
Assessment of Human Exposure (Including Interference to Implantable Devices) to Low-Frequency Electromagnetic Field in Modern Microgrids, Power Systems and Electric Transports


Abstract
:1. Introduction
- Body current flow possibly interfering with the nervous system and other endogenous systems (such as retina, heart, etc.);
- Heating at a higher frequency due to dielectric losses and molecule movement;
- Mechanical forces on metallic implants in case of large field intensities;
- In general interference to implanted devices.
2. Principles of Interaction and Interference Coupling
2.1. Interaction of Electromagnetic Field with Subject’s Body
- The physical characteristics of the body models representing persons with different circumference and males/females (male results on average with 25% larger current density results); considering the specific publications and the reported results, also the use of, for example, European (Norman and Naomi) and Japanese (Taro and Hanako) body models has an influence, with 52 different tissues for the latter compared to about 38–41 for the former, and with the classification of white and grey matter only in the Japanese models [52].
- The methods to process the model voxels values, depending on the reference guideline/standard: ICNIRP requires calculations on 2 × 2 × 2 mm3 elements taking the 99th percentile value and IEEE the maximum of 5-mm long filaments to compare to the BR or DRL, respectively [47]. When operating spatial averaging over larger volumes and surfaces, such as with 1 cm2 for the calculation of the current density Ji, the collection of adjacent mesh cells for an equivalent 1-cm2 area may include or not non-nerve tissues and this causes a large variation in the order of 5 to 12, leading to larger, but more stable, values when non-nerve tissues are excluded [52].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Body Areas and Conditions | Internal E-Field Ei | Internal Current Density Ji | ||
|---|---|---|---|---|---|
| B-Field [mV/m/mT] | E-Field [mV/m/(kV/m)] | B-Field [(mA/m2)/mT] | E-Field [(mA/m2)/(kV/m)] | ||
| ICNIRP 2010 [3] | Brain | 23–33 | 1.7–2.6 | — | — |
| ICNIRP 2010 [3] | Skin | 20–60 | 12–33 | — | — |
| Hirata 2009 [52] | Taro, Cerebro- Spinal Fluid | — | — | 74.8–81.5 | — |
| Hirata 2009 [52] | Taro, Skin | 312 | — | — | — |
| Hirata 2009 [52] | Taro, spinal cord /grey matter | 27.7–89.1 | — | 2.26–22.4 | — |
| Hirata 2009 [52] | Hanako, Cerebro- Spinal Fluid | — | — | 50.3–57.4 | — |
| Hirata 2009 [52] | Hanako, Skin | 97.7 | — | — | — |
| Hirata 2009 [52] | Hanako, spinal cord/grey matter | 25.9–65.1 | — | 2.25–16.7 | — |
| Hirata 2009 [52] | Norman, grey matter | 30.7–48.6 | — | 3.32–3.56 | — |
| Hirata 2009 [52] | Naomi, grey matter | 25.7–31.4 | — | 2.81–2.98 | — |
| Dimbylow 2000 [56] | Brain | — | — | — | 0.176 |
| Dimbylow 2000 [56] | Muscle | — | — | — | 0.832 |
| Dimbylow 2007 [57] | Naomi, pregnant foetal body (13–38 w) | 9.11–21.4 | 1.12–1.56 | 3.78–7.34 | 0.29–0.47 |
| Dimbylow 2007 [57] | Naomi, pregnant foetal brain (13–38 w) | 5.52–24.7 | 0.67–1.62 | 0.77–3.37 | 0.11–0.19 |
2.1.1. Static Fields
- Magnetic induction:
- Lorentz forces on mobile ionic charges, as for flowing blood, thus causing current flow and internal electric field build-up; in [5] for an external magnetic induction field of 5 T an induced current density of 100 mA/m2 is estimated, that corresponds to the 10% of the maximum endogenous current from cardiac electrical activity;
- By virtue of Faraday’s law an external time-varying field, as well as movement within a static magnetic field, can both induce an electromotive force; the magnitude of induction is proportional to the velocity of the movement and amplitude of the gradient. At a 3 T intensity, there are several reported episodes of nausea and phosphenes for patients and workers around magnetic resonance machines. A calculation for a 0.5 m/s speed of movement and a field intensity of 4 T gives the Ei lower bound of 2 V/m for peripheral nerve stimulation, which we saw is at the threshold for phosphenes generation.
- Magneto-mechanical effects:
- Besides the orientation of paramagnetic molecules (that is not considered to affect biological material remarkably), magnetic field gradient can exert a translational force on paramagnetic and diamagnetic materials, the difference being in the force sign. What matters is the product of the field intensity B and its gradient dB/dx, for which a reduction of blood flow in rats was observed for a combination of B = 8 T and product B × dB/dx = 200–400 T2/m (i.e., a gradient of 0.25–0.5 T/cm).
2.1.2. Field at Power Frequency, Harmonics and Supraharmonics
- The former decision of dividing low- and high-frequency intervals at 100 kHz was a matter of convenience.
- The relevant emissions characterizing modern power systems and connected equipment are spread over a significant frequency interval. As an example, the emissions of large power converters on-board a DC electro-train of 25 years ago in [25] were observed up to about 100 kHz, and high-frequency spectrum pollution is expected to increase with faster technology; for electric vehicles emissions E- and H-field levels extend at the largest values up to the main resonance frequency in the order of 1 MHz [60]. It was similar for large power drives [61].
- Conducted emissions are regulated by EMC standards using the 150 kHz boundary, that separates the so-called supraharmonics from the radiofrequency conducted emissions; by experience, conducted emissions of large power converters are significant up to some MHz at most, also as a consequence of internal cabling resonance [60], that turns out to be a significant element that affects the intensity of emissions in the medium frequency range.
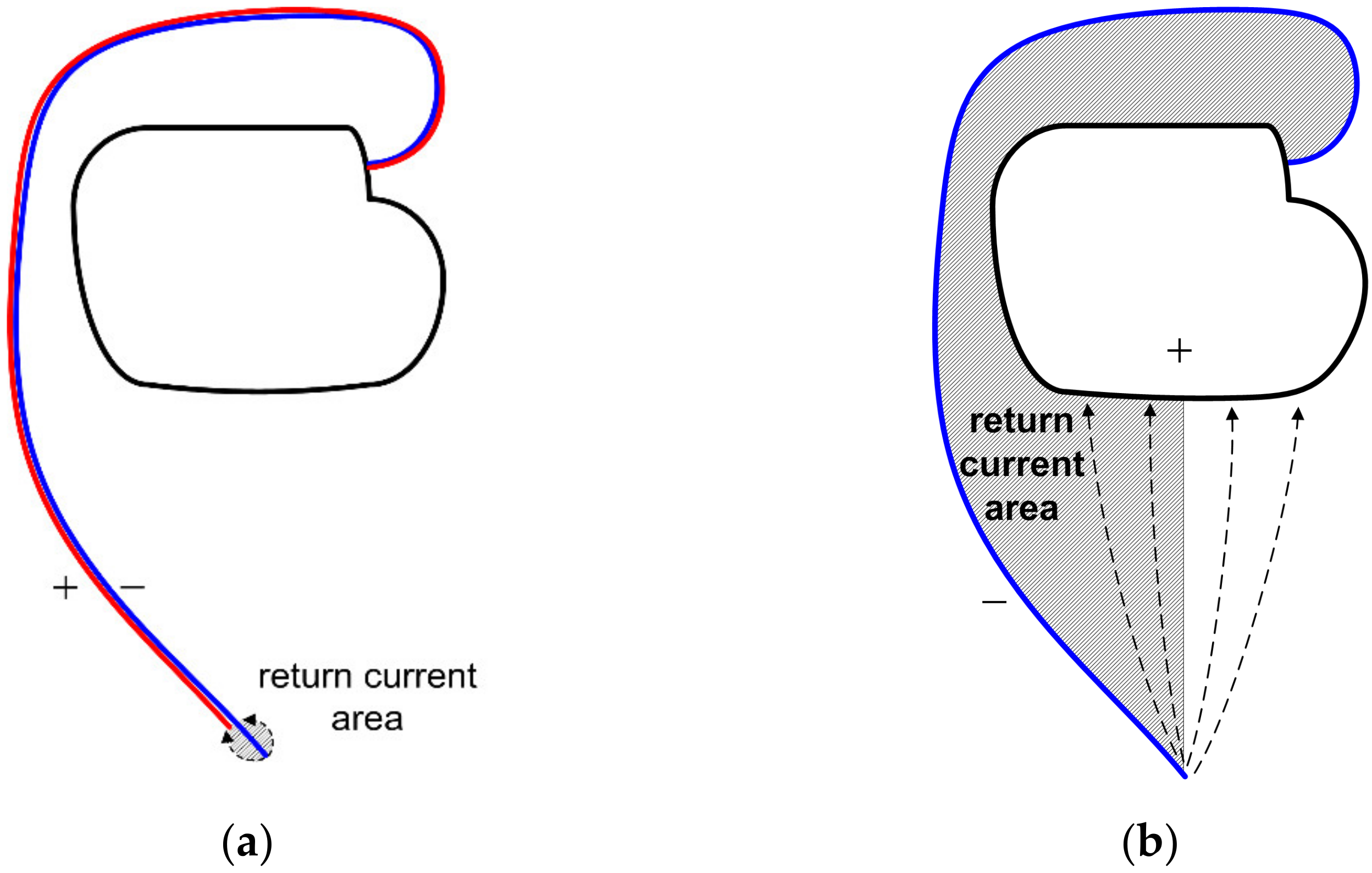
2.2. Interference to Pacemakers and Other Implantable Devices
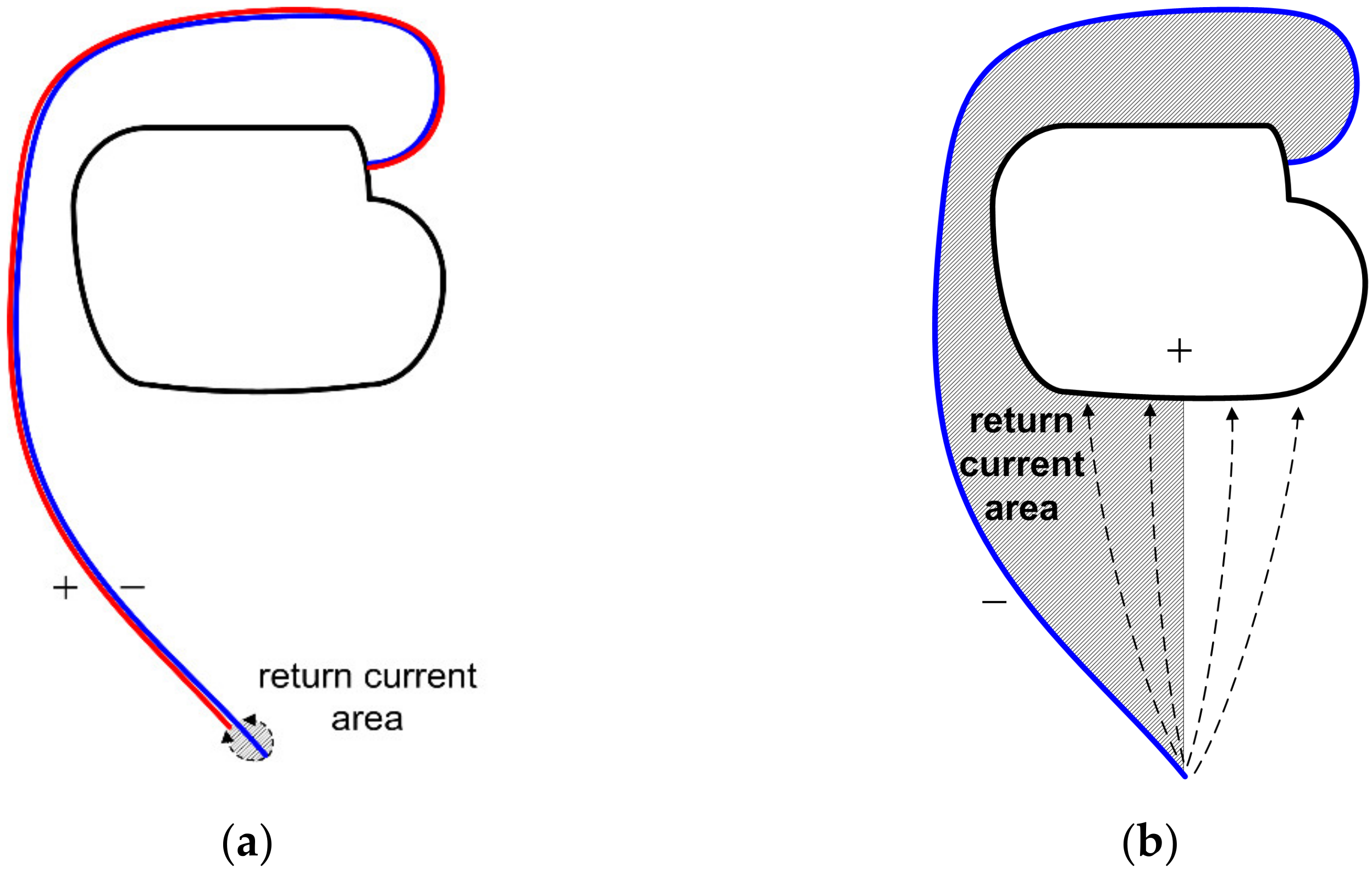
- Tip-to-ring distance taken at the worst-case 20 mm of a typical range of 8 to 20 mm;
- Lead length of 50 cm in a semicircular fashion giving a total area of about 315 cm2 considering actual implantation situations, giving an effective area for induction of 225 cm2; these values are very similar to those in the ISO 14117 [70], where a survey of X-ray images of real implantations is reported;
- With the 20 mm tip-to-ring separation, the area of the equivalent circular sector is 24 cm2 (that is probably slightly overestimated), leading to a proportion between the exposed area of the bipolar case compared to the unipolar case of 11%, confirming the aforementioned order of magnitude of reduction of induction.
