Abstract
Elevated medical waste has urged the improvement of sustainable medical waste treatments. A bibliometric analysis is initially conducted to investigate scientific development of medical waste management to pinpoint the publication trends, influential articles, journals and countries and study hotspots. Publications on medical waste and its management sharply increased since 2020. The most influential article was written by Klemeš et al., and “Waste Management and Research” is the most productive journal. India, China, the United Kingdom, Iran and Italy have published the most works. The research spotlights have switched from “human” and “sustainable development” in 2019 to “COVID-19” and “circular economy” in 2021. Since government acts essentially in handling medical waste and controlling disease transmission, rule implementations among the abovementioned countries are summarized to seek gaps between scientific advancement and regulatory frameworks. For accomplishing a circular economy, waste-to-energy technologies (incineration, gasification, pyrolysis, plasma-based treatments, carbonization, hydrogenation, liquefaction, biomethanation, fermentation and esterification) are comprehensively reviewed. Incineration, gasification, pyrolysis and carbonization are relatively feasible methods, their characteristics and limitations are further compared. By holistically reviewing current status of medical waste research, the focal points involved in management at the policy and technical level have been highlighted to find proper routes for medical waste valorization.
1. Introduction
Waste generated related to medical services containing processes of prevention, diagnosis and therapy for humans and animals is known as medical waste, also called healthcare waste and clinical waste [1,2]. They are majorly produced by health institutions such as clinics and hospitals, research centers and testing laboratories, which have been distinguished into two categories: non-hazardous and hazardous. More than 80% of the non-hazardous property is regarded as general domestic waste, and close to 15% of infectious and radioactive characteristics are hazardous waste [1]. There will be a substantial risk to public health and the environment if the hazardous medical waste has not been appropriately treated and managed [3]. Hence, it is necessary to develop effective treatments for medical waste to reduce or eliminate the adverse effects.
It is shown that the quantity of medical waste maintains an increasing trend. Firstly, life expectancy at birth for both sexes in most countries is enhancing: Japanese men are expected to live 21 years longer in 2020 than in 1950, Canadian women are predicted to survive until 84.7 years old in 2020, compared to 71.7 in 1950 [4]. The aging population has raised the usage of healthcare services and thus caused the generation of medical waste to continue to climb. In addition, the worldwide outbreak of novel coronavirus since 2019 has affected human health and brought risks to the economy, society and environment [5]. Due to the rapid transmission rate of the coronavirus disease, there were approximately 570 million confirmed positive cases and more than 6 million cumulative death cases around the world by July 2022 [1]. Increasing demand for hospitalization and medical service to combat the ongoing pandemic has led to an alarming level of medical waste generation [6]. The production of medical waste during the pandemic in America is more than 8000 Tonnes per day, whereas close to 2200 Tonnes in India [7]. Patients and healthcare workers extensively consume personal protective equipment (PPE), and so do the citizens. Disease prevention policies have caused masks to be necessary for crowded places since 2020 in France, Italy, Germany, South Korea, Japan and China [8]. PPE has been defined as infectious waste in medical waste [9]. Furthermore, the coronavirus is capable of surviving seven days on surfaces of disposable masks [10]. The surging number of discarded PPEs comprising surgical caps, face shields, goggles, masks, gowns, gloves and shoe covers has become a worldwide concern as proper management is required to avoid further virus spread.
Various technologies for medical waste treatment and disposal have been developed and discussed to face the challenge of growing medical waste generation, namely, landfill, incineration, autoclaving, chemical disinfection and microwave sterilization. The most uncomplicated and mature method is to bury the waste at the landfill site of small capital expense, whereas incineration is the most utilized way to minimize the volume of waste [3]. However, the former requires a large amount of land and contaminates the habitat of soil and underground water due to the toxic gas emission, while the latter harms people’s health and the ecosystem for the sake of releasing poisonous gas, including dioxin, mercury and lead [11]. Autoclaving, chemical disinfection and microwaving are the elevated focal points to remove the presence of pathogens in the waste; however, these methods have not been extensively used owing to the insignificant size reduction in medical waste [12]. Therefore, a more sustainable disposal technique for medical waste should be found. Additionally, single-use face coverings are the symbolic infectious waste of medical waste, which filters contain approximately 70% polypropylene and 15% polyethylene that is worthy of recycling and depolymerizing via thermochemical procedures [13]. It is possible to convert disposable masks into value-added products or energy during thermochemical processes that benefit the economy, society and environment to achieve waste-to-energy and sustainable development.
There is no doubt that well-treated medical waste is one of the effective measures to prevent coronavirus from spreading to threaten public health further, so governmental authority performs a vital role in balancing monitoring disease transmission rates and managing medical waste sustainably. Policies established by the government could act as boundaries, comprising categories of medical waste, constraints or limits of pollutant emission and guidelines of the elected technologies. Thus, this paper will consolidate and review differential rules and regulations related to medical waste management in several countries.
Before the COVID-19 pandemic, medical waste disposal methods and management had already been discussed and studied worldwide. A pretty thorough piece of literature has covered the definition of medical waste, relevant regulations in developed and developing countries, medical waste management practices and the drawbacks of incinerating medical waste [2]. After the pandemic outbreak, the rapid increase in the amount of medical waste has led to effective medical waste management becoming the research direction of numerous authors. China and India are popularly investigated and examined since Wuhan was the epicenter of the outbreak and India followed in its footsteps. Practical institutive actions consisting of standardizing China’s medical waste management system, establishing ancillary laws and enhancing disposal capacities have been studied in response to the epidemic, which mainly focused on the operation mechanism of medical waste disposal [14]. Gao et al. [15] pinpointed each patient in village clinics generated 0.17 kg of medical waste per day and analyzed management practices on how village medical centers produce, gather, store, segregate and treat the soaring medical waste in rural China. Meanwhile, technologies treating hazardous waste and regulations supervising its disposal in India have been reviewed to emphasize the urgency of expanding medical waste management facilities [16]. An overall assessment and discussion based on the current resources, laws and practical strategies of bio-medical waste management during the COVID-19 pandemic [17].
Several papers aimed at waste-to-energy have been broadcast to accomplish more sustainable medical waste treatment. Khan et al. [18] have scrutinized the availability and accessibility of monetizing municipal solid waste through thermochemical and biochemical transformation methods for several developing countries and proved that bio-composting had become the most efficient option for converting solid waste into energy. At the same time, medical waste has been justified and demonstrated to be the ideal stock for pyrolysis, which stimulates bio-products manufacturing and sustainability [2]. Among those earlier works, there is a lack of discussion on both developed and developing nations rather than addressing a specific region that required thoroughly considering several angles of medical waste management, including definition, regulations, strategies and standard and novel thermochemical, biochemical and chemical waste-to-energy disposal methods.
This review supplies a comprehensive overview of medical waste management. The importance of developing sustainable medical waste algorithms is figured out in the first session. Second, a bibliometric analysis of publication trends, influential articles, journals and countries and study hotspots is conducted to deeply investigate the current state of scientific development in the research discipline of medical waste management embracing developed and developing countries to give insights into waste-to-wealth development. Based on the literature, compositions of medical waste are initially indicated, which is essential in determining disposal methods. Since governmental policies for handling medical waste can be the booster for the evolution of a circular economy, the most productive countries determined by the analysis are reviewed on the medical waste management regulations and practices. Moreover, the frequently utilized and recently novel treatments for medical waste with the aim to monetize medical waste to be value-added products are technically introduced and compared to provide insights for current and further applications. By holistic reviewing on managerial policy implementations and technical characteristics introductions towards medical waste disposal, future development directions of valorizing medical waste are provided for both developed and developing nations.
2. Methodology
2.1. Data Collection
The Scopus database was commenced in 2004 by Elsevier and allied to the most credible abstract and citation databases allowing access to the literature at a worldwide vision, which was utilized to gather scholars herein. Searched results were constrained to English language and keywords by Boolean logic OR, AND: “medical waste” OR “healthcare waste” OR “biomedical waste” OR “clinical waste” AND “waste management”, in the title, abstract and keywords. Over 1900 papers were found in the Scopus database (details of dataset could be available in the Supplementary Materials), fulfilling the said criteria without a time limit. Among the affirmed documents, more than 70% are categorized as article type being a controlling character while only 9% as reviews. The publications of the article far exceeds the number of review papers concentrating on medical waste management; thus, it is still significant to provide an overview of medical waste management from diverse perspectives in both developed and developing countries. Research manuscripts reporting large datasets that are deposited in a publicly available database should specify where the data have been deposited and provide the relevant accession numbers. If the accession numbers have not yet been obtained at the time of submission, please state that they will be provided during review. They must be provided prior to publication.
2.2. Research Design
The application of the bibliometric approach has been growing in different research fields for its utility in extensive scientific datasets analysis, research influence and impact measurement and study trends demonstration [19]. It is suitable for using bibliometric methods in a broad scope of review with too vast quantities of data to manually examine from the worldwide or regional performance to organizational or researcher prospects [19].
Several steps are included to present this analysis, primarily comprising data collection, analysis and discussion) as shown in Figure 1. First, the research goals and scope must be well-defined before data gathering and tool selection for bibliometrics. So as to extensively analyze prolific components comprising achievement for authors, associations, journals and nations in the discipline of studies, the number of papers should be substantial to hundreds or thousands of levels to be reviewed via bibliometric analysis. Database selection is the determinant for bibliometric techniques. Data collection (as shown in Section 2.1) and literature gathering are performed by limiting keywords and other criteria in the scholars. Second, the search results are processed to execute the bibliometric analysis and summarize findings by visualizing figures. Performance analysis and science mapping are contained to examine research overview of medical waste management and explore the predominant articles, journals, countries and keywords in the field of study. Finally, discussion on medical waste categories, regulations implementations in the most productive nations and feasible waste-to-energy techniques are performed based on the results of bibliometric analysis.
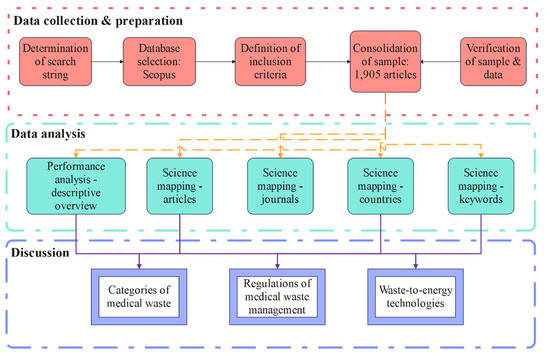
Figure 1.
