Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Enrollment
2.2. Development of a Mathematical Rule for Vertical Implant Position
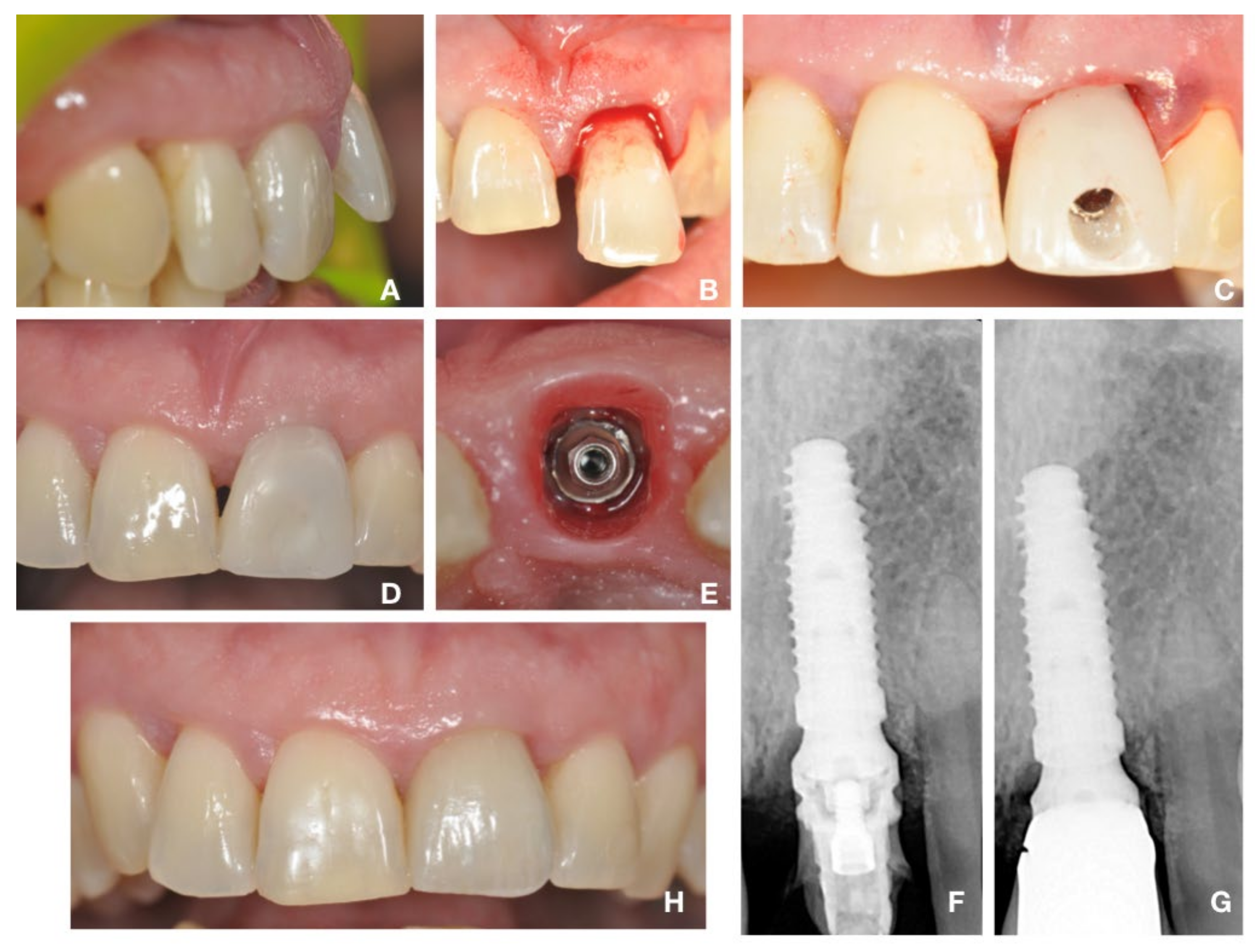
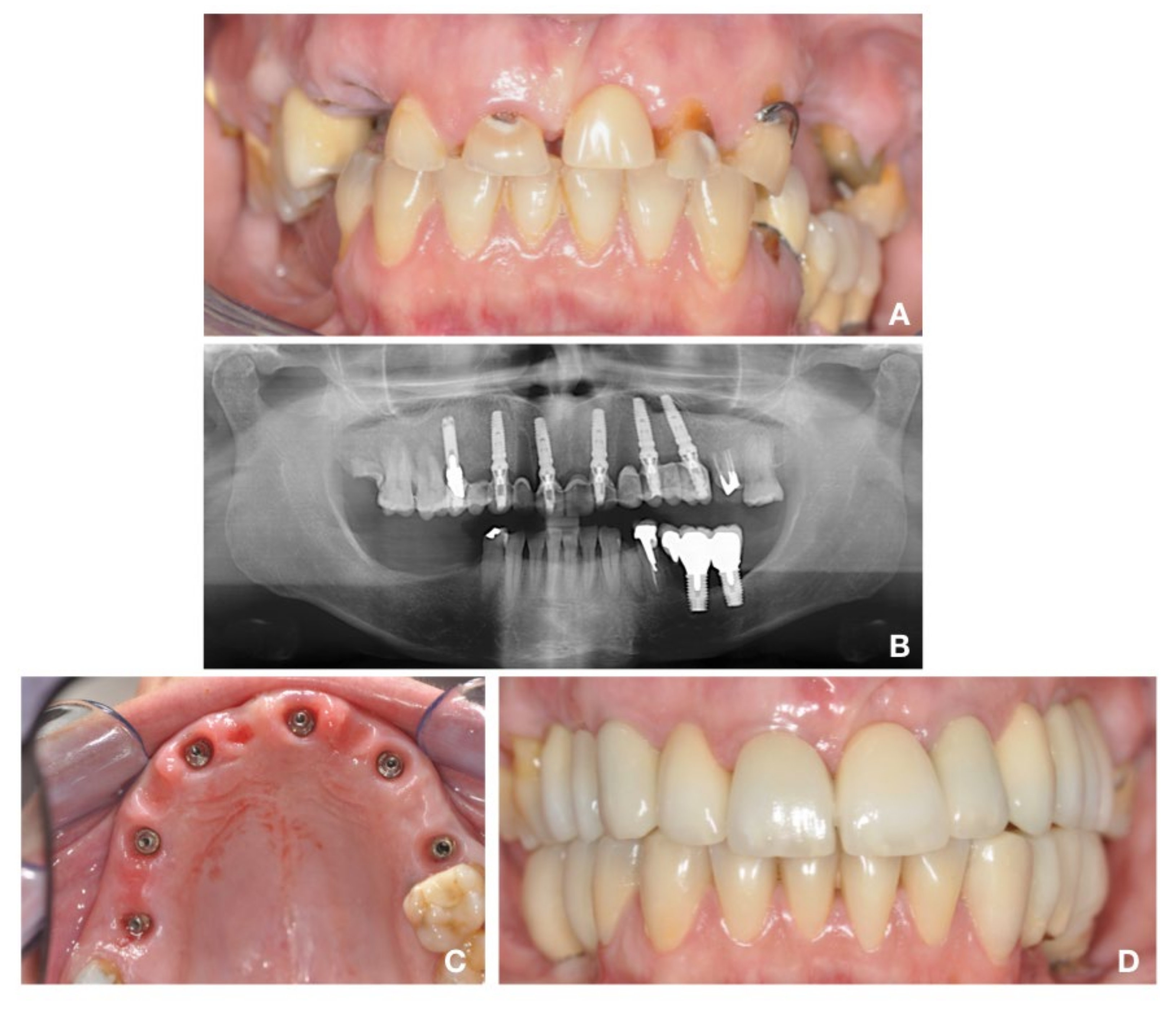
2.3. Surgical Protocol: “Biological Oriented Immediate Loading” (B.O.I.L)
2.4. Prosthetic Protocol
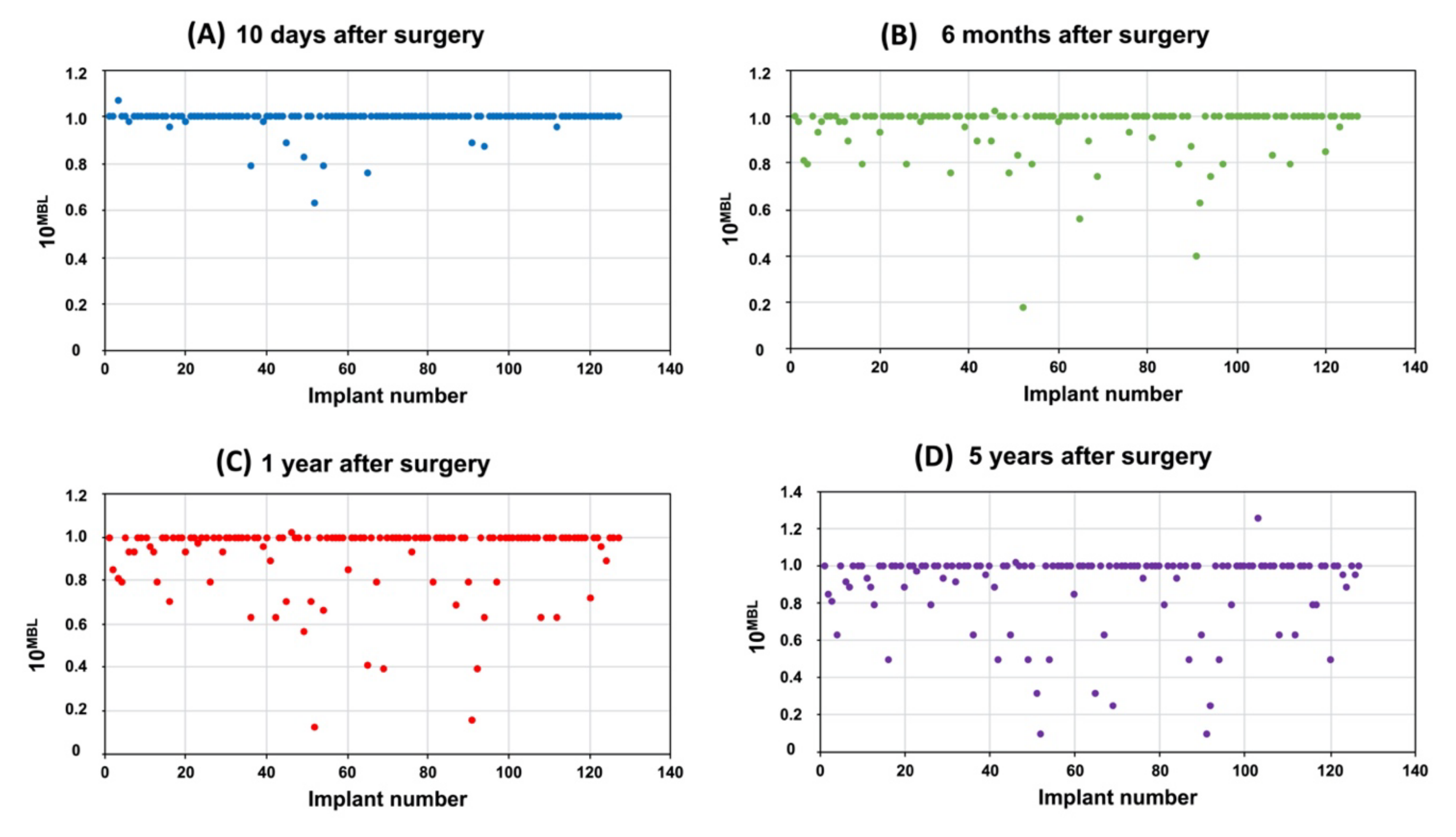
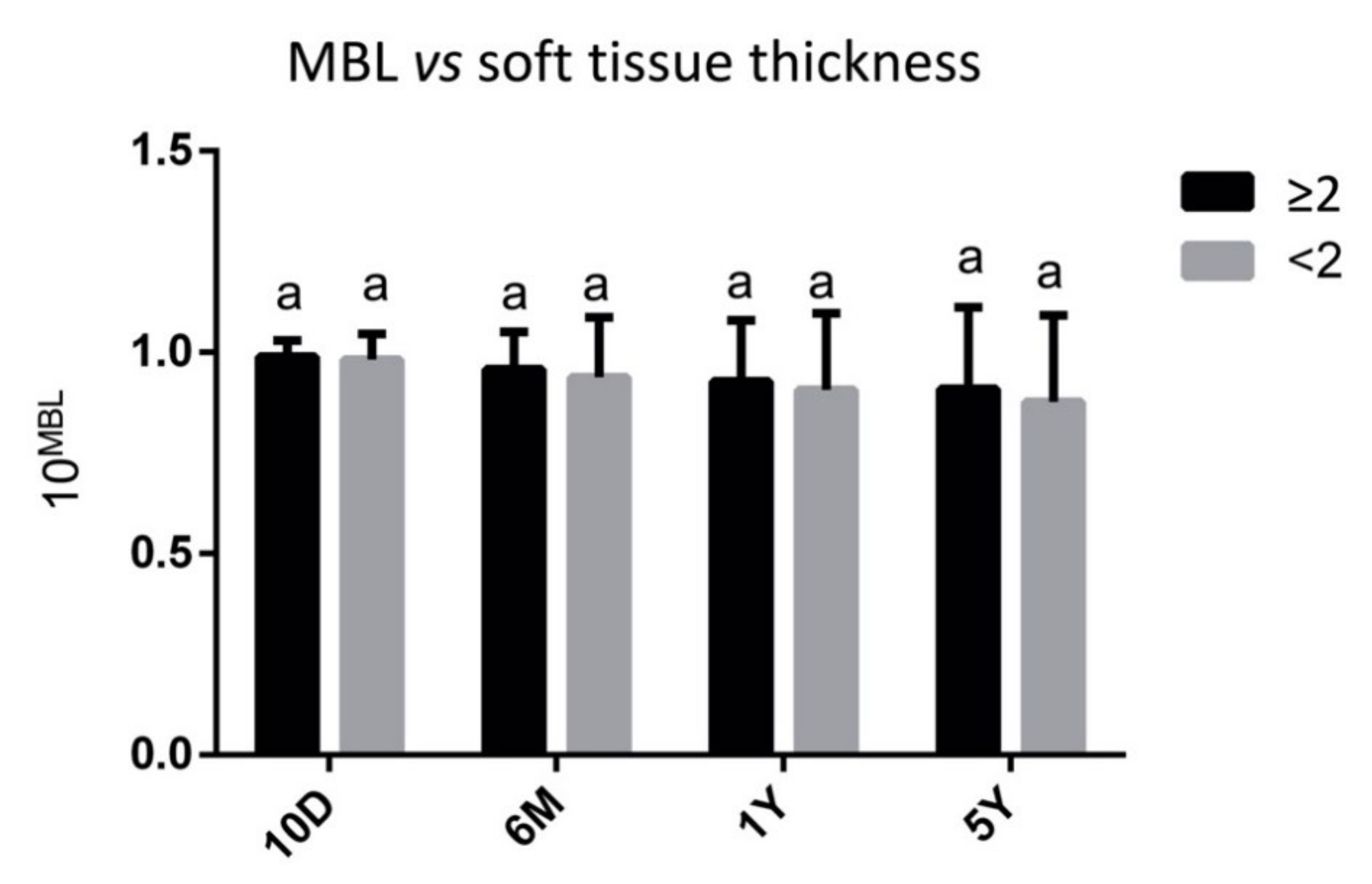
2.5. Radiographic Measurements and Evaluation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tettamanti, L.; Andrisani, C.; Bassi, M.A.; Vinci, R.; Silvestre-Rangil, J.; Tagliabue, A. Immediate Loading Implants: Review of the Critical Aspects. Oral Implantol. 2017, 10, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Schulte, W.; Heimke, G. The Tübinger immediate implant. Quintessenz 1976, 27, 17–23. [Google Scholar] [PubMed]
- Chiapasco, M.; Gatti, C. Implant-Retained Mandibular Overdentures with Immediate Loading: A 3- to 8-Year Prospective Study on 328 Implants. Clin. Implant. Dent. Relat. Res. 2003, 5, 29–38. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for Replacing Missing Teeth: Different Times for Loading Dental Implants. Cochrane Database Syst. Rev. 2013, CD003878. [Google Scholar] [CrossRef]
- Degidi, M.; Piattelli, A.; Iezzi, G.; Carinci, F. Retrospective Study of 200 Immediately Loaded Implants Retaining 50 Mandibular Overdentures. Quintessence Int. 2007, 38, 281–288. [Google Scholar]
- Ragucci, G.M.; Elnayef, B.; Criado-Cámara, E.; Del Amo, F.S.-L.; Hernández-Alfaro, F. Immediate Implant Placement in Molar Extraction Sockets: A Systematic Review and Meta-Analysis. Int. J. Implant. Dent. 2020, 6. [Google Scholar] [CrossRef]
- Ragucci, G.M.; Giralt-Hernando, M.; Méndez-Manjón, I.; Cantó-Navés, O.; Hernández-Alfaro, F. Factors Affecting Implant Failure and Marginal Bone Loss of Implants Placed by Post-Graduate Students: A 1-Year Prospective Cohort Study. Materials 2020, 13, 4511. [Google Scholar] [CrossRef]
