A New Proposal: A Digital Flow for the Construction of a Haas-Inspired Rapid Maxillary Expander (HIRME)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
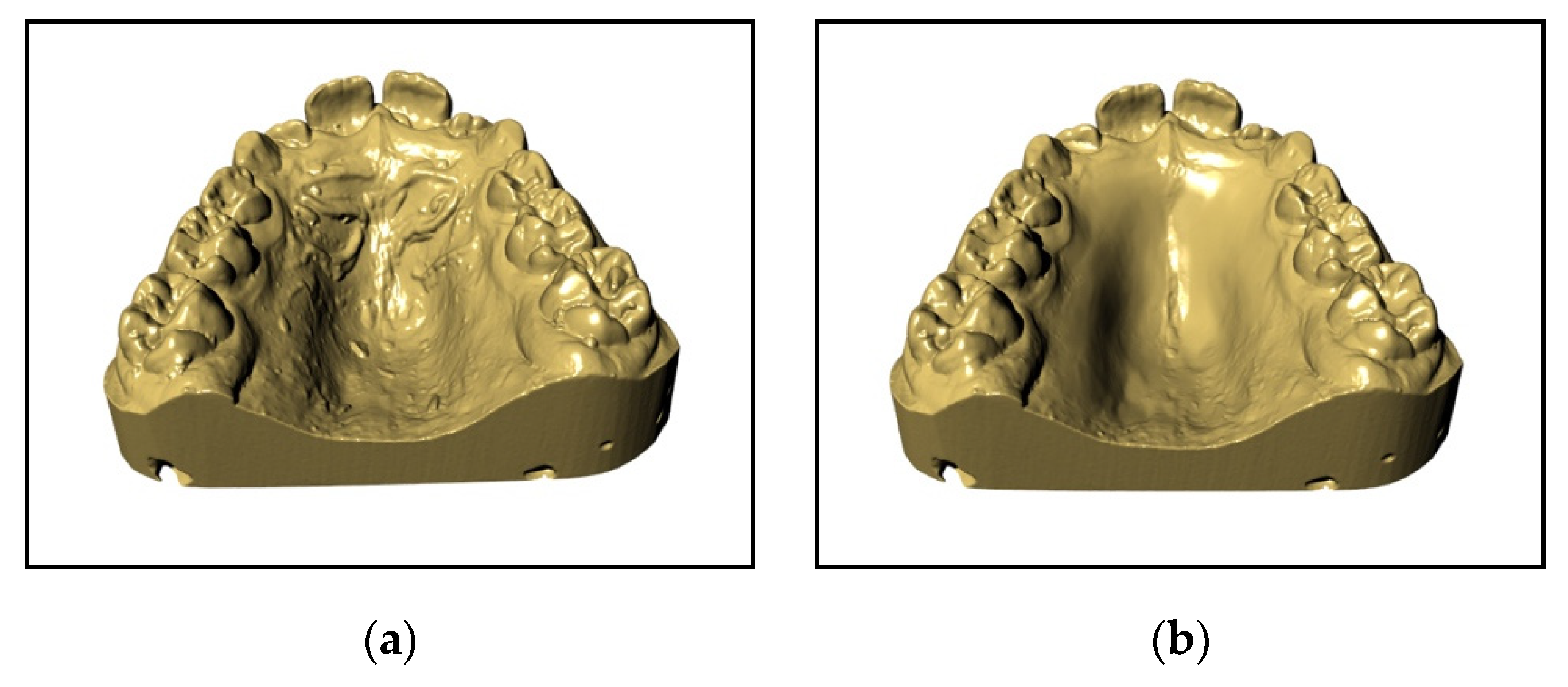
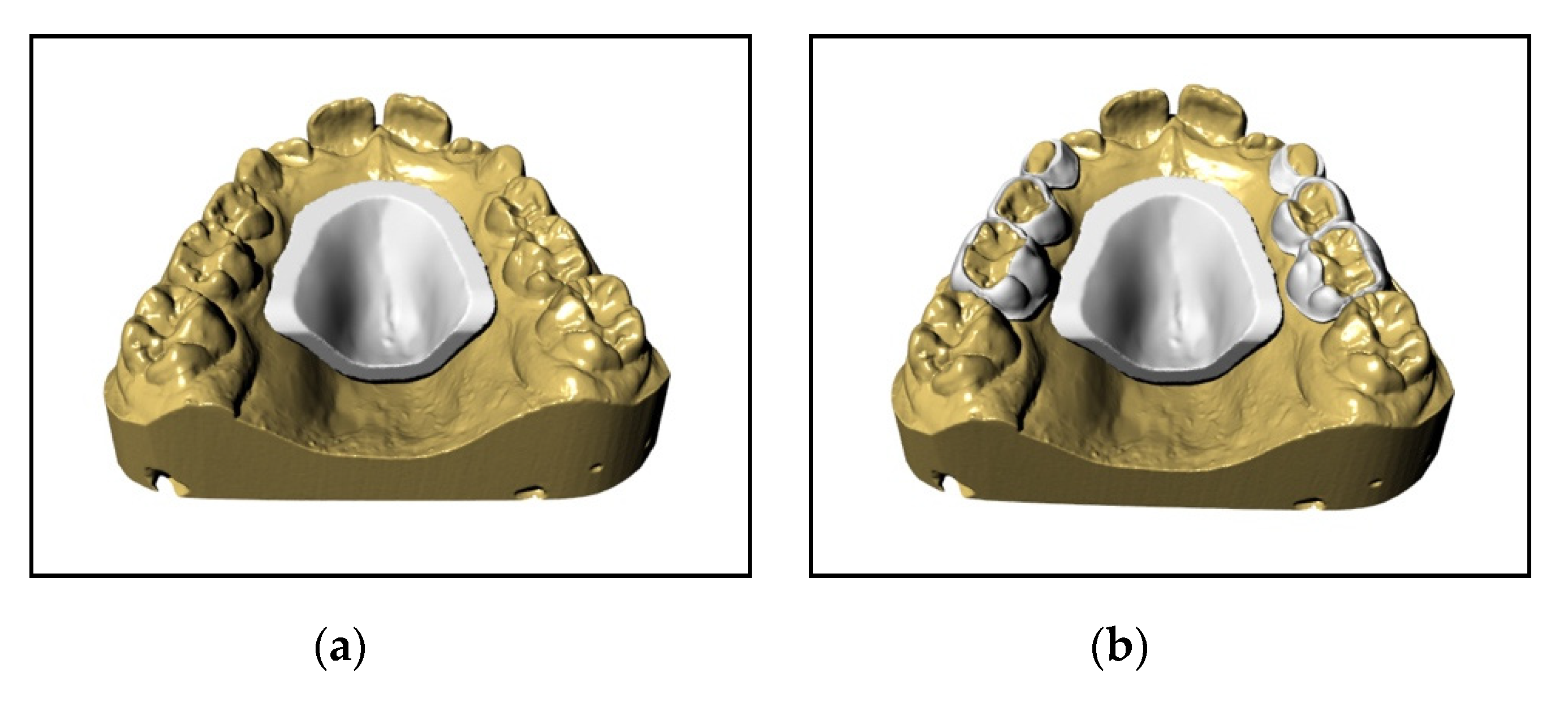
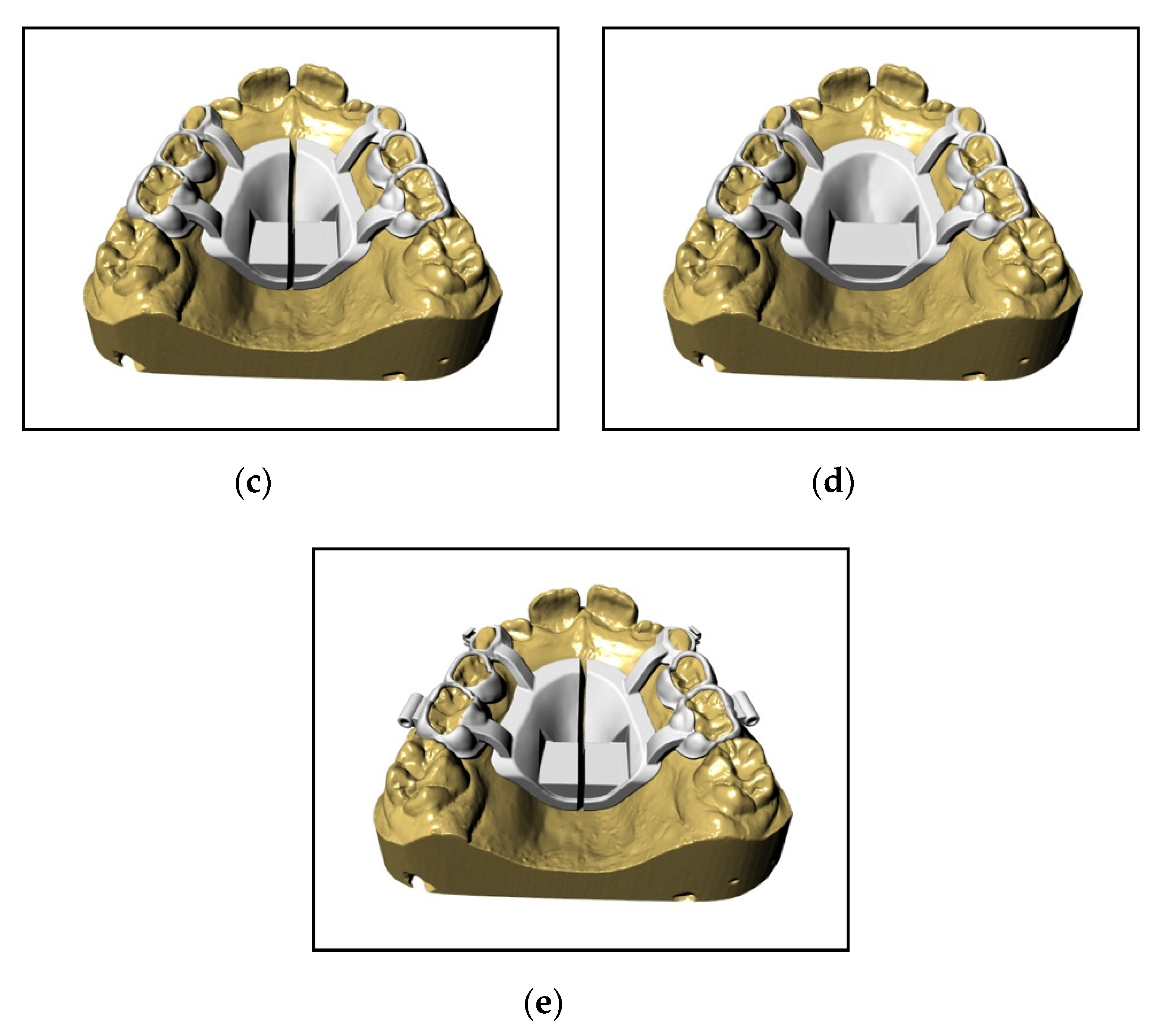
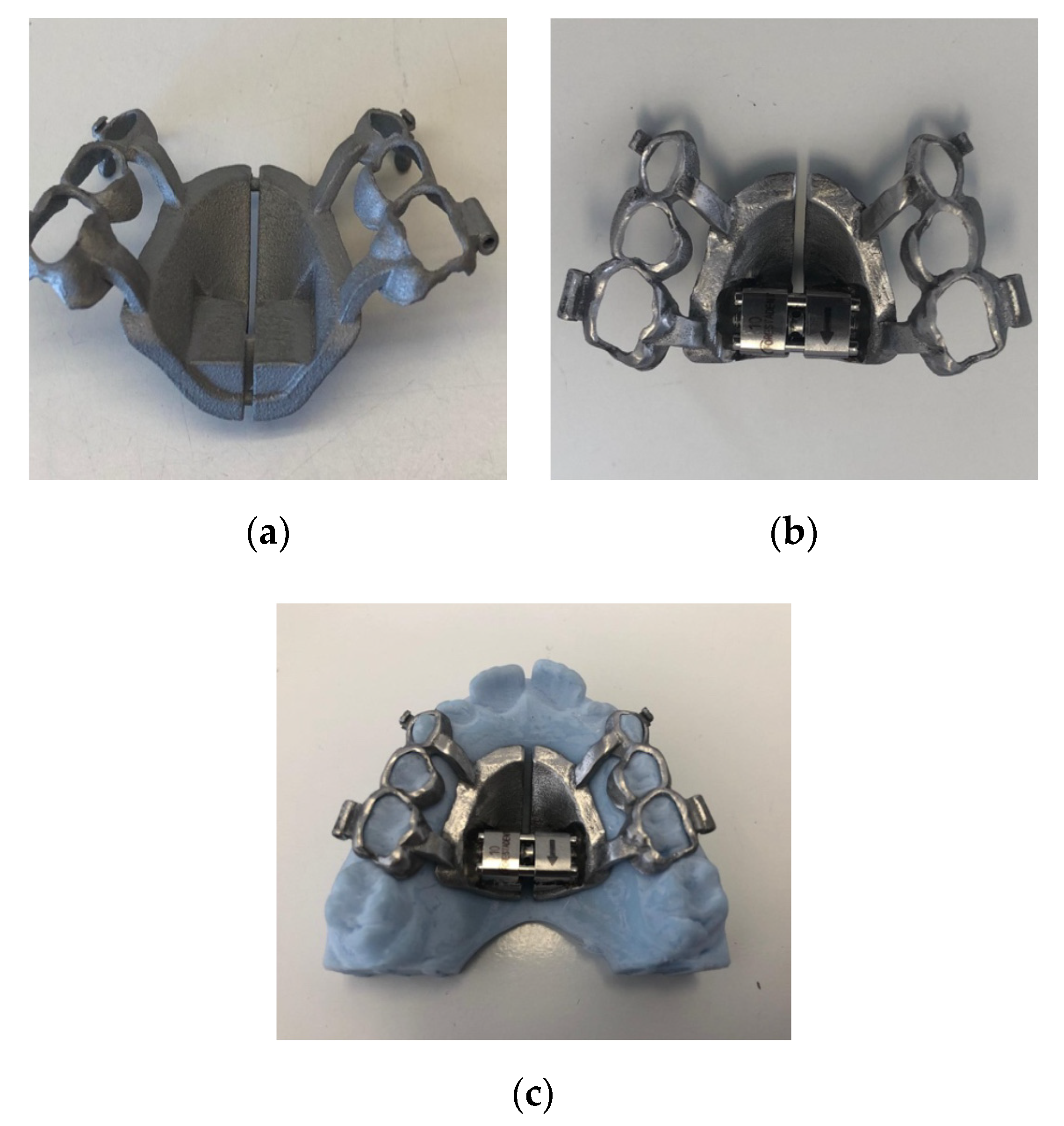
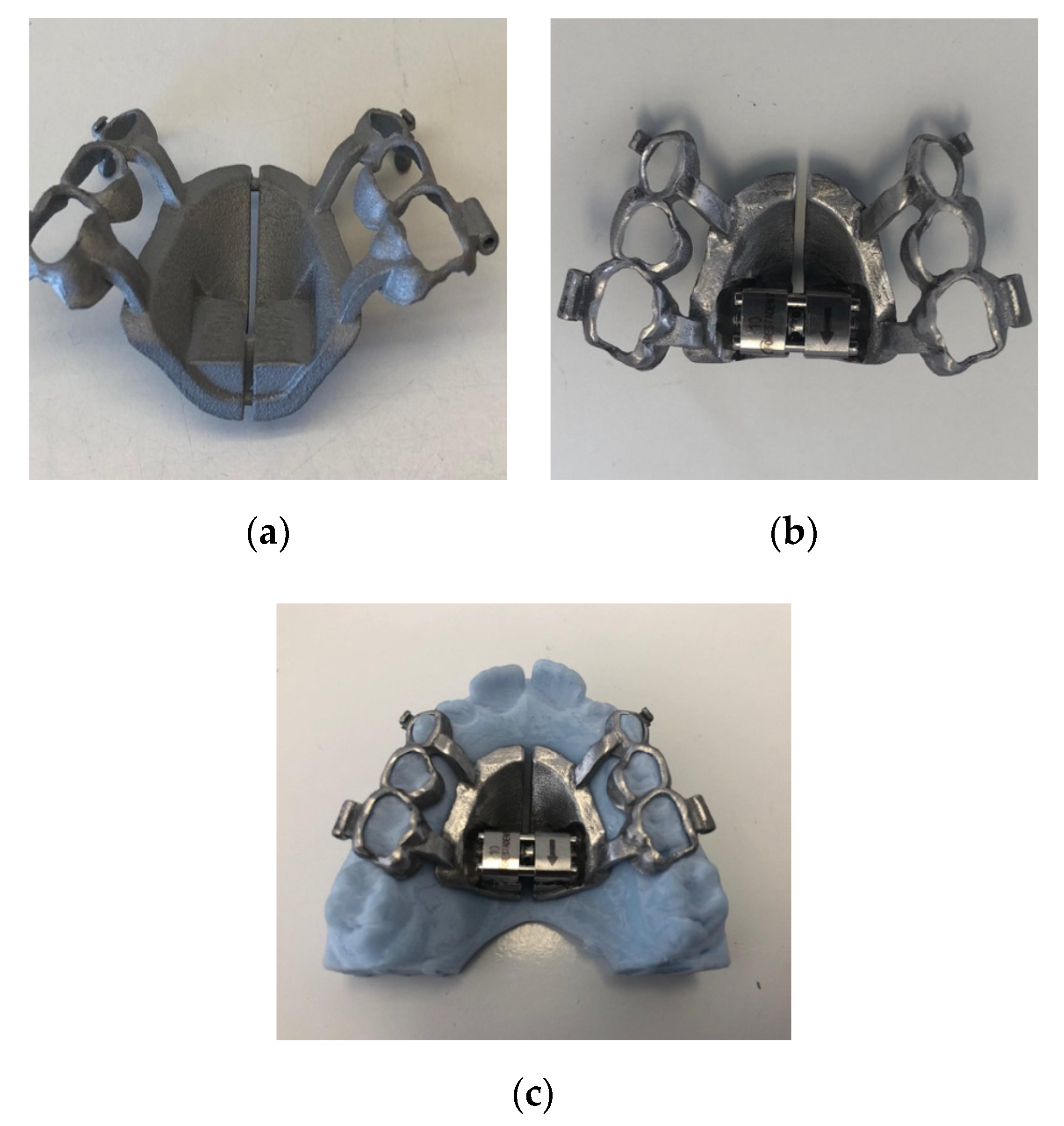
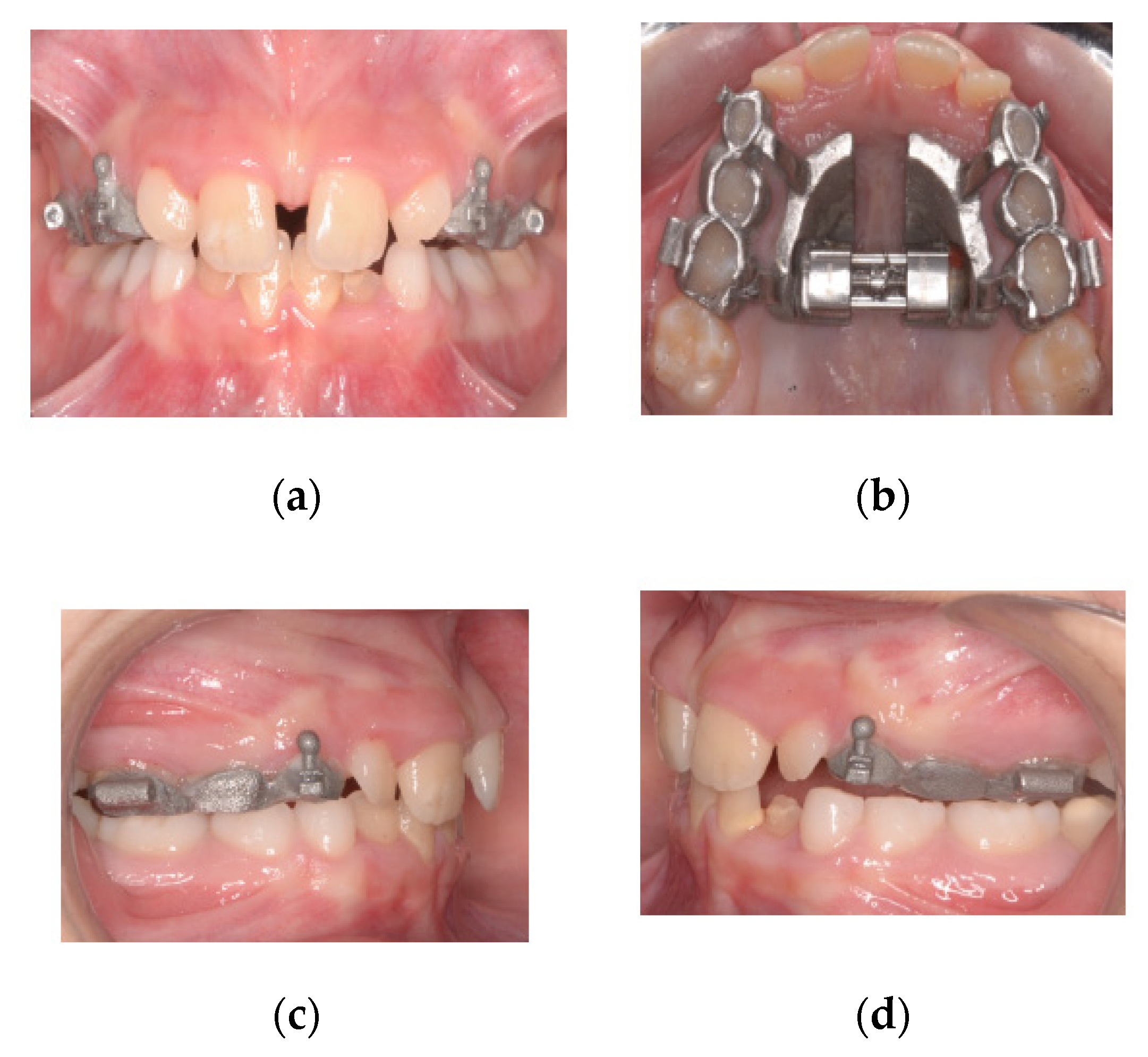
2. Procedure
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zuccati, G.; Casci, S.; Doldo, T.; Clauser, C. Expansion of maxillary arches with crossbite: A systematic review of RCTs in the last 12 years. Eur. J. Orthod. 2011, 35, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.d.P.; Monini, A.d.C.; Gandini, L.G., Jr.; Santos-Pinto, A. Rapid palatal expansion: A comparison of two appliances. Braz. Oral Res. 2012, 26, 242–248. [Google Scholar] [CrossRef]
- Frank, S.W.; Engel, G.A. The effects of maxillary quad-helix appliance expansion on cephalometric measurements in growing orthodontic patients. Am. J. Orthod. 1982, 81, 378–389. [Google Scholar] [CrossRef]
