1. Introduction
Raman spectroscopy is an analytical method that consists of irradiating a sample with a visible laser source, then determining the type and condition of the substance based of the characteristics of the Raman scattered light that is generated. Evaluations of crystallinity, residual stress analyses, and chemical assessments of molecular structures can thus be performed without contact, damage, or radiation exposure. Since Raman spectroscopy allows analysis at the molecular level without requiring fluorescent probes, fixation, or other types of manipulation, it has recently received attention for its potential applications in several fields of medical science, including dentistry [
1]. Various methods of dental analysis using Raman spectroscopy have recently been reported, such as the detection of trace elements in the enamel [
2] and the detection of dentin formation in the dental pulp tissue [
3]. However, Raman spectroscopy as a means of diagnosing dental caries has long been considered difficult. The reason for this is that the sites of dental caries generate fluorescence noise that exceeds the Raman light and varies according to measurement site and configuration. Recently, however, the combination of Raman spectroscopy with optical coherence tomography and fluorescence subtraction methods using multichannel lock-in detection have also been reported in order to avoid fluorescence interference [
4,
5]. Furthermore, modern devices have enabled us to collect Raman data at various measurement sites and configurations and to construct highly reliable algorithms with suitable precision [
6]. When such algorithms are used as diagnostic tools, as we have recently reported, Raman spectroscopy can be used as a novel method for the early diagnosis of dental caries [
1]. Moreover, Raman spectroscopy allows for the detection of a threshold state of irreversible structural change at the very early stages of tooth enamel demineralization, as caused, for example, by carbonated beverages (e.g., Coca-Cola
TM) [
7]. Based on the technique’s confirmed analytical sensitivity, we firmly believe that, in the near future, Raman spectroscopy will allow for a prompt and efficient evaluation of enamel locations that are likely to develop dental caries with high probability.
Dental caries develop as a result of the demineralization of hydroxyapatite, which is in turn a consequence of the acidic environment produced by
Streptococcus mutans, the causative organism of dental caries [
8,
9,
10]. X-ray radiographic imaging, currently the most popular tool in clinical settings for dental diagnosis, evaluates the current condition (simultaneity), whereas Raman spectrometry allows for evaluation of the condition before the onset of disease (predictivity). This unique predictive capacity, which could lead to a paradigm shift in dental diagnostic methods, fits in well with the recently popular concept of preemptive medicine. Preemptive medicine is a new medical paradigm in which a medical treatment is adjusted to suit the mechanism of occurrence and progression of the pathological condition and its etiology [
11]. This goal is achieved by predicting in advance, and with high accuracy, that a disease will develop (predictive diagnosis), or by determining the precise diagnosis before the onset of disease (precise medicine) to prevent or at least delay disease occurrence. To successfully incorporate preemptive medicine into the dental field, highly sensitive diagnostic equipment allowing for the early detection of dental caries will be required. Using Raman spectrophotometry to perform predictive diagnosis with high accuracy (and reliability) at the initial stages prior to the onset of dental caries, and thus intervening before disease development to prevent dental caries, is now technologically possible. In addition, Raman spectrophotometry does not require exposure to radiation. Gonzalez et al. have previously reported that, in Japanese subjects, 3.2% of cancers were due to radiation used in medical diagnostic tests [
12]. In addition, Pearce et al. [
13] have reported that, among children who have been exposed to radiation used in medical diagnostic tests, the risk of subsequently developing leukemia and brain tumors could reach as much as three times higher than normal. Currently, diagnostic imaging in dentistry consists mostly of bitewing and panoramic radiography as well as CT imaging [
14]. Because Raman spectroscopy eliminates the need for radiation exposure, it is believed to be a promising diagnostic tool. Moreover, diagnosis of non-cavitated proximal caries has long been a challenging task when conventional radiographic methods are used [
15]. Accordingly, efforts have been made to develop more sensitive diagnostic tools for detecting initial lesions in populations with high caries risk and prevalence.
Among these innovative approaches are the proposed transillumination-based caries detection methods, which employ either a narrow-beam white light [
16], as in fiber-optic transillumination (FOTI) and digital imaging fiber-optic transillumination (DIFOTI), or a near-infrared source [
17], as in near-infrared transillumination (NIRT). Both of these methods are based on the same principle, which exploits the differences in photon scattering/absorption between healthy and disrupted enamel crystals, imaging the latter in dark shadow. Caries detection by laser fluorescence (LF) [
18] exploits the semi-empirical finding that a monochromatic red light applied to a tooth location with caries can excite a strong (intrinsic) fluorescence emission because of changes in the tooth tissue. This increase in fluorescence is mainly due to a bacterial photosensitive pigment present in caries tissue, but it could also be contributed by other factors related to oral hygiene. The FOTI/DIFOTI, NIRT, and LF methods have all been commercialized in dentistry, and their caries detection sensitivity/specificity is currently under examination [
19]. Nowadays, the LF method is perhaps the most advanced radiation-free method available to enhance early identification of caries and to follow their development through regular successive examinations.
The present study proposes to utilize Raman spectroscopy as an alternative radiation-free method that is superior in sensitivity to LF. We anticipate that the Raman method could play a key diagnostic role in future dentistry now that Raman devices have a sufficiently high sensitivity to be suitable for both diagnostic and preventive purposes.
We have previously established working algorithms for Raman spectrometry in the diagnosis of surface caries in the enamel structure [
6], but its usefulness for caries in the dentin structure has not yet been examined. Dentin, a hard tissue constituting a major component of the tooth, is located between the pulp cavity and the enamel or cementum. The chemical composition of dentin differs greatly from that of enamel, being composed of 70% hydroxyapatite (which makes up 96% of enamel) and 20% collagen fibers. Dentin is softer than enamel; this is believed to be the main reason why dental caries progress rapidly after the dentin is reached. During caries development, when the dentin caries reaches the pulp, severe spontaneous pain may occur as a result of complication by pulpitis. In addition, at that stage of disease development, the dental crown is likely to collapse as a result of the fragility of the tooth, which may ultimately lead to tooth extraction. To avoid this outcome, dental caries must be detected and treated in their very earliest stage, namely, the stage of early enamel demineralization.
In this study, we apply Raman spectroscopy to visualizing and quantifying the extent of dental caries buried in the subsurface of the dentin structure. This study is in line with our previous studies of caries in the enamel structure, but this is our first study treating caries that are hardly diagnosable by either visual examination or conventional methods such as X-rays. Applying the method described in this study may help prevent tooth loss and preserve patients’ quality of life. Raman photonic diagnostics is the key to the successful application of preemptive medicine in dentistry.
2. Materials and Methods
2.1. Teeth
Following consent from the donors, extracted human teeth were collected from the Department of Dentistry at University Hospital, Kyoto Prefectural University of Medicine or the Department of Dentistry, Kyoto Prefectural Rehabilitation Hospital For Mentally and Physically Disabled under the Review Boards (ERB-C-136)(RBMR17) (RBMR19).