- Aslam, A.; Hassan, S.H.; Aslam, H.M.; Khan, D.A. Effect of Platform Switching on Peri-Implant Bone: A 3D Finite Element Analysis. J. Prosthet. Dent. 2019, 121, 935–940. [Google Scholar] [CrossRef]
- Spinato, S.; Stacchi, C.; Lombardi, T.; Bernardello, F.; Messina, M.; Zaffe, D. Biological Width Establishment around Dental Implants Is Influenced by Abutment Height Irrespective of Vertical Mucosal Thickness: A Cluster Randomized Controlled Trial. Clin. Oral Implant. Res. 2019, 30, 649–659. [Google Scholar] [CrossRef]
- De Siqueira, R.A.C.; Gonçalves, R.S., Jr.; Dos Santos, P.G.F.; de Mattias Sartori, I.A.; Wang, H.-L.; Fontão, F.N.G.K. Effect of Different Implant Placement Depths on Crestal Bone Levels and Soft Tissue Behavior: A 5-Year Randomized Clinical Trial. Clin. Oral Implant. Res. 2020, 31, 282–293. [Google Scholar] [CrossRef]
- Van Eekeren, P.; van Elsas, P.; Tahmaseb, A.; Wismeijer, D. The Influence of Initial Mucosal Thickness on Crestal Bone Change in Similar Macrogeometrical Implants: A Prospective Randomized Clinical Trial. Clin. Oral Implant. Res. 2017, 28, 214–218. [Google Scholar] [CrossRef]
- Vervaeke, S.; Matthys, C.; Nassar, R.; Christiaens, V.; Cosyn, J.; De Bruyn, H. Adapting the Vertical Position of Implants with a Conical Connection in Relation to Soft Tissue Thickness Prevents Early Implant Surface Exposure: A 2-Year Prospective Intra-Subject Comparison. J. Clin. Periodontol. 2018, 45, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Perussolo, J.; Souza, A.B.; Matarazzo, F.; Oliveira, R.P.; Araújo, M.G. Influence of the Keratinized Mucosa on the Stability of Peri-Implant Tissues and Brushing Discomfort: A 4-Year Follow-up Study. Clin. Oral Implant. Res. 2018, 29, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Cochran, D.L.; Nummikoski, P.V.; Schoolfield, J.D.; Jones, A.A.; Oates, T.W. A Prospective Multicenter 5-Year Radiographic Evaluation of Crestal Bone Levels over Time in 596 Dental Implants Placed in 192 Patients. J. Periodontol. 