
Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
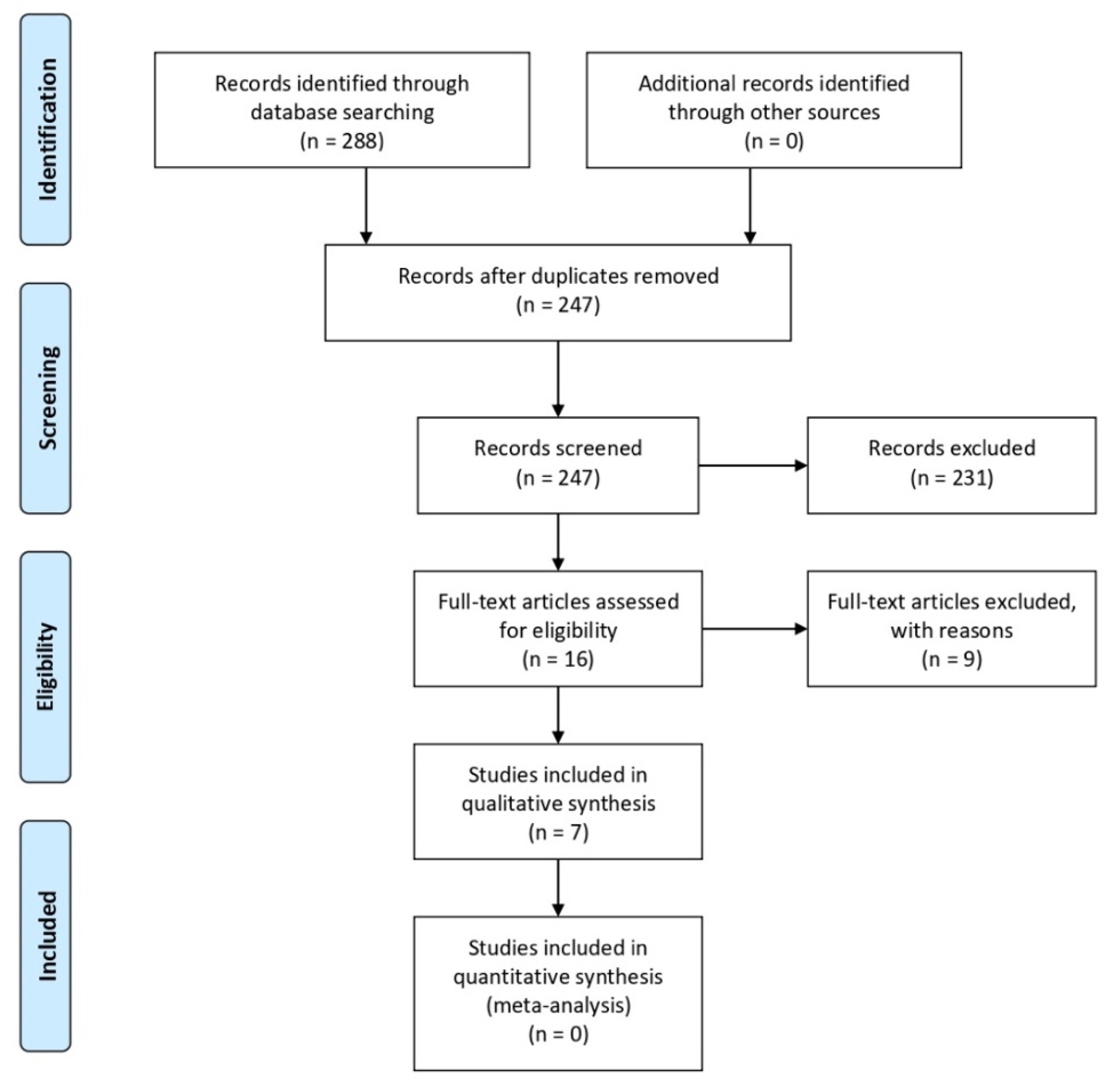
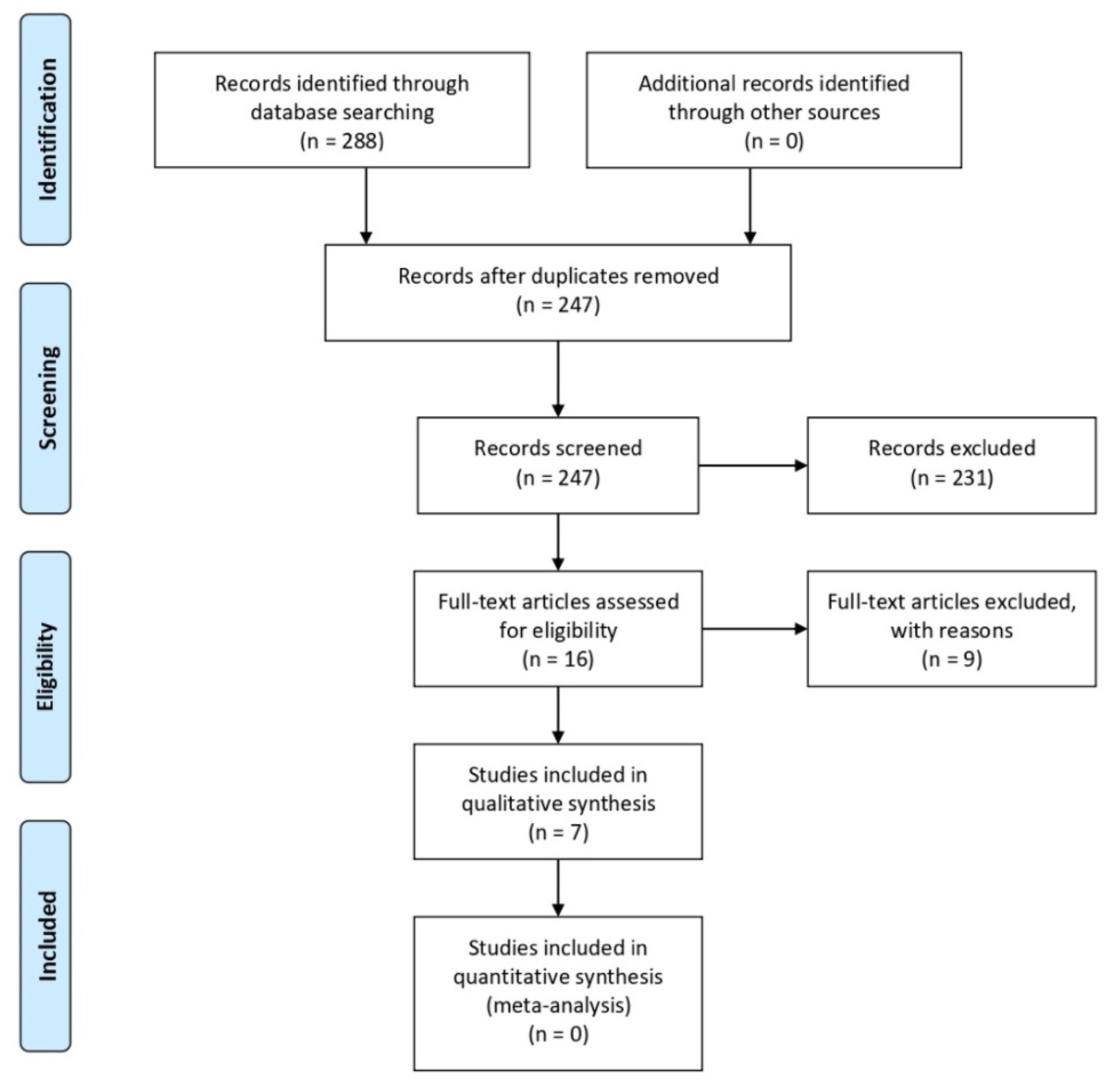
2.1. Search Strategy
2.2. Selection Criteria
3. Results
3.1. Implant Systems
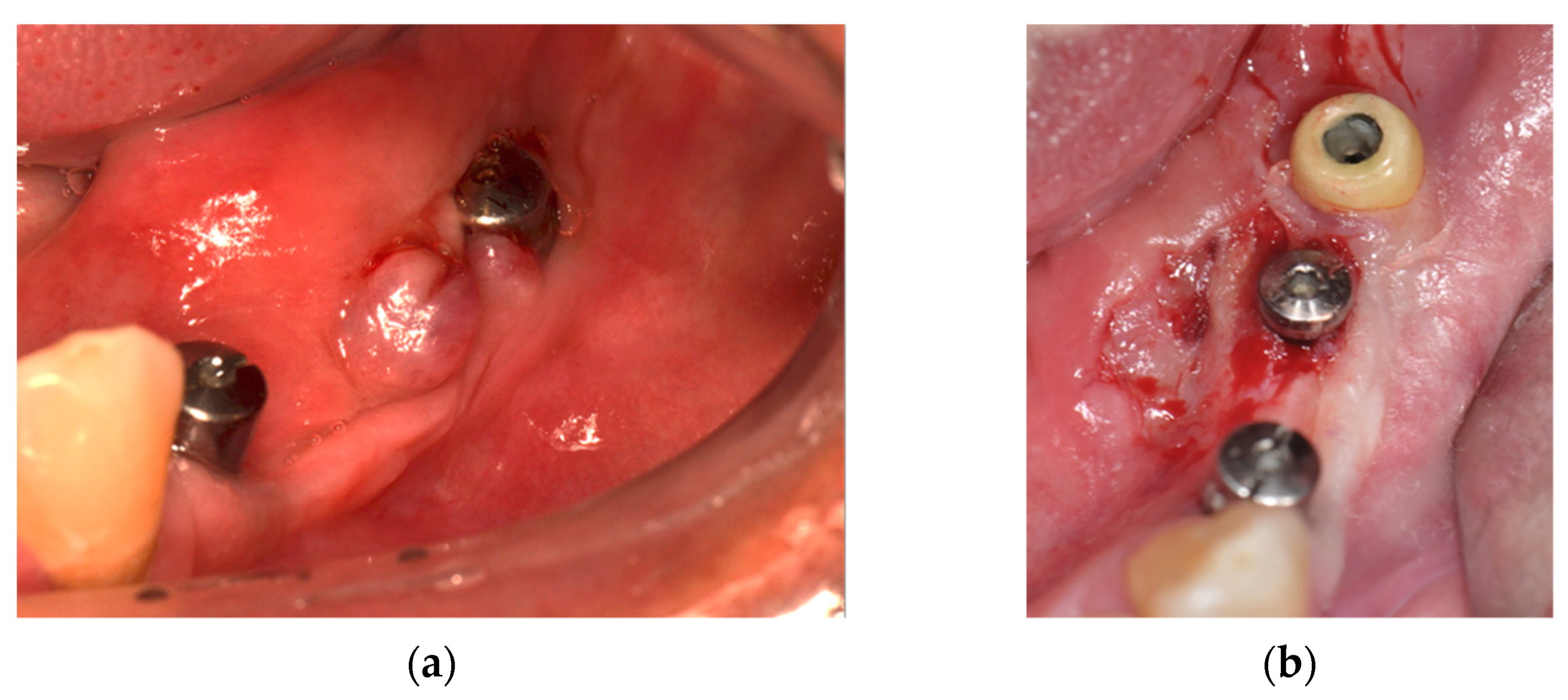
3.2. Clinical Manifestations
3.3. Imaging Tests
3.4. Medications
3.5. Treatment
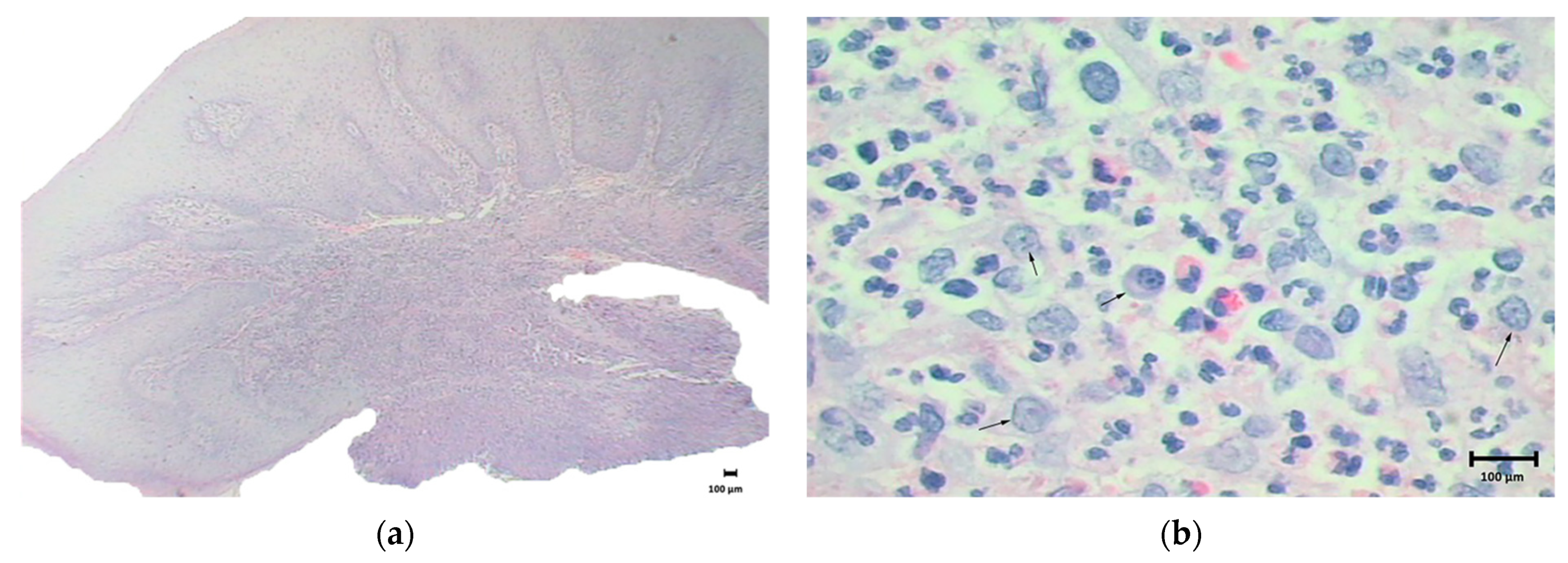
3.6. Histopathological Analysis
3.7. Additional Tests
3.8. Case Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osseointegration. Eur. Spine J. 2001, 10 (Suppl. 2), S96–S101. [Google Scholar] [CrossRef] [Green Version]
- Lyapina, M.; Cekova, M.; Deliverska, M.; Galabov, J.; Kisselova, A. Immunotoxicological aspects of biocompatibility of titanium. J. IMAB Annu. Proc. (Sci. Pap.) 2017, 23, 1550–1558. [Google Scholar] [CrossRef]
- Comino-Garayoa, R.; Cortés-Bretón Brinkmann, J.; Peláez, J.; López-Suárez, C.; Martínez-González, J.M.; Suárez, M.J. Allergies to titanium dental implants: What do we really know about them? A scoping review. Biology 2020, 9, 404. [Google Scholar] [CrossRef] [PubMed]
- Zigante, M.; Peternel, S.; Muhvic Urek, M.; Rincic Mlinaric, M.; Pop Acev, D.; Spalj, S. Smell and taste in titanium and nickel allergic sensitization in orthodontic patients. Orthod. Craniofacial Res. 2020, 23, 517–522. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Mascellaro, A.; Ferrario, S.; Beretta, M. Dental implants placed in resorbed alveolar ridges reconstructed with iliac crest autogenous onlay grafts: A 26-year median follow-up retrospective study. J. Craniomaxillofac. Surg. 2019, 47, 805–814. [Google Scholar] [CrossRef]
- Lini, F.; Poli, P.P.; Beretta, M.; Cortinovis, I.; Maiorana, C. Long-term retrospective observational cohort study on the survival rate of stepped screw titanium implants followed up to 20 years. Int. J. Oral Maxillofac. Implant. 2019, 34, 999–1006. [Google Scholar] [CrossRef]
- Pacheco, K.A. Allergy to Surgical Implants. Clin. Rev. Allergy Immunol. 2019, 56, 72–85. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Amini, F.; Shariati, M.; Sobouti, F.; Rakhshan, V. Effects of fixed orthodontic treatment on nickel and chromium levels in gingival crevicular fluid as a novel systemic biomarker of trace elements: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 666–672. [Google Scholar] [CrossRef]
