Bio-Absorption of Human Dentin-Derived Biomaterial in Sheep Critical-Size Iliac Defects

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
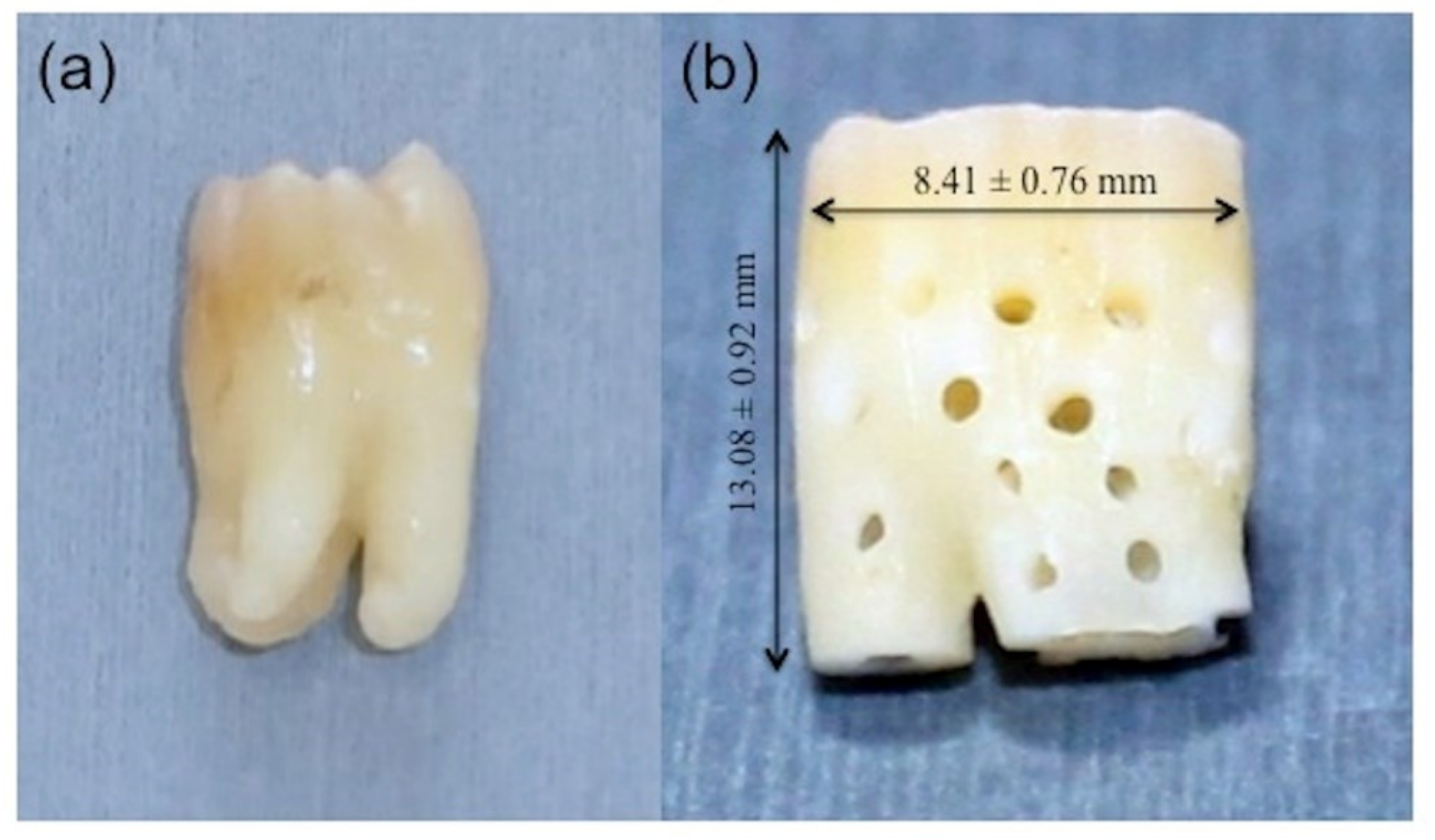
2.1. Perforated Root-Demineralized Dentin Matrix (PR-DDM) Preparation
2.2. Morphological Characterization
2.3. Animal Experiment
2.3.1. Ethics Statement
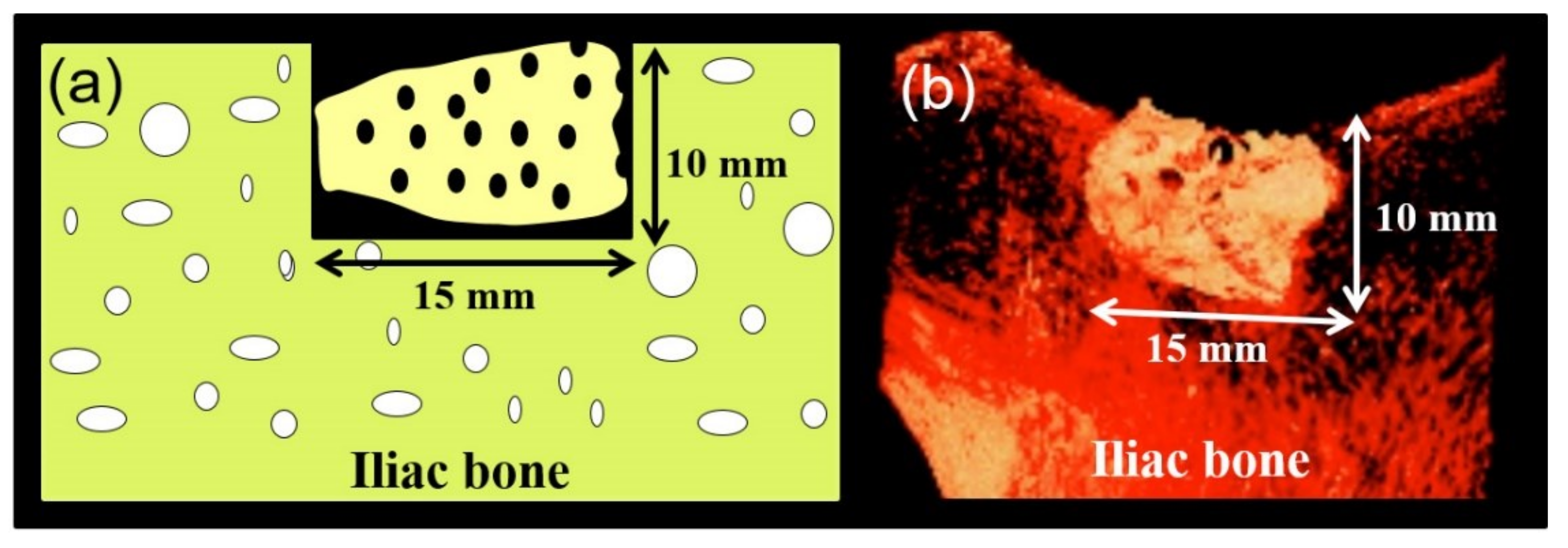
2.3.2. Surgical Procedures
2.3.3. Micro-Computed Tomography (Micro-CT) Analysis
2.3.4. Histological Analysis
2.3.5. Statistical Analysis
3. Results
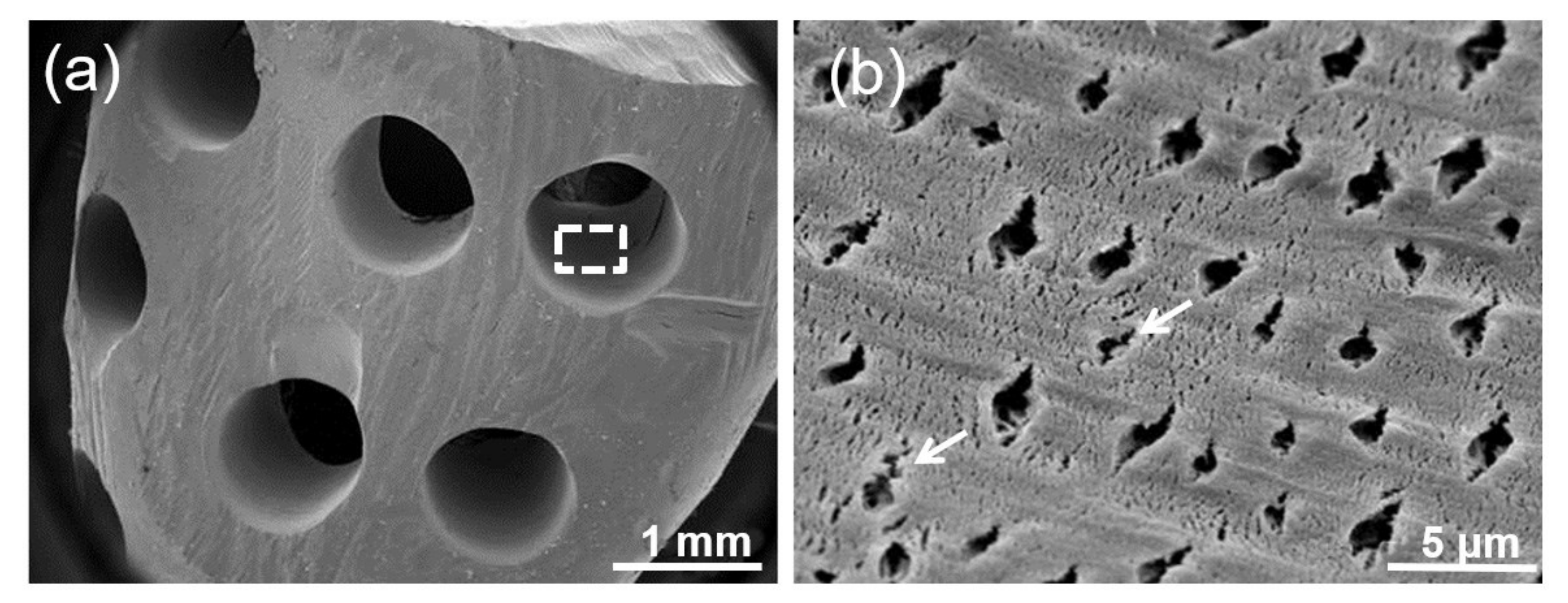
3.1. Surface Topography
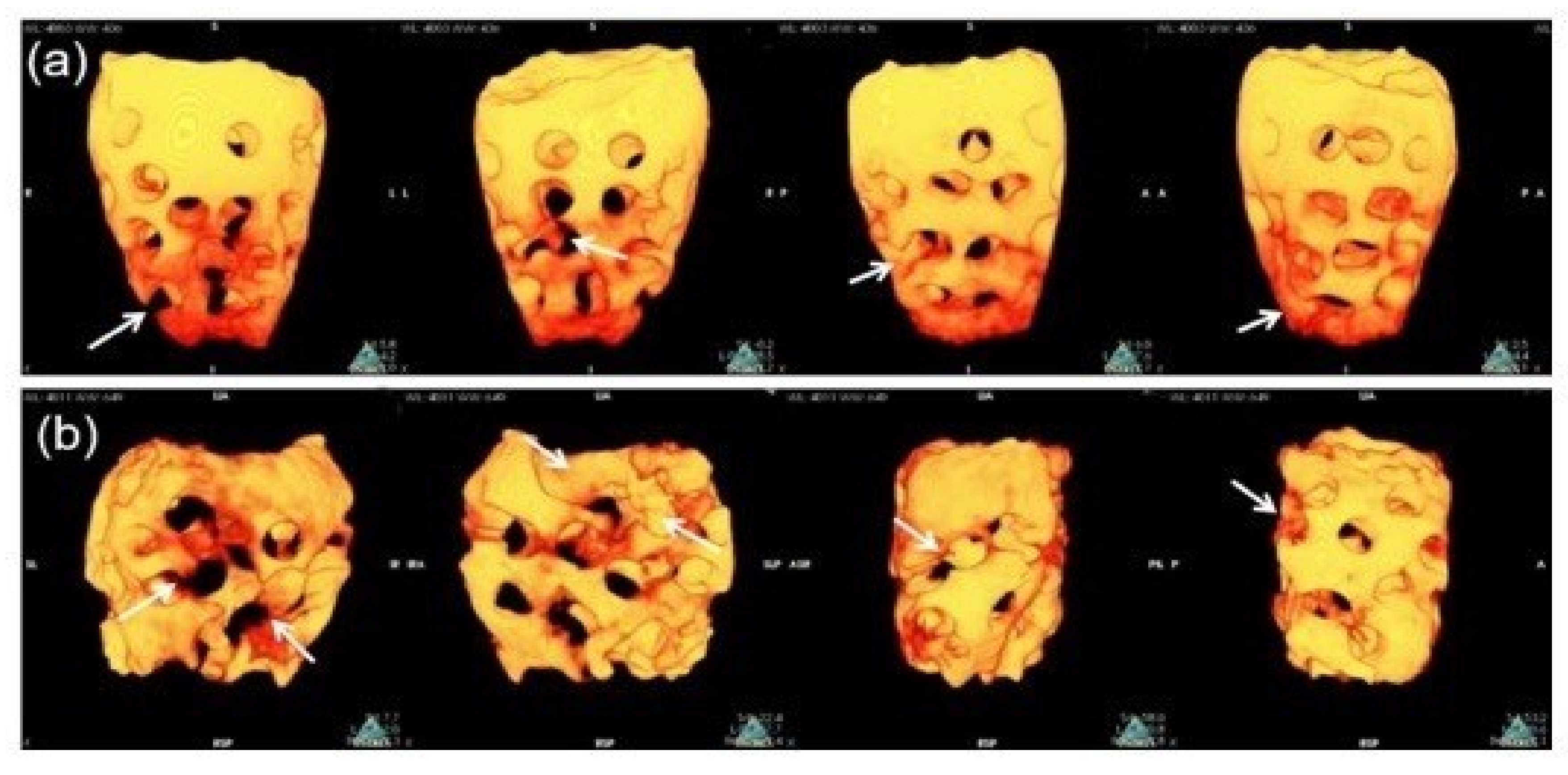
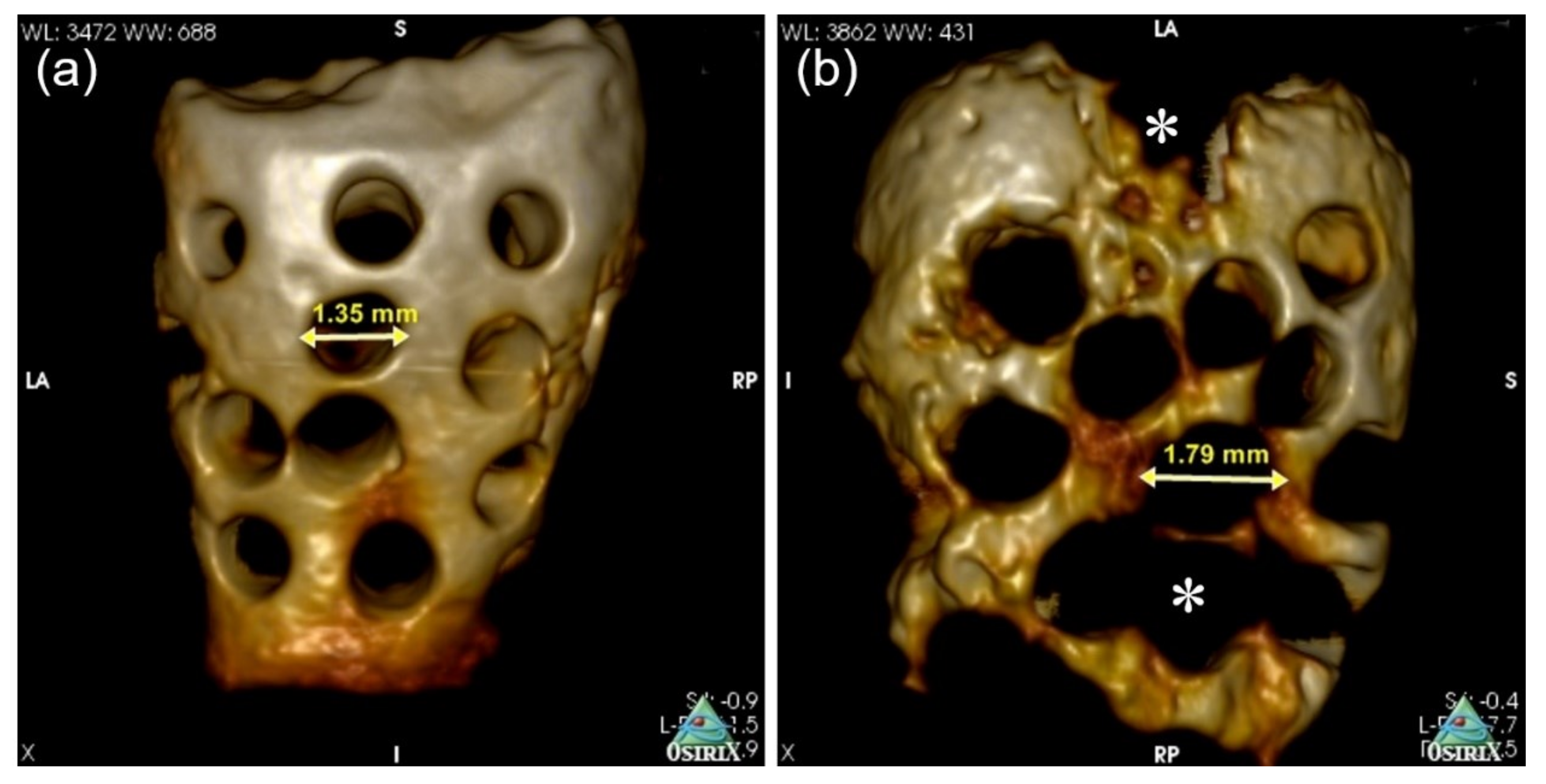
3.2. Bio-Absortion Evaluation by 3D Micro-CT
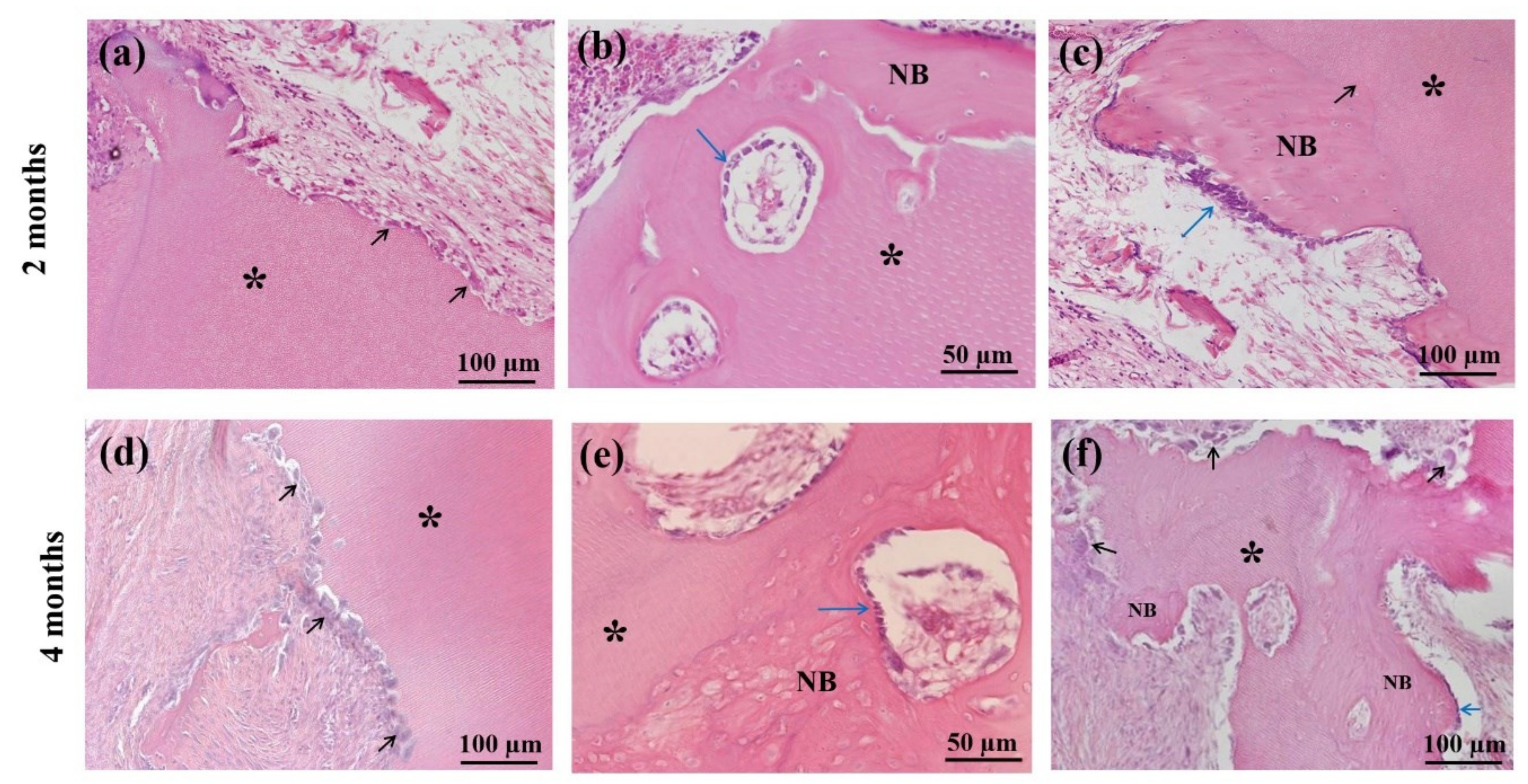
3.3. Histological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murata, M.; Akazawa, T.; Mitsugi, M.; Kabir, M.A.; Um, I.W.; Minamida, Y.; Kim, K.W.; Kim, Y.K.; Sun, Y.; Qin, C. Autograft of dentin materials for bone regeneration. In Advances in Biomaterials Sciences and Biomedical Applications, 1st ed.; Pignatello, R., Ed.; InTech: Rijeka, Croatia, 2013; Volume 15, pp. 391–403. [Google Scholar]
- Mohan, S.; Linkhart, T.A.; Jennings, J.C.; Baylink, D.J. Identification and quantification of four distinct growth factors stored in human bone matrix. J. Bone Miner. Res. 1987, 2, 44–47. [Google Scholar]
- Finkelman, R.D.; Mohan, S.; Jennings, J.C.; Taylor, A.K.; Jepsen, S.; Baylink, D.J. Quantitation of growth factors IGF-I, SGF/IGF-II, and TGF-beta in human dentin. J. Bone Miner. Res. 1990, 5, 717–723. [Google Scholar] [CrossRef]
