Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects—A PRISMA Compliant Systematic Review and Meta-Analysis


 , , , ,
, , , ,  , and
, and 
Abstract
1. Introduction
2. Experimental Section
2.1. Research Question
- P
- Participants with class I and II gingival recession defects
- I
- Intervention with L-PRF with CAF
- C
- Comparison with CAF alone
- O
- Outcome variable, such as gingival thickness (GT), width of keratinized gingiva (WKG), % root coverage (%RC), clinical attachment level (CAL), recession depth (RD) or complete root coverage (CRC).
2.2. Search Methods
2.3. Selection Criteria
- Parallel or split-mouth randomized controlled trials (RCTs);
- Studies employing L-PRF in adjunct to CAF as test group comparing to use of CAF alone as control group for root coverage;
- Studies treating maxillary/mandibular class I or II gingival recession defects.
- Studies with participants free of any systemic diseases nor taking medications that could potentially influence the outcome of periodontal therapy;
- Studies with follow-up periods of 6 months.
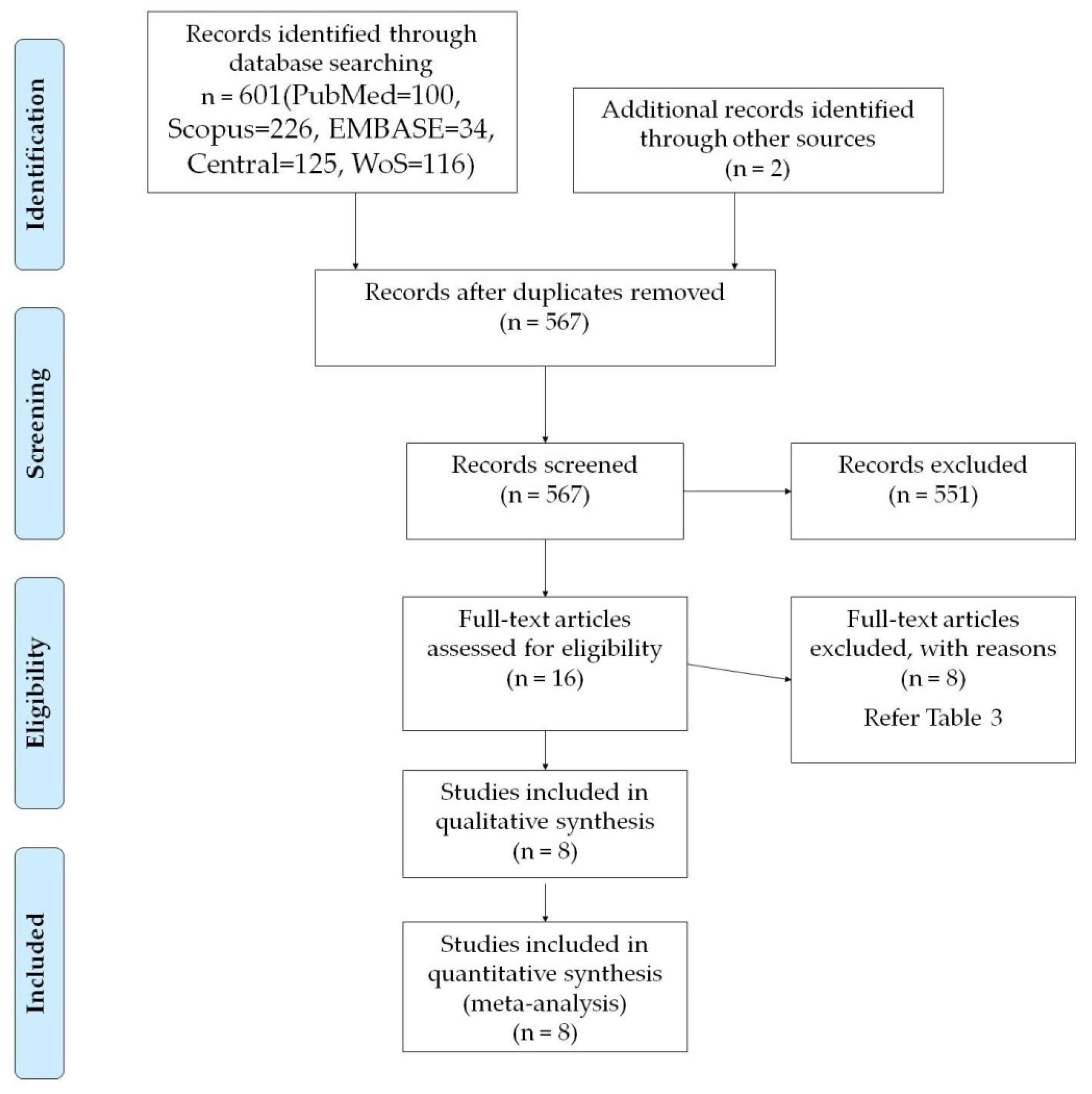
2.4. Selection of Studies
2.5. Data Extraction
- Demographic data of participants
- Type of gingival recession (multiple or single)
- Type of RCT and number of patients
- Type of equipment and protocol used for preparation of L-PRF
- Follow-up period
- Study sponsor and its setting
- Outcome variables, relative to baseline and postoperative recession defect characteristics e.g.: gingival thickness (GT), width of keratinized gingiva (WKG), % root coverage (%RC), clinical attachment level (CAL), recession depth (RD) and complete root coverage (CRC).