- Henry, R.J. Slow maxillary expansion: A review of quad-helix therapy during the transitional dentition. ASDC J. Dent. Child. 1993, 60. [Google Scholar]
- Huynh, T.; Kennedy, D.B.; Joondeph, D.R.; Bollen, A.-M. Treatment response and stability of slow maxillary expansion using Haas, hyrax, and quad-helix appliances: A retrospective study. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 331–339. [Google Scholar] [CrossRef]
- Biederman, W. A hygienic appliance for rapid expansion. JPO J. Pr. Orthod. 1968, 2, 67–70. [Google Scholar]
- Haas, A.J. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961, 31, 73–90. [Google Scholar]
- Wertz, R.A. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am. J. Orthod. 1970, 58, 41–66. [Google Scholar] [CrossRef]
- Koudstaal, M.; Poort, L.; Van Der Wal, K.; Wolvius, E.; Prahl-Andersen, B.; Schulten, A. Surgically assisted rapid maxillary expansion (SARME): A review of the literature. Int. J. Oral Maxillofac. Surg. 2005, 34, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Suri, L.; Taneja, P. Surgically assisted rapid palatal expansion: A literature review. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-J.; Park, Y.-C.; Park, J.-Y.; Hwang, W.-S. Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Moon, W.; Previdente, L.H.; Suzuki, S.S.; Garcez, A.S.; Consolario, A. Mini-screw Assisted Rapid Palatal Expander (MARPE): The Quest for Pure Orthopedic Movement. Dent. Press J. Orthod. 2016, 21, 17–23. [Google Scholar] [CrossRef]
- Lupini, D.; Retrouvey, J.M.; Decesari, D.; Cozzani, M. A Tissue and Boneborne Rapid Palatal Expander. J. Clin. Orthod. 2020, 54, 210–220. [Google Scholar]
- Mutinelli, S.; Cozzani, M. Rapid maxillary expansion in early-mixed dentition: Effectiveness of increasing arch dimension with anchorage on deciduous teeth. Eur. J. Paediatr. Dent. 2015, 16, 115–122. [Google Scholar] [PubMed]
- E Bishara, S.; Staley, R.N. Maxillary expansion: Clinical implications. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 3–14. [Google Scholar] [CrossRef]