- Bass, J.K.; Fine, H.; Cisneros, G.J. Nickel hypersensitivity in the orthodontic patient. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 280–285. [Google Scholar] [CrossRef]
- Olms, C.; Yahiaoui-Doktor, M.; Remmerbach, T.W. Contact allergies to dental materials. Swiss Dent. J. 2019, 129, 571–579. [Google Scholar] [PubMed]
- Razzante, M.C.; Ehredt, D.J.; Clougherty, C.O.; Kriger, S.J.; Menninger, B.A.; Behan Dionisopoulos, S.; Bhakta, P.J.; Bruning, N.G. Type IV Cell-Mediated Hypersensitivity Reaction Caused by Titanium Implant Following Double Calcaneal Osteotomy and First Metatarsal-Cuneiform Arthrodesis: A Case Report and Review of the Literature. J. Foot. Ankle Surg. 2019, 58, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Furrer, S.; Scherer Hofmeier, K.; Grize, L.; Bircher, A.J. Metal hypersensitivity in patients with orthopaedic implant complications-A retrospective clinical study. Contact Dermat. 2018, 79, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Viraben, R.; Boulinguez, S.; Alba, C. Granulomatous dermatitis after implantation of a titanium-containing pacemaker. Contact Dermat. 1995, 33, 437. [Google Scholar] [CrossRef]
- Abdallah, H.I.; Balsara, R.K.; O’Riordan, A.C. Pacemaker contact sensitivity: Clinical recognition and management. Ann. Thorac. Surg. 1994, 57, 1017–1018. [Google Scholar] [CrossRef]
- Al-Shamiri, H.M.; Alaizari, N.A.; Al-Maweri, S.A.; Tarakji, B. Development of pyogenic granuloma and hemangioma after placement of dental implants: A review of literature. J. Int. Soc. Prev. Community Dent. 2015, 5, 77–80. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, T. Allergy related to dental implant and its clinical significance. Clin. Cosmet. Investig. Dent. 2013, 5, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- du Preez, L.A.; Bütow, K.W.; Swart, T.J. Implant failure due to titanium hypersensitivity/allergy?—Report of a case. SADJ J. S. Afr. Dent. Assoc. Tydskr. Die Suid-Afrik. Tandheelkd. Ver. 2007, 62, 24–25. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Khan, L.K.; Kunz, R.; Kleijnen, J.; Antes, G. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Health care Research; Royal Society of Medicine Press: London, UK, 2003; p. 136. [Google Scholar]