2009, 80, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J. Dimension of the Periimplant Mucosa. Biological Width Revisited. J. Clin. Periodontol. 1996, 23, 971–973. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Toti, P.; Quaranta, A.; Derchi, G.; Covani, U. The Clinical Outcomes of Immediate Versus Delayed Restoration Procedures on Immediate Implants: A Comparative Cohort Study for Single-Tooth Replacement. Clin. Implant. Dent. Relat. Res. 2015, 17, 1114–1126. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Toti, P.; Piattelli, A.; Iezzi, G.; Derchi, G.; Covani, U. Extraction Socket Healing in Humans after Ridge Preservation Techniques: Comparison between Flapless and Flapped Procedures in a Randomized Clinical Trial. J. Periodontol. 2014, 85, 14–23. [Google Scholar] [CrossRef]
- Cochran, D.L.; Hermann, J.S.; Schenk, R.K.; Higginbottom, F.L.; Buser, D. Biologic Width around Titanium Implants. A Histometric Analysis of the Implanto-Gingival Junction around Unloaded and Loaded Nonsubmerged Implants in the Canine Mandible. J. Periodontol. 1997, 68, 186–198. [Google Scholar] [CrossRef]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. The Influence of Soft Tissue Thickness on Crestal Bone Changes around Implants: A 1-Year Prospective Controlled Clinical Trial. Int. J. Oral Maxillofac. Implants 2009, 24, 712–719. [Google Scholar]