2.2. Digital Microscopy Experiments
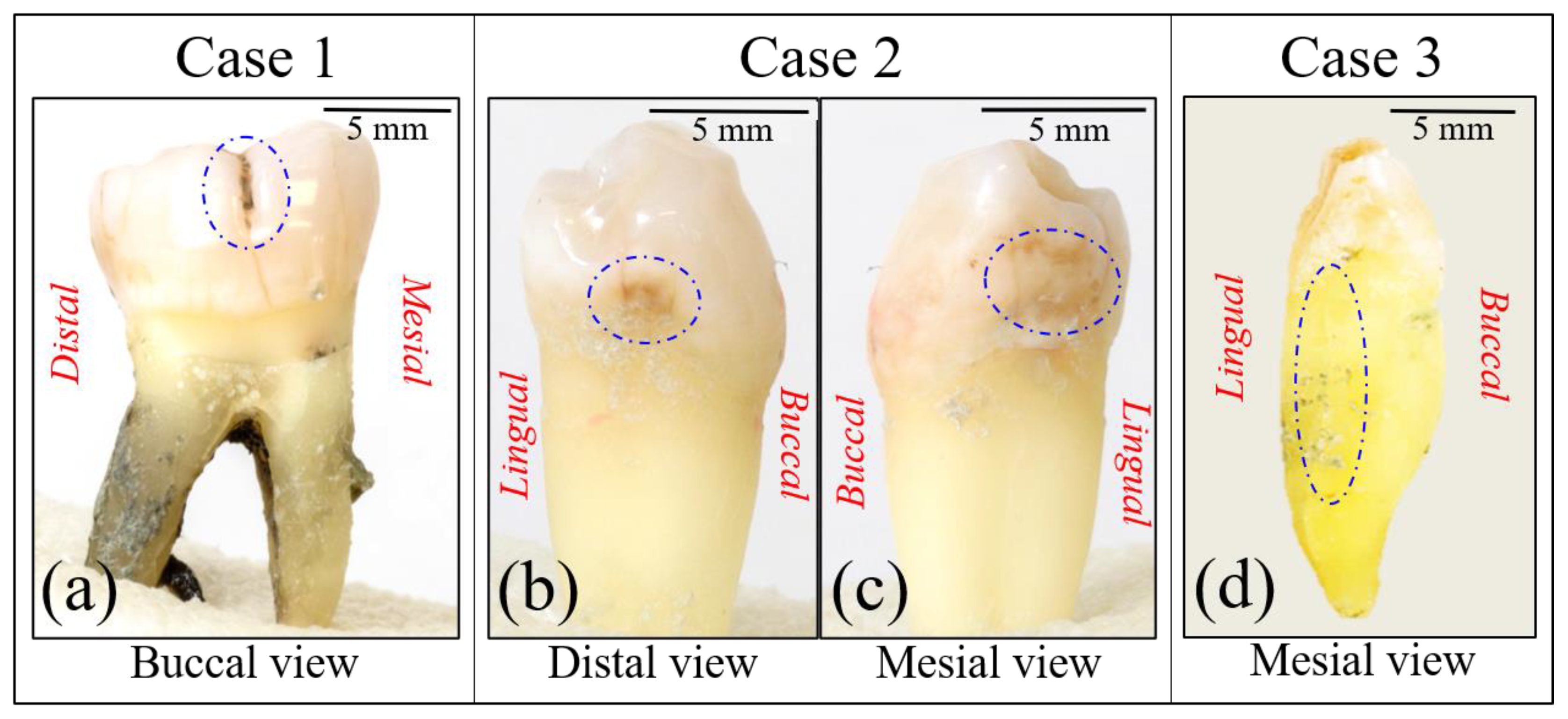
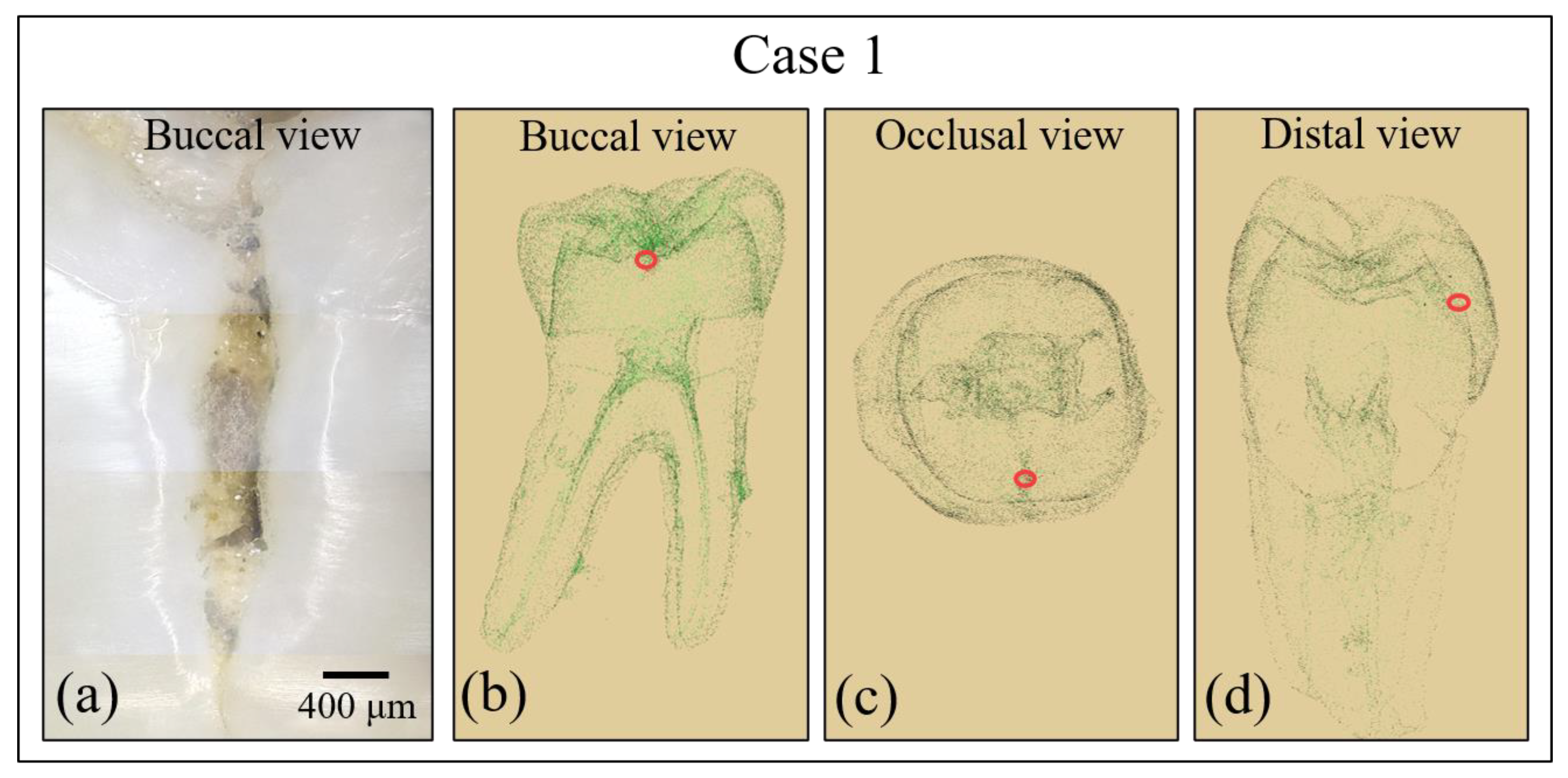
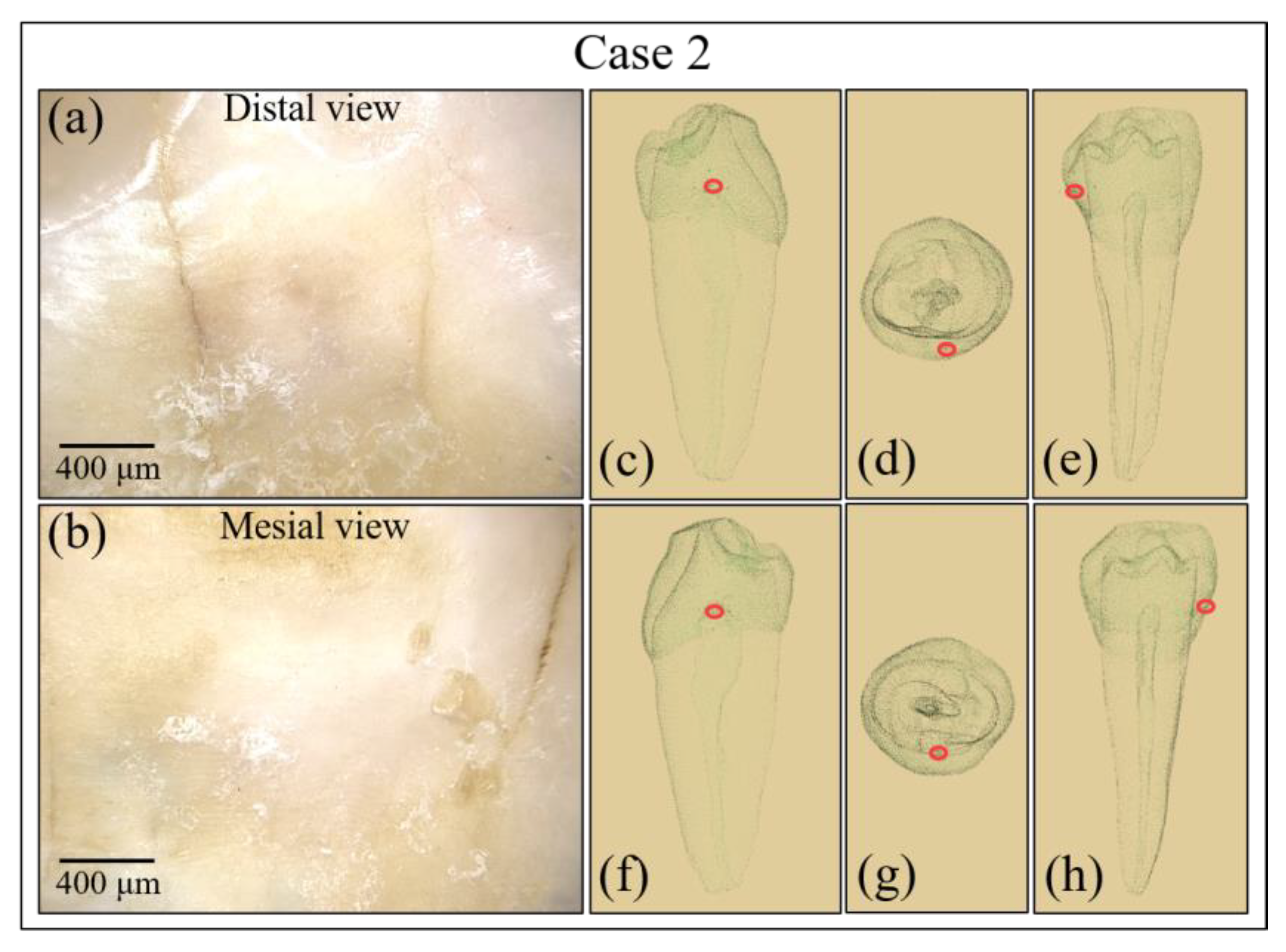
Each sample was examined by using a digital microscope (VHX-2000, Keyence, Osaka, Japan) in order to screen and evaluate the surface morphology of caries and cracks. Digital photographs were taken on fully focused images at ×100 magnification using depth composition function. The images were treated with software provided by the maker of the instrument.
2.3. Radiographic Examination