- Suito, H.; Iwawaki, Y.; Goto, T.; Tomotake, Y.; Ichikawa, T. Oral factors affecting titanium elution and corrosion: An in vitro study using simulated body fluid. PLoS ONE 2013, 8, e66052. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Payne, A.G.; De Silva, R.K.; Duncan, W.J. Titanium allergy: Could it affect dental implant integration? Clin. Oral Implants Res. 2011, 22, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Sicilia, A.; Cuesta, S.; Coma, G.; Arregui, I.; Guisasola, C.; Ruiz, E.; Maestro, A. Titanium allergy in dental implant patients: A clinical study on 1500 consecutive patients. Clin. Oral Implants Res. 2008, 19, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Osman, R.B.; Swain, M.V.; Atieh, M.; Ma, S.; Duncan, W. Ceramic implants (Y-TZP): Are they a viable alternative to titanium implants for the support of overdentures? A randomized clinical trial. Clin. Oral Implants Res. 2014, 25, 1366–1377. [Google Scholar] [CrossRef]
- Müller, K.; Valentine-Thon, E. Hypersensitivity to titanium: Clinical and laboratory evidence. Neuroendocrinol. Lett. 2006, 27, 31–35. [Google Scholar] [PubMed]
- Marino, R.; Capaccio, P.; Pignataro, L.; Spadari, F. Burning mouth syndrome: The role of contact hypersensitivity. Oral Dis. 2009, 15, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P.; Iglhaut, G.; Wollenberg, A.; Cadosch, D.; Summer, B. Allergy or Tolerance: Reduced Inflammatory Cytokine Response and Concomitant IL-10 Production of Lymphocytes and Monocytes in Symptom-Free Titanium Dental Implant Patients. BioMed Res. Int. 2013, 2013, 539834. [Google Scholar] [CrossRef] [Green Version]
- Doyle, E.; Mavrikakis, I.; Lee, E.J.; Emerson, R.; Rainey, A.J.; Brittain, G.P. Type IV hypersensitivity reactions to upper lid gold weight implants-is patch testing necessary? Orbit 2005, 24, 205–210. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Paparella, M.L.; Brandizzi, D.; Cabrini, R.L. Reactive lesions of peri-implant mucosa associated with titanium dental implants: A report of 2 cases. Int. J. Oral Maxillofac. Surg. 2010, 39, 503–507. [Google Scholar] [CrossRef]