2.6. Data Synthesis
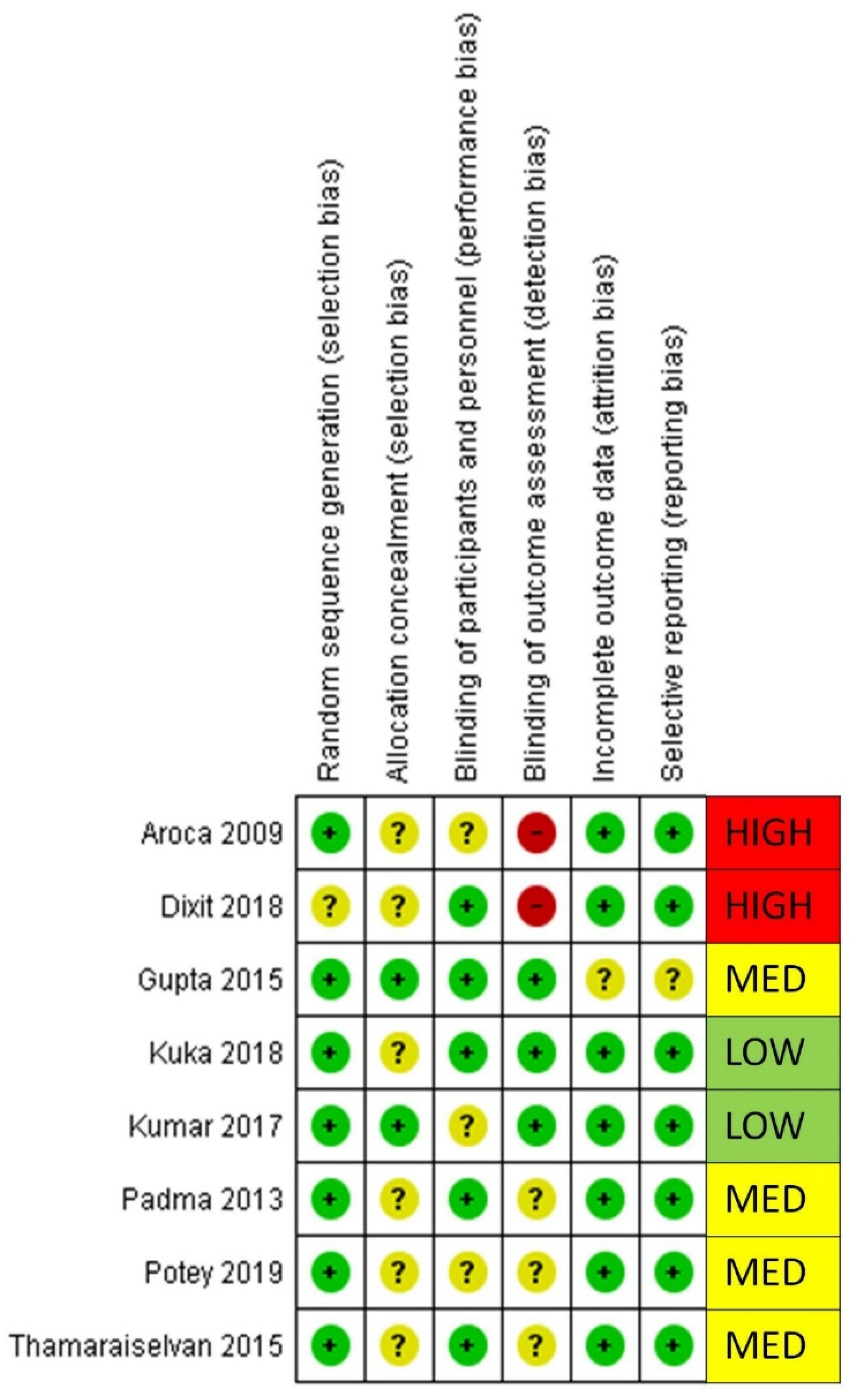
2.7. Risk of Bias Analysis
3. Results
3.1. Meta-Analysis
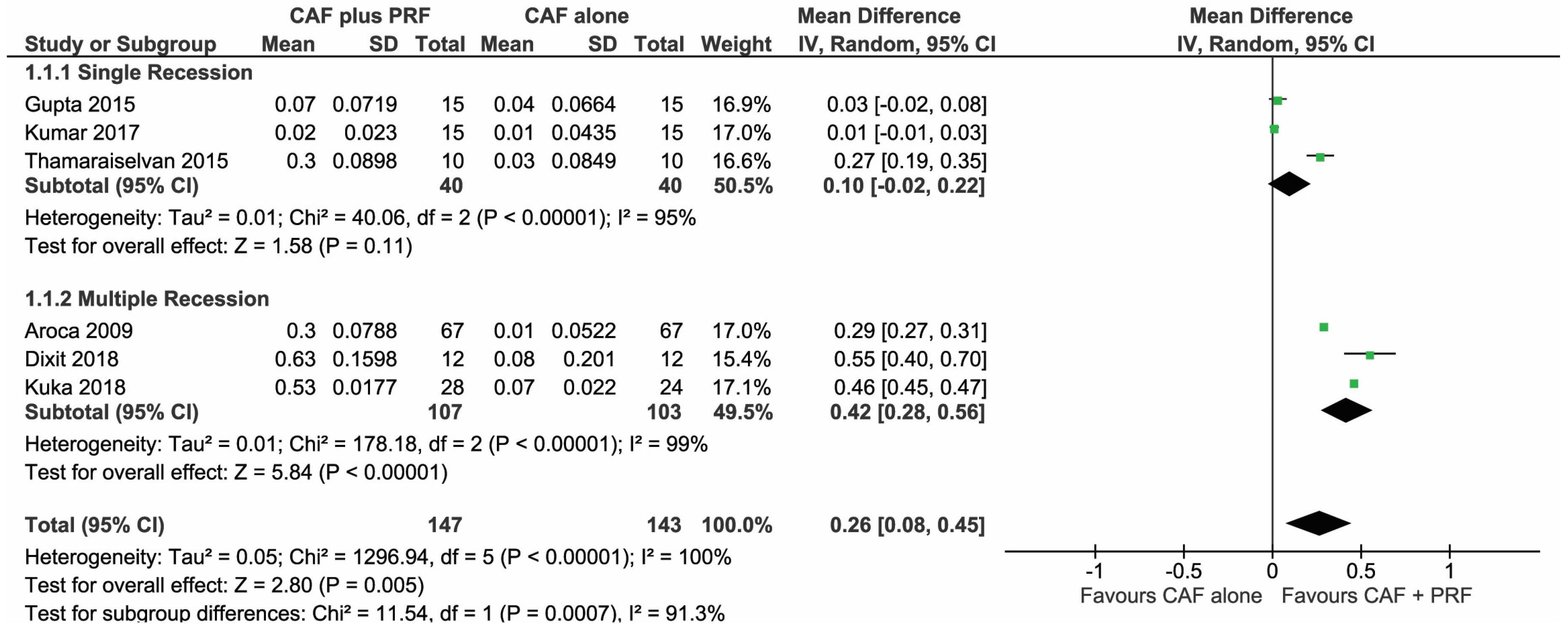
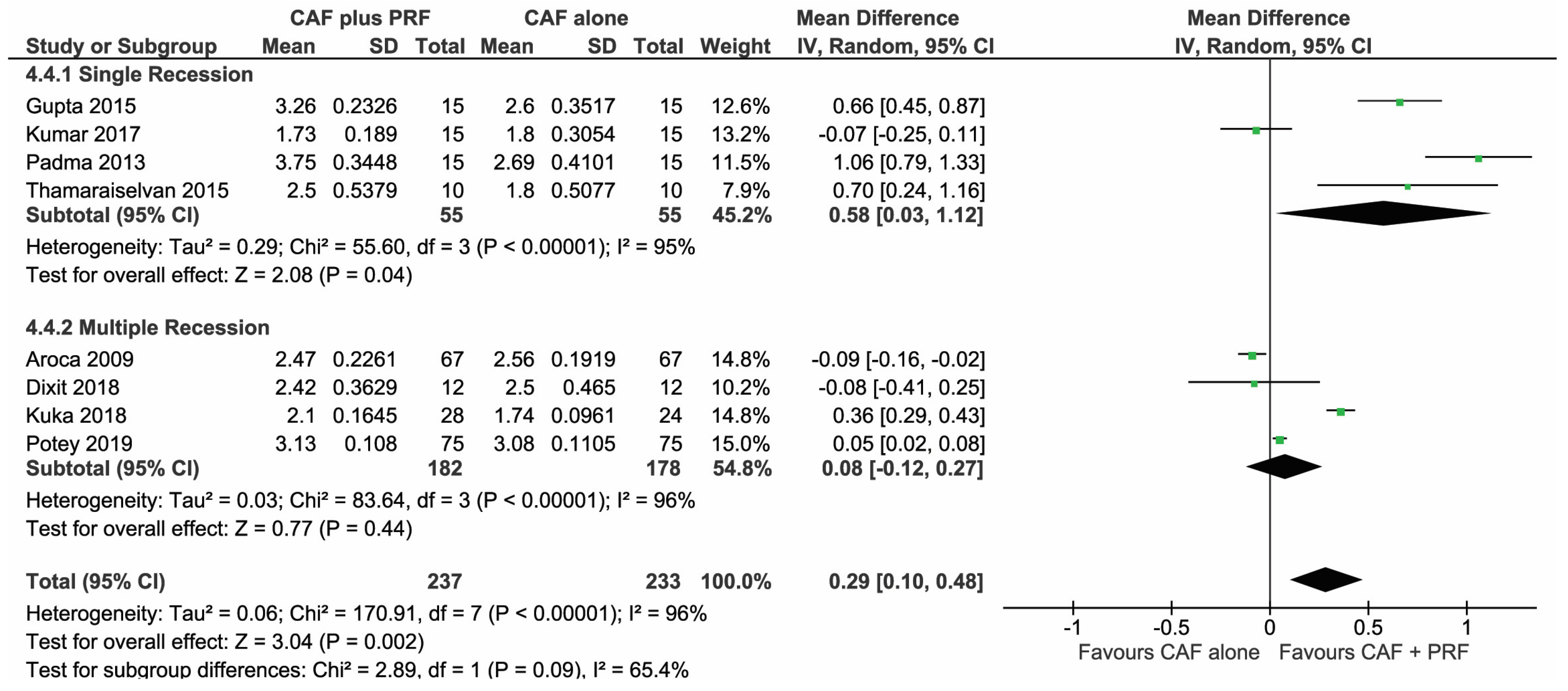
3.1.1. Change in Gingival Thickness (GT)
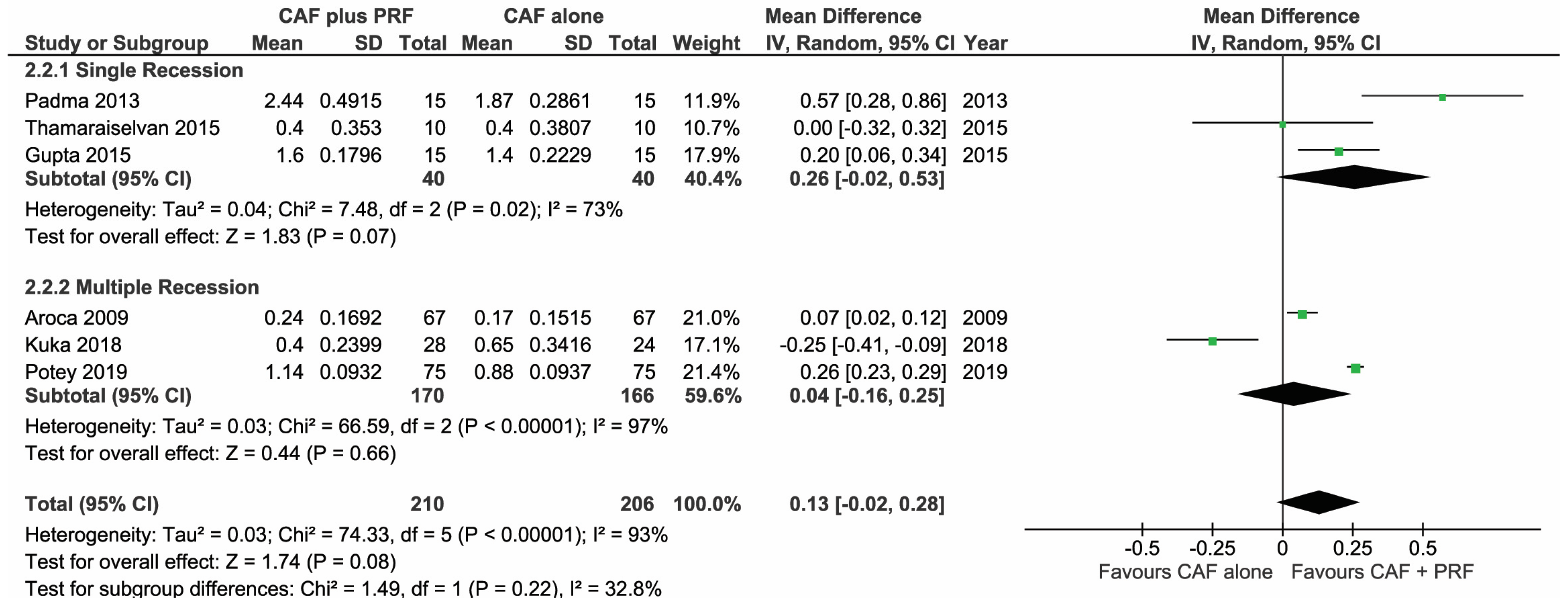
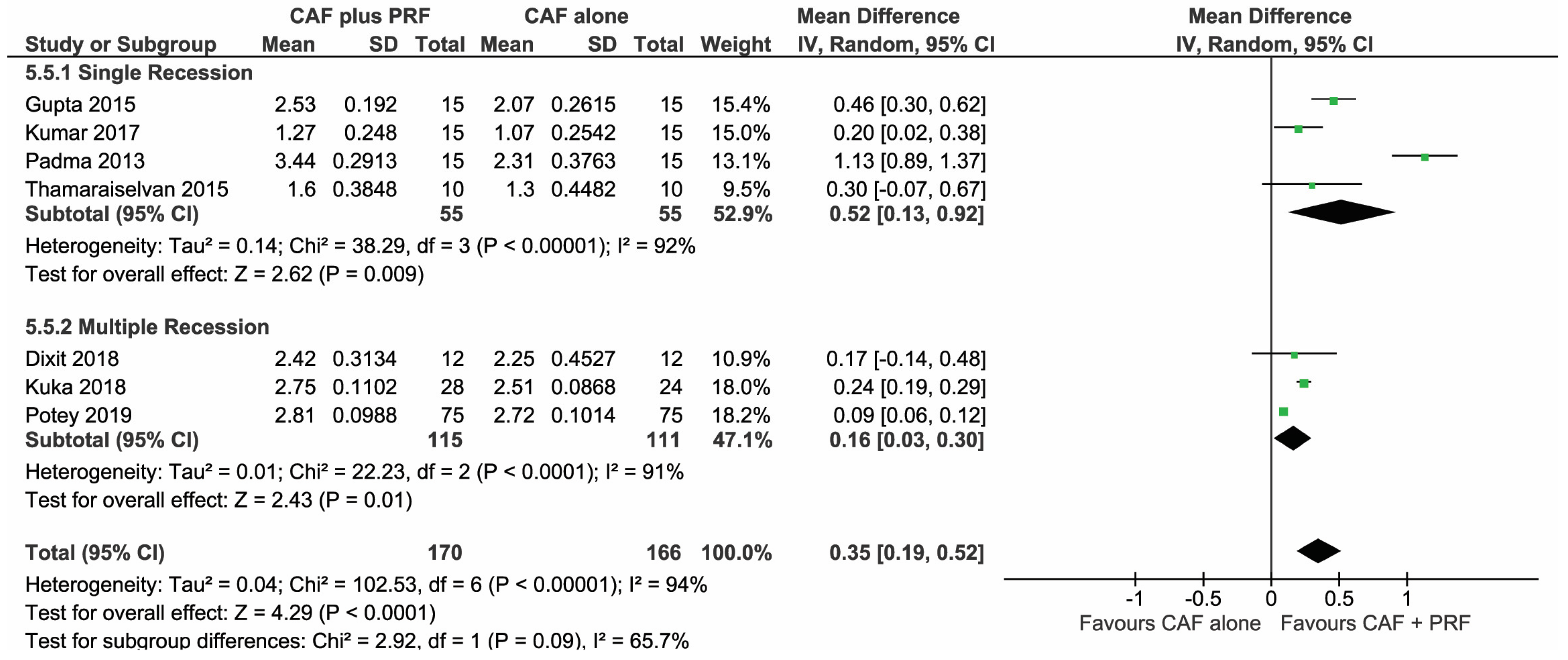
3.1.2. Change in Width of Keratinized Gingiva (WKG)
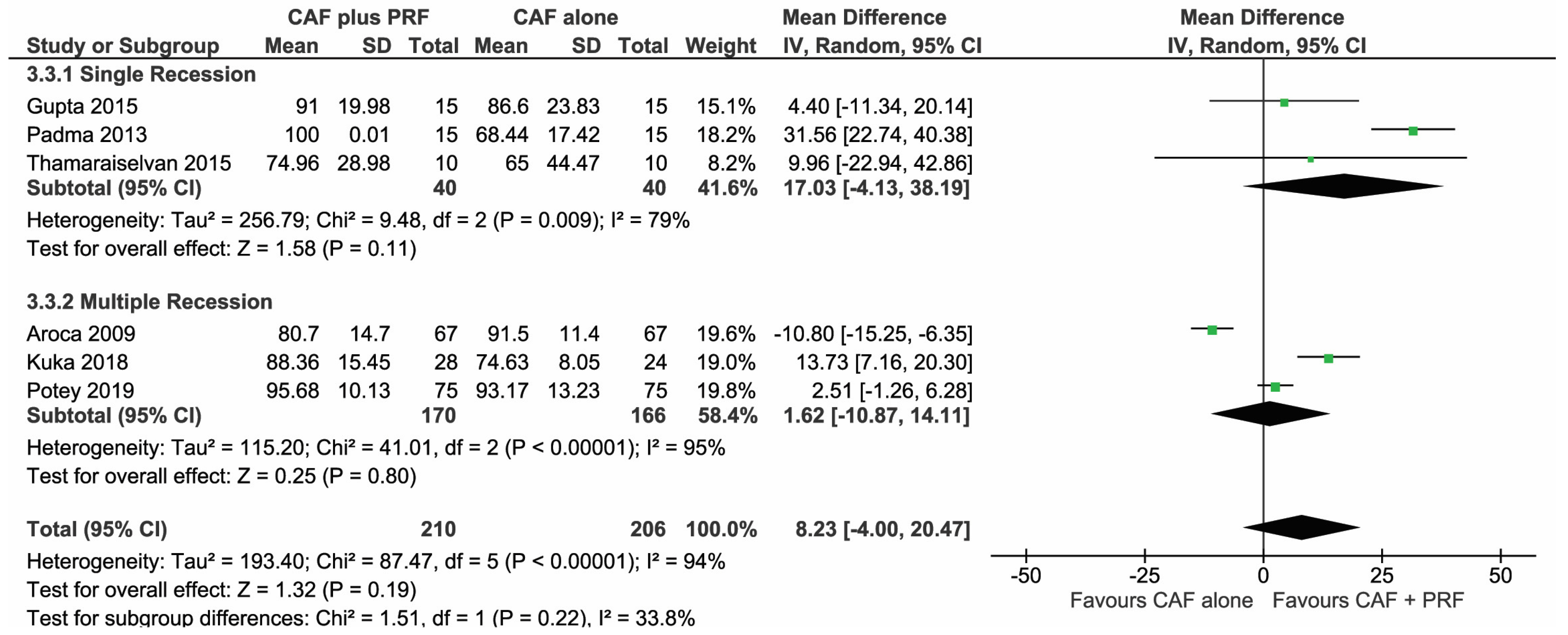
3.1.3. Change in Root Coverage Percentage (%RC)
3.1.4. Change in Clinical Attachment Level (CAL)
3.1.5. Change in Recession Depth (RD)
3.2. Effect of Preparation Protocol for L-PRF
3.3. Effect of Inclusion of Smokers
3.4. Effect of Modifications in CAF Procedure
3.5. Risk of Bias Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jati, A.S.; Furquim, L.Z.; Consolaro, A. Gingival recession: Its causes and types, and the importance of orthodontic treatment. Dent. Press J. Orthod. 2016, 21, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Kent, R.L.; DePaola, P.F. Gingival recession: Intra-oral distribution and associated factors. J. Periodontol. 1994, 65, 864–871. [Google Scholar] [CrossRef]
- Shkreta, M.; Atanasovska-Stojanovska, A.; Dollaku, B.; Belazelkoska, Z. Exploring the gingival recession surgical treatment modalities: A literature review. Open Access Maced. J. Med. Sci. 2018, 6, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, P.; Malet, J.; Borghetti, A. Decision-making in aesthetics: Root coverage revisited. Periodontol. 