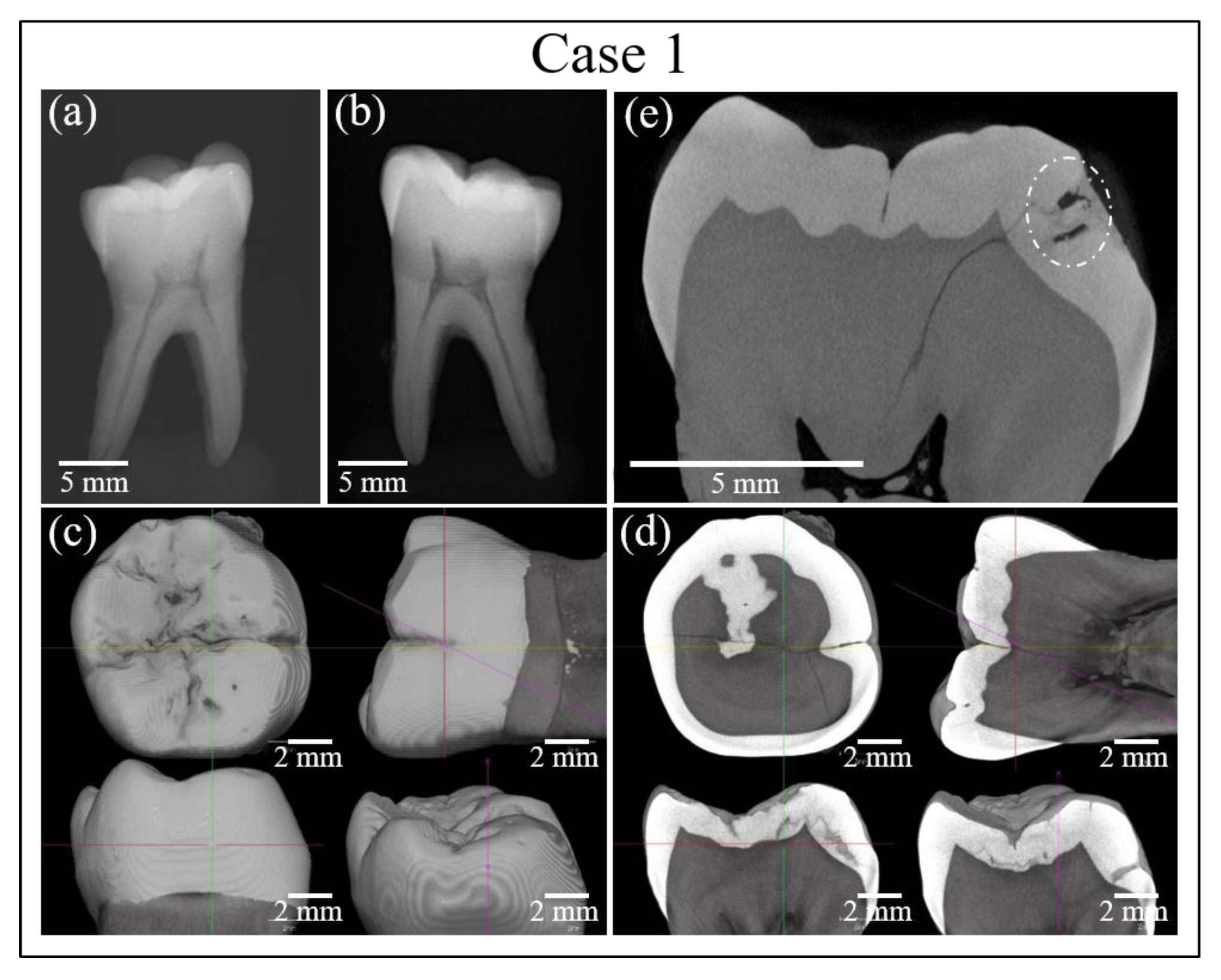
X-ray images of individual samples were obtained with an intraoral X-ray unit (Digora Optime UV, KaVo Dental Systems Co., Ltd., Berlin, Germany). The studied teeth were also subjected to micro CT imaging (inspeXio SMX-225CT, Shimadzu Co., Ltd., Kyoto-shi, Japan and/or CT Lab HX, Rigaku Co., Ltd., Tokyo, Japan). The reconstructed data sets were examined with three-dimensional data analysis software (TRI/3-D-BON, Ratoc System Engineering Co., Ltd., Tokyo, Japan and/or Materialise Mimics, Materialise NV, Leuven, Belgium).