- Suárez-López Del Amo, F.; Lin, G.-H.; Monje, A.; Galindo-Moreno, P.; Wang, H.-L. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. Influence of Thin Mucosal Tissues on Crestal Bone Stability around Implants with Platform Switching: A 1-Year Pilot Study. J. Oral Maxillofac. Surg. 2010, 68, 2272–2277. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, S.; Dierens, M.; Besseler, J.; De Bruyn, H. The Influence of Initial Soft Tissue Thickness on Peri-Implant Bone Remodeling. Clin. Implant. Dent. Relat. Res. 2014, 16, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, H.; Kawahara, D.; Hashimoto, K.; Takashima, Y.; Ong, J.L. Morphologic Studies on the Biologic Seal of Titanium Dental Implants. Report I. In Vitro Study on the Epithelialization Mechanism around the Dental Implant. Int. J. Oral Maxillofac. Implants 1998, 13, 457–464. [Google Scholar]
- Kawahara, H.; Kawahara, D.; Mimura, Y.; Takashima, Y.; Ong, J.L. Morphologic Studies on the Biologic Seal of Titanium Dental Implants. Report II. In Vivo Study on the Defending Mechanism of Epithelial Adhesions/Attachment against Invasive Factors. Int. J. Oral Maxillofac. Implants 1998, 13, 465–473. [Google Scholar]
- Rompen, E. The Impact of the Type and Configuration of Abutments and Their (Repeated) Removal on the Attachment Level and Marginal Bone. Eur. J. Oral Implantol. 2012, 5, S83–S90. [Google Scholar]
- Briguglio, F.; Falcomatà, D.; Marconcini, S.; Fiorillo, L.; Briguglio, R.; Farronato, D. The Use of Titanium Mesh in Guided Bone Regeneration: A Systematic Review. Int. J. Dent. 2019, 2019, 9065423. [Google Scholar] [CrossRef]
- Lang, N.P.; Berglundh, T.; Heitz-Mayfield, L.J.; Pjetursson, B.E.; Salvi, G.E.; Sanz, M. Consensus Statements and Recommended Clinical Procedures Regarding Implant Survival and Complications. Int. J. Oral Maxillofac. Implants 2004, 19, 150–154. [Google Scholar]
- Linkevicius, T.; Apse, P. Influence of Abutment Material on Stability of Peri-Implant Tissues: A Systematic Review. Int. J. Oral Maxillofac. Implants 2008, 23, 449–456. [Google Scholar]