- Kawai, T.; Urist, M.R. Bovine tooth-derived bone morphogenetic protein. J. Dent. Res. 1989, 68, 1069–1074. [Google Scholar] [CrossRef]
- Bessho, K.; Tanaka, N.; Matsumoto, J.; Tagawa, T.; Murata, M. Human dentin-matrix-derived bone morphogenetic protein. J. Dent. Res. 1991, 70, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Um, I.W.; An, H.J.; Kim, K.W.; Hong, K.S.; Murata, M. Effects of demineralized dentin matrix used as an rhBMP-2 carrier for bone regeneration. J. Hard Tissue Biol. 2014, 23, 415–422. [Google Scholar] [CrossRef]
- Ike, K.; Urist, M.R. Recycled dentin root matrix for a carrier of recombinant human bone morphogenetic protein. J. Oral Implantol. 1998, 24, 124–132. [Google Scholar] [CrossRef]
- Murata, M. Bone engineering using human demineralized dentin matrix and recombinant human BMP-2. J. Hard Tissue Biol. 2005, 14, 80–81. [Google Scholar] [CrossRef]
- Murata, M.; Sato, D.; Hino, J.; Akazawa, T.; Tazaki, J.; Ito, K.; Arisue, M. Acid-insoluble human dentin as carrier material for recombinant human BMP-2. J. Biomed. Mater. Res. Part A 2012, 100, 571–577. [Google Scholar] [CrossRef]
- Murata, M.; Arisue, M.; Tazaki, J.; Ito, K.; Hino, J.; Akazawa, T. Biochemical and histo-morphometrical analyses of bone and cartilage induced by human decalcified dentin matrix and BMP-2. Oral Biol. Res. 2011, 35, 9–14. [Google Scholar] [CrossRef]
