation of coronal discoloration following the application of calcium-enriched mixture cement, Biodentine, and mineral trioxide aggregate in endodontically treated teeth. Dent. Res. J. 2019, 16, 53. [Google Scholar] [CrossRef]
- Abbaszadegan, A.; Adl, A.; Javanmardi, S. Assessment of tooth discoloration induced by biodentine and white mineral trioxide aggregate in the presence of blood. J. Conserv. Dent. 2019, 22, 164–168. [Google Scholar] [CrossRef]
- Dozić, A.; Kleverlaan, C.J.; El-Zohairy, A.; Feilzer, A.J.; Khashayar, G. Performance of five commercially available tooth color-measuring devices. J. Prosthodont. 2007, 16, 93–100. [Google Scholar] [CrossRef]
- Gómez-Polo, C.; Gómez-Polo, M.; Celemin-Viñuela, A.; De Parga, J.A.M.V. Differences between the human eye and the spectrophotometer in the shade matching of tooth colour. J. Dent. 2014, 42, 742–745. [Google Scholar] [CrossRef] [PubMed]
- Igiel, C.; Weyhrauch, M.; Wentaschek, S.; Scheller, H.; Lehmann, K.M. Dental color matching: A comparison between visual and instrumental methods. Dent. Mater. J. 2016, 35, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, S.; Peter, A.; Pietrobon, N.; Hämmerle, C. Visual and spectrophotometric shade analysis of human teeth. J. Dent. Res. 2002, 81, 578–582. [Google Scholar] [CrossRef]
- Brandt, J.; Nelson, S.; Lauer, H.-C.; Von Hehn, U.; Brandt, S. In vivo study for tooth colour determination—visual versus digital. Clin. Oral Investig. 2017, 42, 2863–2871. [Google Scholar] [CrossRef] [PubMed]
- Hugo, B.; Witzel, T.; Klaiber, B. Comparison of in vivo visual and computer-aided tooth shade determination. Clin. Oral Investig. 2005, 9, 244–250. [Google Scholar] [CrossRef]
- Moodley, D.S.; Patel, N.; Moodley, T.; Ranchod, H. Comparison of colour differences in visual versus spectrophotometric shade matching. S. Afr. Dent. J. 2015, 70, 402–407. [Google Scholar]
- Derdilopoulou, F.V.; Zantner, C.; Neumann, K.; Kielbassa, A.M. Evaluation of visual and spectrophotometric shade analyses: A clinical comparison of 3758 teeth. Int. J. Prosthodont. 2007, 20, 414–416. [Google Scholar] [PubMed]
- ISO/TR 28642:2016(en) Dentistry—Guidance on Colour Measurement. Available online: https://www.iso.org/obp/ui/#iso:std:69046:en (accessed on 1 July 2021).
- International Commission on Illumination. Recommendations on Uniform Color Spaces, Color-Difference Equations, Psychometric Color Terms. 15; Bureau Central de la CIE: Vienna, Austria, 1978; p. 13. [Google Scholar]
- de Dios Teruel, J.; Alcolea, A.; Hernández, A.; Ortiz-Ruiz, A.J. Comparison of chemical composition of enamel and dentine in human, bovine, porcine and ovine teeth. Arch. Oral Biol. 2015, 60, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Camargo, M.A.; Marques, M.M.; de Cara, A.A. Morphological analysis of human and bovine dentine by scanning electron microscope investigation. Arch. Oral Biol. 2008, 53, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Schilke, R.; Lisson, J.A.; Bauß, O.; Geurtsen, W. Comparison of the number and diameter of dentinal tubules in human and bovine dentine by scanning electron microscopic investigation. Arch. Oral Biol. 2000, 45, 355–361. [Google Scholar] [CrossRef]