Research framework.
Performance analysis and science mapping are the typical techniques for conducting bibliometric evaluation, wherein the primary aim for the former is to clarify the research element contributions, and the latter is to interpret research constituent relationships [20,21]. As for the performance analysis, metrics related to publication and citation decide each constituent’s productivity, achievements and influences in the designated field of study. Bibliographic coupling and analysis for citation, co-citation, co-word and co-authorship are employed to recognize relationships among different components in the research field for science mapping [22]. VOSViewer software is adopted to visualize the networks of bibliometric evaluation, which is a proxy of an interface-based graphical displayer for the network [23].
3. Literature Analysis: An Overview
3.1. Performance Analysis—Descriptive Overview/Publications
With restriction to the keywords “medical waste” or the equivalent terms such as “healthcare waste”, “biomedical waste” or “clinical waste” and “waste management” searching from the title, abstract to keywords, there are 1900 papers found in the Scopus database without a time limit. Close to 30% of documents discussed this kind of waste and its management from the subject discipline of environmental science. At the same time, medicine and engineering ranked second and third, accounting for 24% and 9%, respectively (see Figure 2).
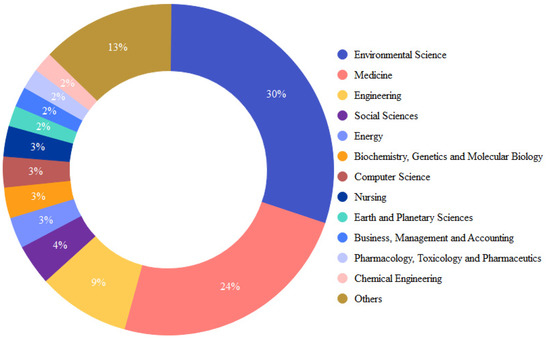
Figure 2.
Discipline contribution.
When published years were narrowed to 2012 and 2022, 1164 pieces of the literature were yielded and analyzed to confirm a 10-year trend of publications. Figure 3 shows a gradually increasing sensation of publications on “waste management” and “medical waste” or its synonyms; the quantities of publications per year fluctuated from around 70 to 100 between 2013 and 2019. Moreover, a sharp rise in publications on the same topic in 2020 and 2021, shown in Figure 3, says the growing attention and concerns in the research field after the outbreak of the novel coronavirus. The number of published papers related to medical waste and its management in 2021 doubled that of 2019, standing for the escalating amount of medical waste that has brought a global threat. Meanwhile, the research focused on “waste management” and “sustainable development” or “sustainability” for “medical waste” or the same type of waste in 2021 was six times more than the number of publications in 2019 shown in Figure 4. The studies conducted related to “waste management” and “waste valorization” or “circular economy” for similar nature of “medical waste” also imply a dramatic increase from 5 pieces of the literature in 2018 to 15 in 2021. These increasing tendencies manifest the growth in attention and awareness of medical waste management after 2019, especially for monetizing medical waste to be a valuable product in environmental science, energy and engineering field of research.

Figure 3.
Total number of publications in 2012–2021 in terms of “medical waste” OR “biomedical waste” OR “clinical waste” OR “healthcare waste” AND “waste management”.
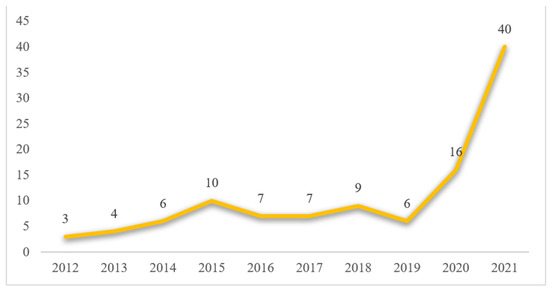
Figure 4.
Number of publications in 2012–2021 in terms of “medical waste” OR “biomedical waste” OR “clinical waste” OR “healthcare waste” AND “waste management” AND “sustainability” OR “sustainable development”.
3.2. Science Mapping—Journals
According to the results generated from the database, 1133 pieces of the literature have been published in 160 journals, and the remaining 31 articles are still in the press. Seventy-two of one hundred and sixty journals published less than three papers, almost half of the source publishers. Figure 5 provides an overview of the top ten productive journals by 2021, which also illustrates the preeminent ten publishers with the most significant output in the research domain of medical waste and its management, occupying more than a quarter of the total number of publications. Moreover, Waste Management and Research are denoted as the most high-yielding journal, which has published 78 pieces of the literature and is more than double the second most productive one called Waste Management with 33 published articles. Consequently, Waste Management and Research is located as the dominant position in the research discipline of medical waste. According to the data displayed in Figure 5, Science of the Total Environment and Environmental Science and Pollution Research ranks third and fourth among the top 10 most productive publishers with relative amounts of articles of 25 and 24, respectively.
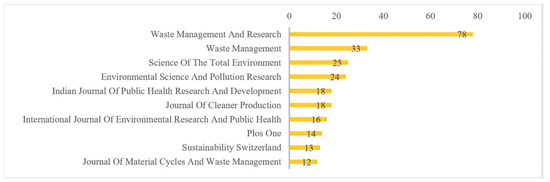
Figure 5.
Top 10 most productive journals.
Concerning the publications per each of the abovementioned journals, the trend between 2017 and 2021 is demonstrated in Figure 6. Figure 6 specifically focuses on the publication amount per the most productive journals in the recent five years, which aims to verify whether the published numbers per journal in these five years are consistent with the past trend. Almost all the contributors have published many essays during the past five years, except the Indian Journal of Public Health Research and Development, which has had no new articles in the last two years. The most significant number of publications is recognized as one of the highest productivity in the designated research field. Figure 6 also shows that Waste Management and Research is the most productive and outstanding journal, with an enormous yield to the total publications during these five years, which has leveled out at around six publications per year during 2017–2020 and 11 articles in 2021. Environmental Science and Pollution Research, Science of the Total Environment and Journal of Cleaner Production rank the second, third and fourth most productive publishers in Figure 6, revealing dramatic rises concerning the number of publications in 2020 and 2021.
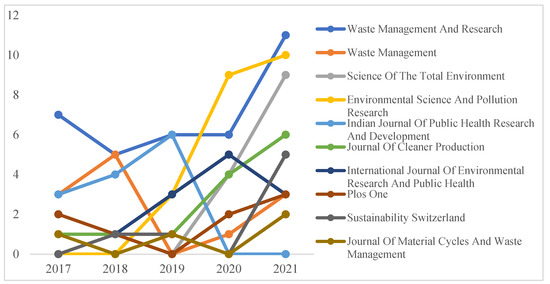
Figure 6.
Publications per journal in 2017–2021.
The number of citations correlates with the journals’ influence and impact on the research area. Figure 7 lists the top 10 most potent journals of the highest significant degree according to the number of cited from 2012 to 2021 in the Scopus database. Science of the Total Environment gained the most citations by 496 during these ten years, indicating the most attention being drawn towards medical waste studies. The following most-cited journal of this field in descending order consists of Waste Management and Research with 406 citations; Journal of Cleaner Production with 342 medals; Resources, Conservation and Recycling with 277 medals and Waste Management with 21 medals.
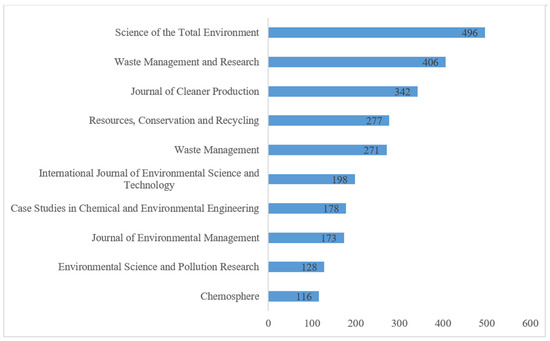
Figure 7.
The number of citations for journals.
3.3. Science Mapping—Articles
The most influential articles equal the largest number of cited in the accustomed research domain, which reveals the essence and impact of the publication based on the cumulative repetitiveness of citations on the chosen database [24]. Figure 8 visualizes the networks of the selected articles related to “waste management” of “clinical waste” or the same kind of waste. Conjointly, Table 1 lists the elite tenth articles according to the number of citations in terms of the medical waste research field. Under the restraints of the search engine, there are 153 pieces of work with a minimum of 5 citations: 8 articles have already been cited more than 100 times, while 3 of them got larger than 200 excerpts. The most influential article with the highest citations of 389 has assessed various plastic products, especially PPEs in the COVID-19 pandemic and epidemic from the whole life cycle impacting waste management systems and proposed plastic waste footprint (PWF) as the key environmental evaluation indices [25]. The second elite is a review article conducted by Lambert and Wagner [26] with 297 citations concentrated on polymers of bio-based and biodegradable characteristics and biodegradability in the actual waste management structure. Sharma et al. [27] pinpointed threats, opportunities and modernizations for handling solid waste during the crisis of COVID-19 and suggested strengthening the local supply chain post-pandemic from the economic aspect, which ranked the third leading paper and was cited 226 times. Moreover, the initial article on the estimation of disposable masks and medical waste generation in 49 countries in Asia during the epidemic executed by Sangkham [28] ranked fourth, with 150 citations. The fifth influential work implemented by Yu et al. [29], with 149 citations, proved that setting up temporary incinerators could be the most effective way to dispose of the overwhelming medical waste in China.
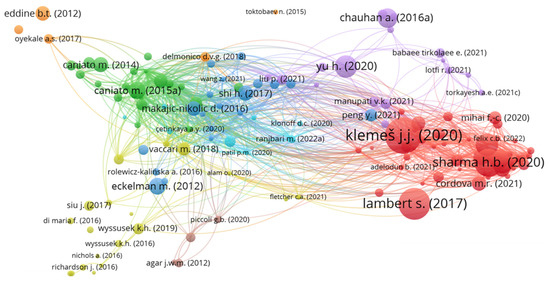
Figure 8.
Visualization network of articles.

Table 1.
Elite tenth articles according to the number of citations in terms of the medical waste.
