1. Introduction
Large bone defects caused by malignant tumor resection, trauma, and infection are currently reconstructed using autologous bone or biomaterials. Good bone union can be achieved using a vascularized autologous bone graft [
1,
2,
3,
4,
5,
6,
7]. However, autologous bone grafts involve major invasion of the donor site. Furthermore, implantation of a vascularized bone graft requires a long operation time and may cause serious complications, including total necrosis of the transplanted tissue due to thrombus of the feeding blood vessel [
7,
8]. Alternatively, the use of synthetic biomaterials as bone grafts does not require a donor site and enables performing shorter and less invasive surgeries. Various biomaterials have been developed that can overcome the shortcomings of autologous bone transplantation [
9,
10]. Nevertheless, because biomaterials are foreign bodies, the main limitations of their use include increased risks of long-term infection, exposure, and damage. At present, metals such as titanium or bioceramics including hydroxyapatite (HAp) and tricalcium phosphate (TCP), are widely used as biomaterials for bone grafts. Titanium has relatively good biocompatibility along with excellent workability and strength but is not bioabsorbable and is considered to be a foreign substance by the body. On the other hand, HAp and TCP have inferior strength to metals, but have osteoconductivity and excellent biocompatibility. These materials allow for the migration, proliferation, differentiation, and extracellular matrix (ECM) deposition of bone progenitor cells. Furthermore, HAp is hardly absorbed in vivo, and absorption is very slow if it does occur. In contrast, TCP is easily decomposed and absorbed in vivo. However, if bone formation in the central part of the biomaterial is insufficient, complete replacement with new bone tissue is hindered. The material then continues to be considered a foreign substance, and sufficient strength cannot be achieved. Consequently, to allow for adaptation to areas with low blood supply (such as large bone defects), an ideal scaffold that facilitates bone cell and blood vessel invasion at the interior of the material is desired.
Several recent studies have suggested that the geometry of biomaterials is important for inducing cell differentiation and tissue formation. To induce hard tissue formation, the optimum shape and size of the pores and optimum geometric structure have been determined [
11,
12,
13,
14]. Kuboki et al. [
11] showed that straight tunnel-shaped HAp with a pore size of 300–400 μm achieved good bone formation. They further determined that the structure of the open tube induces better angiogenesis and bone formation than that of the dead-end tube. Therefore, we postulated that the development of TCP with a honeycomb structure would provide good bone regeneration to the center of the defect, and that TCP decomposition and resorption would enable complete bone replacement.
We have succeeded in developing a new honeycomb β-TCP scaffolding material with through-and-through holes, and it was found that sintering at 1200 °C yields high biocompatibility and bone conductivity [
15]. We also showed that bone formation can be controlled by the size of the through-and-through holes and amount of bone morphogenic protein (BMP)-2. The material with 300 μm through-and-through holes provided an environment suitable for cell proliferation and differentiation and was optimal for inducing bone tissue regeneration [
16]. Furthermore, we obtained good bone tissue regeneration in vivo after implanting honeycomb β-TCP with 300 μm through-and-through holes in a rat zygomatic bone defect model. Although bone tissue regeneration was confirmed, long-term observation was not performed, and thus details regarding the maintenance of regenerated bone tissue, bone remodeling, and β-TCP absorption are unknown. In these previous studies, we used Matrigel for BMP-2 addition, which is often used for culturing induced pluripotent stem cells. However, as Matrigel is comprised of ECM extracted from mouse cancer tissue, its clinical application in humans is difficult. Therefore, in this study, we used the same honeycomb β-TCP with 300 μm through-and-through holes as a bone reconstruction material in a zygomatic bone defect model to observe the long-term result. In addition, we evaluated whether honeycomb β-TCP is suitable as a bone reconstruction material for clinical application, using both Matrigel and collagen, the latter of which is already used clinically as ECM.