2.4. Fluorescence Assessments of Caries
The caries diagnostic device DIAGNOdent™ pen (KaVo Dental, GmbH, Biberach, Germany) was employed for comparison at the same locations where Raman spectra were collected. This is a commercially available device that operates by irradiating the locations of suspected caries with laser light at 655 nm to produce fluorescent excitation at wavelengths of 670–800 nm [
20,
21,
22,
23,
24,
25]. The fluorescence method required preliminary calibrations, which were performed in accordance with the manufacturer’s instructions.
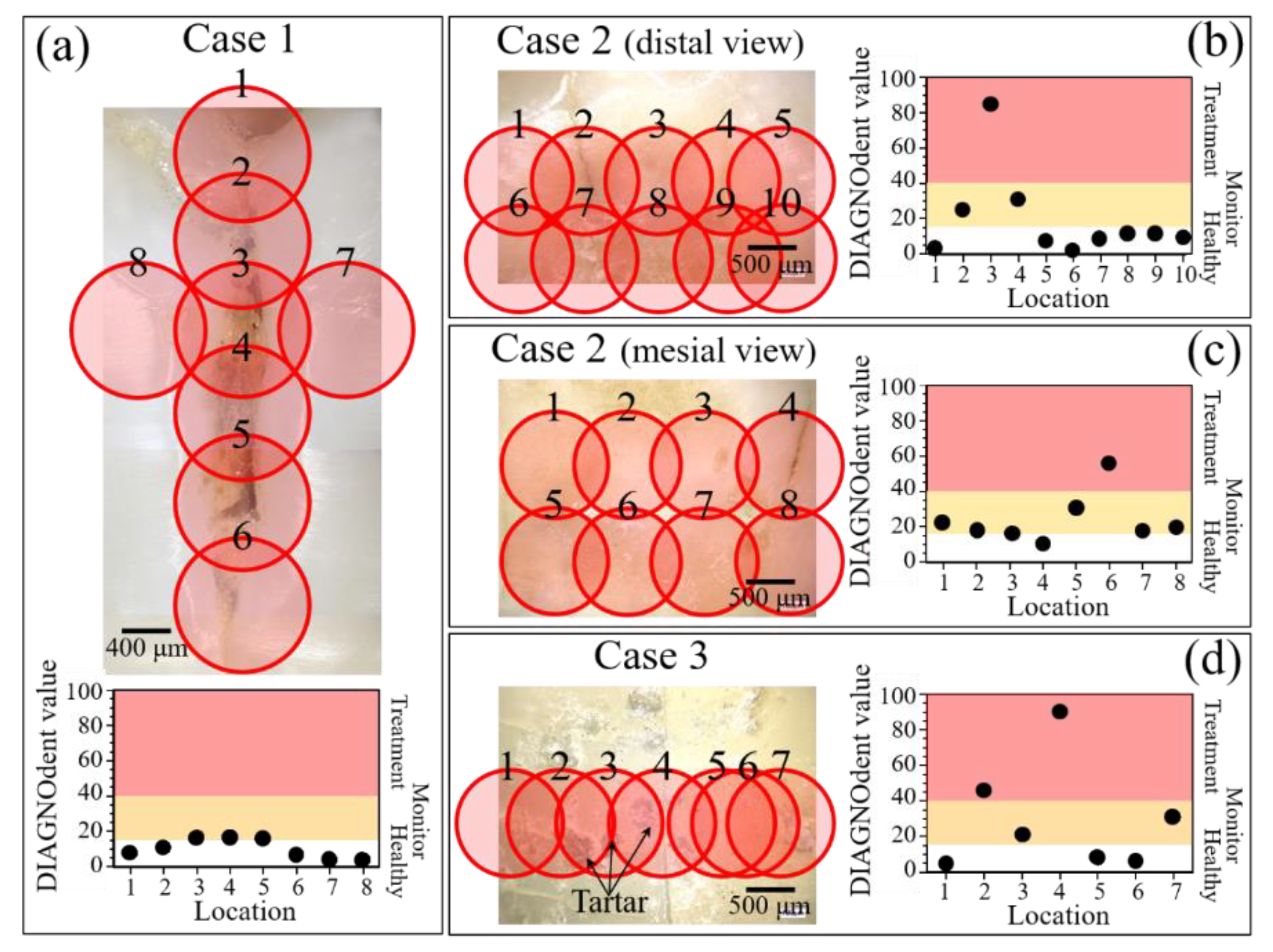
According to these instructions, DIAGNOdent values between 0 and 5 indicated healthy dentin, those between 5 and 40 were representative of initial caries requiring follow-up, and those >40 caries indicated requiring invasive treatment. In our analyses of enamel with suspected caries, we placed the narrow tip of the DIAGNOdent pen perpendicular to the tooth surface and shifted it parallel to the enamel surface to obtain line scans.
2.5. Raman Spectroscopy Experiments
Raman spectroscopic experiments were performed with a confocal Laser Raman microscope (RAMANtouch, Nanophoton Co., Ltd., Osaka, Japan). The excitation source was a green laser beam (532 nm) operating with a power of 200 mW. The power was set to an appropriate value by preliminary adjustment of ND filter and exposure time of the measurement. The microprobe used a 10x objective lens with a numerical aperture of 0.5. Confocal experiments were carried out with a pinhole aperture of 100 µm. The Raman instrument averaged data acquired at each spectral location over 4 successive measurement. Spectral deconvolution has been performed by means of an automatic fitting algorithm enclosed in the commercially available computational package (OriginLab 9.0; OriginLab Corporation, Northampton, MA, USA), using mixed Gaussian/Lorentzian curves. For the baseline, a polynomial function as been use with the same parameter for all the average spectra. Regarding the Raman images, 400 spectra were concurrently acquired on a straight line and images were generated by translating the line along a perpendicular direction.