- Xu, C.; Wang, Y. Cross-linked demineralized dentin maintains its mechanical stability when challenged by bacterial collagenase. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 96, 242–248. [Google Scholar] [CrossRef]
- Murata, M.; Kawai, T.; Kawakami, T.; Akazawa, T.; Tazaki, J.; Ito, K.; Kusano, K.; Arisue, M. Human acid-insoluble dentin with BMP-2 accelerates bone induction in subcutaneous and intramuscular tissues. J. Ceram. Soc. Jpn. 2010, 118, 438–441. [Google Scholar] [CrossRef][Green Version]
- Urist, M.R. Bone: Formation by autoinduction. Science 1965, 150, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Bang, G.; Urist, M.R. Bone induction in excavation chambers in matrix of decalcified dentin. Arch. Surg. 1967, 94, 781–789. [Google Scholar] [CrossRef]
- Yeomans, J.D.; Urist, M.R. Bone induction by decalcified dentine implanted into oral, osseous and muscle tissues. Arch. Oral Biol. 1967, 12, 999–1008. [Google Scholar] [CrossRef]
- Murata, M.; Sato, D.; Akazawa, T.; Taira, T.; Sasaki, T.; Arisue, M. Bone and cartilage induction in nude mice by human demineralized dentin matrix. J. Hard Tissue Biol. 2003, 11, 110–114. [Google Scholar]
- Andersson, L.; Ramzi, A.; Joseph, B. Studies on dentin grafts to bone defects in rabbit tibia and mandible; development of an experimental model. Dent. Traumatol. 2009, 25, 78–83. [Google Scholar] [CrossRef]
- Andersson, L. Dentin xenografts to experimental bone defects in rabbit tibia are ankylosed and undergo osseous replacement. Dent. Traumatol. 2010, 26, 398–402. [Google Scholar] [CrossRef]