- Yan, H.; Afroz, S.; Dalanon, J.; Goto, N.; Hosoki, M.; Matsuka, Y. Metal allergy patient treated by titanium implant denture: A case report with at least 4-year follow-up. Clin. Case Rep. 2018, 6, 1972–1977. [Google Scholar] [CrossRef]
- de Graaf, N.P.J.; Feilzer, A.J.; Kleverlaan, C.J.; Bontkes, H.; Gibbs, S.; Rustemeyer, T. A retrospective study on titanium sensitivity: Patch test materials and manifestations. Contact Dermat. 2018, 79, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Hosoki, M.; Nishigawa, K.; Tajima, T.; Ueda, M.; Matsuka, Y. Cross-sectional observational study exploring clinical risk of titanium allergy caused by dental implants. J. Prosthodont. Res. 2018, 62, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Hosoki, M.; Nishigawa, K.; Miyamoto, Y.; Ohe, G.; Matsuka, Y. Allergic contact dermatitis caused by titanium screws and dental implants. J. Prosthodont. Res. 2016, 60, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Savio, M.; Re, D. A Possible Relationship between Peri-Implantitis, Titanium Hypersensitivity, and External Tooth Resorption: Metal-Free Alternative to Titanium Implants. Case Rep. Dent. 2021, 2021, 8879988. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Type | Sample Size | Mean Age (Years) | Sex | Total Implants | Position | Implant Data |
|---|---|---|---|---|---|---|---|
| Borgonovo et al. [34] | Case report | 1 | 56 | Female | 4 | Mandible | Implants in the region of mandibular teeth (right canine up to first molar) |
| du Preez et al. [18] | Case report | 1 | 49 | Female | 6 | Mandible | GMI, LIBB, IBS, (Southern Implants) |
| Olmedo et al. [29] | Case report | 2 | 69.5 | Females | 3 | Case 1: mandible | Case 1: Titantec 4.1 mm × 10 mm |
| Case 2: maxilla | Case 2: two implants in the region of elements 22 and 23; 4.1 mm × 11.5 mm (unknown brand) | ||||||
| Sicilia et al. [23] | Case series | Test: 35 | Test: 50.2 | Test: 10 males; 25 females | |||
| Control: 35 | Control: 47.69 | Control: 16 males; 18 females | |||||