4. Discussion
4.1. Linking the Raman Spectrum to the Severity of the Cavitated Zone
In previous works [
1,
6,
7], we have systematically and quantitatively monitored the evolution of tooth enamel demineralization according to the chemical formula, Ca
5-y(HPO
4)
y(PO
4)
3−y(OH)
1−y (H
2O)
y. This is a generally valid chemical representation of the enamel apatite structure in the presence of a fraction
y of Ca vacancies. This chemical equation is independent of the way Ca-vacancies form and of the local environment. We demonstrated that this equation maintains its validity in the early stages of tooth demineralization when, conceivably, only screw-axis Ca ions are removed. The structural disorder due to the formation of Ca vacancies (and represented by the stoichiometry parameter,
y) is quantitatively related to the broadening of the 960 cm
−1 apatite band, as both demineralization experiments and phonon density of states calculations have shown [
7]. Note that the vibrational band at 960 cm
−1 is not directly related to chemical bonds involving calcium; rather, the formation of Ca-vacancies creates a state of local disorder in the crystalline structure of hydroxyapatite, which alters the vibrational frequency of PO
43− tetrahedra. Such fluctuations in vibrational energy in turn lead to the observed band broadening. The relationship between the width of the 960 cm
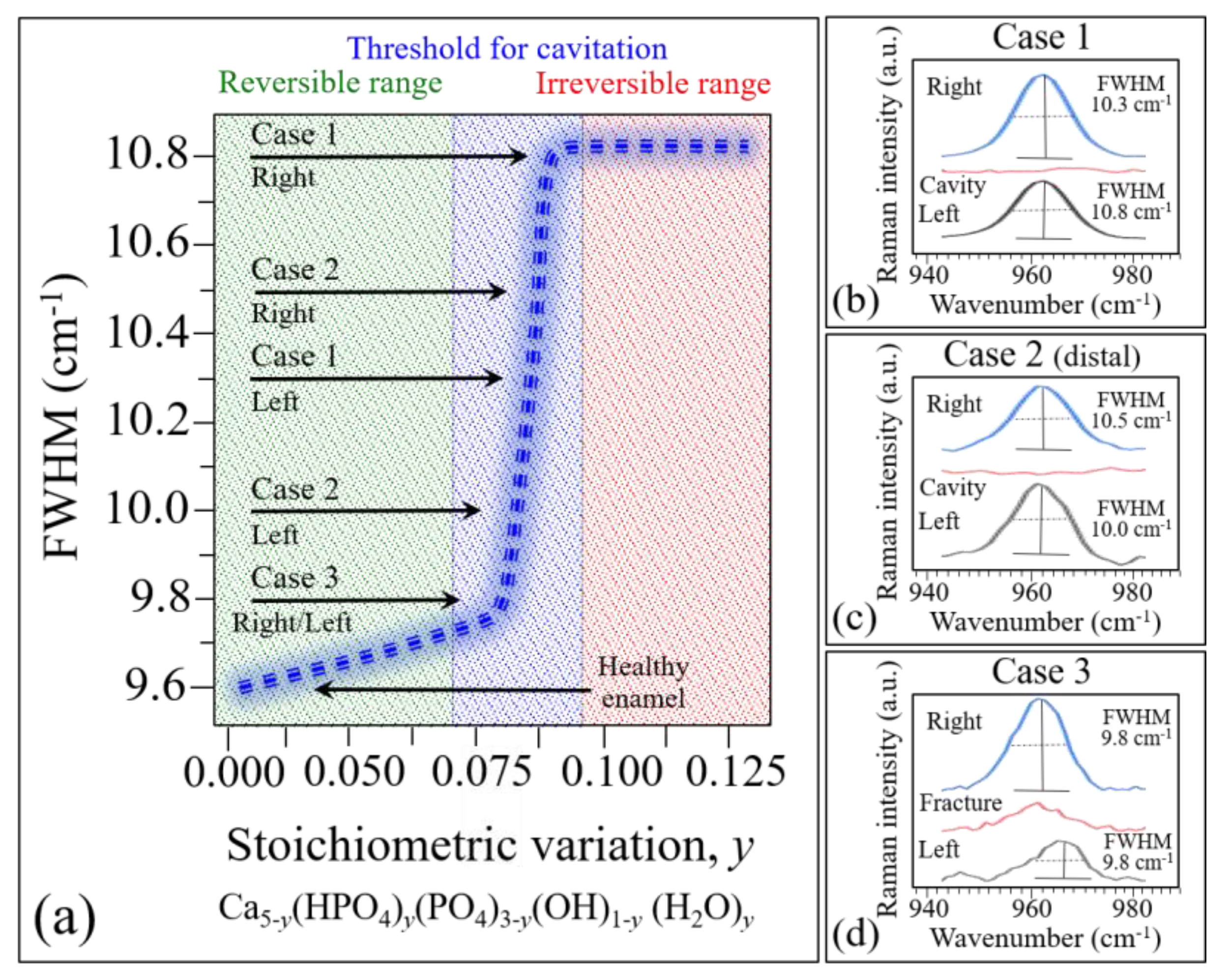
−1 Raman band and the stoichiometry parameter y is shown in
Figure 11a. According to this graph, the full width at half maximum (FWHM) increases linearly with increasing Ca
2+ off-stoichiometry in the hydroxyapatite structure up to a value of 0.08 (corresponding to the presence of ~0.75 mol.% of Ca
2+ vacancies). In this initial interval, the stoichiometry fluctuations are still reversible and can be healed through remineralization. The value
y = 0.08, however, represents a threshold value above which an abrupt increase in FWHM up to ~10.8 cm
-1 occurs until the parameter
y reaches approximately the value 0.1. Above this threshold, the stoichiometric damage is irreversible: a cavity can form and increase in volume over time. Note that the FWHM of the 960 cm
−1 Raman band in healthy enamel and that in a single perfectly stoichiometric hydroxyapatite crystal have been measured at ~9.8 and 9.6, respectively [
1]. The FWHM of the 960 cm
−1 band does not broaden further at
y > 0.1, but its band intensity abruptly decreases and, above a value of
y = 0.125, the Raman signal completely disappears. We shall henceforth use the dependence in
Figure 11a to interpret the present Raman data.
Average spectra were computed from experimental maps collected in three different areas of each of the three studied samples, as shown in
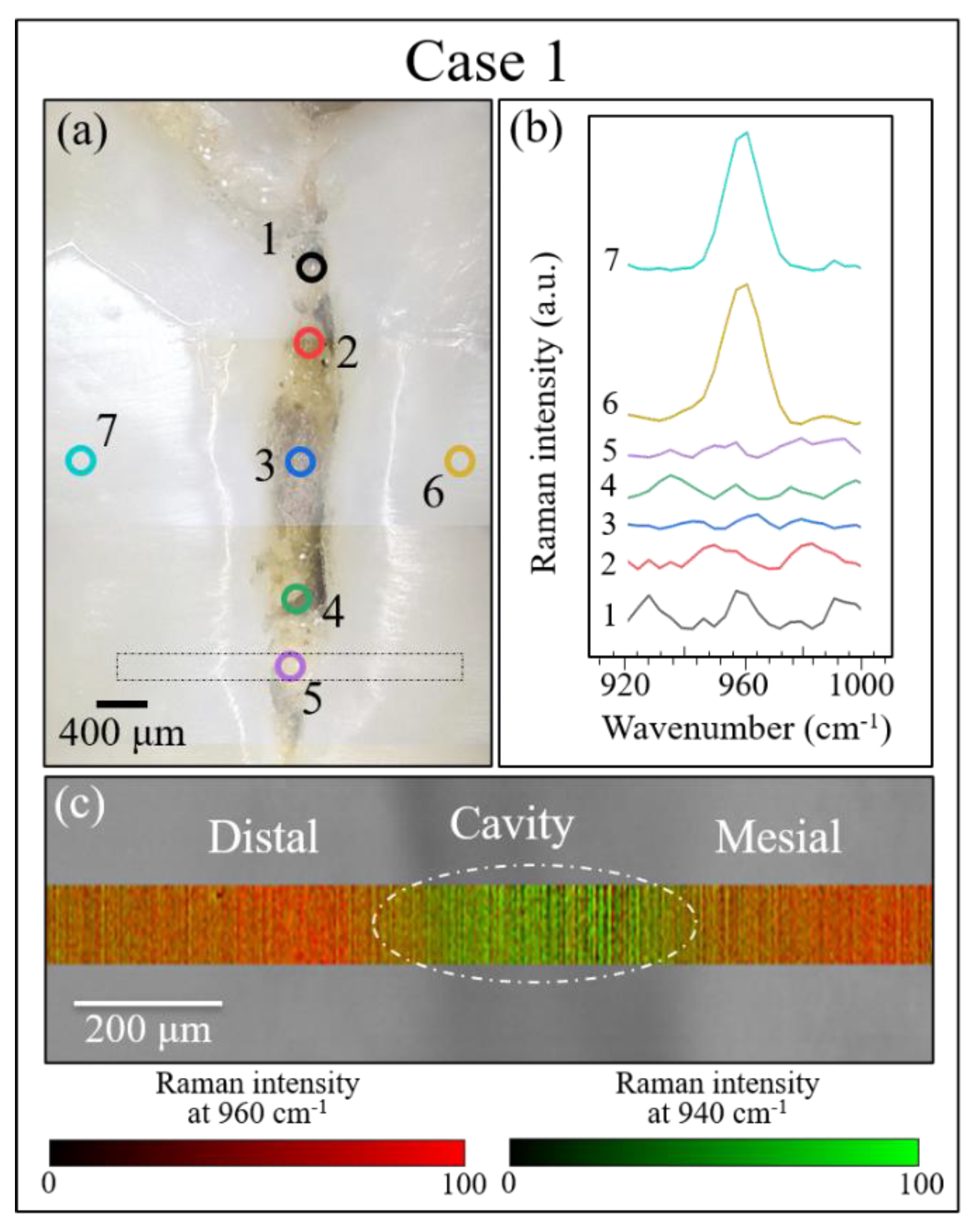
Figure 11b–d. According to the graph in Figure. 11a, the FWHM of average bands can be used to identify the stoichiometric state of a tooth and, accordingly, the severity of the disease in terms of its reversibility (i.e., the possibility of remineralization). According to this criterion, the average stoichiometric state in the right area (on the mesial side) of Case 1 was the most severe, as the tooth decay had reached an irreversible stage (cf. inset in
Figure 11a), while a similar evaluation of the left area (on the distal side) revealed a less severe disease state, as the tooth decay was yet at the threshold of irreversibility (cf.