- Qin, X.; Raj, R.M.; Liao, X.F.; Shi, W.; Ma, B.; Ging, S.Q.; Chen, W.M.; Zhou, B. Using rigidly fixed autogenous tooth graft to repair bone defect: An animal model. Dent. Traumatol. 2014, 30, 380–384. [Google Scholar] [CrossRef]
- Flatley, T.J.; Lynch, K.L.; Benson, M. Tissue response to implants of calcium phosphate ceramic in the rabbit spine. Clin. Orthop. Relat. Res. 1983, 179, 246–252. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, H.K.; Lim, S.C. Combined implantation of particulate dentine, plaster of Paris, and a bone xenograft (Bio-Oss) for bone regeneration in rats. J. Craniofac. Surg. 2001, 29, 282–288. [Google Scholar]
- Kim, Y.K.; Kim, S.G.; Byeon, J.H.; Lee, H.J.; Um, I.U.; Lim, S.C.; Kim, S.Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, Y.K.; Yi, Y.J.; Choi, J.H. Clinical evaluation of ridge augmentation using autogenous tooth bone graft material: Case series study. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Yun, P.Y.; Um, I.W.; Lee, H.J.; Yi, Y.J.; Bae, J.H.; Lee, J. Alveolar ridge preservation of an extraction socket using autogenous tooth bone graft material for implant site development: Prospective case series. J. Adv. Prosthodont. 2014, 6, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.H.; Ahn, J.S.; Lee, J.I.; Ahn, K.J.; Yun, P.Y.; Kim, Y.K. A prospective study on the effectiveness of newly developed autogenous tooth bone graft material for sinus bone graft procedure. J. Adv. Prosthodont. 2014, 6, 528–538. [Google Scholar] [CrossRef]
