
Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU



Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
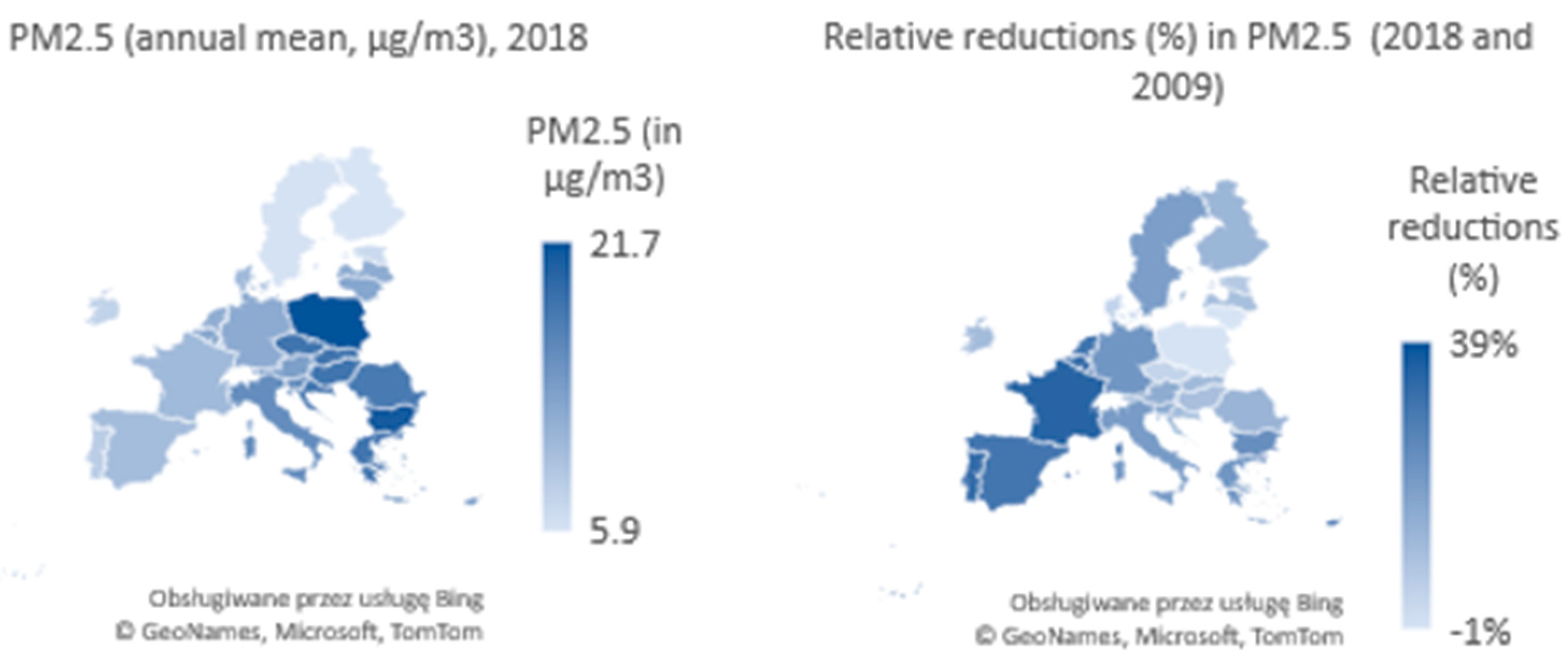
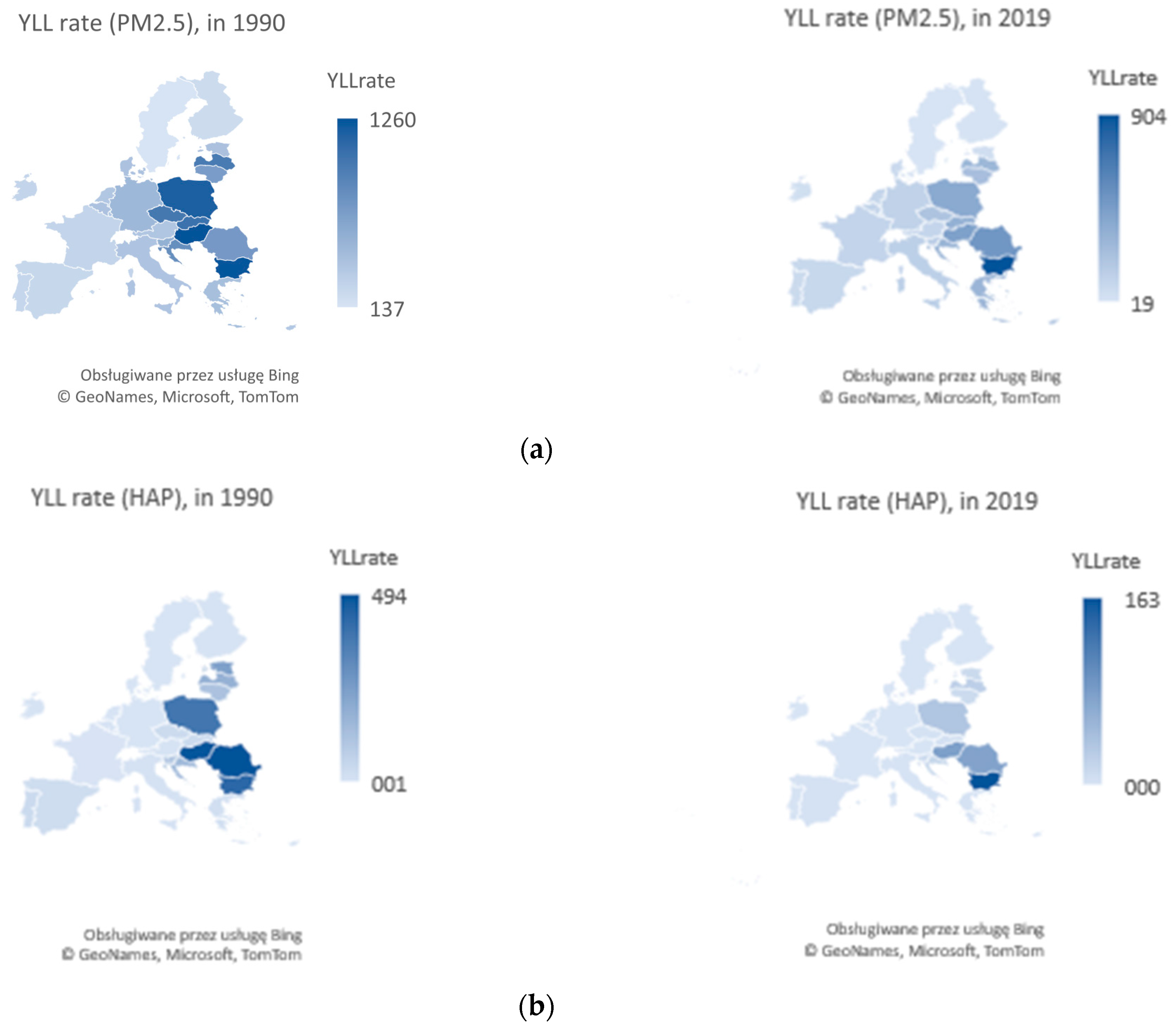
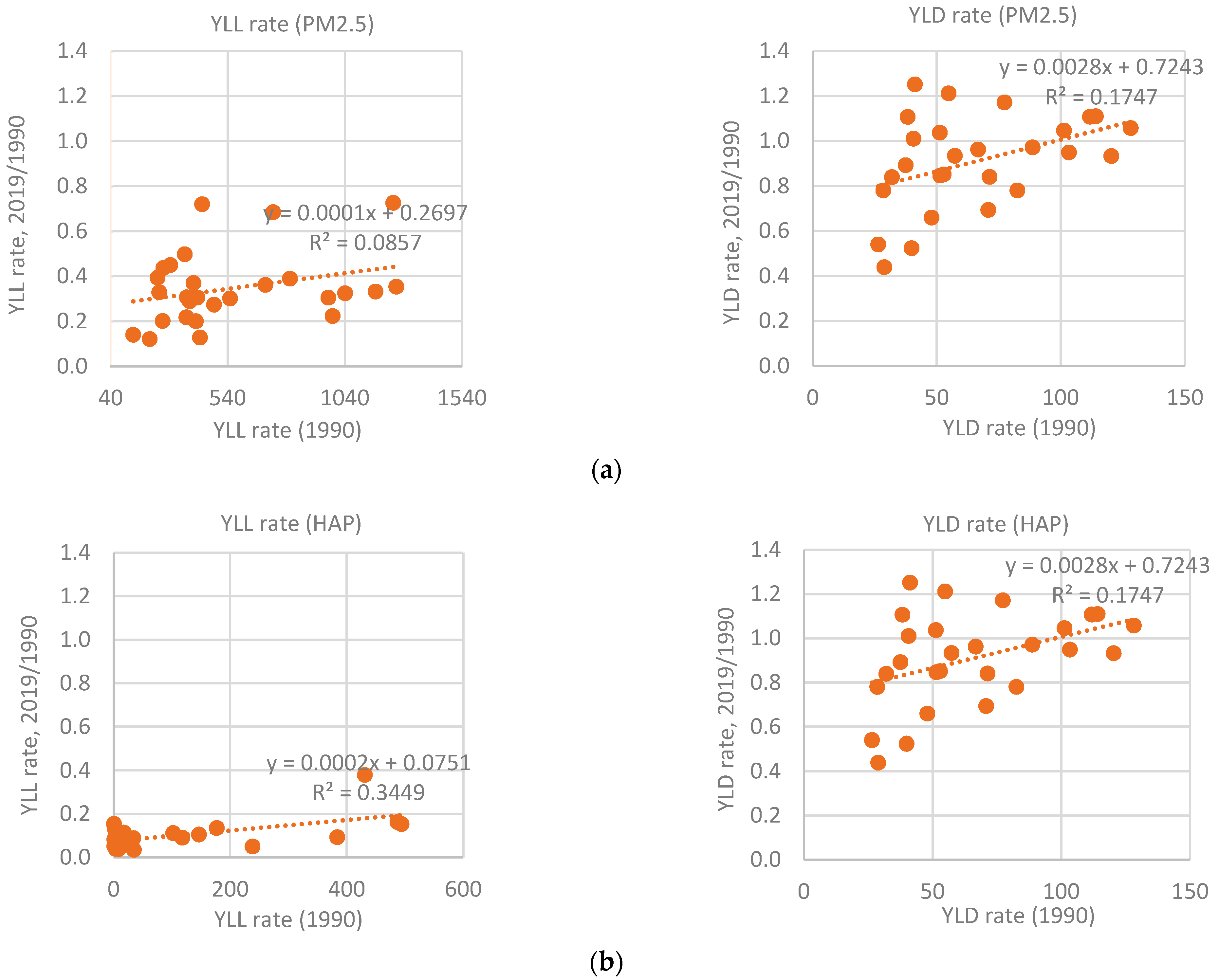
- Ambient particulate matter pollution: annual average daily