Figure 8c) and
Figure 11a,b). Note that the evaluated areas were adjacent to the cavity, while the cavity area itself showed no apatite Raman signal, as expected due to the high level of damage (cf. average spectrum in
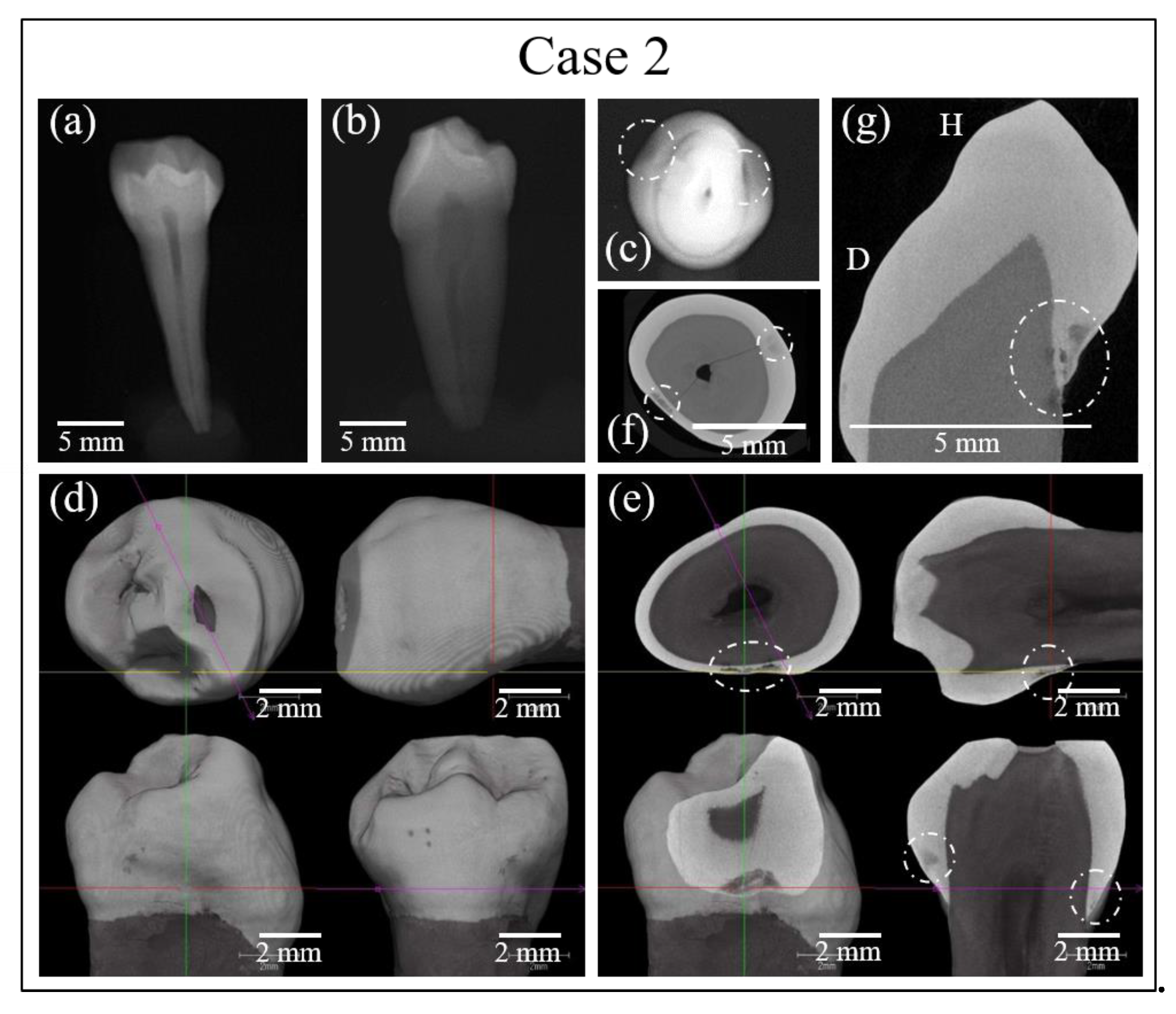
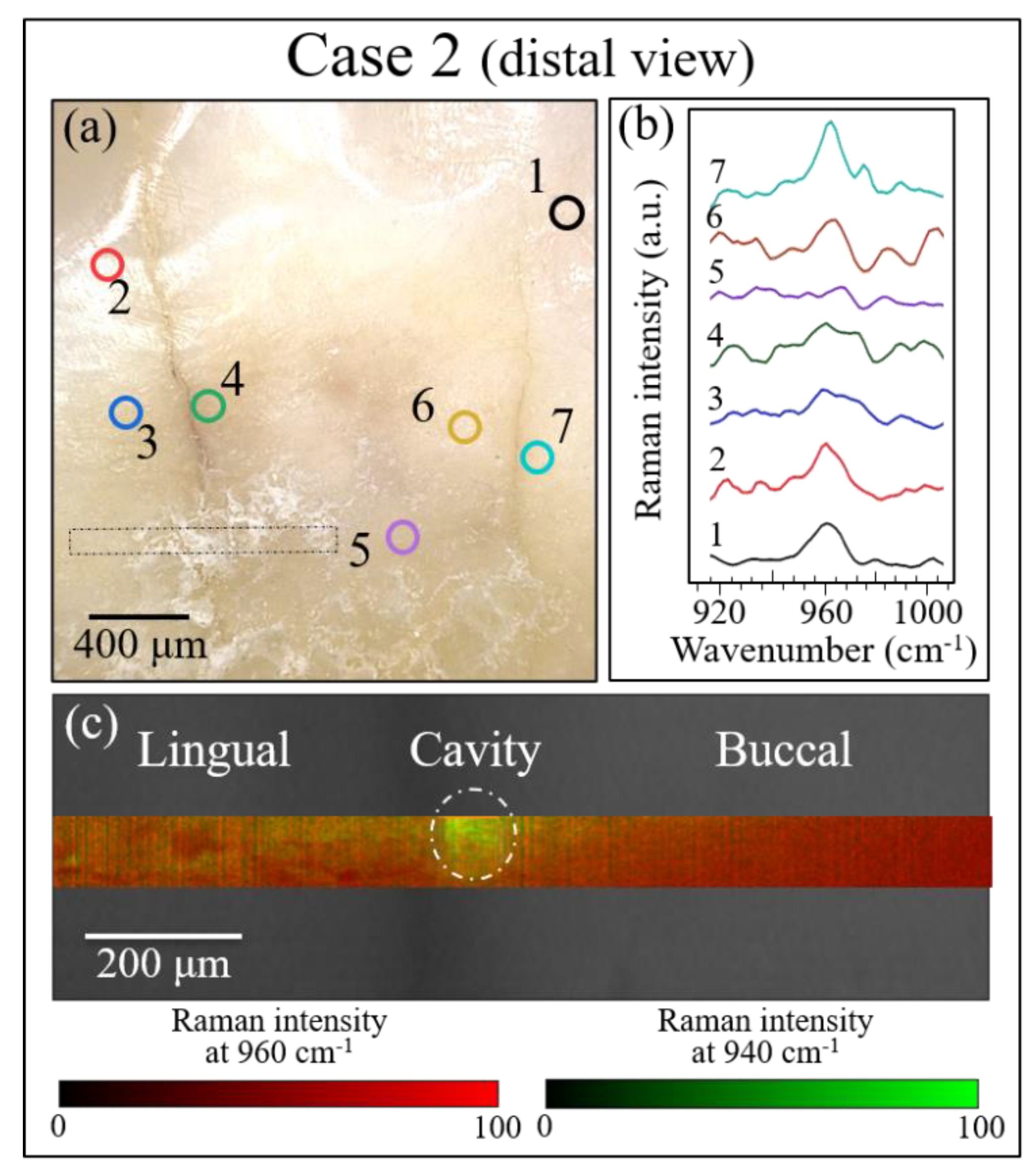
Figure 11b). The Case 2 sample exhibited a similar pattern, with no signal in the cavity zone of the disease, and clear off-stoichiometric states at the threshold for irreversibility in the adjacent right (buccal side) and left (lingual side) zones (cf.
Figure 9c and
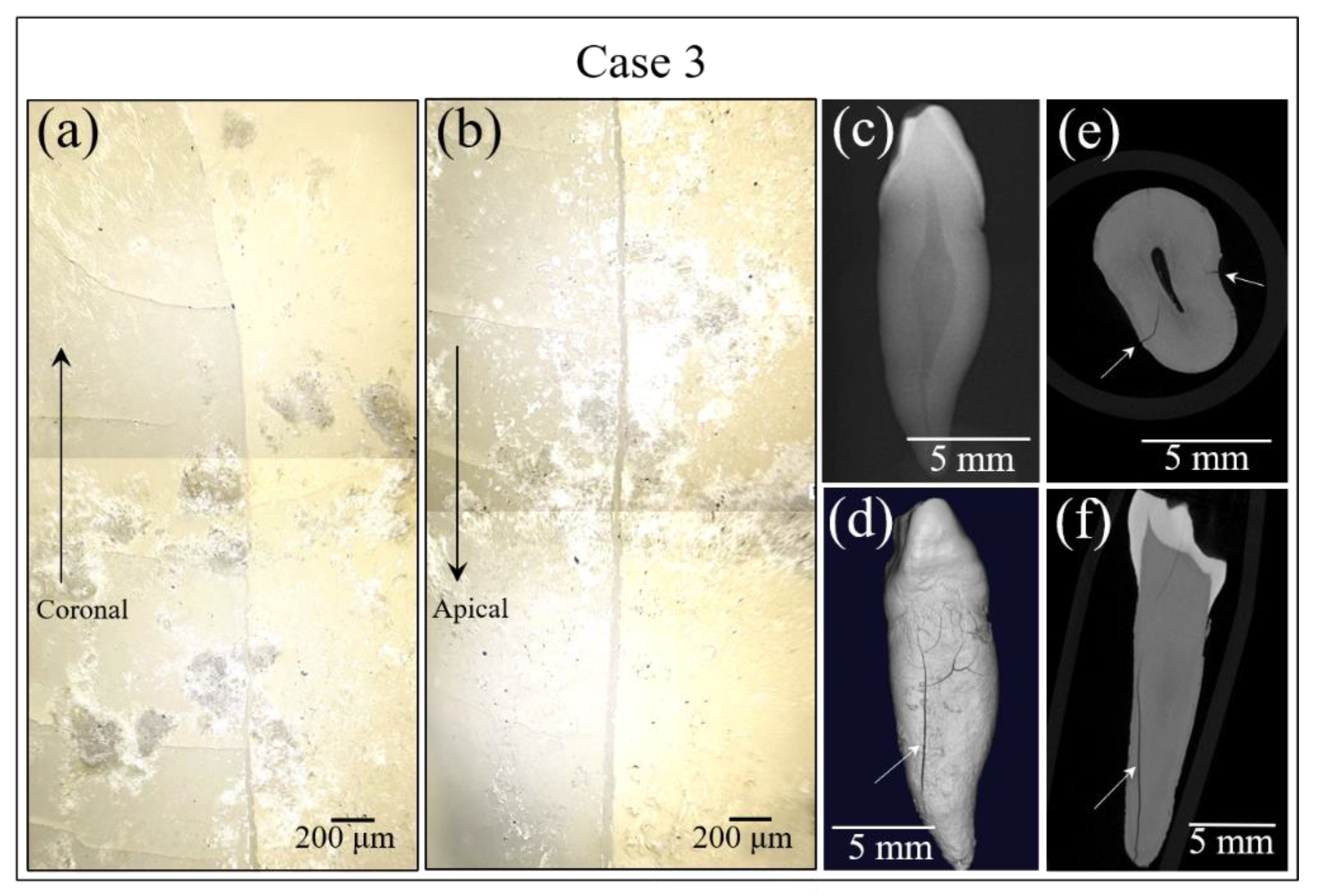
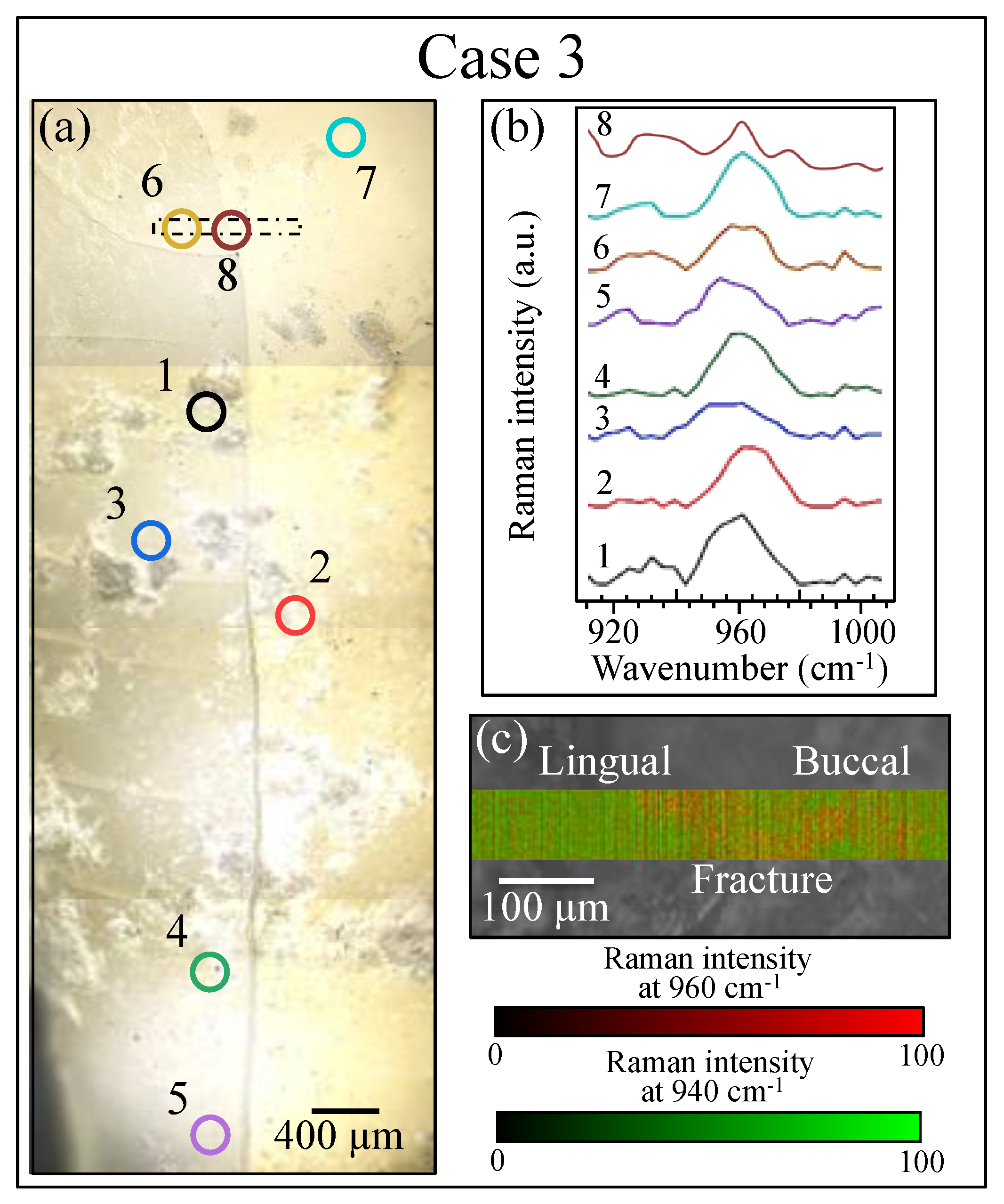
Figure 11a,c). Case 3 was the least severe among the three cases, as shown by its average spectra depicted in
Figure 11d. The Raman signal was still present in the cavity zone, though it was very weak, and its broadness indicated that the tooth decay had progressed into an irreversible state. In the adjacent right (buccal side) and left (lingual side) zones, however, the stoichiometric damage was yet at the limit of reversibility (cf.
Figure 10c and
Figure 11a,d). An interesting detail was the comparison between Location 8 of Case 3 in
Figure 10 and the correspondent Location 4 in
Figure 7d. The high fluorescence signal recorded in the latter would suggest a highly cavitated condition in need of treatment. However, the Raman spectrum recorded at this position (as shown in
Figure 10b) was among the sharpest (and thus the structurally healthiest) ones recorded in this study. We interpreted this discrepancy as a bias of the fluorescence measurement, which was influenced by the presence of tartar residues in the measurement zone and in its neighborhood.
Mapping of the hydroxyapatite structure at the molecular scale was performed in both enamel and dentin and was shown to be useful for locating buried cavities in zones where visual evaluation is difficult. Leaching of Ca2+ ions in decayed areas and the consequent formation of cavities are clearly linked to the altered vibrational behavior of PO43- tetrahedra