| Muller et al. [25] | Clinical and laboratory study | 56 | 53.8 | 17 males; 39 females | |||
| Hosoki et al. [33] | Case report | 1 | 69 | Male | 2 | Right lower molars | Fixture MicroThread system, Astra Tech |
| Hosoki et al. [32] | Clinical study | 270 | 53.9 | 61 males; 209 females |
| Author | Clinical Features | Imaging Features | Medications | Treatment | Histopathology | Other Tests | Results |
|---|---|---|---|---|---|---|---|
| Borgonovo et al. [34] | Swelling and redness in peri-implant tissues and bleeding and a probing depth of 6 mm, bucally and 5 mm lingually, high mucosa sensitivity and implant exposure. | a bony defect with a crater-like shape around first molar implant and cervical decay on teeth and vertical bone loss involved the new implants and the process of external resorption affected the teeth up to the canine | Removal of the titanium implant, after nine months, when allergic symptoms disappeared, five one-piece zirconia implants were inserted, four in the anterior jaw and 1 in the right molar region | Biopsy was performed by taking a sample of cortical and medullary bone to check for bone disorder. the result did not show any kind of bone lesion or disease. | A standard blood tests revealed an increased number of eosinophils. MELISA (Memory Lymphocyte Immunostimulation Assay) test was performed and confirmed titanium hypersensitivity. The bacterial culture was negative. | During the follow-up period, the patient did not refer to any symptoms of peri-implantitis or other problems, and after 18 months from surgery, the clinical-radiographic exams showed the success of the metal-free implant prosthetic rehabilitation. | |
| du Preez et al. [18] | Swelling in peri-implant tissues, swelling in the submental region and lip crease, pain, hyperaemia in peri-implant tissues (no pus and no necrosis) | irregular radiolucent areas at the apex and sides of the implants | Postoperative: Amoxicillin 500 mg 8/8 h and ibuprofen 400 mg 8/8 h; After clinical manifestations: Metronidazole 400 mg | Implant removal, debridement and peri-implant biopsy | 8 samples revealed foci of subacute inflammation, moderate chronic inflammation, lymphocytes, plasma cells, concomitant fibrosis histiocytes; 7 samples revealed granulation tissue and giant cells. | None | Type IV (late) hypersensitivity diagnosis, evidence of a true allergy or hypersensitivity to dental implants |