exposure to outdoor air concentrations of particulate matter with an aerodynamic diameter of ≤2.5 μm (PM 2.5), measured in μg/m³,
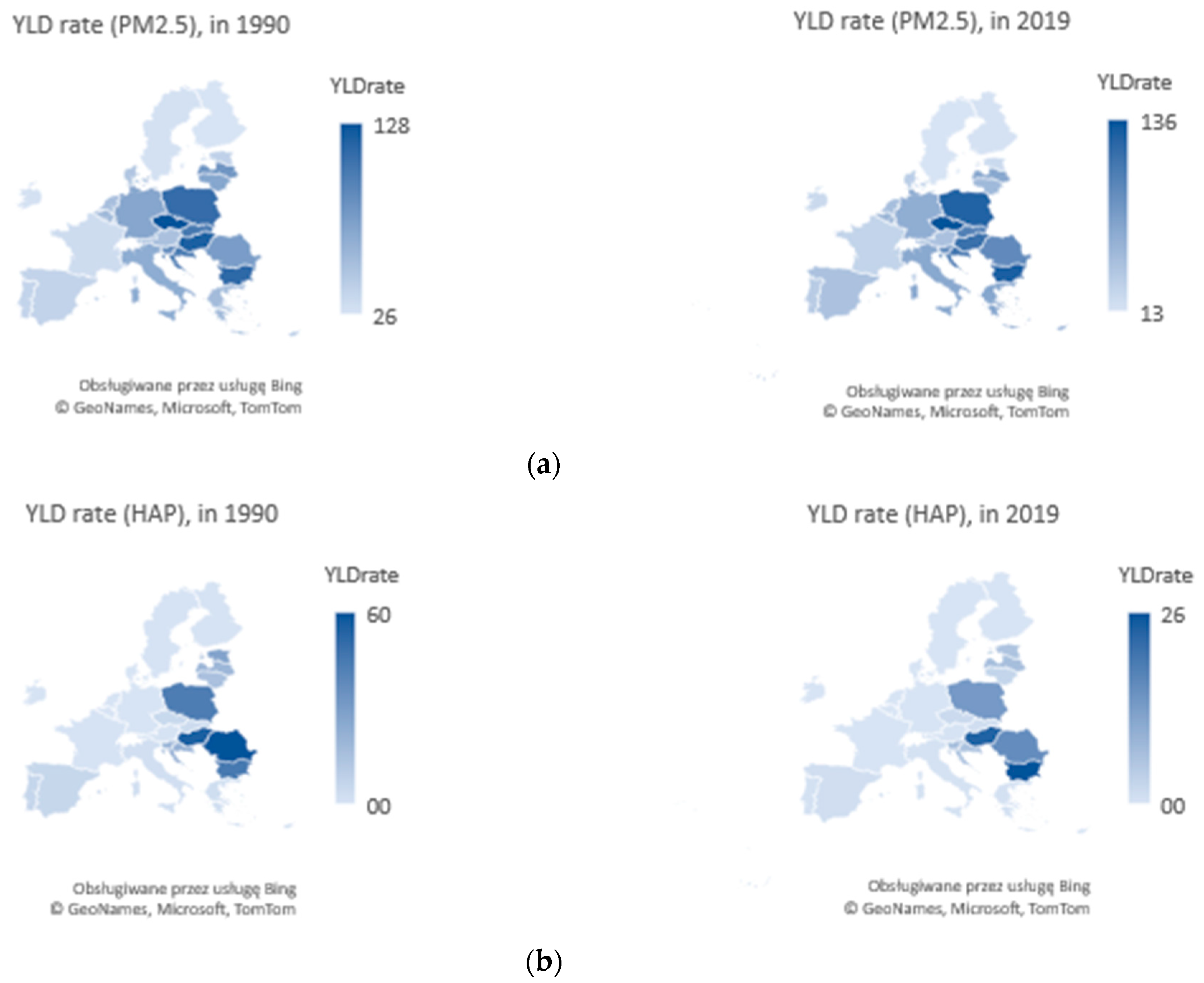
- Household air pollution (HAP) from solid fuels: individual exposure to PM 2.5 due to use of solid fuels.
4. Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Busse, R.; Blümel, M.; Scheller-Kreinsen, D.; Zentner, D. Tackling Chronic Disease in Europe. In Strategies, Interventions and Challenges; World Health Organization: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/326484 (accessed on 10 May 2022).