- Nakamichi, I.; Iwaku, M.; Fusayama, T. Bovine teeth as possible substitutes in the adhesion test. J. Dent. Res. 1983, 62, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Yassen, G.H.; Platt, J.A.; Hara, A. Bovine teeth as substitute for human teeth in dental research: A review of literature. J. Oral Sci. 2011, 53, 273–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Ruiz, A.J.; Teruel-Fernández, J.D.D.; Alcolea-Rubio, L.A.; Hernández-Fernández, A.; Martínez-Beneyto, Y.; Guirado, F.G. Structural differences in enamel and dentin in human, bovine, porcine, and ovine teeth. Ann. Anat. 2018, 218, 7–17. [Google Scholar] [CrossRef]
- Sumikawa, D.A.; Marshall, G.W.; Gee, L.; Marshall, S.J. Microstructure of primary tooth dentin. Pediatr. Dent. 1999, 21, 439–444. [Google Scholar] [PubMed]
- Marin, P.D.; Bartold, P.; Heithersay, G.S. Tooth discoloration by blood: An in vitro histochemical study. Dent. Traumatol. 1997, 13, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Bhavya, B.; Sadique, M.; Simon, E.P.; Ravi, S.; Lal, S. Spectrophotometric analysis of coronal discoloration induced by white mineral trioxide aggregate and Biodentine: An in vitro study. J. Conserv. Dent. 2017, 20, 237–240. [Google Scholar] [CrossRef]
- Namazikhah, M.S.; Nekoofar, M.H.; Sheykhrezae, M.S.; Salariyeh, S.; Hayes, S.J.; Bryant, S.T.; Mohammadi, M.M.; Dummer, P.M.H. The effect of pH on surface hardness and microstructure of mineral trioxide aggregate. Int. Endod. J. 2008, 41, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Marciano, M.A.; Duarte, M.A.H.; Camilleri, J. Dental discoloration caused by bismuth oxide in MTA in the presence of sodium hypochlorite. Clin. Oral Investig. 2015, 19, 2201–2209. [Google Scholar] [CrossRef] [PubMed]
- Keskin, C.; Demiryurek, E.O.; Özyürek, T. Color stabilities of calcium silicate–based materials in contact with different irrigation solutions. J. Endod. 2015, 41, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.C.; Walton, R.E.; Rivera, E.M. Sealer Distribution in Coronal Dentin. J. Endod. 2002, 28, 464–466. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Nr | Lead Author | No. of all Tested Teeth, Teeth in Biodentine, Control Groups | Type of Teeth | Control | Tested Materials | Methods | Irrigation | Colour Measuring Method | Measuring Time | Human Eye Perceptible Colour Change |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Madani et al. (2019) | 68, 20 (10 saline, 10 blood), 8 | Single rooted anteriors | 4 teeth saline, 4 teeth blood, restored with composite | MTA-Angelus, CEM cement, Biodentine | Apical portion of the root sectioned, 5 mm of the root remained. Standart access cavities prepared, canals shaped by #1-6 Gates Glidden Drills. End of the root filled with Composite resin. Sponges with blood or normal saline embedded to CEJ. 3 mm of tested cement were placed in the access cavity on the sponges. After 24 h all the cavities sealed with composite resin by 2 mm. Specimens were kept in an incubator at 37 °C and 100% humidity. | 5.25% NaOCl, saline | Spectrophotometer (Vita Easy shade, Germany) | After praparing the cavity (baseline), 1 day, 1, 6 months | ∆E ≥ 3.3 |