in the hydroxyapatite structure, whose strongest signal corresponded to the P-O bond stretching at ~960 cm−1. Compared to that in healthy enamel, the P-O stretching Raman band clearly decreased in intensity and increased in breadth with increasing severity of tooth decay. A previously developed algorithm allowed us to quantitatively quote an off-stoichiometric chemical equation linking the FWHM of the 960 cm−1 Raman band to the chemistry of enamel demineralization and ultimately to the severity of sub-surface cavity development. Note that, although Raman data for healthy teeth samples generally display a bandwidth at ~9.6 cm−1 or less, this value might show a dependence on age, gender, and race. It, therefore, needs to be calibrated on individual patients at location of healthy enamel or dentin, or possibly be related to data from the same patient in time lapse.
4.2. The Usefulness of the Raman Approach in Preventive Dentistry
Enamel and dentine structures can be evaluated promptly by Raman spectroscopy at any point in their gradual evolution from a healthy state through increasing levels of demineralization related to the effect of incorrect alimentary habits or other pathological circumstances. The risk of tooth cavity formation could then be quantitatively classified by analyzing, at the molecular scale, the vibrational response of the main apatite scaffold present in the structures of both tooth enamel and dentine. The spectroscopic findings presented in this paper clearly demonstrate that the Raman method is useful not only as a diagnostic tool but also as a preventive one.
Progress in diagnostic dentistry requires more accurate risk assessment, earlier detection, and a better understanding of the biological development of dental caries. Recent efforts have focused on the prevention of tooth decay rather than surgical removal [
27]. New diagnostic strategies often fail to work as well as expected in the short term because clinicians lack experience in using these new tools as well as in interpreting their findings; new tools also present cost and safety issues. It should be noted that the micro-radiographic [