| Olmedo et al. [29] | Case 1: two postoperative months, lesion measuring 1 × 1 × 0.6 cm, smooth and bright red surface and bleeding on palpation | Case 1: no bone loss | chlorhexidine 2% postoperatively | Case 1: surgical removal of the lesion and curettage, implant was maintained (biopsy) | Case 1: intense vascular proliferation, mixed inflammatory infiltrate and abundant macrophages. Numerous metal-like particles have been identified, including within macrophages, perivascular region | Identification of metals by emission spectroscopy: did not identify titanium due to small sample | Case 1: pyogenic granuloma diagnosis and 4-year-old patient with no recurrence |
| Case 2: distal vestibular sessile lesion around implant 22 measuring 0.6 × 0.5 × 0.4 cm, red and irregular | Case 2: cup-shaded bone loss | Case 2: surgical removal and buccal bone curettage | Case 2: proliferation of fusiform and round mesenchymal cells, intense vascularization, and numerous multinucleated giant cells. Isolated metal particles | Case 2: Diagnosis of peripheral giant cell granuloma, 2-year-old control patient without injury | |||
| Sicilia et al. [23] | 16 individuals had clinical symptoms and/or implant loss. 19 individuals had a history of other allergies or predisposing factors for implant failure | Skin tests (type I hypersensitivity); Epicutaneous tests (type IV hypersensitivity) | 25.7% tested positive for titanium allergy in the test group. (positive for skin test or epicutaneous test). In the control group, 100% tested negative. | ||||
| Muller et al. [25] | Test MELISA® and patch test | It was not specific to the dental implant group. Test patch was negative for Ti in all cases; MELISA® test was positive for Ti in 37.5% cases, and 21.4% cases showed reaction to Ni. Morphologically, the analyses confirmed the presence of lymphoblasts and in the positive results Ti was observed in the macrophages. Ti may induce hypersensitivity and should not be considered an inert material | |||||