| 2 | Adl et al. (2019) | 70, 30 (15 saline, 15 blood), 10 | Single rooted maxillary anteriors and mandibular premolar | 5 teeth saline, 5 teeth blood | MTA-Angelus, Biodentine | Apical portion of the root sectioned, 10 mm from buccal CEJ remained. Canals prepared from apical aspect to pulp chamber roof (closed system). Canals enlarged with #2-6 Gates Glidden drills, last instrument was ParaPost drill size 7 (1,75 mm diameter). Tested materials packed to buccal CEJ. Cotton pallets placed from apical aspect with normal saline or blood. Apical openings sealed with sticky wax. Every specimen was placed into a single vial-containing 1 mL of saline as the | 2.5% NaOCl, 17% EDTA, saline | Spectrophotometer (Spectroshade MHT S.p.A., Verona, Italy) | Before materials placement, 1 week, 1, 3 months | ΔE > 3.7 |
| 3 | Chen et al. (2020) | 100, 20 (10 saline, 10 blood), 20 | Single canal anteriors | 10 positive control with blood clot up to CEJ, 10 negative control with only saline | EndoSequence RRM putty, EndoSequence RRM fast set putty, Biodentine, ProRoot WMTA | Apical portion of the root sectioned, 10 mm apical from buccal CEJ remained. Coronal access prepared, root canals enlarged with Gates Glidden drills #4. Cotton pallet was placed down to the CEJ, the root ends were sealed with composite resin. Canals filled with blood approximately 4 mm below buccal CEJ, the blood was allowed to clot for 15 min. 2 mm collagen plug placed, then 3 mm of tested materials packed. In the groups with no blood, collagen plug 3 mm below CEJ placed, tested materials placed over it. Access cavities sealed with temporary restorative material. Specimens were stored at 37 °C and 100% humidity. | Passive ultrasonic irrigation with 4% NaOCl, 17% EDTA, distilled water | Spectrophotometer (Ocean Optics, Dunedin, FL), A dental microscope (OPMI ProErgo, Carl Zeiss), high-definitioncamera (Nikon D700, Nikkor 105 mm f/2.8GIF-ED; Nikon, Tokyo, Japan) | Baseline (before appliacation of cement) Day 0, 1, 2, 6 months | ∆E > 3.3 |
| 4 | Shokouhinejad et al. (2016) | 104, 24 (12 saline, 12 blood), 8 | Single rooted anteriors | 4 saline, 4 blood | Biodentine, OrthoMTA, EndoSequence Root Repair Material, ProRoot MTA | Apical portion of the root sectioned, 5 mm apical of roots remained. Coronal access cavities prepared. Root canals were cleaned and shaped using #1 to 6 Gates Glidden drills. Customized cylindrical piece of plastic white foam was inserted into the root canal through the apical opening up to CEJ of the labial surface. Apical part sealed with composite resin. The inserted foam was saturated with fresh human blood or normal saline. 3 mm of tested materials placed inside access cavities, temporary restored with Coltosol, incubated at 37 °C in fully saturated humidity for 24 h, later restored with composite resin. | 5.25% NaOCl, 17% EDTA | Konika CS2000 spectroradiometer (Minolta, Osaka, Japan) | Before materials placement, 24 h, 1, 6 months | NM |