2. Materials and Methods
2.1. Preparation of Honeycomb β-TCP Scaffolds Containing BMP-2
Honeycomb β-TCP sintered at 1200 °C with a diameter of 3 mm, length of 5 mm, and containing 37 through-and-through holes of 300 μm diameter was purchased from Pilot Corporation (Tokyo, Japan) [
14,
15]. The honeycomb β-TCP was autoclaved immediately before implantation for the experiment (
Figure 1a). For the BMP-2 concentration in this study, we determined the concentration that showed the most bone formation in our previous study [
16]. BMP-2 (Peprotech, NJ, USA) was prepared and diluted with BD Matrigel™ (BD Biosciences, Bedford, MA, USA; hereafter referred to as Matrigel) or AteloCell
® (KOKEN, Tokyo, Japan; hereafter referred to as collagen gel) to a concentration of 80 μg/mL. The BMP-2 solution (12.5 μL; 1 μg BMP-2) was filled into the β-TCP scaffold by centrifuging at 1500 rpm for 1 min and then incubated at 37 °C for 30 min. In the group implanted with β-TCP alone, the honeycomb β-TCP was filled with 12.5 μL of Matrigel or collagen gel without BMP-2.
2.2. Animals and Implantation Procedure
All experiments in this study were approved by the Animal Care and Use Committee, Okayama University (OKU-2019493). All surgical procedures were performed under general anesthesia. Five-week-old healthy male Wistar rats (Charles River Laboratories Japan, Kanagawa, Japan) were used in the experiment. The rats were anesthetized by intraperitoneal injection of ketamine hydrochloride (75 mg/kg) and medetomidine hydrochloride (0.5 mg/kg). After operation, atipamezole hydrochloride (1 mg/kg) was intraperitoneally injected to awaken.
For implantation, a skin incision of approximately 8 mm was made at the anterior site of the zygomatic arch, and the zygomatic periosteum was exposed. Next, the zygomatic periosteum was incised with a surgical knife and completely peeled from the zygomatic bone. The zygomatic arch was cut with scissors to produce a complete bone defect of 5 mm. Subsequently, β-TCP alone (TCP group) or β-TCP with BMP-2 added (BMP group) was implanted in the bone defect. In all cases, β-TCP was implanted so that the anterior part was in contact with the zygomatic body, the posterior part was in contact with the zygomatic arch, and the through-and-through holes of β-TCP and the long axis of the bone defect were parallel to each other (
Figure 1b,c).
2.3. Implantation Using Matrigel and Collagen Gel