- Bartley, M.; Sacker, A.; Clarke, P. Employment status, employment conditions, and limiting illness: Prospective evidence from the British household panel survey 1991–2001. J. Epidemiol. Community Health 2004, 58, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Haan, P.; Myck, M. Dynamics of health and labor market risks. J. Health Econ. 2009, 28, 1116–1125. [Google Scholar] [CrossRef] [PubMed]
- Aghion, P.; Howitt, P.; Murtin, F. The relationship between health and growth: When Lucas meets Nelson-Phelps. Natl. Bur. Econ. Res. 2010, w15813, 94–126. [Google Scholar] [CrossRef]
- Jakubowska, A.; Horváthová, Z. Economic Growth and Health: A Comparative Study of the EU Countries. Econ. Sociol. 2016, 9, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Jakubowska, A.; Bilan, S.; Werbiński, J. Chronic diseases and labour resources: “Old and new” European Union member states. J. Int. Stud. 2021, 14, 129–138. [Google Scholar] [CrossRef]
- William, J.; Lewis, M. Health Investments and Economic Growth: Macroeconomic Evidence and Microeconomic Foundations. In World Bank Policy Research Working Paper Series; World Bank: Washington, DC, USA, 2009. [Google Scholar]
- Van Rijn, R.M.; Robroek, S.J.; Brouwer, S.; Burdorf, A. Influence of poor health on exit from paid employment: A systematic review. Occup. Environ. Med. 2014, 71, 295–301. [Google Scholar] [CrossRef]
- Rice, N.E.; Lang, I.A.; Henley, W.; Melzer, D. Common health predictors of early retirement: Findings from the English Longitudinal Study of Ageing. Age Ageing 2011, 40, 54–61. [Google Scholar] [CrossRef]
- Bloom, D.E.; Canning, D.; Fink, G. Disease and development revisited. J. Political Econ. 2014, 122, 1355–1366. [Google Scholar] [CrossRef]
- Abegunde, D.; Stanciole, A. An Estimation of the Economic Impact of Chronic Noncommunicable Diseases in Selected Countries; Working paper; WHO Department of Chronic Diseases and Health Promotion (CHP): Geneva, Switzerland, 2006. [Google Scholar]
- Brown, S.; Sessions, J.G. The economics of absence: Theory and evidence. J. Econ. Surv. 1996, 10, 23–53. [Google Scholar] [CrossRef]
- Radlińska, K.; Klonowska-Matynia, M.; Jakubowska, A.; Kwiatkowski, G. Labor hoarding: An old phenomena in modern times? Case study for EU countries. J. Bus. Econ. Manag. 2020, 21, 872–889. [Google Scholar] [CrossRef]
- Mannino, D.M.; Buist, A.S. Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 2007, 370, 765–773. [Google Scholar] [CrossRef]
- Brownson, R.C.; Haire-Joshu, D.; Luke, D.A. Shaping the context of health: A review of environmental and policy approaches in the prevention of chronic diseases. Annu. Rev. Public Health 2006, 27, 341–370. [Google Scholar] [CrossRef] [PubMed]
- Rosário Filho, N.A.; Urrutia-Pereira, M.; d′Amato, G.; Cecchi, L.; Ansotegui, I.J.; Galán, C.; Pomés, A.; Murrieta-Aguttes, M.; Caraballo, L.; Rouadi, P.; et al. Air pollution and indoor settings. World Allergy Organ. J. 2021, 14, 100499. [Google Scholar] [CrossRef] [PubMed]
- Łyszczarz, B.; Sowa, K. Production losses due to mortality associated with modifiable health risk factors in Poland. Eur. J. Health Econ. 2022, 23, 33–45. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Hammer, M.S.; van Donkelaar, A.; Li, C.; Lyapustin, A.; Sayer, A.M.; Hsu, N.C.; Levy, R.C.; Garay, M.J.; Kalashnikova, O.V.; Kahn, R.A.; et al. Global estimates and long-term trends of fine particulate matter concentrations (1998–2018). Environ. Sci. Technol. 2020, 54, 7879–7890. [Google Scholar] [CrossRef]
- European Environment Agency; González Ortiz, A.; Guerreiro, C.; Soares, J. Air Quality in Europe: 2020 Report; European Environment Agency, Publications Office: Copenhagen, Denmark, 2020. [CrossRef]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923. [Google Scholar] [CrossRef]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, A.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2020; Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 26 May 2022).
- Pimpin, L.; Retat, L.; Fecht, D.; de Preux, L.; Sassi, F.; Gulliver, J.; Belloni, A.; Ferguson, B.; Corbould, E.; Jaccard, A.; et al. Estimating the cross of air pollution to the National Health Service and social care: An assessment and forecast up to 2035. PLoS Med. 2018, 15, e1002602. [Google Scholar] [CrossRef]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.D., III; Thurston, G.; Calle, E.E.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, USA, 2009; Volume 140. [Google Scholar]
- Qiu, H.; Tan, K.; Long, F.; Wang, L.; Yu, H.; Deng, R.; Long, H.; Zhang, Y.; Pan, J. The burden of COPD morbidity attributable to the interaction between ambient air pollution and temperature in Chengdu, China. Int. J. Environ. Res. Public Health 2018, 15, 492. [Google Scholar] [CrossRef]
- Mills, I.C.; Atkinson, R.W.; Kang, S.; Walton, H.; Anderson, H.R. Quantitative systematic review of the associations between short-term exposure to nitrogen dioxide and mortality and hospital admissions. BMJ Open 2015, 5, e006946. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.T.; Pope, C.A., III; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrator risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Analitis, A.; De’Donato, F.; Scortichini, M.; Lanki, T.; Basagana, X.; Ballester, F.; Astrom, C.; Paldy, A.; Pascal, M.; Gasparrini, A.; et al. Synergistic effects of ambient temperature and air pollution on health in Europe: Results from the PHASE project. Int. J. Environ. Res. Public Health 2018, 15, 1856. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.A. systematic review of the relation between long-term exposure to ambient air pollution and chronic diseases. Rev. Environ. Health 2008, 23, 243–298. [Google Scholar] [CrossRef] [PubMed]
- Holland, M. Cost-Benefit Analysis of Final Policy Scenarios for the EU Clean Air Package; European Maritime Safety Agency: Lisbon, Portugal, 2014. Available online: https://policycommons.net/artifacts/1955087/cost-benefit-analysis-of-final-policy-scenarios-for-the-eu-clean-air-package/2706855/ (accessed on 10 May 2022).