| 5 | Palma et al. (2020) | 54, 12 (6 saline, 6 blood), 6 | Premolars | 3 saline, 3 blood | ProRoot MTA, Biodentine, TotalFill BC putty, pulp capping material | Apical portion of the root sectioned, 2 mm apical from CEJ remained. Access cavity was prepared through root-end preparation. Cavities centered on the pulp chamber with 4 mm depth and 2 mm diameter were obtained, ensuring a peripheral minumum of 1 mm enamel and dentin. Cavities were filled with a sterile cotton pellet moistened with saline solution or blood and tested materials inserted into cavities directly over the liquid solutions. All cavities filled with composite resin. Specimens were kept in thedark environment, in an incubator at 37 °C and 100% humidity. | 2.5% NaOCl, 17% EDTA, saline | Canon EOS 5DsR camera, Color assessment was performed ImageJ (National Institutes of Health, NIH) software | Baseline (after cavity preparation), immediately after biomaterial placement and restoration, after 72 h, 7 days, 6 months | ∆E ≥ 3.3 |
| 6 | Al-Hiyasat et al. (2021) | 144, 24, 24 | Maxillary premolars | Nagative with saline and 2 mm composite, positive control with blood and 2 mm composite | GMTA Angelus, ProRoot WMTA, Biodentine, TheraCal, TotalFill | Apical portion of the root sectioned, 1 mm apical from CEJ. Pulp chambers were prepared to a standard size 5 mm depth and leaving 3 mm of buccal thickness. Then 3 mm of tested materials were covered with saline or blood. 2 mm of cavites filled with composite resin. Each tooth was then stored separately in a labelled plastic cuvette in an incubator at 37 °C in 100% humidity in distilled water. | 2.5% NaOCl, normal saline | Spectrophotometer (VITA Easyshade compact; VITA Zahnfabrik, Bad Säckingen, Germany) | Prior material placement, 24 h, 1 week, 1, 3, 6 months | ∆E ≥ 3.7 |
| 7 | Marques Jr. et al. (2021) | 40, 10, 10 | Mandibular premolars | With temporary filling | WMTA Angelus, MTA Repair HP (Angelus), Biodentine | Apical portion of the root sectioned, 7 mm apical from CEJ. A conventional access cavity was prepared and the root canals were shaped by #1-6 Gates Glidden Drills. Root apex was sealed with 2 mm composite resin. Root canals were filled with blood until the CEJ, after 15 min tested materials were placed with a thickness of 3 mm. The access cavity sealed with flowable composite resin. Specimens were stored immersed into distilled water at 37 °C. | 2.5% NaOCl, 17% EDTA, 2.5% NaOCl, distilled water | Sprectrophotometer (VITA Easyshade® Advance 4.0; Vita Zahnfabrik, Bad Sackingen, Germany) | Before cavity preparation, after procedure, 1, 2, 3, 4 months | Perceptibility threshold ΔEab = 1.2, acceptability threshold 2.7 |
| 8 | Keskin et al. (2016) | 60, 20 | Incisors | Baseline | ProRoot wMTA, Biodentine, BioAggregate | Root tips were resected from 3 mm apical level. Root canals were prepared with Gates Glidden drills #2-6, Rely-X Drill size 3 (1.9 mm diameter) until pulp chamber level. Materials compacted to pulp chamber and coronal portion of root canal to a thickness of 4 mm. All materials were compacted with EndoActivator. Cotton pellets were placed into the root canals via apical aspect and was saturated with blood. Apical accesses were sealed with light-cured glass ionomer cement. Specimens were stored in an incubator at 37 °C and 100% humidity. | 5.25% NaOCl, 17% EDTA | Spectrophotometer (VITA Easyshade® compact; VITA Zahnfabrik, Bad Sackingen, Germany), digital camera (Sony Cybershot DSC-W220, Tokyo, Japan) | Before application of materials as baseline, 24 h after, at 30 days | ∆E ≥ 3.3 |