- Lauer, G.; Wiedmann-Al-Ahmad, M.; Otten, J.E.; Hübner, U.; Schmelzeisen, R.; Schilli, W. The Titanium Surface Texture Effects Adherence and Growth of Human Gingival Keratinocytes and Human Maxillar Osteoblast-like Cells in Vitro. Biomaterials 2001, 22, 2799–2809. [Google Scholar] [CrossRef]
- Carinci, F.; Lauritano, D.; Cura, F.; Lopez, M.A.; Andreasi Bassi, M.; Confalone, L.; Pezzetti, F. Prevention of Bacterial Leakage at Implant-Abutment Connection Level: An in Vitro Study of the Efficacy of Three Different Implant Systems. J. Biol. Regul. Homeost. Agents 2016, 30, 69–73. [Google Scholar]
- Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials 2019, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Libonati, A.; Nardi, R.; Gallusi, G.; Angotti, V.; Caruso, S.; Coniglione, F.; Marzo, G.; Mattei, A.; Tecco, S.; Paglia, L. Pain and Anxiety Associated with Computer-Controlled Local Anaesthesia: Systematic Review and Meta-Analysis of Cross-over Studies. Eur. J. Paediatr. Dent. 2018, 19, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.-J.; Chuang, S.-K.; Weber, H.-P. Implant Loading Protocols for Edentulous Patients with Fixed Prostheses: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2014, 29, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Bambini, F.; Memè, L.; Pellecchia, M.; Sabatucci, A.; Selvaggio, R. Comparative Analysis of Deformation of Two Implant/Abutment Connection Systems during Implant Insertion. An in Vitro Study. Minerva Stomatol. 2005, 54, 129–138. [Google Scholar] [PubMed]
- Marchetti, E.; Ratta, S.; Mummolo, S.; Tecco, S.; Pecci, R.; Bedini, R.; Marzo, G. Evaluation of an Endosseous Oral Implant System According to UNI EN ISO 14801 Fatigue Test Protocol. Implant. Dent. 2014, 23, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha, M.; Palomar, M.; Sanchis, J.M.; Guarinos, J.; Balaguer, J. Radiologic Study of Marginal Bone Loss around 108 Dental Implants and Its Relationship to Smoking, Implant Location, and Morphology. Int. J. Oral Maxillofac. Implants 2004, 19, 861–867. [Google Scholar]