- Shakya, M.; Yokozeki, K.; Akazawa, T.; Murata, M. Rapid bone induction of cortical bone treated with ultrasonic demineralization in acidic electrolyzed water. J. Hard Tissue Biol. 2018, 27, 269–271. [Google Scholar] [CrossRef]
- Binderman, I.; Hallel, G.; Nardy, C.; Yaffe, A.; Sapoznikof, L. A novel procedure to process extracted teeth for immediate grafting autogenous dentin. Interdisciplin. Med. Dent. Sci. 2014, 2, 154–158. [Google Scholar]
- Koga, T.; Minamizato, T.; Kawai, Y.; Muira, K.-I.; Takashi, I.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone Regeneration Using Dentin Matrix Depends on the Degree of Demineralization and Particle Size. PLoS ONE 2016, 11, e0147235. [Google Scholar] [CrossRef]
- Gomes, M.F.; Abreu, P.P.; Morosolli, A.R.; Araujo, M.M.; Goulart, M.D. Densitometric analysis of the autogenous demineralized dentin matrix on the dental socket wound healing process in humans. Braz. Oral Res. 2006, 20, 324–330. [Google Scholar] [CrossRef]
- Kabir, M.A.; Murata, M.; Kusano, K.; Zakaria, S.M.; Noor, A.H.M.; Khuda, F.; Hossain, I.; Sultana, S.; Saito, T. Radiological evaluation of human dentin autografts in Bangladesh. J. Hard Tissue Biol. 2014, 23, 363–370. [Google Scholar] [CrossRef][Green Version]
- Gosain, A.K.; Song, L.; Yu, P.; Mehrara, B.J.; Maeda, C.Y.; Gold, L.I.; Longaker, M.T. Osteogenesis in cranial defects: Reassessment of the concept of critical size and the expression of TGF-beta isoforms. Plast. Reconstr. Surg. 2000, 106, 360–371. [Google Scholar] [CrossRef]