3.4. Science Mapping—Collaboration Networks
Eighty-four countries distributed the literature in our search domain, and thirty-six have contributed at least three articles. Figure 9 envisages a collaboration network with differentiated circle diameters and link widths, while the number of publications determines the size of circles and the intensity of collaboration between two nodes controls the thickness of connections. Table 2 is the extension and detailed display of Figure 9, it lists the number of publications and collaboration works per the top ten elite countries. For the number of released articles, Table 2 shows India ranked first of 70 publications for medical waste and its management as the most productive country in this research field. China takes second place with 39 pieces of the literature, whereas the United Kingdom (UK) deems third with 32 published articles. The succeeding productive countries are Iran, Italy and the United States (US), with 28, 24 and 23 publications concentrating on medical waste. Regarding collaboration, China, India and Italy are the top three countries, with 52, 50 and 34 collaborating works with other countries. Based on the results of Figure 9 and Table 2, it is evident that developing countries have become notable characters in medical waste-related research. Yet, improper disposal and treatment approaches for handling medical waste have not been rectified in developing nations, which indicates a bridge is required to build between tremendous productivity in scholars and tiny adaptability in practice [35]. Therefore, the efforts of corresponding governmental authorities regarding medical waste management for the top five countries will be further investigated in Section 4.
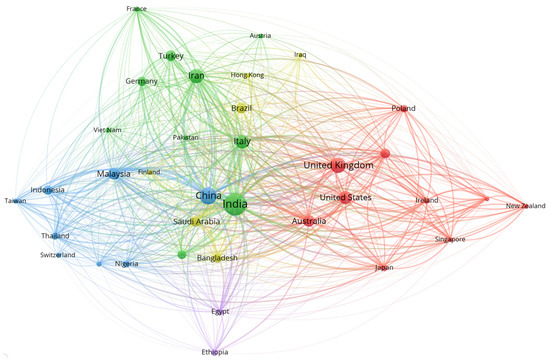
Figure 9.
Collaboration network.
Table 2.
The number of publications and collaboration works per country.
3.5. Science Mapping—Keywords/Research Hotspots
Under the appearance limitation of not less than ten times, 101 of 2939 keywords are formed into a network shown in Figure 10. Keywords co-occurrence represents the frequency of two terms occurring together in a particular article and illustrates the connection between two perceptions, which has been extensively employed in hotspot identification and trend demonstration for the emergent discussion in a specific research discipline [15,36]. According to the overlay visualization in Figure 10, focal points regarding medical waste from time to time are distinctive. Figure 10 displays several sizes of dots with different colors: the diameter of circles equals the number of times occurring in the published works, while the colors are different time periods discussing the terms. The larger the dots are, the hotter discussion of the keywords is; the darker the circles are, the more outdated the hotspots are. Referring to the results of Figure 10, medical waste management and disposal were linked to natural resources and personnel put environmental impacts and sustainable development as the first consideration in 2019. Governmental practice guidelines, several treatment approaches such as incineration, landfill and microwave radiation, also public health were taken into account for managing medical waste in 2020. The dramatically increasing amount of plastic waste as personal protective equipment generated in the novel coronavirus pandemic arouses researchers’ attention to the circular economy and waste-to-energy technology—pyrolysis in 2021.
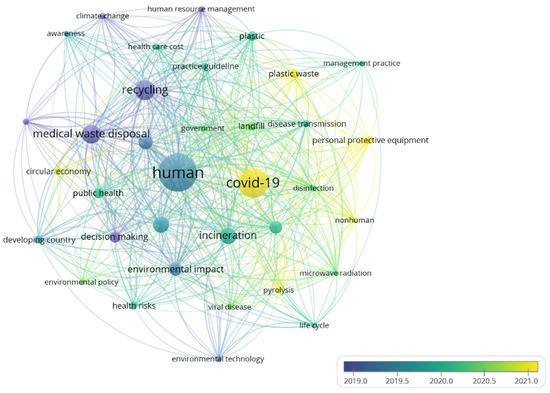
Figure 10.
Keyword network.
4. Results and Discussion
4.1. Categories of Medical Waste
According to the World Health Organization, waste with non-hazardous characteristics similar to domestic solid waste has occupied nearly 85% of the total waste produced by all activities related to providing medical services [1]. The resting proportion of garbage has been categorized as a hazardous type that jeopardizes public health and the global environment [2]. Due to the escalating increase in medical waste during the coronavirus pandemic, it is valuable to classify the composition of medical waste that is the determinant for ways of disposal, especially for tackling the vast amount of COVID-19 waste.
Non-hazardous medical waste is regarded as a general type of waste that does not cause a crisis in physical, biological, chemical and radioactive systems. Waste of metropolitan type includes discarded plastic flasks, food waste and packaging and paper from healthcare facilities are non-flammable medical solid waste [37]. This type of waste is similar to household waste with the capability to be recycled and managed sustainably; however, it still contains the potential for disease transmission since asymptomatic sufferers of SARS-CoV-2 also produce daily rubbish. Apart from the general medical waste, seven categories of hazardous waste are produced by the endeavors related to health management shown in Table 3.
Table 3.
Classifications and definitions of hazardous medical waste [1,38].
4.2. Regulations of Medical Waste Management
Government authority plays an essential role in policymaking for both reward and punishment systems to boost the sustainably of medical waste management. Table 3 lists the regulations and treatment approaches among these five countries. A number of innovative treatment ways for converting medical waste into costly products have been developed and analyzed in the literature from India and China, but incineration is still the most widely and primarily applied method. Accordingly, a gap is found between actual implementation and scientific research for those advanced technologies.
Developed countries and developing nations perform distinctively in medical waste management. The guidelines and regulations set in developed nations such as UK and Italy are much earlier and more specific from medical waste segregation, collection, transportation and storage to disposal. As for developing countries including India, China and Iran, the requirements of medical waste management have not been clearly stated, especially for the emission standards though there are more relevant published documents in these two countries as illustrated in Table 2. Moreover, owing to the applicability of waste types, incineration is the most popular treatment approach for medical waste worldwide. Referring to Table 4, China is the largest daily medical waste producer during the pandemic, temporary incinerators have been installed as the emergency treatment path, but the coverage rate of utilization still should be considered. Therefore, minimizing emissions of toxic particles and greenhouse gases and maximizing the efficiency of waste-to-energy by using incineration are required to be further studied.
Table 4.
Regulations and treatment methods of medical waste.
4.3. Technologies for Medical Waste Management
Regarding the results from the bibliometric analysis, there are strong relationships between medical waste and several keywords, including “COVID-19”, “plastic waste”, “personal protective equipment” and “circular economy” since 2021. Reduce, reuse, recycle and recover are the 4Rs in the concept of circular economy, which aims to minimize utilization of sources and maximize reusability of the existing substances, as well as alter waste to be a resource supplier to continue the designated process for product or energy regeneration [53,54]. Thus, the valorization of medical waste is one of the possible solutions for a circular economy in a more sustainable algorithm. This paper limits the scope of the treatment approaches for medical waste monetization to those with the ability of volume reduction. There are three classifications consisting of thermochemical, biochemical and chemical technologies are shown in Figure 11.
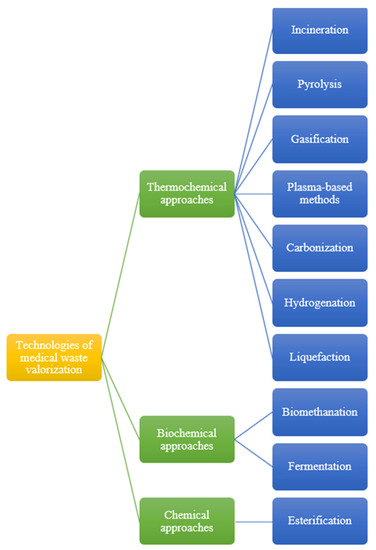
Figure 11.
Medical waste valorization technologies [55,56,57].
4.3.1. Thermochemical Treatments of Medical Waste Valorization
The thermochemical conversion process means the structure degradation of medical waste with the presence or absence of oxygen at high temperatures. Medical waste that was treated by thermochemical technologies equals energy from medical waste recovered into products under an atmosphere of high temperatures. The dry matter contained in municipal solid waste is the most advisable raw material for thermochemical transformation methods [56]. Accordingly, the dry content from medical waste treated by thermochemical conversion is applicable. For instance, the filter of the used masks primarily contains polypropylene and polyethylene, which can be recycled and depolymerized by thermochemical techniques to generate energy or valuable products to accomplish medical waste valorization. This article will encompass incineration, pyrolysis, gasification, plasma-based methods, carbonization, hydrogenation and liquefaction. Their distinctions from reaction conditions containing amounts of excess air, temperature, pressure and reaction agents, which cause differentiated conversion of intermediate and final value-added products, will be introduced and discussed.
Incineration
Incineration is the most extensively employed method for medical waste decomposition and disinfection in order to minimize waste size and hazardousness, which allows cutting more than 80% of solid mass and 90% of volume [58]. With excessive air, combustible contents of medical waste are entirely decomposed within 800–1450 °C of the operating temperature as oxidation processes [55,59]. Waste-to-energy is achieved since the heat produced in high-temperature incineration is converted into high-temperature steam, which turns a turbine that activates a steam turbine generator to generate electricity, as shown in Figure 12. Furthermore, incinerating polyolefin plastic waste is a possible solution to produce a substitute for conventional fuel due to the comparable calorific values compared with gas and petrol, which converts medical waste into value-added products to circulate the economy [60]. Medical waste incinerator is potentially competent to be ecological when it provides a particular amount of energy sources for energy recovery practice. Meanwhile, it can be a polluter releasing contaminations counting sulfur oxides, chlorines, carbon monoxides or dibenzodioxins when the flue gases are not suitably handled [54,61]. Additionally, Geyer et al. [62] predicted that almost half of the plastic waste around the world will be handled by incineration in 2050. Hence, clean flue gas systems controlling emissions during waste combustion should be further studied and developed.
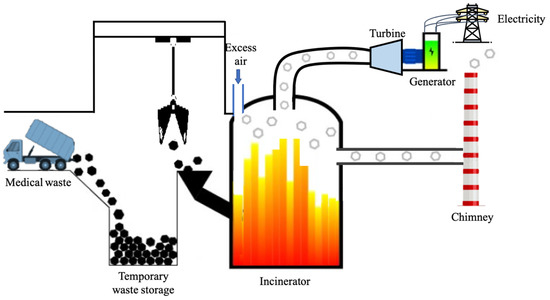
Figure 12.