2.3. Interference to Hearing Aids
- Audiofrequency induction loop systems (AFILSs);
- Modulation radio transmission systems, including digital radio solutions;
- Systems based on infra-red (IR) technology.
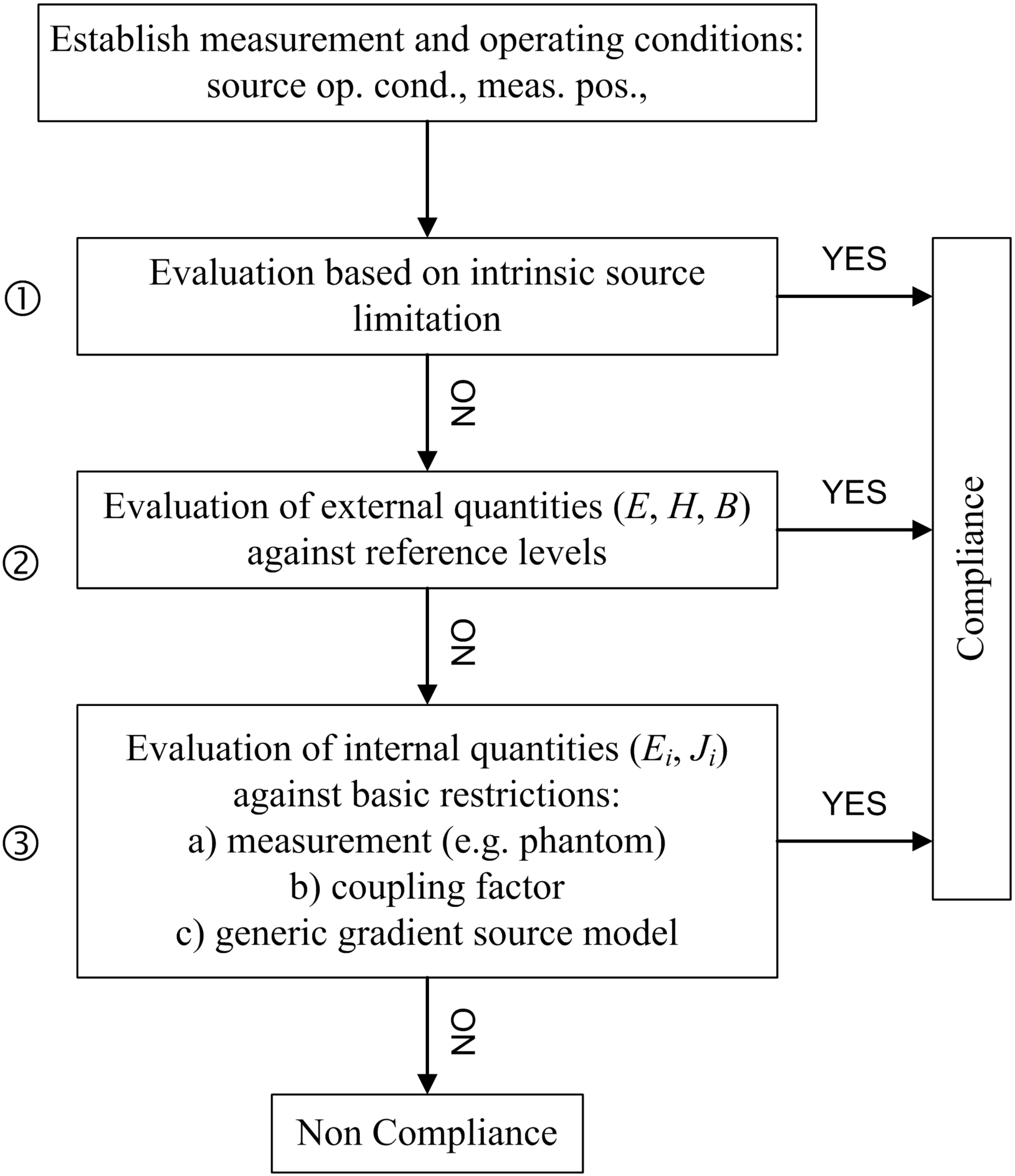
3. Compliance Requirements, Limits, and Frequency Ranges
3.1. Human Exposure
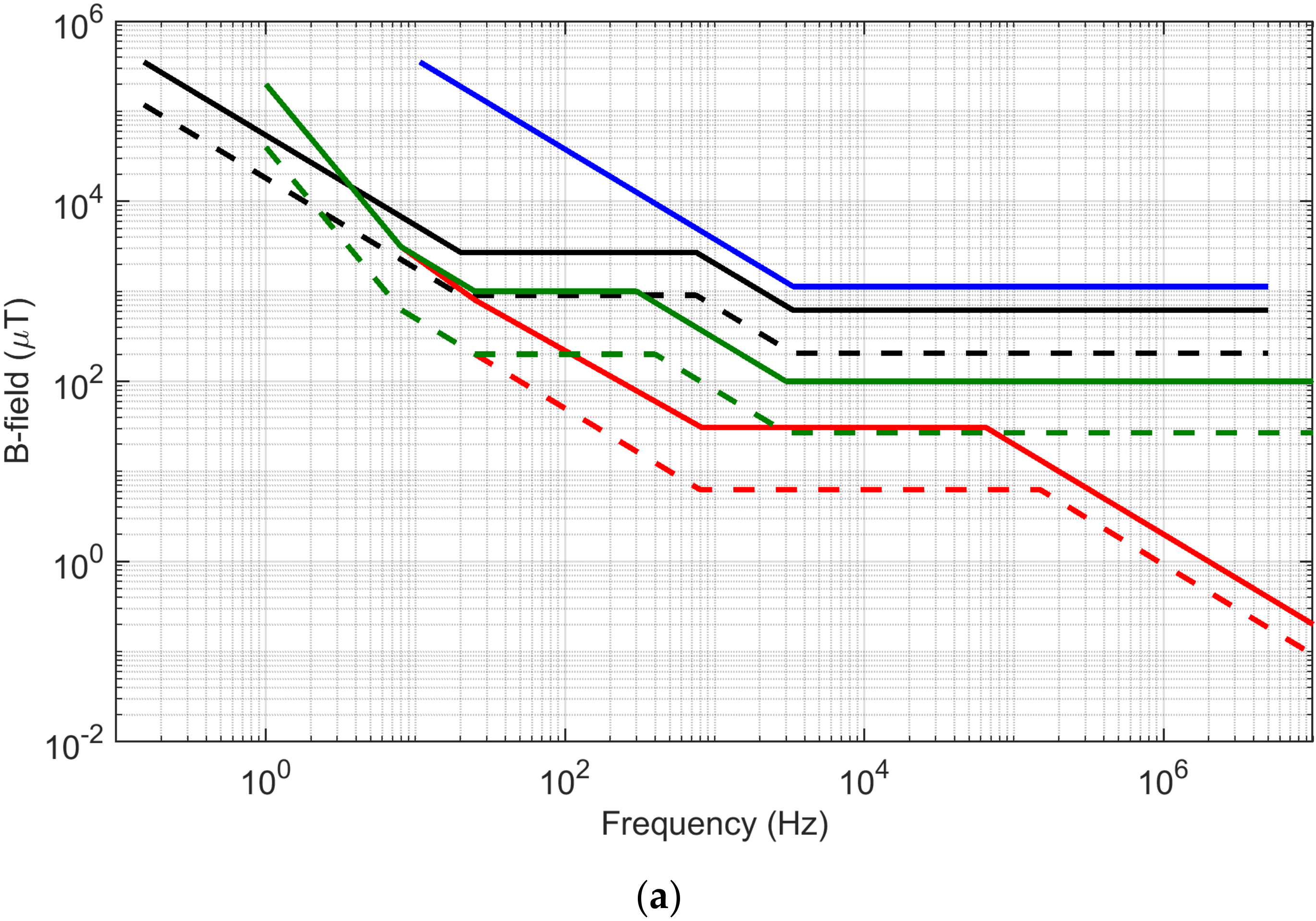
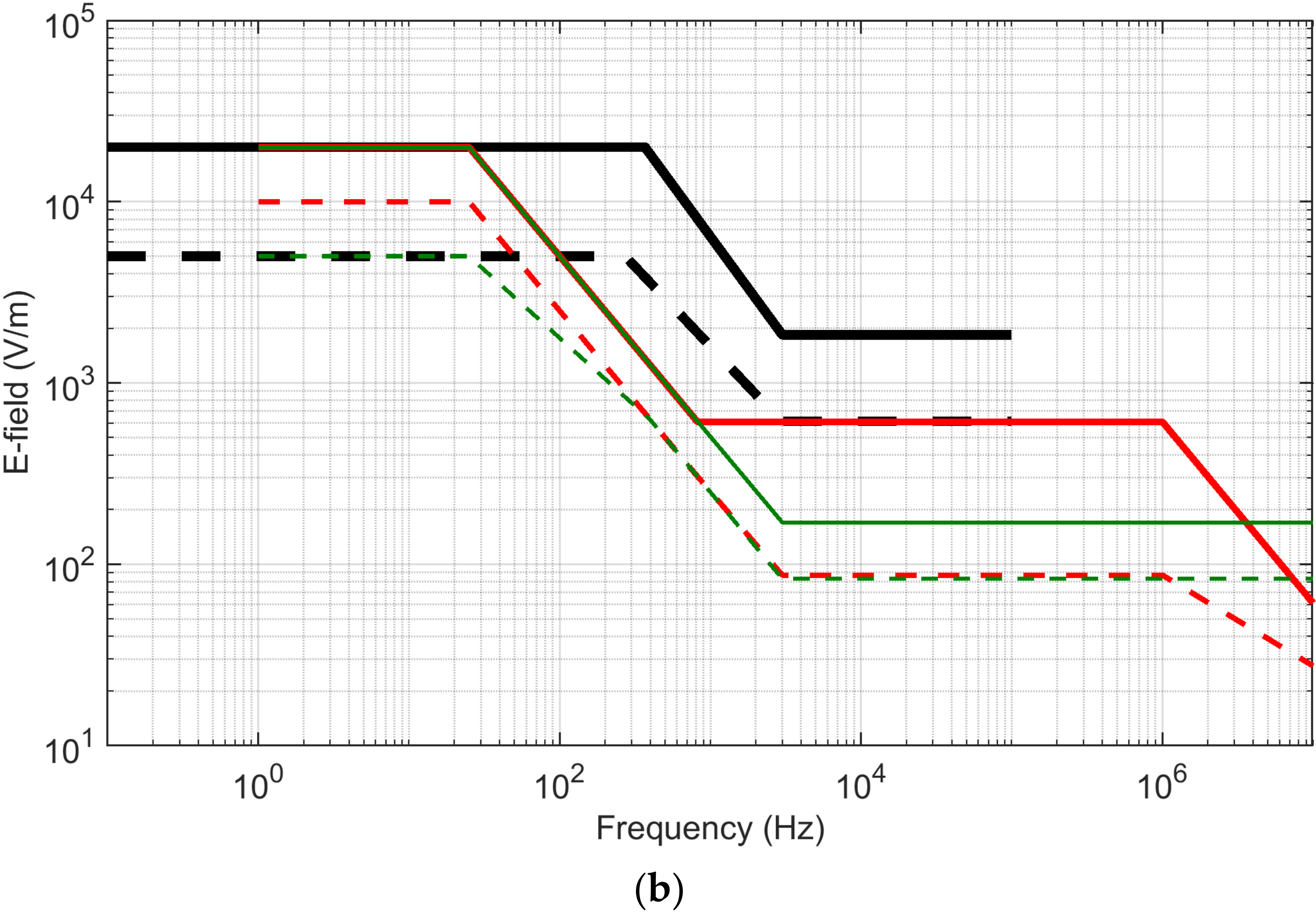
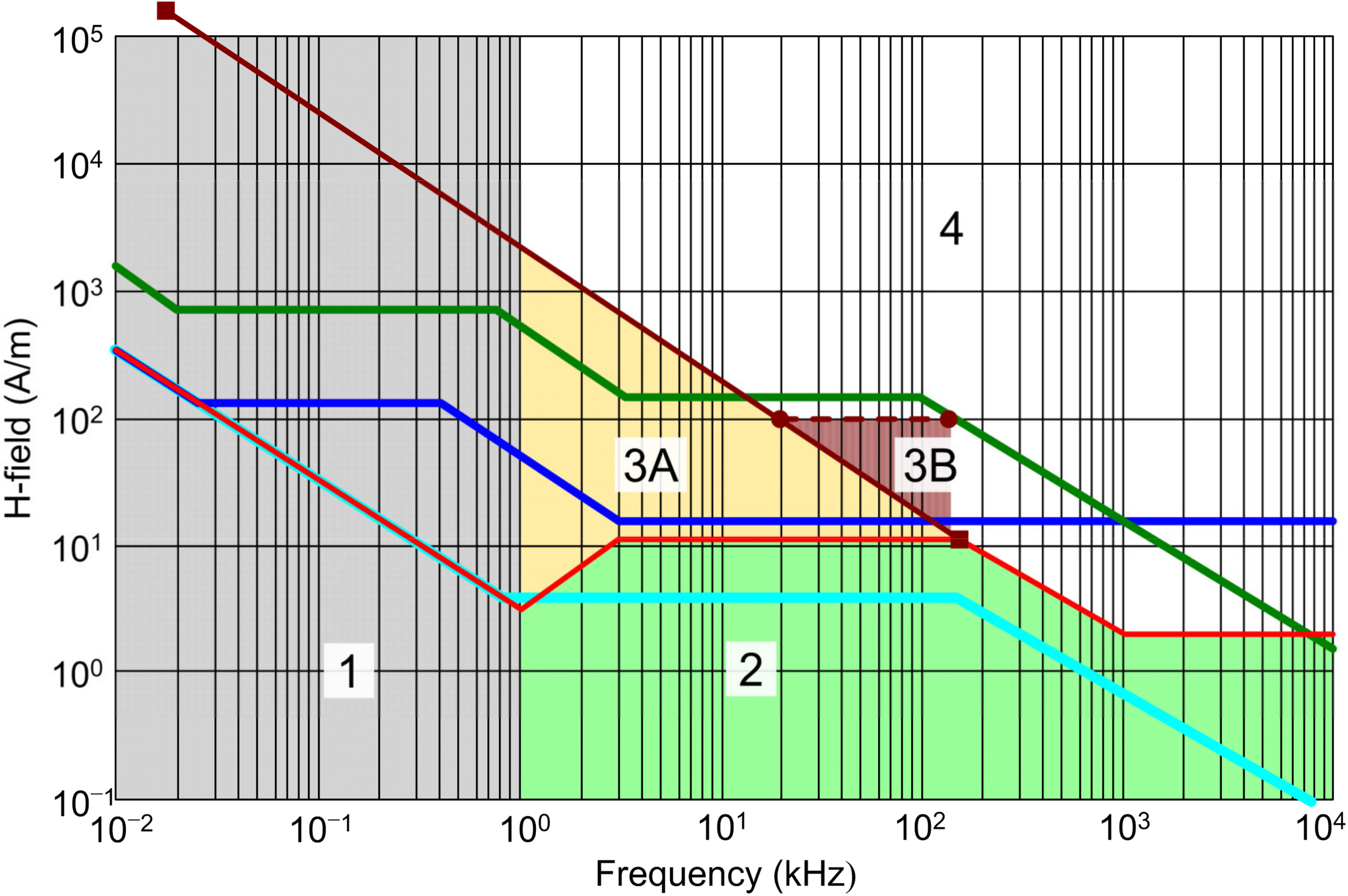
- Comparing the occupational and general public levels of the ICNIRP 1998 and 2010, the B-field RL has increased at high frequency by a factor of 3 and 4, respectively; conversely, for the E-field, the high-frequency values for occupational exposure only has seen a significant increase by about 3.5 times.
- IEEE includes de facto also a limit for the static field, whereas ICNIRP keeps it separate in a different guideline [5].
- IEEE does not report limits for whole-body exposure to the magnetic field (distinguishing three body parts, head, torso, and limbs), but does for the electric field. B-field exposure limits for occupational exposure have a margin of about 2 between head/torso (lower limits) and limbs (higher limits). Conversely, for general public exposure, the higher-margin is obtained by reducing the limits of exposure for head and torso, to less than 50% of the corresponding occupational values, but curiously the exposure limits for limbs are the same of the occupational scenarios.