Matrigel was used as the carrier for BMP-2 in this experiment. In addition to the TCP and BMP groups, a zygomatic bone defect group in which β-TCP was not implanted was also established as a control group. Only the left side was operated, and 6 months after the operation, the rats were euthanized with carbon dioxide gas. Specimens were then collected and fixed with 4% paraformaldehyde (PFA) (control group: n = 3, TCP group: n = 3, BMP group: n = 4).
Collagen gel was also used as the carrier for BMP-2 in this experiment. Based on the results of implantation using Matrigel, implantation using collagen gel as an alternative carrier were performed in the TCP and BMP groups to observe the long-term fate of β-TCP. For micro-CT imaging, only the left zygomatic bone was operated on, and β-TCP was implanted in the same manner as Matrigel experiment (TCP group: n = 4, BMP group: n = 4). In addition, β-TCP was implanted in the zygomatic bone of another group of rats for histological evaluation 1 month after implantation (TCP group: n = 2, BMP group: n = 2).
2.4. Micro-Computed Tomography (CT)
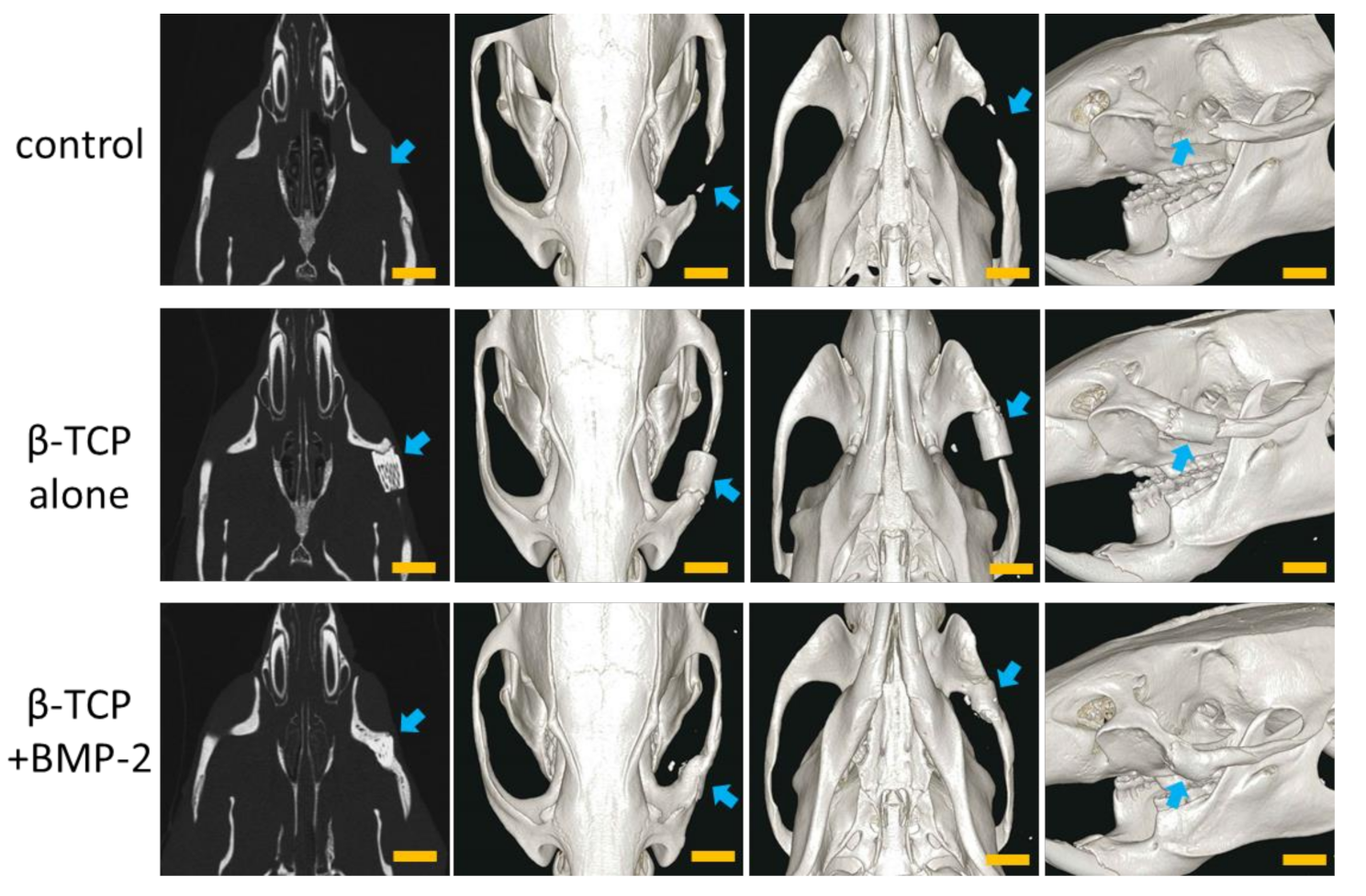
After fixation, the heads of the rats were photographed with a micro-CT LaTheta LCT200 system (Hitachi Aloka Medical, Tokyo, Japan), and the DICOM data obtained were reconstructed using the AZE Virtual Place Lexus 64 workstation and software (AZE, Tokyo, Japan). The zygomatic bone morphology was then qualitatively evaluated from the image in Matrigel experiment at 6 months after the operation.
In collagen gel experiments, at 1 month, 3 months, and 6 months after the operation, we performed micro-CT of the heads of the rats under general anesthesia (isoflurane inhalation) to track the course of recovery and bone regeneration following the operation. Bone morphology was qualitatively evaluated using three-dimensional (3D) reconstructed images as in the Matrigel experiment. Furthermore, the volume of β-TCP and the cross-sectional area at the rear end were measured and evaluated quantitatively.
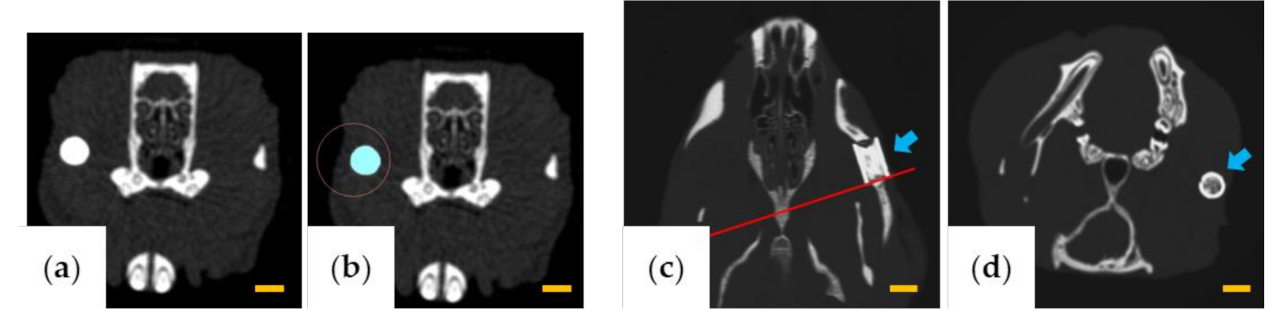
The volume of β-TCP was measured using LaTheta software v.3.50 (Hitachi Aloka Medical, Tokyo, Japan) by designating the β-TCP portion as the region of interest for each slice (
Figure 2a,b). The β-TCP residual rate (%) was calculated from the volumes at 1 month, 3 months, and 6 months, assuming that the volume of β-TCP was 100% immediately after implantation.