Waste-to-electricity during incineration [55,60].
Gasification
Gasification represents a thermal conversion process of medical waste from organic materials into synthesis gases with limited oxygen at high temperatures in the range of 800–1600 °C [63,64]. The produced syngas mainly amounting to carbon dioxide (CO2), carbon monoxide (CO), hydrogen (H2), methane (CH4) and chain compounds solely of hydrogen and carbon could be reprocessed to feedstock or synthetic fuel [54]. Different reaction atmospheres significantly affect the generation of final value-added products defined by air and steam gasification. The atmosphere formed by a ratio of oxygen and nitrogen is known as air gasification, being relatively uncomplicated due to the low calorific content of gases produced. However, steam is the medium of steam gasification to generate gases of high hydrogen value during the endothermic process with colossal energy demand. The purified syngas can remove impurities such as acid gas causing equipment corrosion and tar inducing equipment blockage so that it can be employed in gas boilers, internal combustion engines or gas turbines with high efficiency to recover electricity [65]. Figure 13 demonstrates waste-to-electricity could be achieved by gasification. Khan and Kabir [57] confirmed the sustainability of gasification is 30% higher than that of incineration by comparing four waste-to-electricity technologies in a multi-criteria analysis. Although the syngas produced by gasification consist of more abundant methane and hydrogen than that generated by pyrolysis, a number of impurities are found in the former [66]. Plastic waste gasification always leads to high tar gas generation and some even higher than 150 g/Nm3; consequently, additional gas purification is mandatory [67]. Moreover, the feeding materials with sulfur content less than 0.73 wt%, such as polyvinyl chloride (PVC) and rubber, are infeasible for gasification [68].
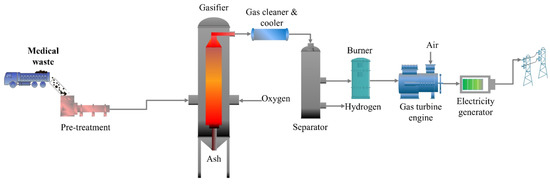
Figure 13.
Waste-to-energy of gasification [57].
Pyrolysis
Pyrolysis is a process for thermally decomposing large polymeric molecules of medical waste into smaller molecules in the atmosphere either with inadequate oxygen or oxygen-free. Plastic waste can be thermally degraded at 540–830 °C under no oxygen conditions [69]. Energy supply is necessary for thermal pyrolysis since it is an endothermic mechanism, whereas a catalyst is required for catalytic pyrolysis as catalytic is used to accelerate chain breakages. Differentiations in feedstock and operational conditions during pyrolysis result in different states of final products including solid, liquid and gas [40]. The authors of [70] proved that pyrolysis technology is capable of transforming medical waste into valuable goods containing biofuel as an alternative fuel and biochar as an adsorbent. Pyrolysis of medical waste can generate liquid fuel and become the energy source for turbines to drive generators and further lead to power production [3]. Aragaw and Mekonnen [71] experimented and revealed that approximately 75% of disposed personal protective equipment could be converted into bio-crude oil via the application of pyrolysis and the quality of the product can be further improved if the catalyst is added. The conceptual process of pyrolysis to convert medical waste into valuable products is shown in Figure 14. Pyrolysis is considered more environmentally protected than incineration owing to the relatively low emission of carbon monoxide and carbon dioxide, which is less than 4 vol% and 9%, respectively [72]. Moreover, it was claimed that it may contribute to more available job positions based on a social management analysis of tire pyrolysis [73]. However, this technology consumes a large amount of heat energy and is at the developing stage with the unavailability of waste rubber treatments.
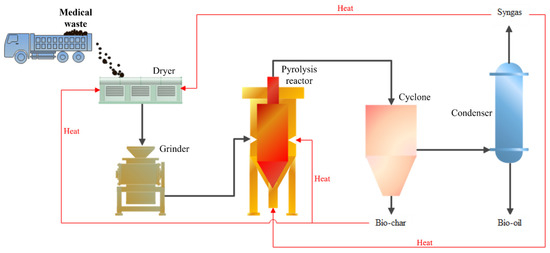
Figure 14.
Waste-to-energy achieved by pyrolysis [72].
Plasma-Based Methods
Plasma technologies are built according to the physical principle that plasma means the fourth state of substances, including radicals, charged ions and free electrons [58]. Matter changes its state when energy is supplied: solids become liquid, and liquids become gaseous. If even more power is provided to a gas, it is ionized and goes into the energy-rich plasma state. When gaseous molecules are strained into high-energy collisions with charged electrons, causing the generation of charged particles, plasma could be produced and several reactions containing ionization, disassociation and re-association are activated. Based on different energy sources and conditions during plasma generation, plasma has been distinguished into thermal and cold plasma [74]. The former has electrons and heavier particles, including ions and neutrons, in thermal equilibrium of the same temperature, whereas the latter has ions and neutrons of lower temperatures than electrons [75]. As for the plasma-based mechanism used for waste management, the treatment processes are of high energy, high densities and high temperatures for rapid heating, reactant transformation and high-temperature feedstock melting that requires a smaller installation scale to handle a given waste throughput [76]. Plasma is an essential approach to achieving valorization of medical waste because of the production of syngas, hydrogen and electricity as valuable products during the process. Plasma-based methods are employed in varied medical waste treatments, namely, plasma gasification, pyrolysis and compaction, as excellent sterilizers [55]. However, electricity acts as the source of energy provided during medical waste treatment, representing a costly energy vector. Moreover, Erdogan and Yilmazoglu [77] reported that the temperature requirements of the thermal plasma generator should reach around 9723 °C, and Munir et al. [78] mentioned that plasma gasification is weak in high capital cost and nitrogen oxide emissions.
Carbonization
Carbonization is a technology for transforming the carbon of polymer waste into unique homogeneous carbonized items, such as char or carbon-centric products containing carbon fibers and carbon nanomaterials by releasing volatile materials [40,67]. Figure 15 illustrates two classifications of carbonization: dry carbonization (Figure 15a) and wet carbonization (Figure 15b). The former is also named torrefaction, which heats the litter gradually from moisture evaporation in the inert environment of 1 atm pressure and 200–300 °C, and the latter is known as wet torrefaction, which manufactures carbonized products by uplifting temperature within 180–280 °C and saturation 2–10 Mpa pressure [67,79]. Dry carbonization is more straightforward and cultivated than wet torrefaction since there is no requirement for waste pressurization and heating before carbonizing. Heat and high calorific char with low chlorine is the main product of these two processes: low content of calcium for torrefaction but low ash content for wet carbonization [80]. Pre-treatment for moisture reduction in medical waste before proceeding to torrefaction could be eliminated due to the dry basis of medical waste. Though disposable face mask primarily made of polypropylene is a crucial determinant for char production from dry carbonization, the generation of corrosive vapors will lead to environmental deterioration [81]. However, the unavailability for continuous operation and the demands of high-pressure reactors and excessive energy for pressuring and heating medical waste are the drawbacks of wet carbonization [82]. Consequently, applying the carbonization technique to handle medical waste still needs further investigation.
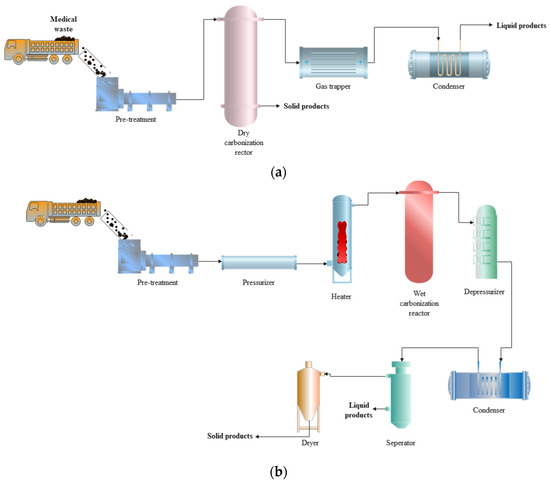
Figure 15.
Carbonization: (a) Dry carbonization generating valuable products; (b) Wet carbonization process producing value-added products.
Hydrogenation
Hydrogenation is a technique used to decompose large hydrocarbon particles into small molecules by breaking C-C bonds under the atmosphere with excess hydrogen and a catalyst under high pressure [83]. Compared with pyrolysis, this technology transforms plastic waste into high-quality fuels in a liquid state through the reduction and saturation of organic matter [64]. Products generated by hydrogenation are distributed in a narrower molecular weight than those of pyrolysis, which improves the selectivity of hydrogenation in the range of C6-C12 for gasoline products [84]. Moreover, hydrogenation has higher transferring efficiencies of mass and heat since there is less limitation for waste processed in solution [85]. However, one of the mandatory elements for the hydrogenation process—the hydrogen stream—is high-priced compared to other fluidizing gases (e.g., nitrogen applied in pyrolysis). Ragaert et al. [86] found that a ton of hydrogen produced by electricity sells for $2800, equivalent to 14 times the price of nitrogen. The high pressure needed for the hydrogenation process leads to harsher equipment becoming necessary. Therefore, hydrocracking is less popular than pyrolysis because of its high-cost requirement and absolute operating conditions.
Liquefaction
Liquefaction is a trendy alternative for turning polymers of waste into liquid value-added products, including transportation fuel and chemical raw materials for industrial usage, which are processed at 300–450 °C and pressurized with various solvents [87]. The application of solvent as reaction media improves heat and mass transfer and targets higher production yield of good quality liquid outputs in milder conditions with lower temperature and pressure [88]. Water and alcohol are of increased accessibility and employed as organic solvents of liquefaction, and alcohol has a relatively low critical point [89]. Liquefaction is differentiated from thermal pyrolysis on the state of hydrogen-donating components and depolymerization execution of plastic waste [90]. This technique does not require feedstock drying but can produce fuel with low moisture and oxygen content with higher heating values. Plastic liquefaction also generates by-products, including char and gas, according to reaction time and temperature, states of raw materials’ solvent and physicochemical characteristics [91]. Ahamed Kameel et al. [89] also pointed out that maximum char and few gases could be formed in low heating temperatures and short processing time. However, the liquefaction of medical waste still needs deeper investigation since there is no adequate information that could be obtained from the previous literature.