2000 2001, 27, 97–120. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Prato, G.P.; Clauser, C.; Cortellini, P. Guided tissue regeneration and a free gingival graft for the management of buccal recession: A case report. Int. J. Periodontics Restor. Dent. 1993, 13, 486–493. [Google Scholar]
- Nunn, M.E.; Miyamoto, T. Coronally advanced flaps (CAF) plus connective tissue graft (CTG) is the gold standard for treatment of Miller class I and II gingival defects. J. Evid. Based Dent. Pract. 2013, 13, 157–159. [Google Scholar] [CrossRef]
- Gupta, P.; Gupta, H. Comparative evaluation of envelope type of advanced flap with and without type I collagen membrane (NEOMEMTM) in the treatment of multiple buccal gingival recession defects: A clinical study. Indian J. Dent. 2014, 5, 190–198. [Google Scholar] [CrossRef]
- Tavelli, L.; Barootchi, S.; Di Gianfilippo, R.; Modarressi, M.; Cairo, F.; Rasperini, G.; Wang, H.-L. Acellular dermal matrix and coronally advanced flap or tunnel technique in the treatment of multiple adjacent gingival recessions. A 12-year follow-up from a randomized clinical trial. J. Clin. Periodontol. 2019, 46, 937–948. [Google Scholar] [CrossRef]
- Bolla, V.; Reddy, P.K.; Kalakonda, B.; Koppolu, P.; Manaswini, E. Coronally advanced flap with amniotic membrane in the treatment of gingival recession: Three case reports. Int. J. Appl. Basic Med. Res. 2019, 9, 111–114. [Google Scholar]