- The IEEE RL values compared to ICNIRP are in general significantly higher, except for the low-frequency E-field where the two correspond.
3.1.1. Field Non-Uniformity, Field Gradient and Space Distribution of Points
Spatial Averaging and Local Exposure
Coupling Factor
- A series of measurements of the B-field with a small volume probe (3 cm2) are taken at small steps (e.g., 0.5 to 1 cm) until the measured B-field drops to 10% of the initial maximum value at a given distance r10 (taken after having identified that position as a hot spot).
- The integral over the distance of the measured B values up to r10 is taken and an equivalent coil with the same integral value is determined; pre-calculated values for various coil radii and distances are shown in Table C.1 of the IEC 62233;
- The factor kc is then determined by complex modeling that takes into account body conductivity σb, besides the coil geometrical factors; pre-calculated values for 50 Hz and σb = 0.1 S/m are reported in Table C.2 of the IEC 62233 and they can be extrapolated to other scenarios linearly in frequency (f/(50 Hz)) and conductivity (σb/(0.1 S/m)).
- For each frequency, the coupling factor ac is determined as the scaled version of kc, namely multiplying it by Blim/Ji,lim (i.e., RL/BR). The value of ac is plotted in Figure C.5 of the IEC 62233 for a coil radius ranging between 10 and 100 mm and the resulting value is quite stable and insensitive to coil radius, provided that the distance is larger than the said maximum coil radius, namely 100 mm.