4.3.2. Biochemical Treatments of Medical Waste Valorization
Apart from thermochemical waste-to-energy conversion technology, biological transformation methods such as biomethanation and fermentation are the second classification to degrade waste by microbial processes. The feedstock of biochemical treatments has been limited to biodegradable types, for example, food waste and yard waste. It is concluded that the wet content of the agricultural waste and biogenic elements in municipal solid waste is the most appropriate raw material for biochemical transformation methods [56]. Thus, the wet matter from medical waste is feasible to be valorized through biochemical conversion processes.
Biomethanation
Biomethanation is also named anaerobic digestion, which biologically degrades organic substances of the material to generate valuable products under oxygen-free conditions [92]. Biogas generated by biomethanation is methane-rich gas functioning as a fuel, comprising methane (CH4) of up to 75%, carbon dioxide (CO2) of 25–50% and other gas products. Digestate is also produced, a nutrient supply functioning as fertilizer—Figure 16 exhibits converting organic waste into wealth by biomethanation. Waste of higher moisture levels and organic content is preferable to a biochemical conversion approach for energy recovery. Sewage sludge and food waste are typical ingredients for anaerobic digestion rather than medical waste; thus, this technology will not be further discussed in this paper [93].
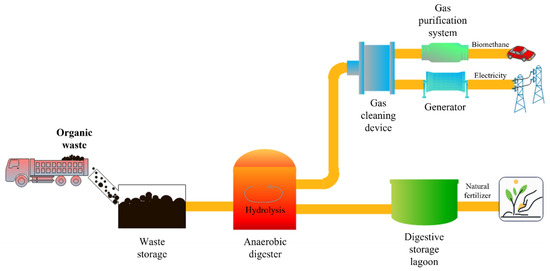
Figure 16.
Waste to wealth achieved by biomethanation.
Fermentation
Fermentation is a biomedical process to convert organic compounds from waste into volatile fatty acids, including alcohols such as ethanol and butanol, lactic acid and hydrogen, under an oxygen-free reaction atmosphere via anaerobic metabolism [56]. Like biomethanation, the fermentation of food waste is more popular than medical waste due to its rich protein, oil, fat, mineral and carbohydrate content, and further converted to valuable products [94]. Bioethanol is one of the value-added products made by fermentation technologies and it is essential in the transportation system as a clean fuel. However, this conversion process requires rigid control and optimization of reaction conditions such as pre-treatments, temperature, pH and microbes that cause fermentation technologies being developing [95,96].
4.3.3. Esterification
Esterification is a chemical reaction between carboxylic acid and alcohol, which generates ester and water with the aid of a catalyst, and the reaction temperature is set to slightly higher than the boiling point temperature of alcohol [18]. Biodiesel of biofuels, as well as solvents containing ethyl acetate and methyl acetate utilized from paints and varnishes to herbicides and pesticides, are the specific products generated from the esterification of reactions between alcohol and fatty acids [97]. Homogeneous and heterogeneous catalysts are used for accelerating the esterification reaction: The former (such as sulfuric acid and hydrochloric acid) can be miscible with the reaction medium and partially protonated the carboxyl group of fatty acid, while the latter is a catalyst in a different phase from the reactant [98,99]. Taking the raw oil material for biodiesel generation as an example, triglyceride is the main component when transesterified with high-purity methanol; fatty acid methyl ester is generated to achieve waste-to-energy, and base-catalyzed transesterification is labeled as the most economical approach for biodiesel production [56]. However, detailed research on waste-to-energy esterification of medical waste is still lacking.
4.4. Future Direction of Medical Waste Management
4.4.1. Thermochemical Treatment toward Waste-to-Energy
Though a whole bunch of technologies have been proposed for medical waste to energy, some of them are still developing at an early stage. Methods such as hydrogenation, liquefaction, fermentation and esterification are not well established and ratified yet in managing waste globally. Due to the complex characteristics of medical waste and disinfection requirements before recycling, chemical and thermal treatment are deemed more suitable for recovering energy from waste, also effectively facilitating disinfection. It was experimentally proved that contaminated materials as well as the COVID-19 virus could be effectively sterilized by thermal disinfection [100,101]. It should be noted that hydrogenation and liquefaction are primarily still investigated at the lab-scale, therefore thermochemical treatment methods mainly covering incineration, gasification, pyrolysis and carbonization are more infeasible and economical options toward medical waste-to-energy currently.
Table 5 shortlists the operation conditions regarding temperature, pressure, reaction agents, presence of oxygen and the final products for five main thermochemical methods. Carbonization requires the lowest temperature, whereas incineration, gasification and pyrolysis have higher temperature demands and thus lead to different degrees of medical waste decomposition. Generally, pyrolysis facility the production of hydrogen at high temperatures [73]. Incineration, pyrolysis and dry carbonization are of similar conditions of pressure; however, gasification and wet carbonization need additional pressure for reactions. Both incineration and gasification involve reactions with oxygen but require different amounts of oxygen for different oxidation degrees. In the comparison of products, pyrolysis and dry carbonization are suggested when liquid products in the forms of bio-oils are preferable. Recently, many studies have focused on co-pyrolysis of suitable feedstocks as the remarkable promotion of produced oil [102]. Regarding the generation of solid residues, incineration will produce the largest amount of bottom ash and fly ash, and gasification and pyrolysis follow in turn. The generated solid waste is always regarded as hazardous due to the existence of heavy metal content, dioxins and furans [67]. Moreover, the produced toxic fly ash should be safely and properly treated by flue gas treatment before releasing to the atmosphere through a tall chimney. Syngas could be formed through gasification and pyrolysis as usage of internal combustion engines or substitute for fuel, in which pollutant has been removed before combustion and resulting in lower emission levels than incineration. Therefore, the government authorities should initiate stricter regulations targeting emission control, especially for incineration.
Table 5.
Operation conditions and production generation of waste-to-energy technologies.
It is inevitable to comprehensively understand the pros and cons of different methods for a wise selection. Table 6 shows the summary of strengths, weaknesses, opportunities and threats of incineration, gasification, pyrolysis and dry and wet carbonization. Incineration, gasification, pyrolysis and carbonization are alternative options for medical waste valorization, but PET, PVC and rubber are still not the available feedstocks for gasification and pyrolysis. Incineration as the most mature technology for medical waste treatment with the ability to minimize waste volume at 90–95% is still valued; however, a flue gas cleaning system and an integrated system are required to develop in order to prevent harmful substances emission and improve waste-to-energy efficiency. Gasification applied in medical waste management which is more environmentally friendly than incineration should be further explored with reference to coal treatment. Pyrolysis, though, requires high investment costs: its internal rate of return can reach 43% if it is invested as a waste management system [67,83]. Due to the limitation of continuous reaction in wet carbonization, dry carbonization with gas treatment could be further investigated as the generated higher energy density products are value-added based on a relatively simple process. In general, it is important to consider the desired intermediate and final value-added products and the availability of the technology required to solve the challenges during the selection of technologies to be employed in medical waste treatment toward energy profit.
Table 6.
SWOT analysis of waste-to-energy technologies.
4.4.2. Collaboration between Policy and Technology
Due to an increasing amount of medical waste produced, clearer and stricter laws and regulations should be enforced, especially for developing countries, so that potentially efficient medical waste disposal methods and management techniques could be practiced more effectively. The governments are suggested to establish an all-rounded infrastructure for effective waste collection, segregation, transportation and valorization. Initially, waste-to-energy technologies selection could be based on the amount of medical waste. Governments are advised to define the handling capacity of each treatment approach, then the executive parties could follow the rules to choose the appropriate technique in the consideration of the economic, environmental and social benefits. For example, countries or regions which are a challenge by the huge amount of medical waste would be more practical to adopt mature technologies such as incineration considering the efficiency. While in some regions with small amounts of medical waste, more environmental-friendly technologies such as pyrolysis and gasification should be encouraged in the policy. Secondly, waste sorting at the source is the initial key to the waste management system, or the authorities could consider separating medical waste according to the different moisture content. For the dry basis of medical waste, waste-to-energy technologies are selected from thermochemical processes, otherwise, chemical and biochemical treatments will be adopted by the wet content of medical waste. Thirdly, regulations act as restraints when the emission standard is well-defined by governmental authorities. For example, gasification and pyrolysis will be more supportive of the harsher emission requirements when compared with incineration.
5. Conclusions
This article aims at revealing the current status of research and future direction for medical waste management from a comprehensive perspective, which is expected to provide practical guidance on sustainable medical waste treatment. This article has first conducted a bibliometric evaluation of the ongoing scientific development for medical waste, consisting of publication trends, dominant journals, influential nations and research hotspots, with the aid of performance analysis and science mapping. Definition and categories of medical waste are initially introduced. India, China, the UK, Iran and Italy were found as the top five productive countries and keywords of “COVID-19”, “circular economy” and “plastic waste” have been identified as the focus in 2021. Following these findings, the regulation implementations among these five nations have been reviewed to find the gap between scientific advancement and actual policy framework since a crucial characteristic is performed by governmental authority. The results show that developed countries such as UK and Italy have much stricter and more specific guidelines and regulations on medical waste treatment compared with the other three developing countries although India and China rank top two in the number of publications. A series of waste-to-energy methods covering thermochemical, biochemical and chemical conversion technologies were introduced systematically to achieve a circular economy with increasing medical waste. By comparative analysis, thermochemical treatment methods mainly comprising incineration, gasification, pyrolysis and carbonization are regarded as the practical and feasible options currently and their characteristics and limitations were further compared and discussed for a wise selection. Furthermore, a potential match between regulations and technologies was explored according to the real situation. Considering the amount of medical waste produced and the current regulations, it is claimed that medical waste disposal in developing countries would become more effective and efficient by enforcing stricter laws and regulations while in developed countries advanced technologies with low emissions such as gasification are expected to be employed for a sustainable goal.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/en16031074/s1. Dataset generated by Scopus and used in bibliometric analysis.
Author Contributions
Conceptualization, Y.T.C., J.Z. and J.R.; methodology, Y.T.C.; software, Y.T.C.; Validation, Y.T.C. and J.Z.; data curation, Y.T.C., J.Z. and Y.L.; formal analysis, Y.T.C. and Y.W.; writing—original draft, Y.T.C., J.Z. and J.R.; writing—review and editing; Y.T.C., J.Z. and J.R.; supervision, J.R.; funding acquisition, Y.W. and J.R. All authors have read and agreed to the published version of the manuscript.