- Jankovic, S.; Aleksic, Z.; Milinkovic, I.; Dimitrijevic, B. The coronally advanced flap in combination with platelet-rich fibrin (PRF) and enamel matrix derivative in the treatment of gingival recession: A comparative study. Eur. J. Esthet. Dent. 2010, 5, 260–273. [Google Scholar] [PubMed]
- Biradar, S.M.; Satyanarayan, A.; Kulkarni, A.J.; Patti, B.; Mysore, S.K.; Patil, A. Clinical evaluation of the effect of platelet rich plasma on the coronally advanced flap root coverage procedure. Dent. Res. J. 2015, 12, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Nieri, M.; Pagliaro, U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J. Clin. Periodontol. 2014, 41 (Suppl. S15), S44–S62. [Google Scholar] [CrossRef] [PubMed]
- Hofmänner, P.; Alessandri, R.; Laugisch, O.; Aroca, S.; Salvi, G.E.; Stavropoulos, A.; Sculean, A. Predictability of surgical techniques used for coverage of multiple adjacent gingival recessions—A systematic review. Quintessence Int. 2012, 43, 545–554. [Google Scholar]
- Panda, S.; Panda, S.; Satpathy, A.; Das, A.C. Laterally pedicled flap and connective tissue graft for management of orthodontically inflicted gingival recession—A case report. Indian J. Public Health Res. Dev. 2019, 10, 1613–1616. [Google Scholar] [CrossRef]