- Kabir, M.A.; Murata, M.; Akazawa, T.; Kusano, K.; Yamada, K.; Ito, M. Evaluation of perforated dentin scaffold on bone regeneration in critical-size sheep iliac defects. Clin. Oral Implants Res. 2017, 28, e227–e235. [Google Scholar] [CrossRef] [PubMed]
- Akazawa, T.; Murata, M.; Minamida, Y.; Tingting, W.; Kabir, A.; Hino, J.; Tazaki, J.; Ito, M.; Kimura, I. Bioactive surface structure and bio-absorption of human dentin granules designed by the supersonic demineralization and biomimetic coating technique. J. Hard Tissue Biol. 2011, 21, 351–358. [Google Scholar] [CrossRef][Green Version]
- Zerbo, I.R.; Bronckers, A.L.; de Lange, G.L.; Beek, G.J.; Burger, E.H. Histology of human alveolar bone regeneration with a porous tricalcium phosphate-A report of two cases. Clin. Oral Implants Res. 2001, 12, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Karageorgiou, V.; Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 2005, 26, 5474–5491. [Google Scholar] [CrossRef] [PubMed]
- Kuboki, Y.; Takita, H.; Kobayashi, D.; Tsuruga, E.; Inoue, M.; Murata, M.; Nagai, N.; Dohi, Y.; Ohgushi, H. BMP-induced osteogenesis on the surface of hydroxyapatite with geometrically feasible and non-feasible structures: Topology of osteogenesis. J. Biomed. Mater. Res. 1998, 39, 190–199. [Google Scholar] [CrossRef]