Funding
The work described in this paper was supported by a grant from Research Grants Council of the Hong Kong Special Administrative Region, China-General Research Fund (Project ID: P0042030, Funding Body Ref. No: 15304222, Project No. B-Q97U), a grant from Research Centre for Resources Engineering towards Carbon Neutrality (RCRE), The Hong Kong Polytechnic University (PolyU) (Project No.1-BBEC, Project ID: P0043023), and the Research Committee of The Hong Kong Polytechnic University under student account code RHPY.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization Health-Care Waste. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 24 December 2022).
- Windfeld, E.S.; Brooks, M.S.L. Medical Waste Management—A Review. J. Environ. Manag. 2015, 163, 98–108. [Google Scholar] [CrossRef]
- Su, G.; Ong, H.C.; Ibrahim, S.; Fattah, I.M.R.; Mofijur, M.; Chong, C.T. Valorisation of Medical Waste through Pyrolysis for a Cleaner Environment: Progress and Challenges. Environ. Pollut. 2021, 279, 116934. [Google Scholar] [CrossRef] [PubMed]
- Worldometer Population by Country (2022)—Worldometer. Available online: https://www.worldometers.info/world-population/population-by-country/ (accessed on 25 December 2022).
- Mofijur, M.; Fattah, I.M.R.; Alam, M.A.; Islam, A.B.M.S.; Ong, H.C.; Rahman, S.M.A.; Najafi, G.; Ahmed, S.F.; Uddin, M.A.; Mahlia, T.M.I. Impact of COVID-19 on the Social, Economic, Environmental and Energy Domains: Lessons Learnt from a Global Pandemic. Sustain. Prod. Consum. 2021, 26, 343–359. [Google Scholar] [CrossRef]
- Chowdhury, T.; Chowdhury, H.; Rahman, M.S.; Hossain, N.; Ahmed, A.; Sait, S.M. Estimation of the Healthcare Waste Generation during COVID-19 Pandemic in Bangladesh. Sci. Total Environ. 2022, 811, 152295. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.S.; Uddin, S.; Sayem, S.M.; Mohib, K.M. Coronavirus Disease 2019 (COVID-19) Induced Waste Scenario: A Short Overview. J. Environ. Chem. Eng. 2021, 9, 104660. [Google Scholar] [CrossRef]
- World Population Review 2022 World Population by Country. Available online: https://worldpopulationreview.com/ (accessed on 25 December 2022).
- World Health Organization Water, Sanitation, Hygiene, and Waste Management for SARS-CoV-2, the Virus That Causes COVID-19. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC-WASH-2020.4 (accessed on 24 December 2022).
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral Load Dynamics and Disease Severity in Patients Infected with SARS-CoV-2 in Zhejiang Province, China, January-March 2020: Retrospective Cohort Study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [PubMed]
- Makarichi, L.; Jutidamrongphan, W.; Techato, K. anan The Evolution of Waste-to-Energy Incineration: A Review. Renew. Sustain. Energy Rev. 2018, 91, 812–821. [Google Scholar] [CrossRef]
- Kargar, S.; Paydar, M.M.; Safaei, A.S. A Reverse Supply Chain for Medical Waste: A Case Study in Babol Healthcare Sector. Waste Manag. 2020, 113, 197–209. [Google Scholar] [CrossRef]
- Jung, S.; Lee, S.; Dou, X.; Kwon, E.E. Valorization of Disposable COVID-19 Mask through the Thermo-Chemical Process. Chem. Eng. J. 2021, 405, 126658. [Google Scholar] [CrossRef]
- Su, M.; Wang, Q.; Li, R. How to Dispose of Medical Waste Caused by COVID-19? A Case Study of China. Int. J. Environ. Res. Public Health 2021, 18, 12127. [Google Scholar] [CrossRef]
- Gao, Q.; Liu, K.; Song, S.; Li, J.; Nie, J.; Shi, Y.; Xia, Y.; Johnson, T.P.; Cook, J. Medical Waste Management of Village Clinics in Rural China. J. Public Health 2022, 30, 1197–1204. [Google Scholar] [CrossRef]
- Kulkarni, S.J. Biomedical Waste Scenario in India—Regulations, Initiatives and Awareness—Biomedical Engineering International. Available online: https://biomedicalengineering.international/biomedical-waste-scenario-in-india-regulations-initiatives-and-awareness/ (accessed on 24 December 2022).
- Goswami, M.; Goswami, P.J.; Nautiyal, S.; Prakash, S. Challenges and Actions to the Environmental Management of Bio-Medical Waste during COVID-19 Pandemic in India. Heliyon 2021, 7, e06313. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; López-Maldonado, E.A.; Khan, N.A.; Villarreal-Gómez, L.J.; Munshi, F.M.; Alsabhan, A.H.; Perveen, K. Current Solid Waste Management Strategies and Energy Recovery in Developing Countries—State of Art Review. Chemosphere 2022, 291, 133088. [Google Scholar] [CrossRef] [PubMed]
- Primc, K.; Dominko, M.; Slabe-Erker, R. 30 Years of Energy and Fuel Poverty Research: A Retrospective Analysis and Future Trends. J. Clean. Prod. 2021, 301, 127003. [Google Scholar] [CrossRef]
- Donthu, N.; Kumar, S.; Mukherjee, D.; Pandey, N.; Lim, W.M. How to Conduct a Bibliometric Analysis: An Overview and Guidelines. J. Bus. Res. 2021, 133, 285–296. [Google Scholar] [CrossRef]
- Baker, H.K.; Kumar, S.; Pandey, N. Forty Years of the Journal of Futures Markets: A Bibliometric Overview. J. Futures Mark. 2021, 41, 1027–1054. [Google Scholar] [CrossRef]
- Dominko, M.; Verbič, M. The Economics of Subjective Well-Being: A Bibliometric Analysis. J. Happiness Stud. 2019, 20, 1973–1994. [Google Scholar] [CrossRef]
- van Eck, N.J.; Waltman, L. Software Survey: VOSviewer, a Computer Program for Bibliometric Mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Taşkın, Z.; Al, U. A Content-Based Citation Analysis Study Based on Text Categorization. Scientometrics 2018, 114, 335–357. [Google Scholar] [CrossRef]
- Klemeš, J.J.; van Fan, Y.; Tan, R.R.; Jiang, P. Minimising the Present and Future Plastic Waste, Energy and Environmental Footprints Related to COVID-19. Renew. Sustain. Energy Rev. 2020, 127, 109883. [Google Scholar] [CrossRef]
- Lambert, S.; Wagner, M. Environmental Performance of Bio-Based and Biodegradable Plastics: The Road Ahead. Chem. Soc. Rev. 2017, 46, 6855–6871. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.B.; Vanapalli, K.R.; Cheela, V.S.; Ranjan, V.P.; Jaglan, A.K.; Dubey, B.; Goel, S.; Bhattacharya, J. Challenges, Opportunities, and Innovations for Effective Solid Waste Management during and Post COVID-19 Pandemic. Resour. Conserv. Recycl. 2020, 162, 105052. [Google Scholar] [CrossRef] [PubMed]
- Sangkham, S. Face Mask and Medical Waste Disposal during the Novel COVID-19 Pandemic in Asia. Case Stud. Chem. Environ. Eng. 2020, 2, 100052. [Google Scholar] [CrossRef]
- Yu, H.; Sun, X.; Solvang, W.D.; Zhao, X. Reverse Logistics Network Design for Effective Management of Medical Waste in Epidemic Outbreaks: Insights from the Coronavirus Disease 2019 (COVID-19) Outbreak in Wuhan (China). Int. J. Environ. Res. Public Health 2020, 17, 1770. [Google Scholar] [CrossRef]
- Ilyas, S.; Srivastava, R.R.; Kim, H. Disinfection technology and strategies for COVID-19 hospital and bio-medical waste management. Sci. Total Environ. 2020, 749, 141652. [Google Scholar] [CrossRef]
- Kulkarni, B.N.; Anantharama, V. Repercussions of COVID-19 pandemic on municipal solid waste management: Challenges and opportunities. Sci. Total Environ. 2020, 743, 140693. [Google Scholar] [CrossRef]
- Chauhan, A.; Singh, A. A hybrid multi-criteria decision making method approach for selecting a sustainable location of healthcare waste disposal facility. J. Clean. Prod. 2016, 139, 1001–1010. [Google Scholar] [CrossRef]
- Caniato, M.; Tudor, T.; Vaccari, M. International governance structures for health-care waste management: A systematic review of scientific literature. J. Environ. Manag. 2015, 153, 93–107. [Google Scholar] [CrossRef]
- Eckelman, M.; Mosher, M.; Gonzalez, A.; Sherman, J. Comparative Life Cycle Assessment of Disposable and Reusable Laryngeal Mask Airways. Anesth. Analg. 2012, 114, 1067–1072. [Google Scholar] [CrossRef]
- Ranjbari, M.; Shams Esfandabadi, Z.; Zanetti, M.C.; Scagnelli, S.D.; Siebers, P.O.; Aghbashlo, M.; Peng, W.; Quatraro, F.; Tabatabaei, M. Three Pillars of Sustainability in the Wake of COVID-19: A Systematic Review and Future Research Agenda for Sustainable Development. J. Clean. Prod. 2021, 297, 126660. [Google Scholar] [CrossRef]
- Fabregat-Aibar, L.; Barberà-Mariné, M.G.; Terceño, A.; Pié, L. A Bibliometric and Visualization Analysis of Socially Responsible Funds. Sustainability 2019, 11, 2526. [Google Scholar] [CrossRef]
- Rowan, N.J.; Laffey, J.G. Unlocking the Surge in Demand for Personal and Protective Equipment (PPE) and Improvised Face Coverings Arising from Coronavirus Disease (COVID-19) Pandemic—Implications for Efficacy, Re-Use and Sustainable Waste Management. Sci. Total Environ. 2021, 752, 142259. [Google Scholar] [CrossRef] [PubMed]
- Das, A.K.; Islam, M.N.; Billah, M.M.; Sarker, A. COVID-19 Pandemic and Healthcare Solid Waste Management Strategy—A Mini-Review. Sci. Total Environ. 2021, 778, 146220. [Google Scholar] [CrossRef] [PubMed]
- Bandela, D.R. COVID-19: Here Is What You Should Do to Safely Dispose Your Used Mask—DownToEarth. Available online: https://www.downtoearth.org.in/news/waste/covid-19-here-is-what-you-should-do-to-safely-dispose-your-used-mask-71006 (accessed on 24 December 2022).