| 9 | Marconyak Jr. et al. (2016) | 90, 15, 15 | Mandibular third molars | Negative control no treatment, ProRoot MTA positive | ProRoot MTA, ProRoot wMTA, EndoSequence Root Repair Material, MTA Angelus, Biodentine | Standart coronal access cavities, buccal enamel dentin chickness 3 mm, materials placed 3 mm thickness above orifice level and allowed to set. A 3 mm thickness of glass ionomer was placed over each material and allowed to set. Access cavities filled with composite, shade matched to the coronal tooth structure. Specimens were stored separately in phosphate buffered saline solution at 37 °C and 100% humidity. | 6% NaOCl | Spectrophotometer (VITA Easy Shade; VITA Zahnfabrik, Germany), digital camera (Nikon D80; Nikon, Tokyo, Japan) | Baseline, after access preparation, after material placement, 1, 7, 30, 60 days | ∆E ≥ 3.3 |
| 10 | Kohli et al. (2015) | 80, 10, 10 | Single canal maxillary anteriors | No filling (negative control) | EndoSequence RRM putty, EndoSequence RRM fast set paste, Biodentine, white MTA, grey MTA, AHPlus sealer, TAP | Apical portion of the root sectioned, 10 mm apical from buccal CEJ remained. Coronal access cavities prepared, root canals were instrumented to a final size 60/04. EndoSequence Ni-Ti rotary files. Moist cotton pellet was placed from access cavity, plugged to the CEJ, entire coronal pulp chamber filled with temporary restorative material. Canals filled with tested material from the apical access, test material did not encroach on the pulp chamber. Tested materials was placed 6 mm length from CEJ to apical extent. Remaining canal sealed with Cavit. Specimens were stored in an incubator in 100% humidity at 37 °C. | Passive ultrasonic irrigation with 3% NaOCl, 17% EDTA, distilled water | Spectrophotometer (Ocean Optics, Dunedin, FL). Photographs were taken using a dental operating microscope (Carl Zeiss OPMI ProErgo) with an internal high definition camera at 7.5 magnification Spectrophotometer (SpectroShade, Handy Dental Type 713000; MHT, Arbizzano di Negar, Verona, Italy) | Day 0 (after tooth prepation, before placement of materials), 7, 1, 2, 6 months | ∆E ≥ 3.7 |
| 11 | Valles et al. (2015) | 35, 16, 3 | Single rooted. Each group: 8 maxillary, 8 mandibular teeth, equal numbers of central, lateral incisors, canines | Composite alone | ProRoot WMTA, Biodentine | Apical portion of root sectioned, 1 mm apical from CEJ of root remained. Retrograde access cavity prepared 2 mm to incisal edge. Tested materials placed into cavities and not sealed. After 48 h sealed with composite. Specimens were kept at room temperature at 100% relative humidity and below a compact fluorescent lamp. | 4.2% NaOCl, saline | Spectrophotometer (SpectroShade, Handy Dental Type 713000; MHT, Arbizzano di Negar, Verona, Italy) | After material placement, 1, 2 weeks, 1, 3, 6 months | NM |