- Wennerberg, A.; Sennerby, L.; Kultje, C.; Lekholm, U. Some Soft Tissue Characteristics at Implant Abutments with Different Surface Topography. A Study in Humans. J. Clin. Periodontol. 2003, 30, 88–94. [Google Scholar] [CrossRef]
- Barros, R.R.M.; Novaes, A.B.; Muglia, V.A.; Iezzi, G.; Piattelli, A. Influence of Interimplant Distances and Placement Depth on Peri-Implant Bone Remodeling of Adjacent and Immediately Loaded Morse Cone Connection Implants: A Histomorphometric Study in Dogs. Clin. Oral Implant. Res. 2010, 21, 371–378. [Google Scholar] [CrossRef]
- Pellicer-Chover, H.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D.; Gomar-Vercher, S.; Agustín-Panadero, R.; Peñarrocha-Diago, M. Impact of Crestal and Subcrestal Implant Placement in Peri-Implant Bone: A Prospective Comparative Study. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e103–e110. [Google Scholar] [CrossRef]
- Do Nascimento, C.; Miani, P.K.; Pedrazzi, V.; Muller, K.; de Albuquerque, R.F. Bacterial Leakage along the Implant-Abutment Interface: Culture and DNA Checkerboard Hybridization Analyses. Clin. Oral Implant. Res. 2012, 23, 1168–1172. [Google Scholar] [CrossRef]
- Dibart, S.; Warbington, M.; Su, M.; Skobe, Z. In Vitro Evaluation of the Implant-Abutment Bacterial Seal: The Locking Taper System. Int. J. Oral Maxillofac. Implants 2005, 20, 732–737. [Google Scholar]
- De Siqueira, R.A.C.; Fontão, F.N.G.K.; Sartori, I.A.d.M.; Santos, P.G.F.; Bernardes, S.R.; Tiossi, R. Effect of Different Implant Placement Depths on Crestal Bone Levels and Soft Tissue Behavior: A Randomized Clinical Trial. Clin. Oral Implant. Res. 2017, 28, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Puisys, A.; Steigmann, M.; Vindasiute, E.; Linkeviciene, L. Influence