- Martinez, G.S.; Spadaro, J.V.; Chapizanis, D.; Kendrovski, V.; Kochubovski, M.; Mudu, P. Health impacts and economic costs of air pollution in the metropolitan area of Skopje. Int. J. Environ. Res. Public Health 2018, 15, 626. [Google Scholar] [CrossRef] [PubMed]
- Hanly, P.; Soerjomataram, I.; Sharp, L. Measuring the societal burden of cancer: The cost of lost productivity due to premature cancer-related mortality in Europe. Int. J. Cancer 2015, 136, E136–E145. [Google Scholar] [CrossRef]
- Dechezleprêtre, A.; Rivers, N.; Stadler, B. The Economic Cost of Air Pollution: Evidence from Europe. In OECD Economics Department Working Papers; No. 1584; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Gouveia, N. Addressing Environmental Health Inequalities. Int. J. Environ. Res. Public Health 2016, 13, 858. [Google Scholar] [CrossRef]
- Ashraf, Q.H.; Lester, A.; Weil, D.N. When Does Improving Health Raise GDP? NBER Macroecon. Annu. 2008, 23, 157–204. [Google Scholar] [CrossRef] [Green Version]
- Briggs, D. Environmental pollution and the global burden of disease. Br. Med. Bull. 2003, 68, 1–24. [Google Scholar] [CrossRef]
- Lahelma, E. Health inequalities—The need for explanation and intervention. Eur. J. Public Health 2006, 16, 339. [Google Scholar] [CrossRef]
- Diderichsen, F. Resource Allocation for Health Equity: Issues and Methods; World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Mushkin, S.J. Health as an Investment. J. Political Econ. 1962, 70 Pt 2, 129–157. [Google Scholar] [CrossRef]
- Grossman, M. The Human Capital Model. In Handbook of Health Economics; Culyer, A.J., Newhouse, J.P., Eds.; Elsevier: New York, NY, USA, 2000; Volume 1A. [Google Scholar]
- Lechtenböhmer, S.; Barthel, C.; Merten, F.; Schneider, C.; Schüwer, D.; Seifried, D. Redesigning urban infrastructures for a low-emission future. An overview of urban low-carbon technologies. SAPI EN. S. Surv. Perspect. Integr. Environ. Soc. 2010, 3, 1–16. Available online: https://journals.openedition.org/sapiens/1042 (accessed on 12 May 2022).
- Rabe, M. Energetyka Rozproszona w Polityce Regionalnej; CeDeWu: Warszawa, Poland, 2021. [Google Scholar]
- Williams, A. Calculating the global burden of disease: Time for a strategic reappraisal? Health Econ. 1999, 8, 1–8. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D. Measuring the global burden of disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EU Member States | Groups of EU | Ambient Particulate Matter Pollution | Household Air Pollution from Solid Fuels | ||||||