- Panda, S.; Panda, S.; Das, A.C.; Mohanty, R. Modified coronally advanced flap procedure using orthodontic buttons: A case report. Indian J. Public Health Res. Dev. 2019, 10, 1665–1668. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e56–e60. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Karanxha, L.; Panda, S.; Bucchi, C.; Nadathur Doraiswamy, J.; Sankari, M.; Ramamoorthi, S.; Varghese, S.; Taschieri, S. Autologous platelet concentrates for treating periodontal infrabony defects. Cochrane Database Syst. Rev. 2018, 2018, CD011423. [Google Scholar] [CrossRef]
- Tonnesen, M.G.; Feng, X.; Clark, R.A. Angiogenesis in wound healing. J. Investig. Dermatol. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef]
- Eming, S.A.; Brachvogel, B.; Odorisio, T.; Koch, M. Regulation of angiogenesis: Wound healing as a model. Prog. Histochem. Cytochem. 2007, 42, 115–170. [Google Scholar] [CrossRef]
- Chatterjee, S.S.; Das, A.C.; Panda, S. Platelet rich fibrin: A promising innovation in periodontics. Indian J. Public Health Res. Dev. 2019, 10, 772–775. [Google Scholar] [CrossRef]
- Schär, M.O.; Diaz-Romero, J.; Kohl, S.; Zumstein, M.A.; Nesic, D. Platelet-rich concentrates differentially release growth factors and induce cell migration in vitro. Clin. Orthop. Relat. Res. 2015, 473, 1635–1643. [Google Scholar] [CrossRef] [PubMed]
- Borie, E.; Oliví, D.G.; Orsi, I.A.; Garlet, K.; Weber, B.; Beltrán, V.; Fuentes, R. Platelet-rich fibrin application in dentistry: A literature review. Int. J. Clin. Exp. Med. 2015, 8, 7922–7929. [Google Scholar]