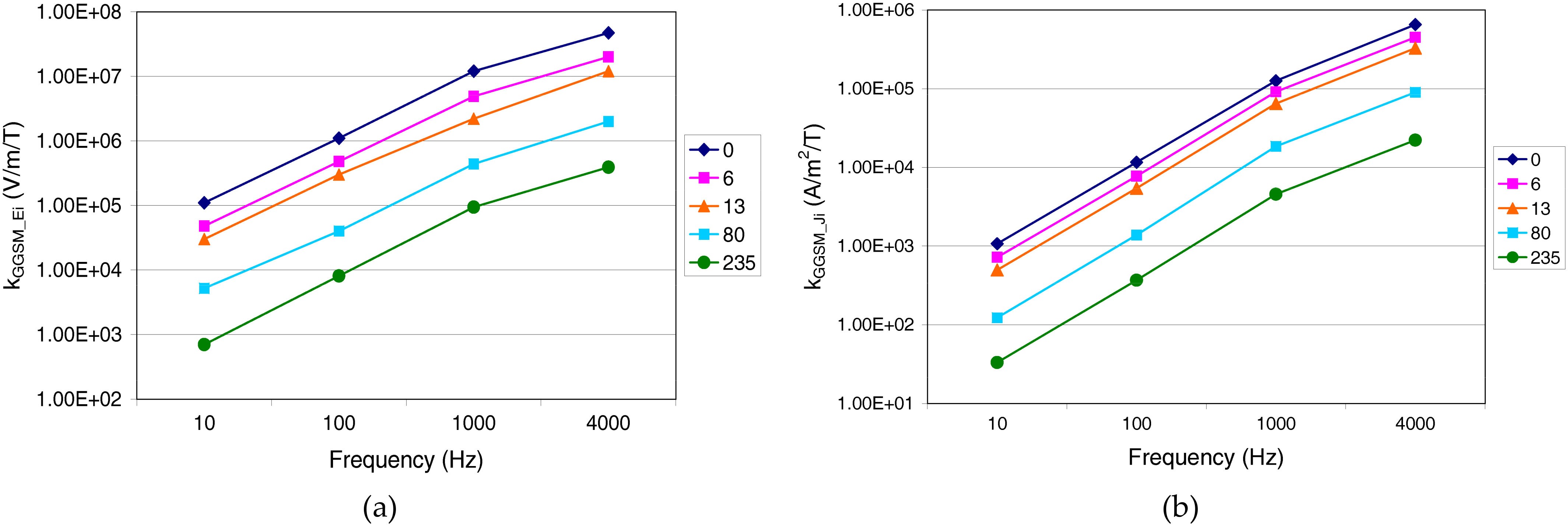
Generic Gradient Source Model (GGSM)
3.1.2. Multiple Spectrum Components at Different Frequencies
3.1.3. Non-Sinusoidal Field Waveforms
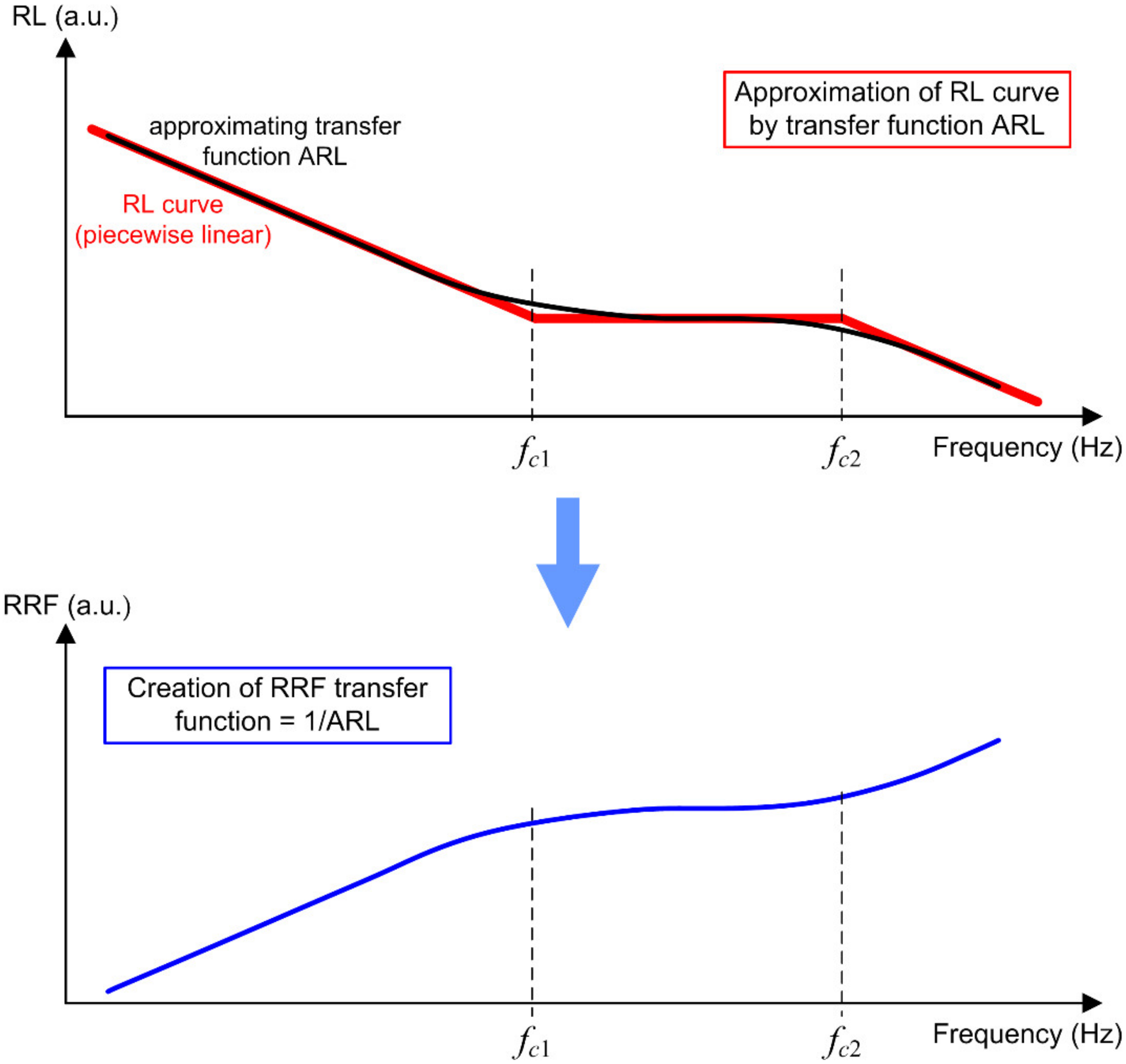
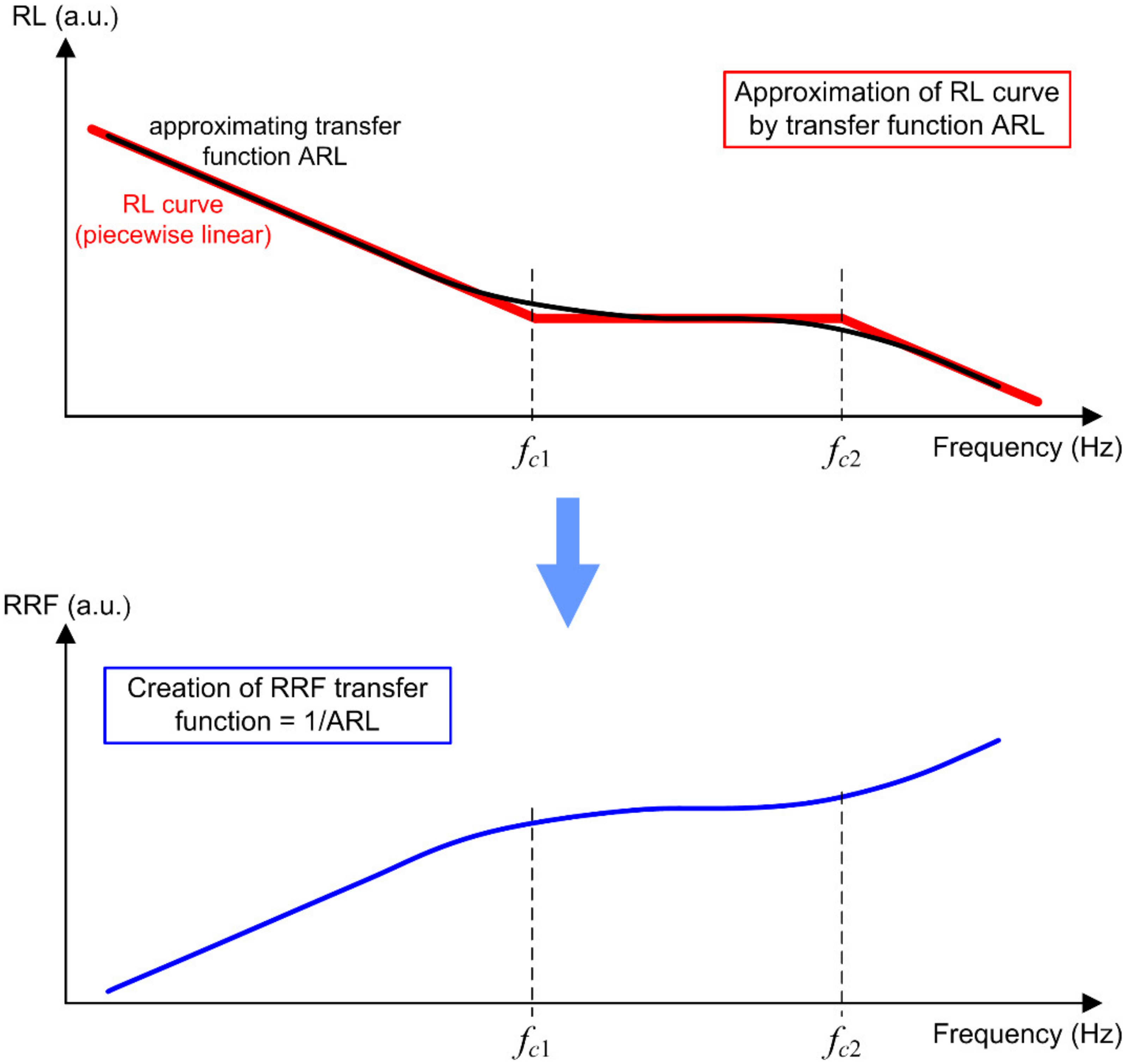
- Smoothing of corners, common also to analog implementations, for which there is an unavoidable loss of accuracy that can be evaluated as sketched in Figure 5;
- Phase response, that should not alter the phase relationship of the signal components; a zero-phase shift digital filter can always be implemented by exploiting the phase shift compensation occurring of the signal is passed through the filter twice, in the two time directions [85];
- Filter performance with respect to the adopted sampling frequency, compared to that of the original data samples: the RRF implementation in [25] revealed that to control filter response accuracy, the signal must be upsampled by about an order of magnitude, yet increasing correspondingly the computational burden.
3.1.4. Transients, Time Variability, and Time Averaging
- Changes to the spectrum of emissions (as in the case of a power drive or static power converter, exemplified for a French train in Figure 4 of the IEC 61786-2 and characterized in [89] for AC and DC rolling stock), or
- Transient waveforms, as caused by load steps, inrush, switch on/off and short circuits; it is generally agreed that major transients of this type should be discarded [82], but no criteria are given for example for repeated inrush events and switch on/off of loads.
3.1.5. Additivity of Exposure to Electric and Magnetic Fields
- A typical high-voltage OHL provides both electric and magnetic field, in the order of some kV/m and several tens of μT at ground level beneath the line, and considering “ICNIRP 2010” in Table 2 results in alike contributions of internal electric field Ei in the brain of 3–5 and 1–2 mV/m, respectively; considering instead the fetal body labeled as “Dimbylow 2007”, the resulting values are about 2–4 and 0.5–1 mV/m; the contributions are clearly located in the same body region, the brain, and are commensurable, and should be summed together;
- For a different source that is prevalently magnetic (such as an MV/LV power transformer) at about 5–10 μT with a marginal electric field of some hundreds V/m, the previous contributions become 0.3–0.5 and 1–2 mV/m and 0.2–0.4 and 0.5–1 mV/m, resulting again in two alike terms, this time with prevalence of magnetic field induction, again in the same body region.
3.2. Interference to Implantable Devices
3.2.1. Pacemakers (PMs), Implantable Cardioverter Defibrillators (ICDs,) and Cardiac Resynchronization Therapy Devices (CRTs)
- (T1.1) protection from the mis-reception of cardiac signals due to EMI, guaranteeing that the pacemaker provides its signals unaltered: square-wave modulated test signal (100 ms on, 600 ms off) with three quite extended frequency ranges (16.6 Hz to 150 kHz, 150 kHz to 10 MHz and 10 MHz to 450 MHz) and correspondingly amplitude ranging between 2–900 mVpp, 0.9–10 Vpp, and 10 Vpp for the three frequency ranges); above 150 kHz the signal is amplitude modulated with a modulation depth of 95% at alternating intervals of 100 ms on, 600 ms off.
- (T1.2) extension of protection from mis-reception for the frequency interval 450–3000 MHz either by verification of the presence of feed-through filter for all leads going through the enclosure with a minimum insertion loss of 30 dB or by applying a test in line with the AAMI PC69 standard.
- (T1.3) protection from persisting malfunction with a test signal consisting of a swept sinusoid between 16.6 Hz and 140 kHz of 1 Vpp amplitude, increased proportionally to a frequency above 20 kHz (so that at 140 kHz it is 7 Vpp); when considering malfunction the tests signal is not square-wave modulated.