- Asim, N.; Badiei, M.; Sopian, K. Review of the Valorization Options for the Proper Disposal of Face Masks during the COVID-19 Pandemic. Environ. Technol. Innov. 2021, 23, 101797. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Song, Y.; Liu, Y.; Zhong, Y. Assessment of Medical Waste Generation, Associated Environmental Impact, and Management Issues after the Outbreak of COVID-19: A Case Study of the Hubei Province in China. PLoS ONE 2022, 17, e0259207. [Google Scholar] [CrossRef] [PubMed]
- Kang, A.; Ren, L.; Hua, C.; Song, H.; Dong, M.; Fang, Z.; Zhu, M. Environmental Management Strategy in Response to COVID-19 in China: Based on Text Mining of Government Open Information. Sci. Total Environ. 2021, 769, 145158. [Google Scholar] [CrossRef]
- Yang, L.; Yu, X.; Wu, X.; Wang, J.; Yan, X.; Jiang, S.; Chen, Z. Emergency Response to the Explosive Growth of Health Care Wastes during COVID-19 Pandemic in Wuhan, China. Resour. Conserv. Recycl. 2021, 164, 105074. [Google Scholar] [CrossRef]
- Rizan, C.; Bhutta, M.F.; Reed, M.; Lillywhite, R. The Carbon Footprint of Waste Streams in a UK Hospital. J. Clean. Prod. 2021, 286, 125446. [Google Scholar] [CrossRef]
- UK Health Security Agency Living Safely with Respiratory Infections, Including COVID-19—GOV.UK. Available online: https://www.gov.uk/guidance/living-safely-with-respiratory-infections-including-covid-19 (accessed on 24 December 2022).
- Ministry of Social Affairs and Health. Waste Management Prepared for the Epidemic Caused by the Coronavirus. Available online: https://stm.fi/documents/1271139/21475529/Waste+management+prepared+for+the+epidemic+caused+by+the+coronavirus.pdf/9e77c1eb-2fa5-2cdb-a4b3-de80792a5d51/Waste+management+prepared+for+the+epidemic+caused+by+the+coronavirus.pdf (accessed on 24 December 2022).
- Shams, M.; Alam, I.; Mahbub, M.S. Plastic Pollution during COVID-19: Plastic Waste Directives and Its Long-Term Impact on the Environment. Environ. Adv. 2021, 5, 100119. [Google Scholar] [CrossRef]
- Hossini, H.; Atashkar, S.; Massahi, T. Face Mask Consumption and Medical Waste Generation during the COVID-19 Pandemic in Iran: Challenges and Problems. Int. J. Health Life Sci. 2021, 7, 115046. [Google Scholar] [CrossRef]
- Torkashvand, J.; Pasalari, H.; Jonidi-Jafari, A.; Kermani, M.; Nasri, O.; Farzadkia, M. Medical Waste Management in Iran and Comparison with Neighbouring Countries. Int. J. Environ. Anal. Chem. 2020, 102, 2805–2818. [Google Scholar] [CrossRef]
- Puertas, R.; Carracedo, P.; Marti, L. Environmental Policies for the Treatment of Waste Generated by COVID-19: Text Mining Review. Waste Manag. Res. 2022, 40, 1480–1493. [Google Scholar] [CrossRef] [PubMed]
- Ragazzi, M.; Rada, E.C.; Schiavon, M. Municipal Solid Waste Management during the SARS-CoV-2 Outbreak and Lockdown Ease: Lessons from Italy. Sci. Total Environ. 2020, 745, 141159. [Google Scholar] [CrossRef] [PubMed]
- Talluri, M. Emergenza COVID-19: Indicazioni SNPA Sulla Gestione Dei Rifiuti|SNPA—Sistema Nazionale Protezione Ambiente. Available online: https://www.snpambiente.it/2020/03/24/emergenza-covid-19-indicazioni-snpa-sulla-gestione-dei-rifiuti/ (accessed on 24 December 2022).
- Hahladakis, J.N.; Iacovidou, E.; Gerassimidou, S. Plastic Waste in a Circular Economy. In Plastic Waste and Recycling; Academic Press: Cambridge, MA, USA, 2020; pp. 481–512. [Google Scholar] [CrossRef]
- Teymourian, T.; Teymoorian, T.; Kowsari, E.; Ramakrishna, S. Challenges, Strategies, and Recommendations for the Huge Surge in Plastic and Medical Waste during the Global COVID-19 Pandemic with Circular Economy Approach. Mater. Circ. Econ. 2021, 3, 6. [Google Scholar] [CrossRef]
- Helsen, L. Waste-to-Energy through thermochemical processes: Matching waste with process. In Proceedings of the 1st International Academic Symposium on Enhanced Landfill Mining, Houthalen-Helchteren, Belgium, 4–6 October 2010. [Google Scholar]
- World Energy Council World Energy Resources 2016|World Energy Council. Available online: https://www.worldenergy.org/publications/entry/world-energy-resources-2016 (accessed on 25 December 2022).
- Khan, I.; Kabir, Z. Waste-to-Energy Generation Technologies and the Developing Economies: A Multi-Criteria Analysis for Sustainability Assessment. Renew Energy 2020, 150, 320–333. [Google Scholar] [CrossRef]
- Shareefdeen, Z. Hazardous Waste Management: Advances in Chemical and Industrial Waste Treatment and Technologie; Springer: Berlin/Heidelberg, Germany, 2022; ISBN 9783030952617. [Google Scholar]
- Kassim, F.O.; Thomas, C.P.; Afolabi, O.O. Integrated conversion technologies for sustainable agri-food waste valorization: A critical review. Biomass Bioenergy 2022, 156, 106314. [Google Scholar] [CrossRef]
- Costiuc, L.; Tierean, M.; Baltes, L.; Patachia, S. Experimental Investigation on the Heat of Combustion for Solid Plastic Waste Mixtures. Environ. Eng. Manag. J. 2015, 14, 1295–1302. [Google Scholar] [CrossRef]
- Thind, P.S.; Sareen, A.; Singh, D.D.; Singh, S.; John, S. Compromising Situation of India’s Bio-Medical Waste Incineration Units during Pandemic Outbreak of COVID-19: Associated Environmental-Health Impacts and Mitigation Measures. Environ. Pollut. 2021, 276, 116621. [Google Scholar] [CrossRef]
- Geyer, R.; Jambeck, J.R.; Law, K.L. Production, Use, and Fate of All Plastics Ever Made. Sci. Adv. 2017, 3, e1700782. [Google Scholar] [CrossRef]
- Awasthi, M.K.; Sarsaiya, S.; Chen, H.; Wang, Q.; Wang, M.; Awasthi, S.K.; Li, J.; Liu, T.; Pandey, A.; Zhang, Z. Global Status of Waste-to-Energy Technology. In Current Developments in Biotechnology and Bioengineering: Waste Treatment Processes for Energy Generation; Elsevier: Amsterdam, The Netherlands, 2019; pp. 31–52. [Google Scholar] [CrossRef]
- Zhang, F.; Zhao, Y.; Wang, D.; Yan, M.; Zhang, J.; Zhang, P.; Ding, T.; Chen, L.; Chen, C. Current Technologies for Plastic Waste Treatment: A Review. J. Clean. Prod. 2021, 282, 124523. [Google Scholar] [CrossRef]
- Sun, Y.; Qin, Z.; Tang, Y.; Huang, T.; Ding, S.; Ma, X. Techno-Environmental-Economic Evaluation on Municipal Solid Waste (MSW) to Power/Fuel by Gasification-Based and Incineration-Based Routes. J. Environ. Chem. Eng. 2021, 9, 106108. [Google Scholar] [CrossRef]
- Guan, G.; Kaewpanha, M.; Hao, X.; Abudula, A. Catalytic Steam Reforming of Biomass Tar: Prospects and Challenges. Renew. Sustain. Energy Rev. 2016, 58, 450–461. [Google Scholar] [CrossRef]
- Purnomo, C.W.; Kurniawan, W.; Aziz, M. Technological Review on Thermochemical Conversion of COVID-19-Related Medical Wastes. Resour. Conserv. Recycl. 2021, 167, 105429. [Google Scholar] [CrossRef] [PubMed]
- Hazan, M.A.; Mamat, M.S.; Ismail, I.; Hussein, M.Z.; Yaakob, Y. Fractionation of Waste Nitrile Butadiene Rubber (NBR) Latex Sludge. AIP Conf. Proc. 2019, 2151, 020012. [Google Scholar] [CrossRef]
- Wang, J.; Shen, J.; Ye, D.; Yan, X.; Zhang, Y.; Yang, W.; Li, X.; Wang, J.; Zhang, L.; Pan, L. Disinfection Technology of Hospital Wastes and Wastewater: Suggestions for Disinfection Strategy during Coronavirus Disease 2019 (COVID-19) Pandemic in China. Environ. Pollut. 2020, 262, 114665. [Google Scholar] [CrossRef] [PubMed]
- Fakayode, O.A.; Aboagarib, E.A.A.; Zhou, C.; Ma, H. Co-Pyrolysis of Lignocellulosic and Macroalgae Biomasses for the Production of Biochar—A Review. Bioresour. Technol. 2020, 297, 122408. [Google Scholar] [CrossRef] [PubMed]
- Aragaw, T.A.; Mekonnen, B.A. Current Plastics Pollution Threats Due to COVID-19 and Its Possible Mitigation Techniques: A Waste-to-Energy Conversion via Pyrolysis. Environ. Syst. Res. 2021, 10, 8. [Google Scholar] [CrossRef]
- Singh, R.K.; Ruj, B. Time and Temperature Depended Fuel Gas Generation from Pyrolysis of Real World Municipal Plastic Waste. Fuel 2016, 174, 164–171. [Google Scholar] [CrossRef]
- Antoniou, N.A.; Zorpas, A.A. Quality protocol and procedure development to define end-of-waste criteria for tire pyrolysis oil in the framework of circular economy strategy. Waste Manag. 2019, 95, 161–170. [Google Scholar] [CrossRef]