- Eren, G.; Atilla, G. Platelet-rich fibrin in the treatment of localized gingival recessions: A split-mouth randomized clinical trial. Clin. Oral Investig. 2014, 18, 1941–1948. [Google Scholar] [CrossRef]
- Aleksić, Z.; Janković, S.; Dimitrijević, B.; Divnić-Resnik, T.; Milinković, I.; Leković, V. The use of platelet-rich fibrin membrane in gingival recession treatment. Srp. Arh. Celok. Lek. 2010, 138, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Mufti, S.; Dadawala, S.M.; Patel, P.; Shah, M.; Dave, D.H. Comparative evaluation of platelet-rich fibrin with connective tissue grafts in the treatment of Miller’s class I gingival recessions. Contemp. Clin. Dent. 2017, 8, 531–537. [Google Scholar]
- Cortellini, P.; Tonetti, M.; Baldi, C.; Francetti, L.; Rasperini, G.; Rotundo, R.; Nieri, M.; Franceschi, D.; Labriola, A.; Prato, G.P. Does placement of a connective tissue graft improve the outcomes of coronally advanced flap for coverage of single gingival recessions in upper anterior teeth? A multi-centre, randomized, double-blind, clinical trial. J. Clin. Periodontol. 2009, 36, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 67–82. [Google Scholar] [CrossRef]
- Li, R.; Liu, Y.; Xu, T.; Zhao, H.; Hou, J.; Wu, Y.; Zhang, D. The additional effect of autologous platelet concentrates to coronally advanced flap in the treatment of gingival recessions: A systematic review and meta-analysis. Available online: https://www.hindawi.com/journals/bmri/2019/2587245/ (accessed on 28 March 2020).