- (T1.4) protection from temporary malfunction during tests with a signal consisting of a sinusoid with frequency stepped between 16.6 Hz and 167 kHz and slowly increasing its amplitude from 0 to 1 Vpp at each frequency point.
- (T2.1) a total immunity to a static field of 1 mT (criterion A) and protection from malfunction after application of a 10 mT intensity (criterion B).
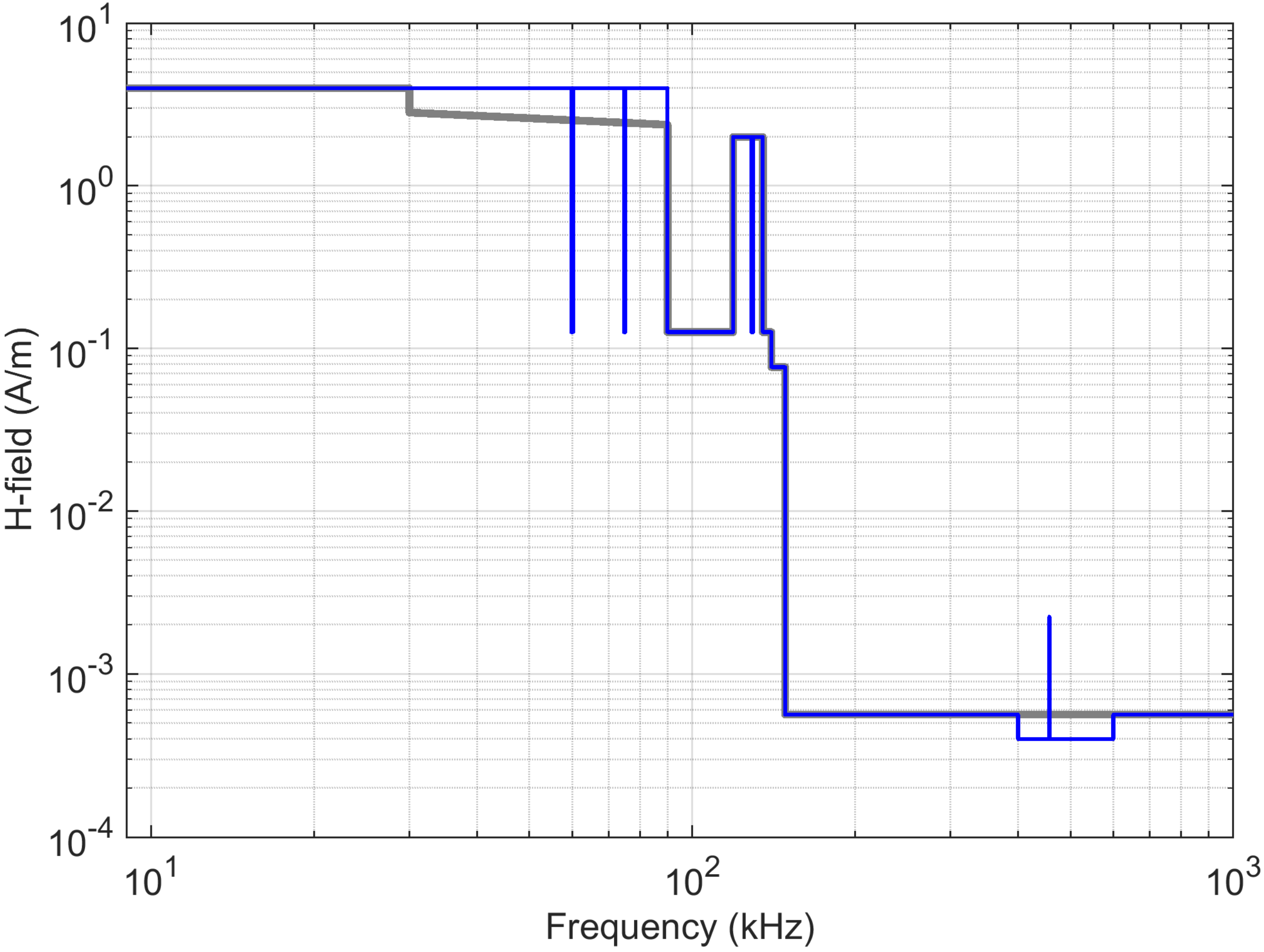
- (T2.2) protection from malfunction after application of a magnetic field at variable frequency, ranging from 1 kHz to 140 kHz and intensity of 150 A/m up to 100 kHz (linearly decreased between 100 and 140 kHz).
- Upper-frequency limit for test T1.1 reduced to 385 MHz from 450 MHz;
- Test T1.2 modified as optional characterization in the range 385 to 3000 MHz, but the tests procedure is described in detail;
- For the immunity to static magnetic fields (test T2.1), the protection from malfunction is extended to 50 mT.
3.2.2. Cochlear and Auditory Brainstem Implants
3.2.3. Neurostimulators
3.2.4. Circulatory Support Devices
3.2.5. Occupational Exposure of IMDs
3.2.6. Conclusions and General Framework
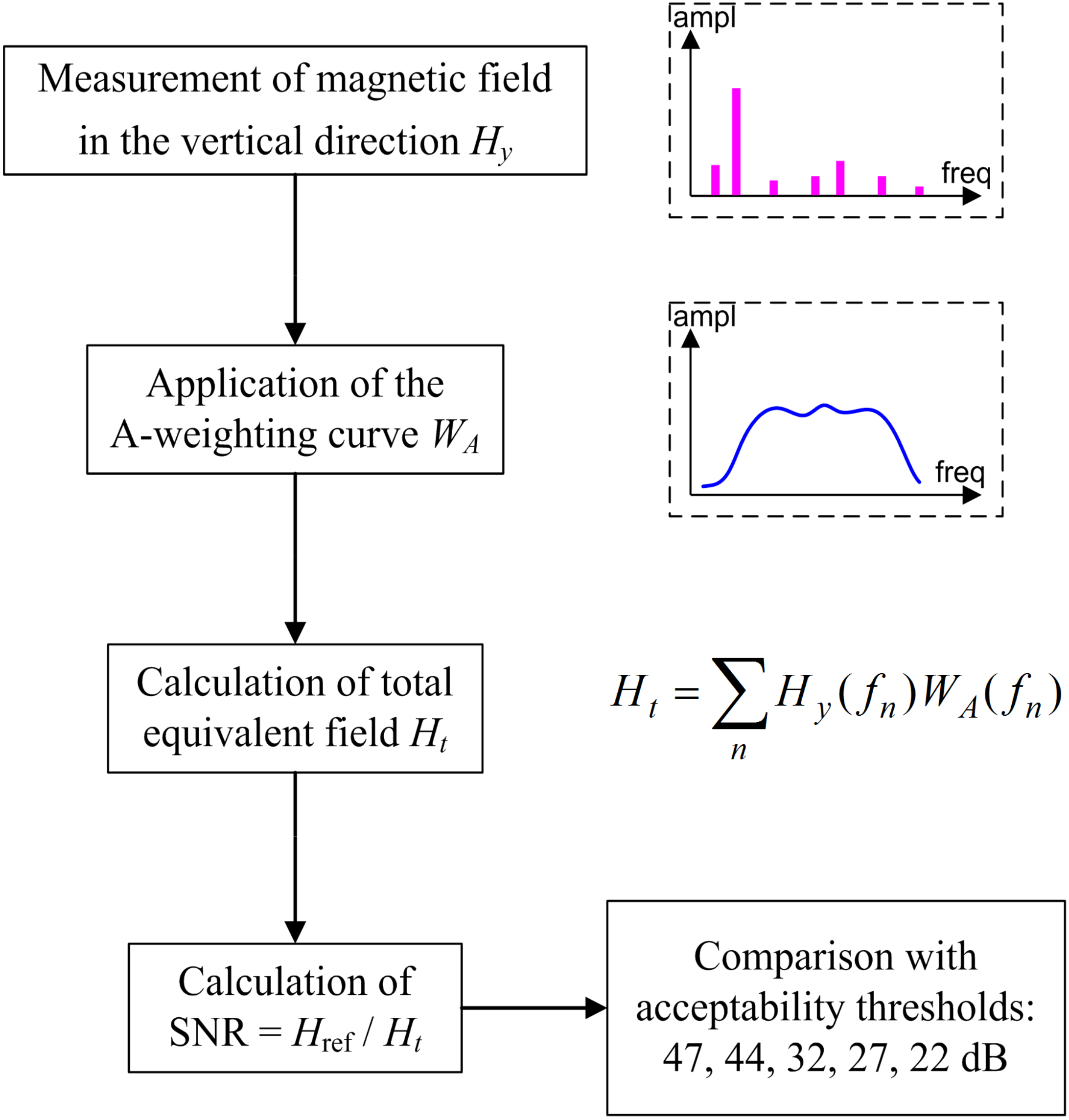
3.3. Interference to Hearing Aids
- Frequency response flat within 1 dB between 50 Hz and 10 kHz, falling with at least 6 dB/octave at the boundaries;
- Frequency response in A-weighted mode to conform between 100 Hz and 5 kHz “to Class 2 m specification in EN 61672-1 [103].”