- Sikarwar, V.S.; Hrabovský, M.; van Oost, G.; Pohořelý, M.; Jeremiáš, M. Progress in Waste Utilization via Thermal Plasma. Prog. Energy Combust. Sci. 2020, 81, 100873. [Google Scholar] [CrossRef]
- Kaushal, R.; Rohit; Dhaka, A.K. A Comprehensive Review of the Application of Plasma Gasification Technology in Circumventing the Medical Waste in a Post-COVID-19 Scenario. Biomass Convers. Biorefin. 2022, 1, 1–16. [Google Scholar] [CrossRef]
- Heberlein, J.; Murphy, A.B. Thermal Plasma Waste Treatment. J. Phys. D Appl. Phys. 2008, 41, 053001. [Google Scholar] [CrossRef]
- Erdogan, A.A.; Yilmazoglu, M.Z. Plasma Gasification of the Medical Waste. Int. J. Hydrogen Energy 2021, 46, 29108–29125. [Google Scholar] [CrossRef] [PubMed]
- Munir, M.T.; Mardon, I.; Al-Zuhair, S.; Shawabkeh, A.; Saqib, N.U. Plasma Gasification of Municipal Solid Waste for Waste-to-Value Processing. Renew. Sustain. Energy Rev. 2019, 116, 109461. [Google Scholar] [CrossRef]
- Zaini, I.N.; Novianti, S.; Nurdiawati, A.; Irhamna, A.R.; Aziz, M.; Yoshikawa, K. Investigation of the Physical Characteristics of Washed Hydrochar Pellets Made from Empty Fruit Bunch. Fuel Process. Technol. 2017, 160, 109–120. [Google Scholar] [CrossRef]
- Nobre, C.; Alves, O.; Longo, A.; Vilarinho, C.; Gonçalves, M. Torrefaction and Carbonization of Refuse Derived Fuel: Char Characterization and Evaluation of Gaseous and Liquid Emissions. Bioresour. Technol. 2019, 285, 121325. [Google Scholar] [CrossRef]
- Joseph, B.; James, J.; Kalarikkal, N.; Thomas, S. Recycling of Medical Plastics. Adv. Ind. Eng. Polym. Res. 2021, 4, 199–208. [Google Scholar] [CrossRef]
- Darmawan, A.; Budianto, D.; Aziz, M.; Tokimatsu, K. Retrofitting Existing Coal Power Plants through Cofiring with Hydrothermally Treated Empty Fruit Bunch and a Novel Integrated System. Appl. Energy 2017, 204, 1138–1147. [Google Scholar] [CrossRef]
- Al-Salem, S.M.; Lettieri, P.; Baeyens, J. Recycling and Recovery Routes of Plastic Solid Waste (PSW): A Review. Waste Manag. 2009, 29, 2625–2643. [Google Scholar] [CrossRef]
- Munir, D.; Irfan, M.F.; Usman, M.R. Hydrocracking of Virgin and Waste Plastics: A Detailed Review. Renew. Sustain. Energy Rev. 2018, 90, 490–515. [Google Scholar] [CrossRef]
- Liu, S.; Kots, P.A.; Vance, B.C.; Danielson, A.; Vlachos, D.G. Plastic Waste to Fuels by Hydrocracking at Mild Conditions. Sci. Adv. 2021, 7, 8283–8304. [Google Scholar] [CrossRef] [PubMed]
- Ragaert, K.; Delva, L.; van Geem, K. Mechanical and Chemical Recycling of Solid Plastic Waste. Waste Manag. 2017, 69, 24–58. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Ahmad, N.; Maafa, I.M.; Ahmed, U.; Akhter, P.; Shehzad, N.; Amjad, U.; Hussain, M. Thermal Conversion of Polystyrene Plastic Waste to Liquid Fuel via Ethanolysis. Fuel 2020, 279, 118498. [Google Scholar] [CrossRef]
- Naik, S.N.; Goud, V.V.; Rout, P.K.; Dalai, A.K. Production of First and Second Generation Biofuels: A Comprehensive Review. Renew. Sustain. Energy Rev. 2010, 14, 578–597. [Google Scholar] [CrossRef]
- Ahamed Kameel, N.I.; Wan Daud, W.M.A.; Abdul Patah, M.F.; Mohd Zulkifli, N.W. Influence of Reaction Parameters on Thermal Liquefaction of Plastic Wastes into Oil: A Review. Energy Convers. Manag. X 2022, 14, 100196. [Google Scholar] [CrossRef]
- Vicente, G.; Aguado, J.; Serrano, D.P.; Sánchez, N. HDPE Chemical Recycling Promoted by Phenol Solvent. J. Anal. Appl. Pyrolysis 2009, 85, 366–371. [Google Scholar] [CrossRef]
- Seshasayee, M.S.; Savage, P.E. Oil from Plastic via Hydrothermal Liquefaction: Production and Characterization. Appl. Energy 2020, 278, 115673. [Google Scholar] [CrossRef]
- Khoshand, A.; Bafrani, A.H.; Zahedipour, M.; Mirbagheri, S.A.; Ehtehsami, M. Prevention of Landfill Pollution by Multicriteria Spatial Decision Support Systems (MC-SDSS): Development, Implementation, and Case Study. Environ. Sci. Pollut. Res. 2018, 25, 8415–8431. [Google Scholar] [CrossRef]
- Kumar, M.; Dutta, S.; You, S.; Luo, G.; Zhang, S.; Show, P.L.; Sawarkar, A.D.; Singh, L.; Tsang, D.C.W. A Critical Review on Biochar for Enhancing Biogas Production from Anaerobic Digestion of Food Waste and Sludge. J. Clean. Prod. 2021, 305, 127143. [Google Scholar] [CrossRef]
- Waqas, M.; Rehan, M.; Khan, M.D.; Nizami, A.S. Conversion of Food Waste to Fermentation Products. Encycl. Food Secur. Sustain. 2019, 501–509. [Google Scholar] [CrossRef]
- Chilakamarry, C.R.; Mimi Sakinah, A.M.; Zularisam, A.W.; Sirohi, R.; Khilji, I.A.; Ahmad, N.; Pandey, A. Advances in Solid-State Fermentation for Bioconversion of Agricultural Wastes to Value-Added Products: Opportunities and Challenges. Bioresour. Technol. 2022, 343, 126065. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Luo, J.; Fang, S.; Huang, W.; Zhang, Y.; Zhang, L.; Cheng, X.; Du, W.; Fang, F.; Cao, J.; et al. Mechanisms of Allicin Exposure for the Sludge Fermentation Enhancement: Focusing on the Fermentation Processes and Microbial Metabolic Traits. J. Environ. Sci. 2022, 115, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Petibon, R.; Aiken, C.P.; Ma, L.; Xiong, D.; Dahn, J.R. The Use of Ethyl Acetate as a Sole Solvent in Highly Concentrated Electrolyte for Li-Ion Batteries. Electrochim. Acta 2015, 154, 287–293. [Google Scholar] [CrossRef]
- Fattahi, N.; Triantafyllidis, K.; Luque, R.; Ramazani, A. Zeolite-Based Catalysts: A Valuable Approach toward Ester Bond Formation. Catalysts 2019, 9, 758. [Google Scholar] [CrossRef]
- Hazmi, B.; Rashid, U.; Kawi, S.; Mokhtar, W.N.A.W.; Yaw, T.C.S.; Moser, B.R.; Alsalme, A. Palm Fatty Acid Distillate Esterification Using Synthesized Heterogeneous Sulfonated Carbon Catalyst from Plastic Waste: Characterization, Catalytic Efficacy and Stability, and Fuel Properties. Process Saf. Environ. Prot. 2022, 162, 1139–1151. [Google Scholar] [CrossRef]
- Kampf, G.; Voss, A.; Scheithauer, S. Inactivation of Coronaviruses by Heat. J. Hosp. Infect. 2020, 105, 348. [Google Scholar] [CrossRef]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.A.; Hui, K.P.Y.; Yen, H.L.; Chan, M.C.W.; Peiris, M.; Poon, L.L.M. Stability of SARS-CoV-2 in Different Environmental Conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Mabrouki, J.; Abbassi, M.A.; Khiari, B.; Jellali, S.; Zorpas, A.A.; Jeguirim, M. The dairy biorefinery: Integrating treatment process for Tunisian cheese whey valorization. Chemosphere 2022, 293, 133567. [Google Scholar] [CrossRef]
- Kumar, A.; Samadder, S.R. A Review on Technological Options of Waste to Energy for Effective Management of Municipal Solid Waste. Waste Manag. 2017, 69, 407–422. [Google Scholar] [CrossRef]
- Nobre, C.; Vilarinho, C.; Alves, O.; Mendes, B.; Gonçalves, M. Upgrading of Refuse Derived Fuel through Torrefaction and Carbonization: Evaluation of RDF Char Fuel Properties. Energy 2019, 181, 66–76. [Google Scholar] [CrossRef]
- Shen, Y.; Yu, S.; Ge, S.; Chen, X.; Ge, X.; Chen, M. Hydrothermal Carbonization of Medical Wastes and Lignocellulosic Biomass for Solid Fuel Production from Lab-Scale to Pilot-Scale. Energy 2017, 118, 312–323. [Google Scholar] [CrossRef]
- Datta, P.; Mohi, G.K.; Chander, J. Biomedical Waste Management in India: Critical Appraisal. J. Lab. Physicians 2018, 10, 006–014. [Google Scholar] [CrossRef] [PubMed]
- Moya, D.; Aldás, C.; López, G.; Kaparaju, P. Municipal Solid Waste as a Valuable Renewable Energy Resource: A Worldwide Opportunity of Energy Recovery by Using Waste-To-Energy Technologies. Energy Procedia 2017, 134, 286–295. [Google Scholar] [CrossRef]
- Yek, P.N.Y.; Cheng, Y.W.; Liew, R.K.; Wan Mahari, W.A.; Ong, H.C.; Chen, W.H.; Peng, W.; Park, Y.K.; Sonne, C.; Kong, S.H.; et al. Progress in the Torrefaction Technology for Upgrading Oil Palm Wastes to Energy-Dense Biochar: A Review. Renew. Sustain. Energy Rev. 2021, 151, 111645. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).