of Vertical Soft Tissue Thickness on Crestal Bone Changes Around Implants with Platform Switching: A Comparative Clinical Study. Clin. Implant. Dent. Relat. Res. 2015, 17, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Akcalı, A.; Trullenque-Eriksson, A.; Sun, C.; Petrie, A.; Nibali, L.; Donos, N. What Is the Effect of Soft Tissue Thickness on Crestal Bone Loss around Dental Implants? A Systematic Review. Clin. Oral Implant. Res. 2017, 28, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Gobbato, L.; Avila-Ortiz, G.; Sohrabi, K.; Wang, C.-W.; Karimbux, N. The Effect of Keratinized Mucosa Width on Peri-Implant Health: A Systematic Review. Int. J. Oral Maxillofac. Implants 2013, 28, 1536–1545. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-H.; Chan, H.-L.; Wang, H.-L. The Significance of Keratinized Mucosa on Implant Health: A Systematic Review. J. Periodontol. 2013, 84, 1755–1767. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Mummolo, S.; Tecco, S.; Continenza, M.A.; Marzo, G. Caracterización Histológica de La Membrana de Los Factores de Crecimiento Concentrados Sacco. Int. J. Morphol. 2017, 35, 114–119. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The Long-Term Efficacy of Currently Used Dental Implants: A Review and Proposed Criteria of Success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar]
- French, D.; Cochran, D.L.; Ofec, R. Retrospective Cohort Study of 4,591 Straumann Implants Placed in 2,060 Patients in Private Practice with up to 10-Year Follow-up: The Relationship Between Crestal Bone Level and Soft Tissue Condition. Int. J. Oral Maxillofac. Implants 2016, 31, e168–e178. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Nardi, D.; Piattelli, A. Immediate Provisionalization of Implants Placed in Fresh Extraction Sockets Using a Definitive Abutment: The Chamber Concept. Int. J. Periodont. Restor. Dent. 2013, 33, 559–565. [Google Scholar] [CrossRef]