To evaluate the change of the cross-sectional area of β-TCP, AZE Virtual Place Lexus 64 was used to reconstruct the image of the rear edge of β-TCP in a plane perpendicular to the through-and-through holes (
Figure 2c,d). Six months after implantation, the area of β-TCP was measured using ImageJ software v.1.52 (National Institutes of Health, Bethesda, MD, USA) and was calculated as a percentage relative to the area in a cross-section before implantation.
2.5. Histology
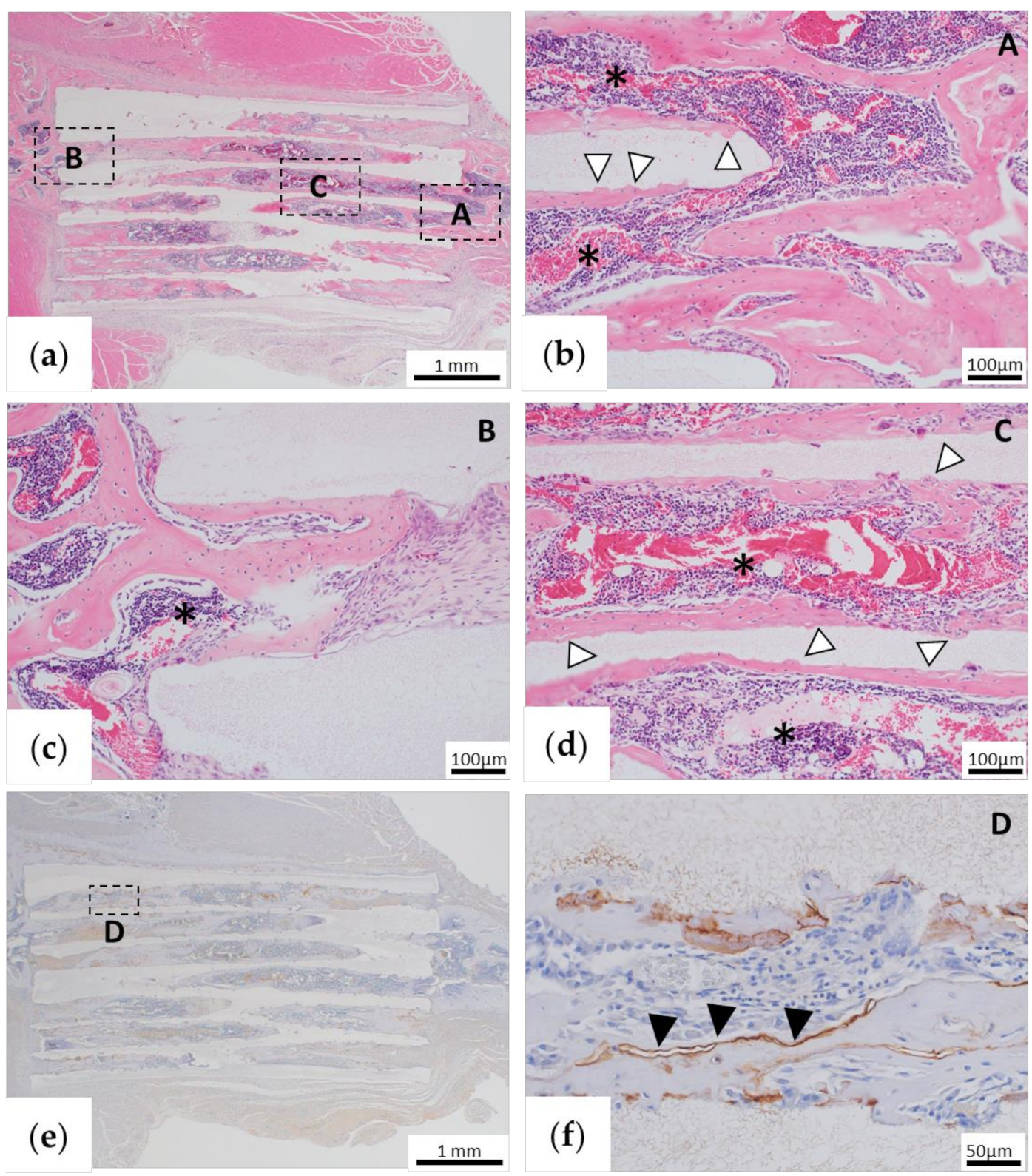
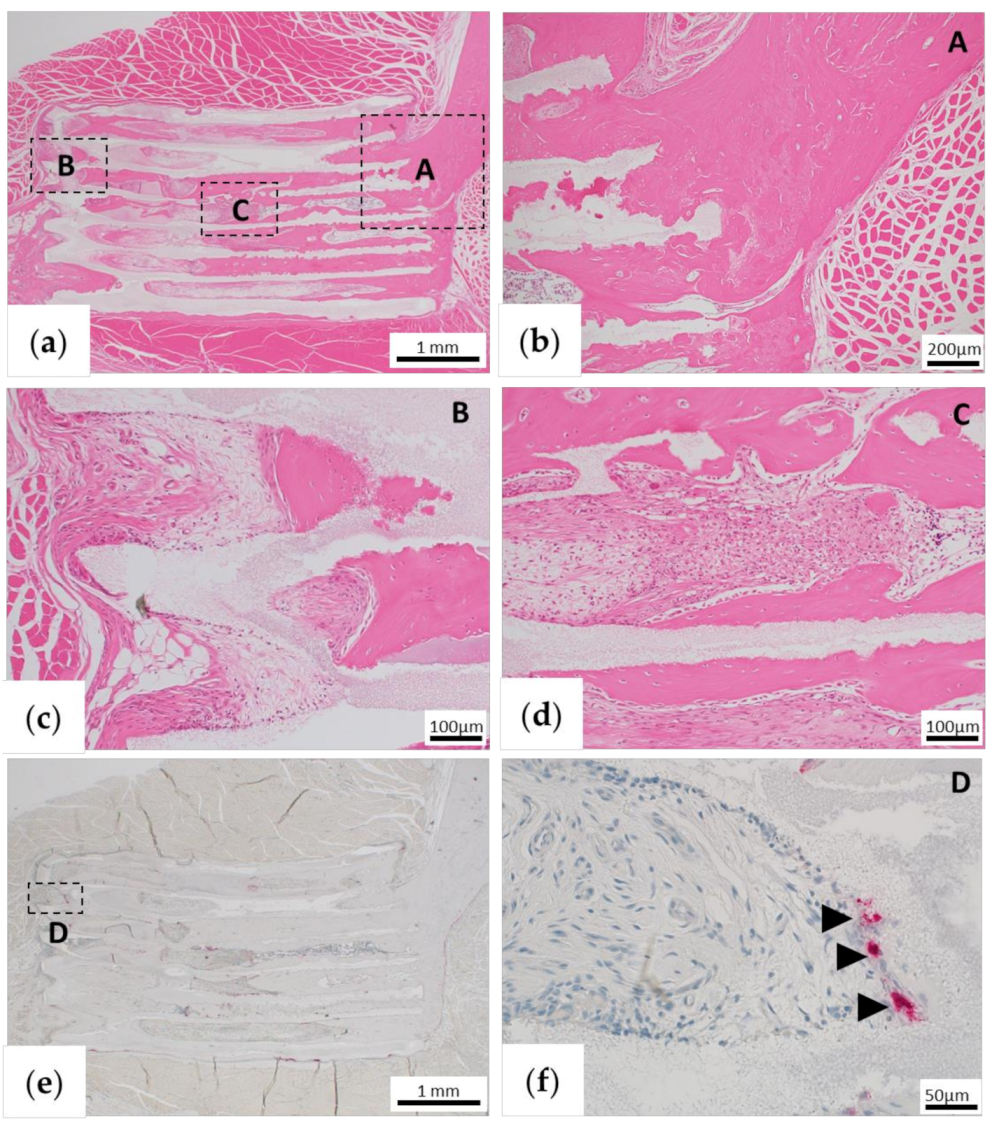
Rats were euthanized 1 or 6 months after implantation, and tissues containing β-TCP were removed. The excised tissue was fixed with 4% PFA and then decalcified in 10% ethylenediaminetetraacetic acid for 3 weeks. The tissue was embedded in paraffin and sliced to a thickness of 5 μm. The sections were chemically stained with hematoxylin and eosin (HE) and observed histologically.