- Al-Asfour, A.; Farzad, P.; Andersson, L.; Joseph, B.; Dahlin, C. Host tissue reactions of non-deminerali-zed autogenic and xenogenic dentin blocks implanted in a non-osteogenic environment. An experimental study in rabbits. Dent. Traumatol. 2014, 30, 198–203. [Google Scholar] [CrossRef]
- Uematsu, H.; Hoshino, E. Predominant obligate anaerobes in human periodontal pockets. J. Periodontal. Res. 1992, 27, 15–19. [Google Scholar] [CrossRef]
- Fujita, M.; Uehara, O.; Miyakawa, H.; Naito, S.; Kabir, M.A.; Murata, M.; Nakazawa, F. Detection of bacteria in human tooth-derived biomaterials. In Advances in Oral Tissue Engineering; Murata, M., Um, I.W., Eds.; Quintessence Publishing Co. Inc.: Chicago, IL, USA, 2014; pp. 31–32. [Google Scholar]
- El-Karim, I.; Lundy, F.T.; Linden, G.J.; Lamey, P.J. Extraction and radioimmunoassay quantitation of neuropeptide Y (NPY) and vasoactive intestinal polypeptide (VIP) from human dental pulp tissue. Arch. Oral Biol. 2003, 48, 249–254. [Google Scholar] [CrossRef]
- Badran, Z.; Pilet, P.; Verron, E.; Bouler, J.M.; Weiss, P.; Grimand, G.; Guicheux, J.; Soueidan, A. Assay of in vitro osteoclast activity on dentine, and synthetic calcium phosphate bone substitues. J. Mater. Sci. Mater. Med. 2012, 23, 797–803. [Google Scholar] [CrossRef]
- Pashley, D.H.; Tay, F.R.; Yiu, C.; Hashimoto, M.; Breschi, L.; Carvalho, R.M.; Ito, S. Collagen degradation by host-derived enzymes during aging. J. Dent. Res. 2004, 83, 216–221. [Google Scholar] [CrossRef]