|---|---|---|---|---|---|---|---|---|---|
| YLL Rate (2019) | Percentage Change 1990–2019 | Rankings | YLL Rate (2019) | Percentage Change 1990–2019 | Rankings | ||||
| 2019 | 1990 | 2019 | 1990 | ||||||
| Bulgaria | EU-CEE | 904.0 | −27.5% | 1 | 2 | 163.35 | −62.1% | 1 | 3 |
| Romania | EU-CEE | 501.8 | −31.6% | 2 | 8 | 75.48 | −84.7% | 3 | 1 |
| Hungary | EU-CEE | 444.8 | −64.7% | 3 | 1 | 78.98 | −83.8% | 2 | 2 |
| Poland | EU-CEE | 388.0 | −66.9% | 4 | 3 | 35.52 | −90.7% | 4 | 4 |
| Slovakia | EU-CEE | 337.8 | −67.6% | 5 | 4 | 3.00 | −91.2% | 10 | 11 |
| Croatia | EU-CEE | 313.2 | −61.1% | 6 | 7 | 15.37 | −89.5% | 6 | 7 |
| Greece | EU-14 | 310.0 | −28.1% | 7 | 12 | 2.02 | −88.6% | 12 | 14 |
| Latvia | EU-CEE | 295.7 | −69.5% | 8 | 6 | 23.84 | −86.6% | 5 | 6 |
| Lithuania | EU-CEE | 253.0 | −63.9% | 9 | 9 | 10.69 | −90.9% | 9 | 8 |
| Czechia | EU-CEE | 220.5 | −77.7% | 10 | 5 | 2.57 | −91.8% | 11 | 12 |
| Cyprus | - | 177.6 | −50.3% | 11 | 20 | 0.32 | −96.2% | 18 | 15 |
| Slovenia | EU-CEE | 165.9 | −69.9% | 12 | 10 | 11.39 | −88.9% | 8 | 9 |
| Italy | EU-14 | 145.7 | −63.0% | 13 | 16 | 0.68 | −90.9% | 15 | 16 |
| Malta | - | 132.5 | −55.1% | 14 | 21 | 0.33 | −94.9% | 17 | 17 |
| Germany | EU-14 | 131.9 | −72.6% | 15 | 11 | 0.13 | −84.7% | 25 | 27 |
| Belgium | EU-14 | 125.3 | −69.5% | 16 | 14 | 0.20 | −92.0% | 20 | 21 |
| France | EU-14 | 115.7 | −56.4% | 17 | 22 | 0.30 | −86.7% | 19 | 22 |
| Netherlands | EU-14 | 112.3 | −69.4% | 18 | 18 | 0.13 | −92.1% | 24 | 24 |
| Austria | EU-14 | 109.3 | −71.1% | 19 | 17 | 0.37 | −89.0% | 16 | 20 |
| Spain | EU-14 | 94.7 | −60.7% | 20 | 25 | 1.75 | −93.2% | 13 | 13 |
| Portugal | EU-14 | 81.6 | −67.1% | 21 | 24 | 1.20 | −96.6% | 14 | 10 |
| Denmark | EU-14 | 80.8 | −80.0% | 22 | 15 | 0.12 | −91.7% | 26 | 25 |
| Luxembourg | EU-14 | 79.1 | −78.3% | 23 | 19 | 0.17 | −91.6% | 22 | 23 |
| Estonia | EU-CEE | 53.8 | −87.3% | 24 | 13 | 11.85 | −95.0% | 7 | 5 |
| Ireland | EU-14 | 52.6 | −79.9% | 25 | 23 | 0.18 | −95.6% | 21 | 18 |
| Finland | EU-14 | 25.1 | −87.9% | 26 | 26 | 0.14 | −96.0% | 23 | 19 |
| Sweden | EU-14 | 19.1 | −86.0% | 27 | 27 | 0.07 | −94.9% | 27 | 26 |
| Selected statistics | |||||||||
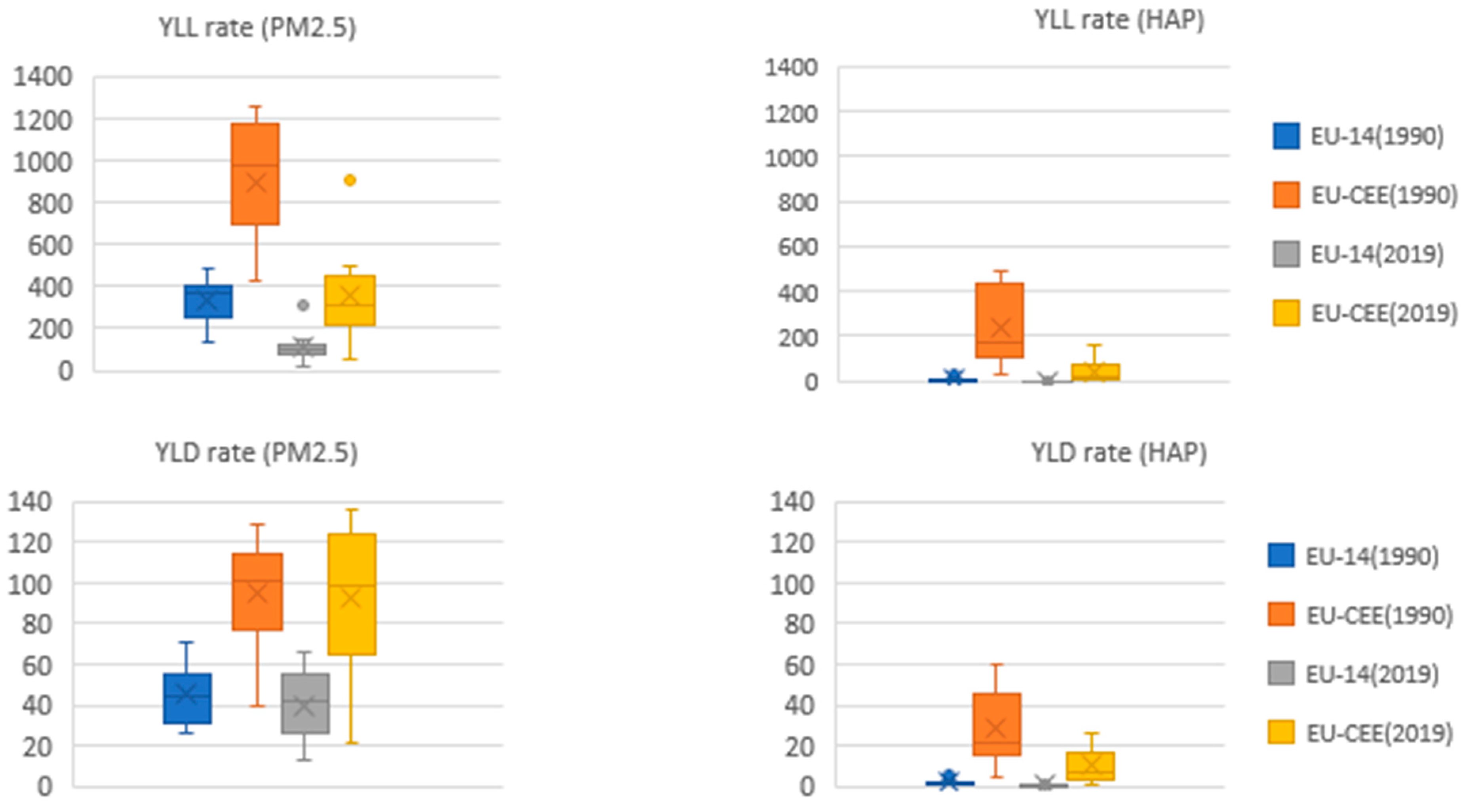
| Average | EU-27 | 210.1 | −65.3% | 16.30 | −90.0% | ||||
| Interval | 884.8 | 163.28 | |||||||
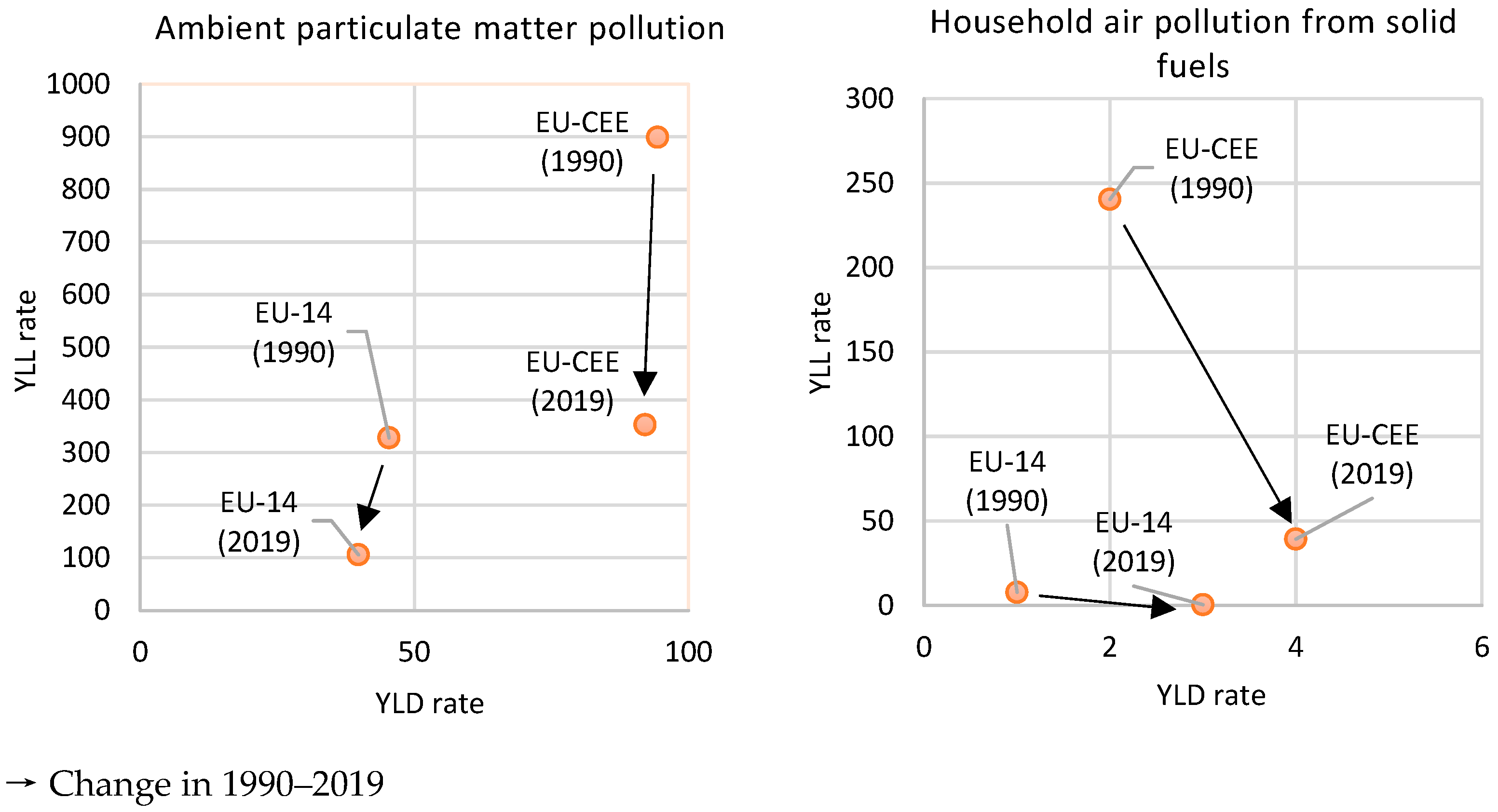
| Average | EU-14 | 105.9341 | −69.3% | 0.53 | −91.7% | ||||