| 12 | Araghi et al. (2019) | 64, 20, 4 | Single rooted. Each group: 8 maxillary, 8 mandibular teeth, equal numbers of central, lateral incisors, canines | No cement after root canal treatment | MTA-Angelus, Biodentine, CEM cement | Standart access cavities prepared. Root canals enlarged with Gates Glidden drills #1-3, hand K-files, Mtwo (VDW, Germany) rotary files, then filled with gutta-percha and AH26 sealer using lateral compaction technique, gutta-percha was cut at the level of orifice. 3 mm of tested cement applied, teeth restored with composite matching teeth color. Specimens were immersed in saline and stored at room temperature under natural lighting. Saline solution was refreshed every 3 days. | Saline, 0.5% NaOCl | Spectrophotometer (Vita EasyShade® compact, VITA Zahnfabrik, Germany) | Baseline (before application of cement), 1 week, 1, 2, 3 months | NM |
| 13 | Nagas et al. (2021) | 64, 20, 4 | Third molars | Negative control no cement, intact teeth | ProRoot MTA, MTA Angelus, NeoMTA, EndoSequence Putty, Biodentine | Coronal endodontic access cavities were made, coronal pulps were removed. Tested material placed 3 mm-thick on the pulp chamber floor. Thin layer of glass ionomer was placed over tested materials. Remaining access cavity was restored with acid-etch composite matching color with coronal tooth stucture. Specimens were stored separately in phosphate buffered saline solution at 37 °C in 100% humidity. | Non | Spectrophotometer (Spectroshade MHT S.P.A., Verona, Italy) and digital images with Canon EOS 650D | Baseline before endodontic access, immediately after placement, | ∆E ≥ 3.3 |
| 14 | Ramos et al. (2016) | 28, 7, 14 | Premolars | 7 negative (dry cotton pallets), 7 positive (fresh blood cotton pallets) | ProRoot MTA, Biodentine | Apical portion of the root sectioned, 2 mm apical from CEJ remained. Pulp tissues extirpated via the cervical cut with Hedstrom files. Access cavities prepared, tested material plugs 2 mm diameter and 5 mm height placed. For control groups cotton pellets, dry or moistened with blood, placed into the cavities. All cavities sealed with glass ionomer cement. specimens were stored in the dark in a 100% humidity at 37 °C with normal atmospheric gas levels. | Non | Colorimeter (PR-650 SpectraScan Colorimeter; PHOTO RESEARCH Inc, Chatsworth, CA, USA) | Baseline (after praparation of the cavities, before application of cement), after cavites sealing, 6, 52 weeks | ∆E ≥ 2.3 |
| Nr | Lead Author | Human Eye Perceptible Color Change | Given Parameter | Group | Before Material Placement, Baseline | After Material Placement | 72 Hours | 1 Week | 2 Weeks | 1 Month | 6 Weeks | 2 Months | 3 Months | 4 Months | 6 Months | 52 Weeks | 24 Months |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Adl et al. (2019) | ∆E > 3.7 | ΔE | Biodentine | V | 2.28 ± 1.62 | 2.38 ± 1.84 | 3.24 ± 2.23 | |||||||||
| Control saline | V | 1.92 ± 1.59 | 3.23 ± 1.76 | 2.90 ± 1.70 | |||||||||||||
| Biodentine | V | 3.20 ± 2.11 | 3.06 ± 2.38 | 4.20 ± 2.89 | |||||||||||||
| Control blood | V | 5.50 ± 4.21 | 6.00 ± 3.97 | 8.32 ± 5.78 | |||||||||||||
| 2 | Chen et al. (2020) | ∆E > 3.3 | ∆E | Biodentine no blood | V | 1.88 ± 1.06 | 1.99 ± 0.90 | 2.09 ± 0.95 | 2.29 ± 0.85 | ||||||||
| Control saline | V | 1.29 ± 0.59 | 1.5 ± 0.42 | 1.7 ± 0.86 | 1.71 ± 0.34 | ||||||||||||
| Biodentine | V | 6.56 ± 2.87 | 6.46 ± 2.72 | 6.15 ± 1.80 | 6.82 ± 2.37 | ||||||||||||
| Control blood | V | 14.3 ± 8.52 | 12.63 ± 10.5 | 11.09 ± 9.25 | 10.25 ± 9.89 | ||||||||||||
| 3 | Palma et al. (2020) | ∆E ≥ 3.3 | ∆E | Biodentine | V | 1.5 ± 0.6 | 1.4 ± 0.0 | 3.4 ± 0.9 | 3.4 ± 0.9 | ||||||||