4. Assessment and Instrumentation
4.1. Requirements for Instrumentation
4.1.1. Frequency Range
4.1.2. Dynamic Range
4.1.3. Triaxial Probe and Isotropy
4.1.4. Linearity
4.1.5. Amplitude Accuracy, Response Flatness, and Uncertainty
4.1.6. Impact of Uncertainty on Compliance
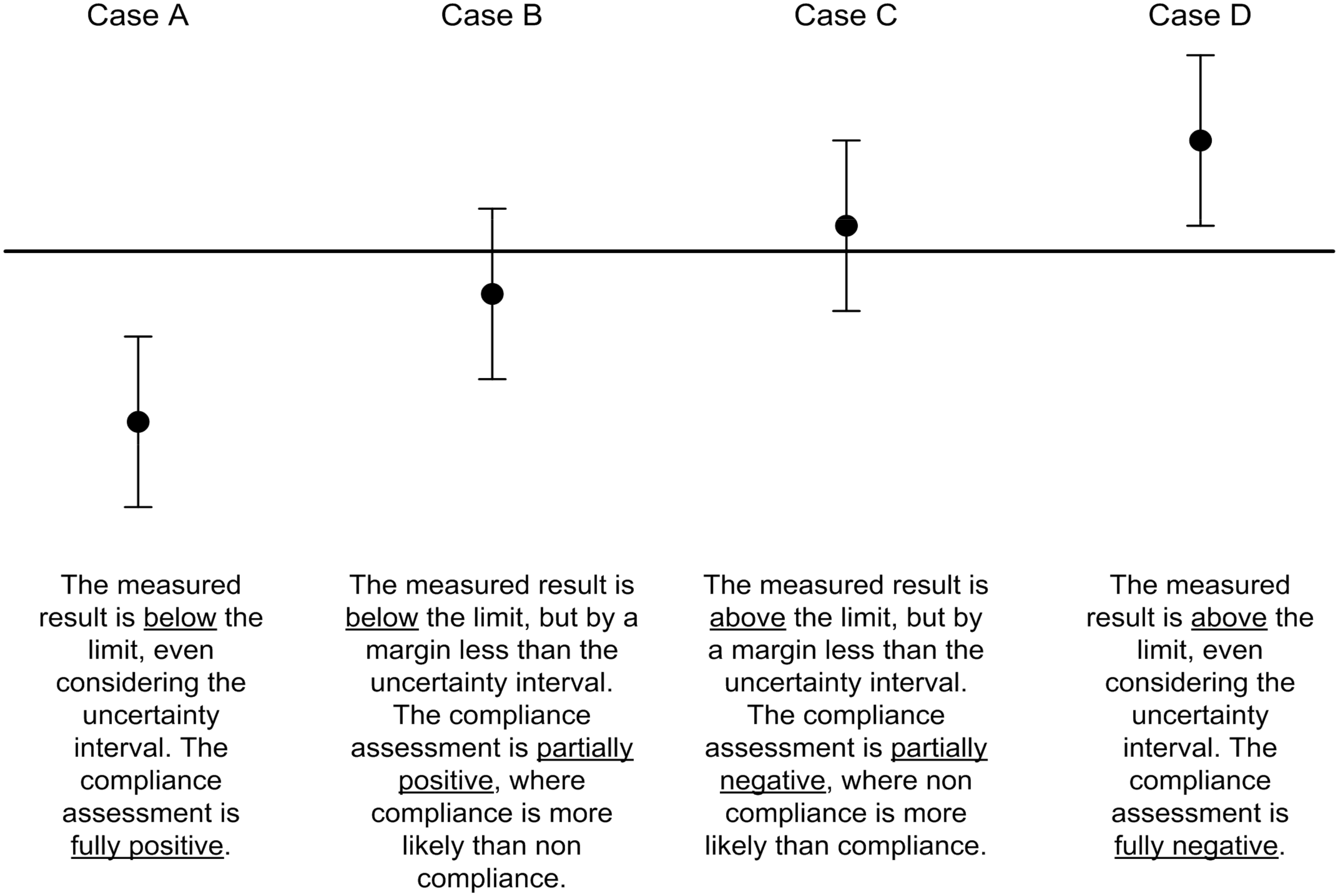
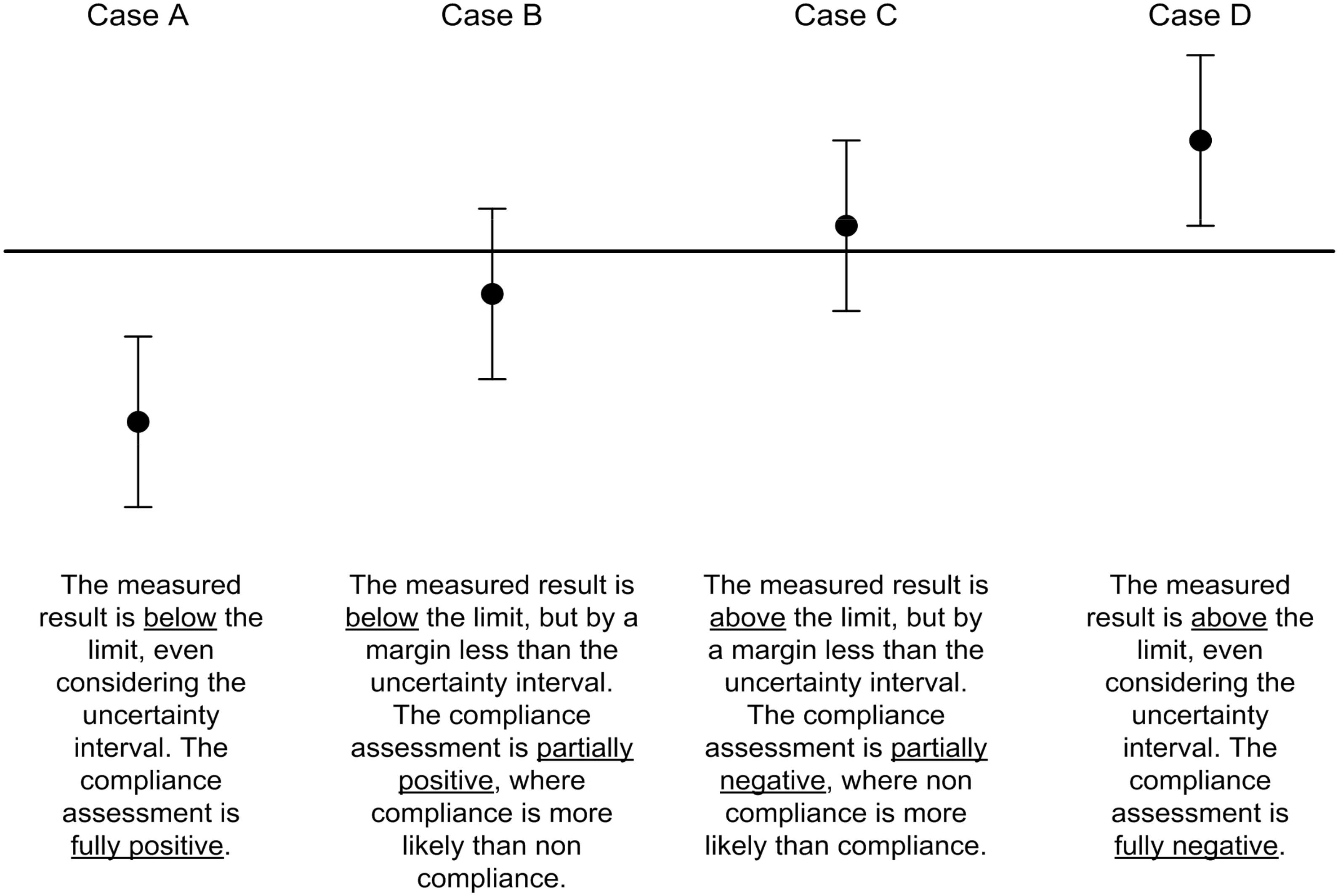
- If u(xm) ≤ umax then the measured value xm can be compared directly with the limit xlim (e.g., a reference level or the unity limit for the ICNIRP index).
- If u(xm) > umax then the actual uncertainty must be included, compared to the maximum uncertainty, resulting in a reduction of the limit by a so-called “penalty” that is shown at the denominator:
- There must be a standard specifying umax for the specific application; in many cases, compliance is interpreted in an absolute sense, so without taking into consideration uncertainty and the probabilistic nature of measured values and the outcome of assessment (a good analysis of some cases is reported in [107]).
- The uncertainty u(xm) may be related to the measurement setup and determined with a Type B approach, or associated to repeated measurements and determined with a Type A approach (including the variability of the operating conditions and the external noise sources, to cite the most evident exogenous influences, besides the instrumental uncertainty); this was discussed in detail for the measurement of electromagnetic field of large equipment and installations [108,109].
4.1.7. Factors Influencing Uncertainty and Uncertainty Budget
4.2. Human Exposure Assessment
4.3. Implantable Medical Devices
4.4. Hearing Aids
4.5. General Measurement Precautions
5. Conclusions
Funding
Conflicts of Interest
References
- ICNIRP. Guidelines for Limiting Exposure to Time-Varying Electric, Magnetic, and Electromagnetic Fields (up to 300 GHz). Health Phys. 1998, 75, 494–522. [Google Scholar]
- ICNIRP. Guidance on Determining Compliance of Exposure to Pulsed Fields and Complex Non-Sinusoidal Waveforms below 100 kHz with ICNIRP Guidelines. Health Phys. 2003, 84, 383–387. [Google Scholar]
- ICNIRP. Guidelines for Limiting Exposure to Time-Varying Electric and Magnetic Fields (1 Hz–100 kHz). Health Phys. 2010, 99, 818–836. [Google Scholar]
- ICNIRP. Guidelines for Limiting Exposure to Electromagnetic Fields (100 kHz–300 GHz). Health Phys. 2020, 118, 483–524. [Google Scholar]
- ICNIRP. Guidelines on Limits of Exposure to Static Magnetic Fields. Health Phys. 2009, 96, 504–514. [Google Scholar]
- Salvan, A.; Ranucci, A.; Lagorio, S.; Magnani, C.; SETIL Research Group. Childhood Leukemia and 50 Hz Magnetic Fields: Findings from the Italian SETIL Case-Control Study. Int. J. Environ. Res. Public Health 2015, 12, 2184–2204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajšek, P.; Ravazzani, P.; Grellier, J.; Samaras, T.; Bakos, J.; Thuróczy, G. Review of Studies Concerning Electromagnetic Field (EMF) Exposure Assessment in Europe: Low Frequency Fields (50 Hz–100 kHz). Int. J. Environ. Res. Public Health 2016, 13, 875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salceanu, A.; Paulet, M.V.; Neagu, C.D.; Bordeianu, D.F. On the coupling influence of the relative position of human trunk with respect to the overhead high-voltage power line. Acta IMEKO 2020, 9, 53–58. [Google Scholar] [CrossRef]
- Ignatenko, I.V.; Vlasenko, S.A. Health assessment of the electrical contact-line connections in view of the operational traction load pattern of the electric rolling stock. In IOP Conference Series: Materials Science and Engineering; IOP Publishing: Bristol, UK, 2020; Volume 918, p. 012154. [Google Scholar] [CrossRef]
- Safigianni, A.S.; Tsompanidou, C.G. Electric- and Magnetic-Field Measurements in an Outdoor Electric Power Substation. IEEE Trans. Power Deliv. 2008, 24, 38–42. [Google Scholar] [CrossRef]
- EU Dir. 2013/35. Directive of the European Parliament of 26 June 2013 on the Minimum Health and Safety Requirements Regarding the Exposure of Workers to the Risks Arising from Physical Agents (Electromagnetic Fields) (20th Individual Directive within the Meaning of Article 16(1) of Directive 89/391/EEC) and Repealing Directive 2004/40/EC; European Union: Brussels, Belgium, 2013. [Google Scholar]
- IEC 60118-4. Electroacoustics—Hearing Aids—Part 4: Induction-Loop Systems for Hearing Aid Purposes—System Performance Requirements; IEC: Geneva, Switzerland, 2015. [Google Scholar]
- AS 1428.5. Design for Access and Mobility—Part 5: Communication for People Who are Deaf or Hearing Impaired; Australian Standards: Sidney, NSW, Australia, 2010; (reconfirmed 2016). [Google Scholar]
- Hakuta, Y.; Watanabe, T.; Takenaka, T.; Ito, T.; Hirata, A. Safety Standard Compliance of Human Exposure From Vehicle Cables Using Coupling Factors in the Frequency Range of 0.3–400 kHz. IEEE Trans. Electromagn. Compat. 2021, 63, 313–318. [Google Scholar] [CrossRef]
- Campi, T.; Cruciani, S.; Maradei, F.; Feliziani, M. Magnetic Field during Wireless Charging in an Electric Vehicle According to Standard SAE J2954. Energies 2019, 12, 1795. [Google Scholar] [CrossRef] [Green Version]
- Cirimele, V.; Freschi, F.; Giaccone, L.; Pichon, L.; Repetto, M. Human Exposure Assessment in Dynamic Inductive Power Transfer for Automotive Applications. IEEE Trans. Magn. 2017, 53, 1–4. [Google Scholar] [CrossRef]
- Ding, P.-P.; Bernard, L.; Pichon, L.; Razek, A. Evaluation of Electromagnetic Fields in Human Body Exposed to Wireless Inductive Charging System. IEEE Trans. Magn. 2014, 50, 1037–1040. [Google Scholar] [CrossRef]
- Vassilev, A.; Ferber, A.; Wehrmann, C.; Pinaud, O.; Schilling, M.; Ruddle, A.R. Magnetic Field Exposure Assessment in Electric Vehicles. IEEE Trans. Electromagn. Compat. 2014, 57, 35–43. [Google Scholar] [CrossRef]
- Christ, A.; Douglas, M.; Nadakuduti, J.; Kuster, N. Assessing Human Exposure to Electromagnetic Fields From Wireless Power Transmission Systems. Proc. IEEE 2013, 101, 1482–1493. [Google Scholar] [CrossRef]
- Emadi, A.; Rajashekara, K.; Williamson, S.S.; Lukic, S. Topological Overview of Hybrid Electric and Fuel Cell Vehicular Power System Architectures and Configurations. IEEE Trans. Veh. Technol. 2005, 54, 763–770. [Google Scholar] [CrossRef]
- EN 103 409. System Reference Document (SRdoc); Wireless Power Transmission (WPT) Systems for Electric Vehicles (EV) Operating in the Frequency Band 79–90 kHz; ETSI: Sophia Antipolis, France, 2016. [Google Scholar]
- Celaya-Echarri, M.; Azpilicueta, L.; Lopez-Iturri, P.; Aguirre, E.; De Miguel-Bilbao, S.; Ramos, V.; Falcone, F. Spatial Characterization of Personal RF-EMF Exposure in Public Transportation Buses. IEEE Access 2019, 7, 33038–33054. [Google Scholar] [CrossRef]
- Buyakova, N.; Zakaryukin, V.; Kryukov, A.; Lagunova, N. Electromagnetic safety of railway electrification systems under deicing. Energy Saf. Energy Econ. 2018, 5, 5–10. [Google Scholar] [CrossRef]
- Halgamuge, M.N.; Abeyrathne, C.D.; Mendis, P. Measurement and analysis of electromagnetic fields from trams, trains and hybrid cars. Radiat. Prot. Dosim. 2010, 141, 255–268. [Google Scholar] [CrossRef]
- Bellan, D.; Gaggelli, A.; Maradei, F.; Mariscotti, A.; Pignari, S. Time-Domain Measurement and Spectral Analysis of Nonstationary Low-Frequency Magnetic-Field Emissions on Board of Rolling Stock. IEEE Trans. Electromagn. Compat. 2004, 46, 12–23. [Google Scholar] [CrossRef]
- EN 50500. Measurement Procedures of Magnetic Field Levels Generated by Electronic and Electrical Apparatus in the Railway Environment with Respect to Human Exposure; CENELEC: Brussels, Belgium, 2015. [Google Scholar]
- Mariscotti, A.; Sandrolini, L. Review of models and measurement methods for compliance of electromagnetic emissions of electric machines and drives. Acta IMEKO 2021, 10, 162–173. [Google Scholar] [CrossRef]
- IEC 62597. Measurement Procedures of Magnetic Field Levels Generated by Electronic and Electrical Apparatus in the Railway Environment with Respect to Human Exposure; IEC: Geneva, Switzerland, 2019. [Google Scholar]
- EN 300 330. Short Range Devices (SRD);Radio Equipment in the Frequency Range 9 kHz to 25 MHz and Inductive Loop Systems in the Frequency Range 9 kHz to 30 MHz; Harmonised Standard Covering the Essential Requirements of Article 3.2 of Directive 2014/53/EU; ETSI: Sophia Antipolis, France, 2016. [Google Scholar]
- EU Commission. Decision of the EU Commission no. 2017/1483 of 8 August 2017 Amending Decision 2006/771/EC on Harmonisation of the Radio Spectrum for Use by Short-Range Devices and Repealing Decision 2006/804/EC; European Union: Brussels, Belgium, 2017. [Google Scholar]
- Sandrolini, L.; Mariscotti, A. Signal Transformations for Analysis of Supraharmonic EMI Caused by Switched-Mode Power Supplies. Electronics 2020, 9, 2088. [Google Scholar] [CrossRef]