- Aroca, S.; Keglevich, T.; Barbieri, B.; Gera, I.; Etienne, D. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6-month study. J. Periodontol. 2009, 80, 244–252. [Google Scholar] [CrossRef]
- Padma, R.; Shilpa, A.; Kumar, P.A.; Nagasri, M.; Kumar, C.; Sreedhar, A. A split mouth randomized controlled study to evaluate the adjunctive effect of platelet-rich fibrin to coronally advanced flap in Miller’s class-I and II recession defects. J. Indian Soc. Periodontol. 2013, 17, 631–636. [Google Scholar]
- Dixit, N.; Lamba, A.K.; Faraz, F.; Tandon, S.; Aggarwal, K.; Ahad, A. Root coverage by modified coronally advanced flap with and without platelet-rich fibrin: A clinical study. Indian J. Dent. Res. 2018, 29, 600–604. [Google Scholar] [PubMed]
- Potey, A.M.; Kolte, R.A.; Kolte, A.P.; Mody, D.; Bodhare, G.; Pakhmode, R. Coronally advanced flap with and without platelet-rich fibrin in the treatment of multiple adjacent recession defects: A randomized controlled split-mouth trial. J. Indian Soc. Periodontol. 2019, 23, 436–441. [Google Scholar]
- Gupta, S.; Banthia, R.; Singh, P.; Banthia, P.; Raje, S.; Aggarwal, N. Clinical evaluation and comparison of the efficacy of coronally advanced flap alone and in combination with platelet rich fibrin membrane in the treatment of Miller Class I and II gingival recessions. Contemp. Clin. Dent. 2015, 6, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Thamaraiselvan, M.; Elavarasu, S.; Thangakumaran, S.; Gadagi, J.S.; Arthie, T. Comparative clinical evaluation of coronally advanced flap with or without platelet rich fibrin membrane in the treatment of isolated gingival recession. J. Indian Soc. Periodontol. 2015, 19, 66–71. [Google Scholar] [CrossRef]
- Kumar, A.; Bains, V.K.; Jhingran, R.; Srivastava, R.; Madan, R.; Rizvi, I. Patient-centered microsurgical management of gingival recession using coronally advanced flap with either platelet-rich fibrin or connective tissue graft: A comparative analysis. Contemp. Clin. Dent. 2017, 8, 293–304. [Google Scholar] [PubMed]
- Kuka, S.; Ipci, S.D.; Cakar, G.; Yılmaz, S. Clinical evaluation of coronally advanced flap with or without platelet-rich fibrin for the treatment of multiple gingival recessions. Clin. Oral Investig. 2018, 22, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Pinto, N.; Quirynen, M. Letter to the editor: RE: Optimized platelet-rich fibrin with the low-speed concept: Growth factor release, biocompatibility, and cellular response. J. Periodontol. 2019, 90, 119–121. [Google Scholar] [CrossRef]
- Panda, S.; Karanxha, L.; Goker, F.; Satpathy, A.; Taschieri, S.; Francetti, L.; Das, A.C.; Kumar, M.; Panda, S.; Fabbro, M.D. Autologous platelet concentrates in treatment of furcation defects—A systematic review and meta-analysis. Int. J. Mol. Sci. 2019, 20, 1347. [Google Scholar] [CrossRef]
- Panda, S.; Sankari, M.; Satpathy, A.; Jayakumar, D.; Mozzati, M.; Mortellaro, C.; Gallesio, G.; Taschieri, S.; Del Fabbro, M. Adjunctive effect of autologus platelet-rich fibrin to barrier membrane in the treatment of periodontal intrabony defects. J. Craniofac. Surg. 2016, 27, 691–696. [Google Scholar] [CrossRef]
- Strauss, F.-J.; Nasirzade, J.; Kargarpoor, Z.; Stähli, A.; Gruber, R. Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: A systematic review of in vitro studies. Clin. Oral Investig. 2020, 24, 569–584. [Google Scholar] [CrossRef]
- Tsai, C.-H.; Shen, S.-Y.; Zhao, J.-H.; Chang, Y.-C. Platelet-rich fibrin modulates cell proliferation of human periodontally related cells in vitro. J. Dent. Sci. 2009, 4, 130–135. [Google Scholar] [CrossRef]
- Pini Prato, G.; Pagliaro, U.; Baldi, C.; Nieri, M.; Saletta, D.; Cairo, F.; Cortellini, P. Coronally advanced flap procedure for root coverage. Flap with tension versus flap without tension: A randomized controlled clinical study. J. Periodontol. 2000, 71, 188–201. [Google Scholar] [CrossRef] [PubMed]
- Malenica, M.; Prnjavorac, B.; Bego, T.; Dujic, T.; Semiz, S.; Skrbo, S.; Gusic, A.; Hadzic, A.; Causevic, A. Effect of cigarette smoking on haematological parameters in healthy population. Med. Arch. 2017, 71, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Pini-Prato, G.; Magnani, C.; Zaheer, F.; Rotundo, R.; Buti, J. Influence of inter-dental tissues and root surface condition on complete root coverage following treatment of gingival recessions: A 1-year retrospective study. J. Clin. Periodontol. 2015, 42, 567–574. [Google Scholar] [CrossRef]
- Bayer, A.; Tohidnezhad, M.; Lammel, J.; Lippross, S.; Behrendt, P.; Klüter, T.; Pufe, T.; Jahr, H.; Cremer, J.; Rademacher, F.; et al. Platelet-released growth factors induce differentiation of primary keratinocytes. Available online: https://www.hindawi.com/journals/mi/2017/5671615/ (accessed on 30 March 2020).