2.6. Immunohistochemical Staining of Osteopontin (OPN)
In the specimens collected at 1 month after the operation, the presence of OPN, a non-collagen protein produced by osteoblasts in the ECM of the bone, was confirmed to evaluate bone formation.
The sections were deparaffinized, hydrophilized, and then incubated in proteinase K for 15 min at room temperature. Endogenous peroxidase was blocked with a 0.3% hydrogen peroxide solution in methanol for 20 min. Non-specific binding sites were blocked with 10% normal rabbit antiserum (Vector Laboratories, Burlingame, CA, USA) for 10 min. Sections were incubated with monoclonal antibodies against rat OPN (Immuno-Biological Laboratories, Gunma, Japan) using the Vectastain ABC mouse kit (Vector Laboratories) according to the manufacturer instructions. The procedure was as follows: (1) incubation with primary antibody at a dilution of 1:50; (2) incubation with 1:200 diluted secondary anti-mouse IgG antibody for 30 min; (3) incubation of the avidin-biotin-peroxidase complex (ABC; Vector Laboratories) at a dilution of 1:50 for 30 min; and (4) treatment with diaminobenzidine for color development and nuclear counterstaining with Mayer’s hematoxylin. After staining, the cells were observed using an optical microscope. The control sections were treated in the same way in the absence of the primary antibody.
2.7. Tartrate-Resistant Acid Phosphatase (TRAP) Staining
TRAP staining was performed on a sample collected 6 months after implantation to confirm remodeling by osteoclasts. The staining was performed using the TRAP Staining Kit (Primary Cell, Hokkaido, Japan) according to the manufacturer’s instructions.
2.8. Statistical Analysis
All data are presented as the mean ±SD. Statistical analysis was performed using two-sided t-tests. P values < 0.01 were considered statistically significant.
4. Discussion
The treatment of zygomatic bone defect requires artificial biomaterials that induce vigorous bone formation, and most importantly, aesthetic recovery is also essential for the treatments of zygomatic bone defect. In the field of plastic surgery, it is the most important for zygomatic bone regeneration to recover bone tissue aesthetically, so simply regenerating bone tissue does not meet the needs of patient. However, to date, there have been no reports of artificial biomaterials that meet these conditions. To the best of our knowledge, the present study is the first reported attempt to form vigorous and aesthetic bone tissue in zygomatic bone defect using honeycomb β-TCP in long-term observation.
In many artificial bone studies, the materials, porosity, and pore shape have been optimized to enhance internal vascular invasion, osteocyte differentiation, and tissue formation using bioceramics such as HAp and β-TCP [
13,
17,
18,
19,
20,
21,
22]. Some long-term studies have been conducted, but most studies have only assessed bone formation based on extraosseous implantation such as intramuscular implantation [
19,
20,
21,
22], and there are few reports on long-term bone formation and morphological changes after intraosseous implantation. In our previous study, we used honeycomb β-TCP with complete through-and-through holes with a pore size of 300 μm, which was transplanted into a rat model with a complete zygomatic bone defect. In this previous study, we confirmed good bone tissue regeneration [
16]. However, this was a short-term result obtained 1 month after implantation alongside the addition of the potent bone growth factor BMP-2. Therefore, most of the β-TCP was not absorbed, and the aesthetic recovery was also not sufficient. Thus, it was necessary to observe the long-term morphological and histological changes. In addition, 1 month after implantation, bone induction was not observed with honeycomb β-TCP alone without BMP-2. However, some studies in which bioceramics were ectopically implanted showed bone formation over a long period of time, demonstrating its bone inducibility [
19,
20,
22]. Yuan et al. [
22] implanted β-TCP into the muscle of a dog and did not observe bone formation after 30 days, but it was observed after 150 days. From these reports, we postulated that bone induction may be achieved by long-term placement of honeycomb β-TCP without the addition of BMP-2.