| Hosoki et al. [33] | Eczema 2 years after implant placement, triggered by orthopaedic surgery | No changes | Removal of orthopaedic screws (50% improvement), removal of metal restorations and oral prostheses (30% improvement), removal of implants | Patch Test for 28 metal types | Study concluded that the patient was possibly sensitized by orthopaedic surgery and developed implant allergy to Ti | ||
| Hosoki et al. [32] | 4 patients had allergic manifestations of eczema and local reactions | 3 of the patients who presented reactions underwent implant removal | Patch Test for 28 metal types | 217 patients (80.4%) positive for at least one metal. Of the 16 patients with signs of allergy after implant placement, 11 of these were positive for other metals and 4 were positive for Ti |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poli, P.P.; de Miranda, F.V.; Polo, T.O.B.; Santiago Júnior, J.F.; Lima Neto, T.J.; Rios, B.R.; Assunção, W.G.; Ervolino, E.; Maiorana, C.; Faverani, L.P. Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report. Materials 2021, 14, 5239. https://doi.org/10.3390/ma14185239
Poli PP, de Miranda FV, Polo TOB, Santiago Júnior JF, Lima Neto TJ, Rios BR, Assunção WG, Ervolino E, Maiorana C, Faverani LP. Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report. Materials. 2021; 14(18):5239. https://doi.org/10.3390/ma14185239
Chicago/Turabian StylePoli, Pier Paolo, Fábio Vieira de Miranda, Tárik Ocon Braga Polo, Joel Ferreira Santiago Júnior, Tiburtino José Lima Neto, Bárbara Ribeiro Rios, Wirley Gonçalves Assunção, Edilson Ervolino, Carlo Maiorana, and Leonardo Perez Faverani. 2021. "Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report" Materials 14, no. 18: 5239. https://doi.org/10.3390/ma14185239
APA StylePoli, P. P., de Miranda, F. V., Polo, T. O. B., Santiago Júnior, J. F., Lima Neto, T. J., Rios, B. R., Assunção, W. G., Ervolino, E., Maiorana, C., & Faverani, L. P. (2021). Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report. Materials, 14(18), 5239. https://doi.org/10.3390/ma14185239