- Xian, L.J.; Chowdhury, S.R.; Bin Saim, A.; Idrus, R.B.H. Concentration-dependent effect of platelet-rich plasma on keratinocyte and fibroblast wound healing. Cytotherapy 2015, 17, 293–300. [Google Scholar] [CrossRef]
- Pini Prato, G.P.; Baldi, C.; Nieri, M.; Franseschi, D.; Cortellini, P.; Clauser, C.; Rotundo, R.; Muzzi, L. Coronally advanced flap: The post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J. Periodontol. 2005, 76, 713–722. [Google Scholar] [CrossRef]
- Miron, R.; Choukroun, J.; Ghanaati, S. Controversies related to scientific report describing g-forces from studies on platelet-rich fibrin: Necessity for standardization of relative centrifugal force values. Int. J. Growth Factors Stem Cells Dent. 2018, 1, 80. [Google Scholar] [CrossRef]
- Pini Prato, G.; Tinti, C.; Vincenzi, G.; Magnani, C.; Cortellini, P.; Clauser, C. Guided tissue regeneration versus mucogingival surgery in the treatment of human buccal gingival recession. J. Periodontol. 1992, 63, 919–928. [Google Scholar] [CrossRef]
- Khorshidi, H.; Raoofi, S.; Bagheri, R.; Banihashemi, H. Comparison of the mechanical properties of early leukocyte- and platelet-rich fibrin versus PRGF/Endoret membranes. Int. J. Dent. 2016, 2016, 1849207. [Google Scholar] [CrossRef]
- Dohan, E.; de Peppo, G.M.; Doglioli, P.; Sammartino, G. Slow release of growth factors and thrombospondin-1 in Choukroun’s platelet-rich fibrin (PRF): A gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors 2009, 27, 63–69. [Google Scholar] [CrossRef]
- Castro, A.B.; Herrero, E.R.; Slomka, V.; Pinto, N.; Teughels, W.; Quirynen, M. Antimicrobial capacity of Leucocyte-and Platelet Rich Fibrin against periodontal pathogens. Sci. Rep. 2019, 9, 81–88. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author & Year | Recession Type | No. of Patients | Smoker | Defects (Test/ Control) | Age Range | Male/ Female | Follow-up (Months) | Complete Root Coverage (CRC) | |
|---|---|---|---|---|---|---|---|---|---|
| Test | Control | ||||||||
| Aroca et al. 2009 [24] | Multiple | 20 | Yes | 67/67 | 22–47 | 5/5 | 1, 3 & 6 | 35/67 | 50/67 |
| Padma et al. 2012 [25] | Single | 15 | No | 15/15 | 18–35 | NR | 1, 3 & 6 | 15/15 | 0/15 |
| Gupta et al. 2015 [26] | Single | 26 | No | 15/15 | 20–50 | 16/10 | 3 & 6 | 12/15 | 11/15 |
| Thamaraiselvan et al. 2015 [27] | Single | 20 | No | 10/10 | 21–47 | 18/2 | 6 | 5/10 | 5/10 |
| Kumar A et al. 2017 [28] | Single | 36 | No | 15/15 | 25–45 | 34/2 | 3 & 6 | 9/15 | 4/15 |
| Dixit N et al. 2018 [29] | Multiple | 12 | No | 12/12 | 18–50 | 7/5 | 3 & 6 | NR | NR |
| Kuka S et al. 2018 [30] | Multiple | 24 | No | 28/24 | 21–41 | 11/13 | 12 | 15/28 | 8/24 |
| Potey et al. 2019 [31] | Multiple | 20 | No | 75/75 | 22–47 | 16/4 | 3 & 6 | 62/75 | 59/75 |
| Author and Year | Study Design | Intervention Type | PRF Preparation Protocol | |||
|---|---|---|---|---|---|---|
| Test | Control | Equipment | Speed (RPM) | Time (min) | ||
| Aroca et al. 2009 [24] | Split Mouth | MCAF with L-PRF | MCAF | EBA 20 Centrifuge, Hettich, Tuttlingen, Germany | 3000 | 10 |
| Padma et al. 2012 [25] | Split Mouth | CAF with L-PRF | CAF | Not Mentioned | 3000 | 10 |
| Gupta et al. 2015 [26] | Parallel | CAF with L-PRF | CAF | REMI centrifuge, REMI Labs, India | 2700 | 12 |
| Thamaraiselvan et al. 2015 [27] | Parallel | CAF with L-PRF | CAF | Not Mentioned | 3000 | 10 |
| Kumar A et al. 2017 [28] | Parallel | CAF with L-PRF | CAF | Not Mentioned | 3000 | 10 |
| Dixit N et al. 2018 [29] | Split-mouth | CAF with L-PRF | CAF | Not Mentioned | 2700 | 12 |
| Kuka S et al. 2018 [30] | Parallel | CAF with L-PRF | CAF | EBA 20 centrifuge, | 3000 | 10 |
| Hettich, Tutlingen, Germany | ||||||
| Potey et al. 2019 [31] | Split Mouth | CAFB with L-PRF | CAFB | Not Mentioned | 3000 | 10 |
| Author and Year | Reason for Exclusion |
|---|---|
| Jankovic et al. 2010 [32] | Comparison with Enamel Matrix Derivative |
| Jankovic et al. 2012 [33] | Comparison with Connective Tissue Graft |
| Patel et al. 2018 [34] | Comparison between microsurgical and conventional technique |
| Rehan et al. 2018 [35] | Comparison with amniotic membrane |
| Ramireddy et al. 2018 [36] | Treatment of recession by glass ionomer cement and L-PRF |
| Brignardello 2018 [37] | Uncertain Randomization and Blinding |
| Culhauglu et al. 2018 [38] | Dose dependant L-PRF vs. Connective Tissue Graft |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panda, S.; Satpathy, A.; Chandra Das, A.; Kumar, M.; Mishra, L.; Gupta, S.; Srivastava, G.; Lukomska-Szymanska, M.; Taschieri, S.; Del Fabbro, M. Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects—A PRISMA Compliant Systematic Review and Meta-Analysis. Materials 2020, 13, 4314. https://doi.org/10.3390/ma13194314
Panda S, Satpathy A, Chandra Das A, Kumar M, Mishra L, Gupta S, Srivastava G, Lukomska-Szymanska M, Taschieri S, Del Fabbro M. Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects—A PRISMA Compliant Systematic Review and Meta-Analysis. Materials. 2020; 13(19):4314. https://doi.org/10.3390/ma13194314
Chicago/Turabian StylePanda, Saurav, Anurag Satpathy, Abhaya Chandra Das, Manoj Kumar, Lora Mishra, Swati Gupta, Gunjan Srivastava, Monika Lukomska-Szymanska, Silvio Taschieri, and Massimo Del Fabbro. 2020. "Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects—A PRISMA Compliant Systematic Review and Meta-Analysis" Materials 13, no. 19: 4314. https://doi.org/10.3390/ma13194314
APA StylePanda, S., Satpathy, A., Chandra Das, A., Kumar, M., Mishra, L., Gupta, S., Srivastava, G., Lukomska-Szymanska, M., Taschieri, S., & Del Fabbro, M. (2020). Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects—A PRISMA Compliant Systematic Review and Meta-Analysis. Materials, 13(19), 4314. https://doi.org/10.3390/ma13194314