In the previous zygomatic bone defect model study, the experiments were conducted using Matrigel as carrier for delivery of BMP-2 [
16]. Although Matrigel is widely used in many bone-inducing animal experiments, it is extracted from cultured mouse osteosarcoma cells. This complication makes extrapolation of these results for human application difficult. Therefore, new experiments were performed using Matrigel and collagen gel as BMP-2 carriers in our previous skull defect model experiment using honeycomb β-TCP [
23]. The results showed no significant differences in bone formation among both Matrigel group and collagen gel group. However, the skull and zygomatic bone are different regarding their histological and physiological structures. The skull has plate-like morphology and does not move physiologically, and its osteoblasts are supplied from the dura mater. In contrast, the zygomatic bone is constantly moving, since it is connected to the muscles involved in mastication, and the osteoblasts cannot be supplied by the periosteum in a completely transected bone defect. Thus, it is more difficult to regenerate zygomatic bone. To test this possibility, in the present study, we first conducted experiments using Matrigel as a carrier for growth factors. In the control group, only partial bone regeneration was obtained at 6 months, and the defect remained. In the TCP group, bone formation that could not be confirmed after 1 month could be confirmed after 6 months. This result is consistent with that obtained by Yuan et al. [
22]. In the BMP group, good union with the bone was achieved, and remodeling was observed wherein the shape of the implanted β-TCP changed to a morphology very similar to that of the original zygomatic bone. Next, we conducted experiments using collagen gel as a carrier for BMP-2. One month after the implantation, β-TCP with BMP-2 using the collagen gel also showed good bone union, similar to the result of a previous study, in which Matrigel was used as a carrier [
16]. Furthermore, to observe the process of long-term bone formation and morphological changes, micro-CT follow-up was performed over time at 1, 3, and 6 months after the implantation. In the BMP group, bone formation similar to the morphology of the zygomatic bone was observed around β-TCP at 1 month. Six months later, it was confirmed that the β-TCP and new bone were absorbed, and remodeling occurred to reproduce the original zygomatic bone shape. In the TCP group, bone formation was observed in both the stump of the β-TCP and in the central part of the β-TCP pore. This phenomenon may indicate that bone induction was obtained without BMP-2. In this study, there was no major difference of bone formation and remodeling between Matrigel and collagen gel in CT images and histological findings at 1 and 6 months (data not shown), demonstrating the usefulness of the honeycomb β-TCP using a clinically applicable collagen gel.
Interestingly, in the BMP group, new bone was formed on the entirety of the β-TCP at first. Then, bone resorption occurred in the part protruding from the original zygomatic bone shape, and the zygomatic bone shape was naturally reproduced. In other words, bone resorption occurred due to remodeling. In clinical practice, some reports have indicated that hypertrophy or atrophy of the vascularized fibular bone graft is caused by remodeling after reconstruction of the lower extremity or the mandible [
24,
25,
26,
27,
28]. The study in which vascularized bone grafts were implanted in rats and examined with or without mechanical stress showed that mechanical stress induced bone hypertrophy; conversely, reduced mechanical stress resulted in a decreased bone mass [
29,
30]. Similar to these reports, the honeycomb β-TCP used in this study was also incorporated into the bone matrix or gradually replaced with bone tissue via remodeling at the site of mechanical stress. At the site protruding from the original zygomatic bone shape, we postulated that β-TCP was absorbed via remodeling to restore the original zygomatic bone shape because there was no mechanical stress.
In the TCP group, the stump of the zygomatic bone was absorbed after 1 month, after which bone formation occurred from the stump and united with β-TCP. This resorption may have been caused by moving the zygomatic bone with the movement of the rat itself, because a rat is not able to rest spontaneously. Therefore, if the zygomatic bone can be internally fixed and kept at rest, good bone regeneration may be achieved from an early stage.
The main limitation of this study was that the surgical site could not be kept at rest after the operation. Moreover, the defect was a small area because β-TCP was implanted in the zygomatic bone of the rat. If β-TCP is implanted in large animals and internal fixation leads to the surgical site being at rest, good bone formation may be obtained without the addition of BMP-2. In addition, this effect can be confirmed in a state closer to the clinical state by implanting in a larger defect. Although the observation period in this study was 6 months, further morphological changes may be observed by carrying out analyses for a longer period. In addition, more frequent follow-up may lead to the elucidation of new mechanisms of remodeling. Finally, in the future, in order to elucidate the mechanism of TCP remodeling in bone reconstruction, we would like to examine the factors related to mechanical stress, such as MAPK signaling pathway and so on, which has been reported to be related to bone remodeling in recent years [
31,
32].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