| Interval | 290.9 | 1.94 | |||||||
| Average | EU-CEE | 352.6 | −62.5% | 39.8 | −86.8% | ||||
| Interval | 850.2 | 151.5 | |||||||
| EU Member States | Groups of EU | Ambient Particulate Matter pollution | Household Air Pollution from Solid Fuels | ||||||
|---|---|---|---|---|---|---|---|---|---|
| YLD Rate (2019) | Percentage Change 1990–2019 | Rankings | YLD Rate (2019) | Percentage Change 1990–2019 | Rankings | ||||
| 2019 | 1990 | 2019 | 1990 | ||||||
| Czechia | EU-CEE | 135.6 | 5.7% | 1 | 1 | 1.87 | −61.7% | 10 | 12 |
| Bulgaria | EU-CEE | 126.7 | 11.0% | 2 | 3 | 26.15 | −42.0% | 1 | 3 |
| Poland | EU-CEE | 123.8 | 10.7% | 3 | 4 | 13.76 | −68.3% | 4 | 4 |
| Hungary | EU-CEE | 112.2 | −6.8% | 4 | 2 | 23.65 | −57.0% | 2 | 2 |
| Croatia | EU-CEE | 106.0 | 4.6% | 5 | 6 | 6.25 | −71.2% | 7 | 6 |
| Slovakia | EU-CEE | 98.1 | −5.1% | 6 | 5 | 1.08 | −73.3% | 12 | 13 |
| Romania | EU-CEE | 90.6 | 17.1% | 7 | 9 | 16.08 | −73.0% | 3 | 1 |
| Slovenia | EU-CEE | 86.2 | −2.9% | 8 | 7 | 7.32 | −62.9% | 5 | 7 |
| Greece | EU-14 | 66.5 | 21.1% | 9 | 14 | 0.56 | −80.5% | 14 | 14 |
| Latvia | EU-CEE | 64.4 | −22.0% | 10 | 8 | 6.85 | −63.9% | 6 | 8 |
| Italy | EU-14 | 64.2 | −3.8% | 11 | 12 | 0.50 | −76.7% | 15 | 15 |
| Germany | EU-14 | 60.0 | −16.0% | 12 | 10 | 0.08 | −53.2% | 24 | 27 |
| Belgium | EU-14 | 53.5 | −6.7% | 13 | 13 | 0.11 | −75.2% | 22 | 21 |
| Malta | - | 53.1 | 3.6% | 14 | 17 | 0.18 | −87.3% | 17 | 16 |
| Cyprus | - | 51.6 | 25.1% | 15 | 19 | 0.13 | −89.3% | 18 | 17 |
| Lithuania | EU-CEE | 49.1 | −30.7% | 16 | 11 | 2.89 | −80.8% | 9 | 9 |
| Netherlands | EU-14 | 45.0 | −14.9% | 17 | 15 | 0.07 | −78.4% | 27 | 25 |
| Austria | EU-14 | 43.6 | −15.4% | 18 | 16 | 0.21 | −66.6% | 16 | 18 |
| Spain | EU-14 | 42.4 | 10.7% | 19 | 22 | 1.20 | −78.8% | 11 | 11 |
| Luxembourg | EU-14 | 41.1 | 1.0% | 20 | 20 | 0.12 | −62.6% | 19 | 24 |
| Portugal | EU-14 | 33.5 | −10.8% | 21 | 23 | 0.63 | −89.9% | 13 | 10 |
| Denmark | EU-14 | 31.6 | −34.1% | 22 | 18 | 0.07 | −71.1% | 26 | 26 |
| France | EU-14 | 26.9 | −16.1% | 23 | 24 | 0.10 | −73.7% | 23 | 23 |
| Ireland | EU-14 | 22.3 | −22.0% | 24 | 26 | 0.11 | −80.9% | 21 | 20 |
| Estonia | EU-CEE | 20.9 | −47.6% | 25 | 21 | 5.98 | −78.1% | 8 | 5 |
| Finland | EU-14 | 14.3 | −46.0% | 26 | 27 | 0.12 | −80.1% | 20 | 19 |
| Sweden | EU-14 | 12.7 | −56.1% | 27 | 25 | 0.07 | −81.6% | 25 | 22 |
| Selected statistics | |||||||||
| Average | EU-27 | 62.1 | −9.1% | 4.30 | −72.5% | ||||