- Sandrolini, L.; Mariscotti, A. Impact of short-time fourier transform parameters on the accuracy of EMI spectra estimates in the 2-150 kHz supraharmonic interval. Electr. Power Syst. Res. 2021, 195, 107130. [Google Scholar] [CrossRef]
- Canova, A.; Freschi, F.; Giaccone, L.; Repetto, M. Exposure of Working Population to Pulsed Magnetic Fields. IEEE Trans. Magn. 2010, 46, 2819–2822. [Google Scholar] [CrossRef]
- Sipus, Z.; Susnjara, A.; Skrivervik, A.K.; Poljak, D.; Bosiljevac, M. Influence of Uncertainty of Body Permittivity on Achievable Radiation Efficiency of Implantable Antennas—Stochastic Analysis. IEEE Trans. Antennas Propag. 2021, 69, 6894–6905. [Google Scholar] [CrossRef]
- Huang, Y.; Wiart, J. Simplified Assessment Method for Population RF Exposure Induced by a 4G Network. IEEE J. Electromagn. RF Microwaves Med. Biol. 2017, 1, 34–40. [Google Scholar] [CrossRef]
- Susnjara, A.; Dodig, H.; Poljak, D.; Cvetkovic, M. Stochastic-Deterministic Thermal Dosimetry Below 6 GHz for 5G Mobile Communication Systems. IEEE Trans. Electromagn. Compat. 2021, PP, 1–13. [Google Scholar] [CrossRef]
- IEEE Std. C95.1. IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz; IEEE: Piscataway, NJ, USA, 2005. [Google Scholar]
- IEEE Std. C95.6. IEEE Standard for Safety Levels with Respect to Human Exposure to Electromagnetic Fields, 0-3 kHz; IEEE: Piscataway, NJ, USA, 2002. [Google Scholar]
- IEEE Std. C95.1. IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar]
- IEEE Std. C95.3.1. IEEE Recommended Practice for Measurement and Computation of Electric, Magnetic, and Electromagnetic Fields with Respect to Human Exposure to Such Fields, 0 Hz to 100 kHz; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar]
- Stam, R. Comparison of International Policies on Electromagnetic Fields (Power Frequency and Radiofrequency Fields); National Institute for Public Health and the Environment: Utrecht, The Netherlands, 2017.
- Madjar, H.M. Human radio frequency exposure limits: An update of reference levels in Europe, USA, Canada, China, Japan and Korea. In Proceedings of the International Symposium on Electromagnetic Compatibility—EMC EUROPE, Wroclaw, Poland, 5–9 September 2016. [Google Scholar] [CrossRef]
- Taki, M. Bioelectromagnetics researches in Japan for human protection from electromagnetic field exposures. IEEJ Trans. Electr. Electron. Eng. 2016, 11, 683–695. [Google Scholar] [CrossRef]
- Yamazaki, K. Assessment methods for electric and magnetic fields in low and intermediate frequencies related to human exposures and the status of their standardization. Electron. Commun. Jpn. 2020, 103, 10–18. [Google Scholar] [CrossRef]
- Nyenhuis, J.A.; Bourland, J.D.; Kildishev, A.V.; Schaefer, D.J. Health effects and safety of intense gradient fields. In Magnetic Resonance Procedures: Health Effects and Safety; CRC Press: Boca Raton, FL, USA, 2016; pp. 31–54. [Google Scholar]
- So, P.; Stuchly, M.; Nyenhuis, J. Peripheral Nerve Stimulation by Gradient Switching Fields in Magnetic Resonance Imaging. IEEE Trans. Biomed. Eng. 2004, 51, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Diao, Y.; Gomez-Tames, J.; Rashed, E.A.; Kavet, R.; Hirata, A. Spatial Averaging Schemes of In Situ Electric Field for Low-Frequency Magnetic Field Exposures. IEEE Access 2019, 7, 184320–184331. [Google Scholar] [CrossRef]
- Saunders, R.D.; Jefferys, J. Weak electric field interactions in the central nervous system. Heal. Phys. 2002, 83, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.D.; Jefferys, J.G.R. A neurobiological basis for ELF guidelines. Heal. Phys. 2007, 92, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Kanai, R.; Chaieb, L.; Antal, A.; Walsh, V.; Paulus, W. Frequency-Dependent Electrical Stimulation of the Visual Cortex. Curr. Biol. 2008, 18, 1839–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Environmental Health Criteria No. 238—Extremely Low Frequency (ELF) Fields; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Hirata, A.; Wake, K.; Watanabe, S.; Taki, M. In-situ electric field and current density in Japanese male and female models for uniform magnetic field exposures. Radiat. Prot. Dosim. 2009, 135, 272–275. [Google Scholar] [CrossRef] [Green Version]
- Magne, I.; Deschamps, F. Electric field induced in the human body by uniform 50 Hz electric or magnetic fields: Bibliography analysis and method for conservatively deriving measurable limits. J. Radiol. Prot. 2016, 36, 419–436. [Google Scholar] [CrossRef] [PubMed]
- IEC 60479-1. Effects of Current on Human Beings and Livestock—Part 1: General Aspects; IEC: Geneva, Switzerland, 2018. [Google Scholar]
- IEC 63167. Assessment of Contact Current Related to Human Exposure to Electric, Magnetic and Electromagnetic Fields; IEC: Geneva, Switzerland, 2018. [Google Scholar]
- Dimbylow, P.J. Current densities in a 2 mm resolution anatomically realistic model of the body induced by low frequency electric fields. Phys. Med. Biol. 2000, 45, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Dimbylow, P. Development of pregnant female, hybrid voxel-mathematical models and their application to the dosimetry of applied magnetic and electric fields at 50 Hz. Phys. Med. Biol. 2006, 51, 2383–2394. [Google Scholar] [CrossRef] [PubMed]
- Barchanski, A.; De Gersem, H.; Gjonaj, E.; Weiland, T. Impact of the displacement current on low-frequency electromagnetic fields computed using high-resolution anatomy models. Phys. Med. Biol. 2005, 50, N243–N249. [Google Scholar] [CrossRef]
- Park, S.W.; Wake, K.; Watanabe, S. Calculation Errors of the Electric Field Induced in a Human Body Under Quasi-Static Approximation Conditions. IEEE Trans. Microw. Theory Tech. 2013, 61, 2153–2160. [Google Scholar] [CrossRef]
- Gao, X.; Su, D. Suppression of a Certain Vehicle Electrical Field and Magnetic Field Radiation Resonance Point. IEEE Trans. Veh. Technol. 2017, 67, 226–234. [Google Scholar] [CrossRef]
- Küllmer, A.; Hermanns, K.; Enders, A. Field emission characteristics of high power converters. In Proceedings of the IEEE International Sympocium on Electromagnetic Compatibility, Brugge, Belgium, 2–6 September 2013. [Google Scholar]
- Witters, D. Facing the Challenges of Electromagnetic Interference With Medical Devices in the Wireless World. In Proceedings of the 27th General Assembly of the International Union of Radio Science, Maastricht, The Netherlands, 17–24 August 2002. [Google Scholar]
- Pinski, S.L.; Trohman, R.G. Interference in implanted cardiac devices, Part I. Pacing Clin. Electrophysiol. 2002, 25, 1367–1381. [Google Scholar] [CrossRef] [PubMed]
- Irnich, W. Electronic security systems and active implantable medical devices. Pacing Clin. Electrophysiol. 2002, 25, 1235–1258. [Google Scholar] [CrossRef] [PubMed]
- McIvor, M.E.; Reddinger, J.; Floden, E.; Sheppard, R.C.; Johnson, D.; Becker, G.I.; Mayotte, M. Study of Pacemaker and Implantable Cardioverter Defibrillator Triggering by Electronic Article Surveillance Devices (SPICED TEAS). Pacing Clin. Electrophysiol. 1998, 21, 1847–1861. [Google Scholar] [CrossRef] [PubMed]
- EN 50364. Product Standard for Human Exposure to Electromagnetic Fields from Devices Operating in the Frequency Range 0 Hz to 300 GHz, Used in Electronic Article Surveillance (EAS), Radio Frequency Identification (RFID) and Similar Applications; CENELEC: Brussels, Belgium, 2018. [Google Scholar]
- Gercek, C.; Kourtiche, D.; Nadi, M.; Magne, I.; Schmitt, P.; Souques, M. Computation of Pacemakers Immunity to 50 Hz Electric Field: Induced Voltages 10 Times Greater in Unipolar Than in Bipolar Detection Mode. Bioengineering 2017, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- EN 50527-2-1. Procedure for the Assessment of the Exposure to Electromagnetic Fields of Workers Bearing Active Implantable Medical Devices—Part 1: General; CENELEC: Brussels, Belgium, 2016. [Google Scholar]
- EN 50527-2-2. Procedure for the Assessment of the Exposure to Electromagnetic Fields of Workers Bearing Active Implantable Medical Devices—Part 2-2: Specific Assessment for Workers with Cardioverter Defibrillators (ICDs); CENELEC: Brussels, Belgium, 2018. [Google Scholar]
- ISO 14117. Active Implantable Medical Devices—Electromagnetic Compatibility—EMC Test Protocols for Implantable Cardiac Pacemakers, Implantable Cardioverter Defibrillators and Cardiac Resynchronization Devices; ISO: Geneva, Switzerland, 2019. [Google Scholar]
- ISO 19363. Electrically Propelled Road Vehicles—Magnetic Field Wireless Power Transfer—Safety and Interoperability Requirements; ISO: Geneva, Switzerland, 2020. [Google Scholar]
- IEC 60118-13. Electroacoustics—Hearing Aid —Part 13: Electromagnetic Compatibility (EMC); IEC: Geneva, Switzerland, 2016. [Google Scholar]
- Welcome Aboard the Fleet of the Future. Available online: https://www.bart.gov/about/projects/cars (accessed on 3 August 2021).