28], fiber-optic transillumination [
29], laser fluorescence [
30], and electrical conductance methods [
31] are not yet considered improvements on the traditional methods, because their results are not generalizable, because their ultimate outputs are prone to scatter, or because they are insufficiently safe [
32,
33]. Raman spectroscopy could represent a breakthrough as it outperforms all of these other methods in terms not only of performance but also of safety and cost, and could thus be the key to improving the state of oral health in modern societies, which is increasingly depressed due to newly developed eating patterns.
4.3. The Limitations of This Study
We offered here some clear proofs that the assessment of early enamel demineralization and dental caries is possible by Raman imaging. However, a dedicated instrument for intraoral assessments in medical practice is not yet available in the market. Such handheld instrument should be capable to provide both high sensitivity and sufficient spectral resolution for converting the Raman signal into a reliable and factual medical assessment. This is yet work in progress. Moreover, regarding the type of tooth, we have given extensive descriptions in previous published papers on the same topic (cf. Refs. 1, 6, and 7). However, assessments of deciduous teeth have yet to be performed. Although Ref. 7 suggests that it could be possible to design an experimental procedure addressing the stoichiometry parameter, y. This item has yet been beyond the achievements of the current study. Finally, the present study, as well as the previously published ones (as mentioned above), only refers to teeth collected on Japanese individuals. Note also that, according to ethical constrains in Japan as related to the research ethics committee, which also includes privacy issues, it is not allowed to link the obtained teeth to the age and/or the gender of the donor.

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