| Interval | 122.9 | 26.09 | |||||||
| Average | EU-14 | 39.8 | −14.9% | 0.28 | −75.0% | ||||
| Interval | 53.8 | 7.24 | |||||||
| Average | EU-CEE | 92.1 | −6.0% | 10.17 | −66.6% | ||||
| Interval | 114.7 | 14.2 | |||||||
| Parameters | Mean EU-14 | Mean EU-CEE | t-Test | Welch’s Test | Brown—Forsy the Test | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| t | df | p | t | df | p | Brn-Fors F(1.df) | df Brn-Fors | p Brn-Fors | |||
| YLDrate (PM 2.5) 1990 | 45.3772 | 94.4288 | −6.04802 | 23 | 0.000004 | −5.66218 | 14.82036 | 0.000047 | 2.44880 | 23 | 0.131271 |
| YLDrate (PM 2.5) 2019 | 39.8254 | 92.1480 | −4.86778 | 23 | 0.000065 | −4.50801 | 13.78429 | 0.000510 | 3.70073 | 23 | 0.066852 |
| Parameters | Mann–Whitney U Test | ||||||
|---|---|---|---|---|---|---|---|
| Sum.Rang EU-14 | Sum.Rang EU-CEE | U | Z | p | Z Correc. | p | |
| YLLrate (PM 2.5) 1990 | 107.0000 | 218.0000 | 2.00000 | −4.07849 | 0.000045 | −4.07849 | 0.000045 |
| YLLrate (PM 2.5) 2019 | 120.0000 | 205.0000 | 15.00000 | −3.36681 | 0.000761 | −3.36681 | 0.000761 |
| YLLrate (HAP) 1990 | 107.0000 | 218.0000 | 2.00000 | −4.07849 | 0.000045 | −4.07849 | 0.000045 |
| YLLrate (HAP) 2019 | 105.0000 | 220.0000 | 0.00000 | −4.18798 | 0.000028 | −4.18798 | 0.000028 |
| YLDrate (HAP) 1990 | 109.0000 | 216.0000 | 4.00000 | −3.96900 | 0.000072 | −3.96900 | 0.000072 |
| YLDrate (HAP) 2019 | 106.0000 | 219.0000 | 1.00000 | −4.13324 | 0.000036 | −4.13324 | 0.000036 |
| 1990 | 2019 | 1990 | 2019 | |
|---|---|---|---|---|
| PM 2.5 | HAP | |||
| OR (YLD rate) | 2.1 | 2.3 | 19.1 | 34.0 |
| OR (YLL rate) | 2.8 | 3.3 | 30.9 | 78.6 |
| 1990 | 2019 | 1990 | 2019 | |
|---|---|---|---|---|
| PM 2.5 | HAP | |||
| CV (YLD rate) | 46.5% | 56.7% | 142.2% | 152.6% |
| CV (YLL rate) | 59.9% | 88.7% | 153.6% | 217.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakubowska, A.; Rabe, M. Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU. Energies 2022, 15, 6225. https://doi.org/10.3390/en15176225
Jakubowska A, Rabe M. Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU. Energies. 2022; 15(17):6225. https://doi.org/10.3390/en15176225
Chicago/Turabian StyleJakubowska, Agnieszka, and Marcin Rabe. 2022. "Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU" Energies 15, no. 17: 6225. https://doi.org/10.3390/en15176225
APA StyleJakubowska, A., & Rabe, M. (2022). Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU. Energies, 15(17), 6225. https://doi.org/10.3390/en15176225