- Filho, O.G.D.S.; Montes, L.A.D.P.; Torelly, L.F. Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 268–275. [Google Scholar] [CrossRef]
- Melsen, B. Palatal growth studied on human autopsy material. A histologic microradiographic study. Am. J. Orthod. 1975, 68, 42–54. [Google Scholar] [CrossRef]
- Zimring, J.F.; Isaacson, R.J. Forces produced by rapid maxillary expansion. 3. Forces present during retention. Angle Orthod. 1965, 35, 178–186. [Google Scholar]
- Vardimon, A.; Graber, T.; Pitaru, S. Repair process of external root resorption subsequent to palatal expansion treatment. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 120–130. [Google Scholar] [CrossRef]
- Baysal, A.; Karadede, I.; Hekimoglu, S.; Ucar, F.; Ozer, T.; Veli, I.; Uysal, T. Evaluation of root resorption following rapid maxillary expansion using cone-beam computed tomography. Angle Orthod. 2012, 82, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Kulbersh, V.P.; Jezdimir, B.; Haughey, M.D.D.; Kulbersh, R.; Wine, P.; Kaczynski, R. CBCT assessment of alveolar buccal bone level after RME. Angle Orthod. 2012, 83, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, M.; Andriani, J.D.S.P.; Ribeiro, G.L.U.; Locks, A.; Côrrea, M.; Correa, L.R. Three-dimensional assessment of buccal alveolar bone after rapid and slow maxillary expansion: A clinical trial study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Vanarsdall, R.L.; Secchi, A.G. Periodontal-orthodontic interrelationships. In Orthodontics, Current Principle and Techniques; Graber, T.M., Vanarsdall, R.L., Vig, K.W.L., Eds.; Elsevier Mosby: Philadelphia, PA, USA, 2012; pp. 810–813. [Google Scholar]
- Shungin, D.; Olsson, A.I.; Persson, M. Orthodontic treatment-related white spot lesions: A 14-year prospective quantitative follow-up, including bonding material assessment. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 136.e1–136.e8. [Google Scholar] [CrossRef]