| Control saline | V | 3.8 ± 2.1 | 2.0 ± 0.0 | 2.2 ± 0.9 | 1.6 ± 0.6 | ||||||||||||
| Biodentine | V | 1.6 ± 1.4 | 2.1 ± 1.0 | 3.8 ± 1.2 | 4.6 ± 1.6 | ||||||||||||
| Control blood | V | 4.4 ± 1.4 | 7.7 ± 4.0 | 6.7 ± 2.8 | 8.0 ± 1.7 | ||||||||||||
| 4 | Al-Hiyasat et al. (2021) | ∆E ≥ 3.7 | ∆E | Biodentine | V | 2.284 ± 1.171 | 2.290 ± 1.05 | 3.014 ± 1.403 | 3.290 ± 1.446 | ||||||||
| Control saline | V | 1.669 ± 0.74 | 1.687 ± 0.685 | 2.339 ± 0.863 | 2.915 ± 0.606 | ||||||||||||
| Biodentine | V | 4.070 ± 1.19 | 4.488 ± 1.38 | 6.013 ± 1.896 | 6.681 ± 2.086 | ||||||||||||
| Control blood | V | 8.041 ± 3.10 | 10.558 ± 2.7 | 11.965 ± 3.607 | 12.834 ± 3.935 | ||||||||||||
| 5 | Marques Jr. et al. | ΔEab = 1.2 | ∆E | Biodentine | V | 3.43 ± 192 | 10.27 ± 4.14 | 11.14 ± 4.2 | 11.98 ± 4.53 | 12.39 ± 4.39 | |||||||
| Control | V | 5.03 ± 3.42 | 3.83 ± 1.43 | 3.32 ± 1.92 | 3.85 ± 1.7 | 3.9 ± 1.82 | |||||||||||
| 6 | Valles et al. (2015) | NM | ∆E | Biodentine | V | 2.78 ± 1.13 | 3.76 ± 1.48 | 4.08 ± 1.75 | 4.19 ± 1.39 | 5.28 ± 2.12 | |||||||
| Control | V | 2.88 ± 0.45 | 3.61 ± 0.89 | 4.49 ± 0.69 | 3.20 ± 0.71 | 6.09 ± 1.15 | |||||||||||
| 7 | Araghi et al. | NM | ∆E | Biodentine | V | 8.03 ± 2.82 | 9.85 ± 3.35 | 10.12 ± 3.98 | 12.97 ± 4.95 | 13.01 ± 5.35 | |||||||
| Control | V | 10.51 ± 2.98 | 11.86 ± 0.73 | 17.01 ± 2.12 | 17.77 ± 1.85 | 17.81 ± 2.21 | |||||||||||
| 8 | Nagas et al. (2021) | ∆E ≥ 3.3 | ∆E S | Biodentine | V | 1.80 ± 0.24 | 1.83 ± 0.46 | 1.89 ± 0.53 | 2.04 ± 0.47 | 2.28 ± 0.32 | |||||||
| Negative | V | 1.34 ± 0.24 | 1.35 ± 0.46 | 1.58 ± 0.32 | 1.61 ± 0.47 | 1.68 ± 0.53 | |||||||||||
| ∆E DC- | Biodentine | V | 5.45 ± 0.93 | 5.66 ± 0.91 | 7.07 ± 1.06 | 7.39 ± 0.96 | 7.40 ± 0.88 | ||||||||||
| Negative | V | 5.54 ± 0.91 | 6.51 ± 0.94 | 7.16 ± 1.06 | 7.17 ± 0.96 | 7.26 ± 0.88 | |||||||||||
| ∆E DC+ | Biodentine | V | 6.35 ± 1.11 | 6.58 ± 1.15 | 6.93 ± 1.26 | 7.08 ± 0.80 | 7.23 ± 0.89 | ||||||||||
| Negative control | V | 6 ± 1.11 | 6.05 ± 1.15 | 7.28 ± 1.26 | 8.23 ± 0.8 | 8.35 ± 0.89 | |||||||||||
| 9 | Ramos et al. (2016) | ∆E ≥ 2.3 | ∆E | Biodentine | V | 1.25 ± 0.80 | 3.72 ± 0.65 | 10.84 ± 1.95 | |||||||||
| Positive | V | 3.41 ± 0.78 | 6.80 ± 1.81 | 14.53 ± 2.11 | |||||||||||||
| Negative | V | 1.14 ± 0.37 | 3.92 ± 0.62 | 11.28 ± 2.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slaboseviciute, M.; Vasiliauskaite, N.; Drukteinis, S.; Martens, L.; Rajasekharan, S. Discoloration Potential of Biodentine: A Systematic Review. Materials 2021, 14, 6861. https://doi.org/10.3390/ma14226861
Slaboseviciute M, Vasiliauskaite N, Drukteinis S, Martens L, Rajasekharan S. Discoloration Potential of Biodentine: A Systematic Review. Materials. 2021; 14(22):6861. https://doi.org/10.3390/ma14226861
Chicago/Turabian StyleSlaboseviciute, Monika, Neringa Vasiliauskaite, Saulius Drukteinis, Luc Martens, and Sivaprakash Rajasekharan. 2021. "Discoloration Potential of Biodentine: A Systematic Review" Materials 14, no. 22: 6861. https://doi.org/10.3390/ma14226861
APA StyleSlaboseviciute, M., Vasiliauskaite, N., Drukteinis, S., Martens, L., & Rajasekharan, S. (2021). Discoloration Potential of Biodentine: A Systematic Review. Materials, 14(22), 6861. https://doi.org/10.3390/ma14226861