- D’Ercole, S.; Tripodi, D.; Marzo, G.; Bernardi, S.; Continenza, M.A.; Piattelli, A.; Iaculli, F.; Mummolo, S. Microleakage of Bacteria in Different Implant-Abutment Assemblies: An in Vitro Study. J. Appl. Biomater. Funct. Mater. 2015, 13, e174–e180. [Google Scholar] [CrossRef] [PubMed]
- Lauritano, D.; Moreo, G.; Lucchese, A.; Viganoni, C.; Limongelli, L.; Carinci, F. The Impact of Implant–Abutment Connection on Clinical Outcomes and Microbial Colonization: A Narrative Review. Materials 2020, 13, 1131. [Google Scholar] [CrossRef] [PubMed]
- Sasada, Y.; Cochran, D.L. Implant-Abutment Connections: A Review of Biologic Consequences and Peri-Implantitis Implications. Int. J. Oral Maxillofac. Implants 2017, 32, 1296–1307. [Google Scholar] [CrossRef] [PubMed]
- King, G.N.; Hermann, J.S.; Schoolfield, J.D.; Buser, D.; Cochran, D.L. Influence of the Size of the Microgap on Crestal Bone Levels in Non-Submerged Dental Implants: A Radiographic Study in the Canine Mandible. J. Periodontol. 2002, 73, 1111–1117. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bambini, F.; Orilisi, G.; Quaranta, A.; Memè, L. Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study. Materials 2021, 14, 387. https://doi.org/10.3390/ma14020387
Bambini F, Orilisi G, Quaranta A, Memè L. Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study. Materials. 2021; 14(2):387. https://doi.org/10.3390/ma14020387
Chicago/Turabian StyleBambini, Fabrizio, Giulia Orilisi, Alessandro Quaranta, and Lucia Memè. 2021. "Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study" Materials 14, no. 2: 387. https://doi.org/10.3390/ma14020387
APA StyleBambini, F., Orilisi, G., Quaranta, A., & Memè, L. (2021). Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study. Materials, 14(2), 387. https://doi.org/10.3390/ma14020387