- Mutinelli, S.; Manfredi, M.; Guiducci, A.; Denotti, G.; Cozzani, M. Anchorage onto deciduous teeth: Effectiveness of early rapid maxillary expansion in increasing dental arch dimension and improving anterior crowding. Prog. Orthod. 2015, 16, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cozzani, M.; Guiducci, A.; Mirenghi, S.; Mutinelli, S.; Siciliani, G. Arch width Changes with a Rapid Maxillary Expansion Appliance Anchored to the Primary Teeth. Angle Orthod. 2007, 77, 296–302. [Google Scholar] [CrossRef]
- Cozzani, M.; Fontana, M.; Cozzani, P. A cast-metal Haas-type expander for the deciduous dentition. J. Clin. Orthod. JCO 2010, 44, 738. [Google Scholar]
- Cozzani, M.; Fontana, M.; Cozzani, P.; Bertelli, A. Cast Haas-type RME appliance: A case report. Orthod. Art Pract. Dentofac. Enhanc. 2011, 12, 252–259. [Google Scholar]
- Ben-Bassat, Y.; Yaffe, A.; Steigman, S.; Freeman, J.; Ehrlich, Y. Functional and morphological-occlusal aspects in children treated for unilateral posterior cross-bite. Eur. J. Orthod. 1993, 15, 57–63. [Google Scholar] [CrossRef]
- Santos-Pinto, A.; Buschang, P.H.; Throckmorton, G.S.; Chen, P. Morphological and positional asymmetries of young children with functional unilateral posterior crossbite. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 513–520. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cozzani, M.; Antonini, S.; Lupini, D.; Decesari, D.; Anelli, F.; Doldo, T. A New Proposal: A Digital Flow for the Construction of a Haas-Inspired Rapid Maxillary Expander (HIRME). Materials 2020, 13, 2898. https://doi.org/10.3390/ma13132898
Cozzani M, Antonini S, Lupini D, Decesari D, Anelli F, Doldo T. A New Proposal: A Digital Flow for the Construction of a Haas-Inspired Rapid Maxillary Expander (HIRME). Materials. 2020; 13(13):2898. https://doi.org/10.3390/ma13132898
Chicago/Turabian StyleCozzani, Mauro, Salima Antonini, Daniela Lupini, Davide Decesari, Fabrizio Anelli, and Tiziana Doldo. 2020. "A New Proposal: A Digital Flow for the Construction of a Haas-Inspired Rapid Maxillary Expander (HIRME)" Materials 13, no. 13: 2898. https://doi.org/10.3390/ma13132898