- Murata, M.; Akawaza, T.; Hino, J.; Tazaki, J.; Fujii, M.; Shibata, T.; Arisue, M. Multinucleated giant cells for biomaterials- ceramics and dentin collagen. Key Eng. Mater. 2011, 493–494, 310–314. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar]
- Gendler, E. Perforated demineralized bone matrix: A new form of osteoinductive biomaterial. J. Biomed. Mater. Res. 1986, 20, 687–697. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Explant Period | ||
|---|---|---|---|
| Title | 0 Days | 2 Months | 4 Months |
| Number of marco-pores | 30 | 25.5 ± 3.05 * | 13.3 ± 1.52 * |
| Size of macro-pores (mm) | 1.0 | 1.35 ± 0.13 ** | 1.79 ± 0.08 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabir, M.A.; Murata, M.; Shakya, M.; Yamada, K.; Akazawa, T. Bio-Absorption of Human Dentin-Derived Biomaterial in Sheep Critical-Size Iliac Defects. Materials 2021, 14, 223. https://doi.org/10.3390/ma14010223
Kabir MA, Murata M, Shakya M, Yamada K, Akazawa T. Bio-Absorption of Human Dentin-Derived Biomaterial in Sheep Critical-Size Iliac Defects. Materials. 2021; 14(1):223. https://doi.org/10.3390/ma14010223
Chicago/Turabian StyleKabir, Md Arafat, Masaru Murata, Mamata Shakya, Katsuhisa Yamada, and Toshiyuki Akazawa. 2021. "Bio-Absorption of Human Dentin-Derived Biomaterial in Sheep Critical-Size Iliac Defects" Materials 14, no. 1: 223. https://doi.org/10.3390/ma14010223
APA StyleKabir, M. A., Murata, M., Shakya, M., Yamada, K., & Akazawa, T. (2021). Bio-Absorption of Human Dentin-Derived Biomaterial in Sheep Critical-Size Iliac Defects. Materials, 14(1), 223. https://doi.org/10.3390/ma14010223