- InnoTrans—Ampetronic. Available online: https://www.innotrans.de/en/preview/exhibitors-products/public-transport.html (accessed on 3 August 2021).
- EU Dir. 519/1999. Council Recommendation of 12 July 1999 on the Limitation of Exposure of the General Public to Electromagnetic Fields (0 Hz to 300 GHz); European Union: Brussels, Belgium, 1999. [Google Scholar]
- IEC 61786-2. Measurement of DC Magnetic, AC Magnetic and AC Electric Fields from 1 Hz to 100 kHz with Regard to Exposure of Human Beings—Part 2: Basic Standard for Measurements; IEC: Geneva, Switzerland, 2014. [Google Scholar]
- EN 62110. Electric and Magnetic Field Levels Generated by AC Power Systems—Measurement Procedures with Regard to Public Exposure; CENELEC: Brussels, Belgium, 2009. [Google Scholar]
- IEC 62311. Assessment of Electronic and Electrical Equipment Related to Human Exposure Restrictions for Electromagnetic Fields (0 Hz to 300 GHz); IEC: Geneva, Switzerland, 2019. [Google Scholar]
- IEC 62493. Assessment of Lighting Equipment Related to Human Exposure to Electromagnetic Field; IEC: Geneva, Switzerland, 2015. [Google Scholar]
- IEC 62905. Exposure Assessment Methods for Wireless Power Transfer Systems; IEC: Geneva, Switzerland, 2018. [Google Scholar]
- Campi, T.; Cruciani, S.; De Santis, V.; Maradei, F.; Feliziani, M. Numerical characterization of the magnetic field in electric vehicles equipped with a WPT system. Wirel. Power Transf. 2017, 4, 78–87. [Google Scholar] [CrossRef]
- IEC 62233. Measurement Methods for Electromagnetic Fields of Household Appliances and Similar Apparatus with Regard to Human Exposure; IEC: Geneva, Switzerland, 2005. [Google Scholar]
- Piper, S.; Ball, L.; Mandziuk, M. Numerical Modeling Application of ICNIRP Guidelines to Automobile Occupant Protection. In Proceedings of the IEEE Sympocium on Electromagnetic Compatibility, Signal Integrity and Power Integrity, Long Beach, CA, USA, 30 July–3 August 2018. [Google Scholar] [CrossRef]
- Willmann, B.; Rabe, H.; Leugers, C.; Sassi, O.; Waldera, C.; Vick, R. Current-based EMF assessment method for vehicles. In Proceedings of the International Symposium on Electromagnetic Compatibility—EMC EUROPE, Barcelona, Spain, 2–6 September 2019. [Google Scholar] [CrossRef]
- Lisewski, T.; Mikolajczyk, A.; Abramik, S.; Rucinski, M. Zero Phase Shift Digital Filtering for Assessment of Exposure to Non-Sinusoidal Magnetic Fields. In Proceedings of the International Sympocium on Electromagnetic Compatibility—EMC EUROPE 2016, Wroclaw, Poland, 5–9 September 2016. [Google Scholar] [CrossRef]
- Ruddle, A.R.; Low, L.; Vassilev, A. Evaluating Low Frequency Magnetic Field Exposure from Traction Current Transients in Electric Vehicles. In Proceedings of the International Sympocium on Electromagnetic Compatibility, Brugge, Belgium, 2–6 September 2013. [Google Scholar]
- IEC 61786-1. Measurement of DC Magnetic, AC Magnetic and AC Electric Fields from 1 Hz to 100 kHz with Regard to Exposure of Human Beings—Part 1: Requirements for Measuring Instruments; IEC: Geneva, Switzerland, 2013. [Google Scholar]
- Giaccone, L.; Giordano, D.; Crotti, G. Identification and Correction of Artifact in the Measurement of Pulsed Magnetic Fields. IEEE Trans. Instrum. Meas. 2017, 66, 1260–1266. [Google Scholar] [CrossRef] [Green Version]
- Mariscotti, A. Characterization of Active Power Flow at Harmonics for AC and DC Railway Vehicles. In Proceedings of the IEEE Vehicle Power and Propulsion Conference, Hanoi, Vietnam, 14–17 October 2019. [Google Scholar] [CrossRef] [Green Version]
- EN 45502-1. Implants for Surgery—Active Implantable Medical Devices—Part 1: General Requirements for Safety, Marking and for Information to Be Provided by the Manufacturer; CENELEC: Brussels, Belgium, 2003. [Google Scholar]
- EN 45502-2-1. Active Implantable Medical Devices—Part 2-1: Particular Requirements for Active Implantable Medical Devices Intended to Treat Bradyarrhythmia (Cardiac Pacemakers); CENELEC: Brussels, Belgium, 2003. [Google Scholar]
- EN 45502-2-2. Active Implantable Medical Devices—Part 2-2: Particular Requirements for Active Implantable Medical Devices Intended to Treat Tachyarrhythmia (Includes Implantable Defibrillators); CENELEC: Brussels, Belgium, 2008. [Google Scholar]
- EN 45502-2-3. Active Implantable Medical Devices—Part 2-3: Particular Requirements for Cochlear and Auditory Brainstem Implant Systems; CENELEC: Brussels, Belgium, 2010. [Google Scholar]
- ISO. ISO 14708-1, Implants for Surgery—Active Implantable Medical Devices—Part 1: General Requirements for Safety, Marking and for Information to Be Provided by the Manufacturer; ISO: Geneva, Switzerland, 2014. [Google Scholar]
- ISO. ISO 14708-2, Implants for Surgery—Active Implantable Medical Devices—Part 2: Cardiac Pacemakers; ISO: Geneva, Switzerland, 2019. [Google Scholar]
- ISO. ISO 14708-3, Implants for Surgery—Active Implantable Medical Devices—Part 3: Implantable Neurostimulators; ISO: Geneva, Switzerland, 2017. [Google Scholar]
- ISO. ISO 14708-5, Implants for Surgery—Active Implantable Medical devices—Part 5: Circulatory Support Devices; ISO: Geneva, Switzerland, 2020. [Google Scholar]
- ISO. ISO 14708-6, Implants for Surgery—Active Implantable Medical Devices—Part 6: Particular Requirements for Active Implantable Medical Devices Intended to treat Tachyarrhythmia (including Implantable Defibrillators); ISO: Geneva, Switzerland, 2019. [Google Scholar]
- ISO. ISO 14708-7, Implants for Surgery—Active Implantable Medical Devices—Part 7: Particular Requirements for Cochlear and Auditory Brainstem Implant Systems; ISO: Geneva, Switzerland, 2019. [Google Scholar]
- EN 50527-2-3. (Draft) Procedure for the Assessment of the Exposure to Electromagnetic Fields of Workers Bearing Active Implantable Medical Devices—Part 2–3: Specific Assessment for Workers with Neurostimulators; CENELEC: Brussels, Belgium, 2019. [Google Scholar]
- Tiikkaja, M.; Alanko, T.; Lindholm, H.; Hietanen, M.; Hartikainen, J.; Toivonen, L. Experimental study on malfunction of pacemakers due to exposure to different external magnetic fields. J. Interv. Card. Electrophysiol. 2012, 34, 19–27. [Google Scholar] [CrossRef]
- Napp, A.; Joosten, S.; Stunder, D.; Knackstedt, C.; Zink, M.; Bellmann, B.; Marx, N.; Schauerte, P.; Silny, J. Electromagnetic Interference With Implantable Cardioverter-Defibrillators at Power Frequency—An in Vivo Study. Circulation 2014, 129, 441–450. [Google Scholar] [CrossRef] [Green Version]
- EN 61672-1. Electroacoustics—Sound Level Meters—Part 1: Specifications; CENELEC: Brussels, Belgium, 2013. [Google Scholar]
- ANSI S3.22. Specification of Hearing Aid Characteristics; ANSI: New York, NY, USA, 2014. [Google Scholar]
- Mariscotti, A. A Magnetic Field Probe With MHz Bandwidth and 7-Decade Dynamic Range. IEEE Trans. Instrum. Meas. 2009, 58, 2643–2652. [Google Scholar] [CrossRef]
- Mariscotti, A. Power quality metrics for DC grids with pulsed power loads. Acta IMEKO 2021, 10, 153–161. [Google Scholar] [CrossRef]
- Miceli, R.; Spataro, C.; Roscia, M. Reduction of the uncertainty in the measurements of magnetic fields. In Proceedings of the International Conference on Renewable Energy Research and Application, Milwaukee, WI, USA, 19–22 October 2014. [Google Scholar] [CrossRef]
- Mariscotti, A. Measurement Procedures and Uncertainty Evaluation for Electromagnetic Radiated Emissions From Large-Power Electrical Machinery. IEEE Trans. Instrum. Meas. 2007, 56, 2452–2463. [Google Scholar] [CrossRef]
- Mariscotti, A. Assessment of Electromagnetic Emissions From Synchronous Generators and Its Metrological Characterization. IEEE Trans. Instrum. Meas. 2009, 59, 450–457. [Google Scholar] [CrossRef]
- JCGM 100. Evaluation of Measurement Data—Guide to the Expression of Uncertainty in Measurement; BIPM: Sevres, France, 2008. [Google Scholar]
- Farrance, I.; Frenkel, R. Uncertainty of Measurement: A Review of the Rules for Calculating Uncertainty Components through Functional Relationships. Clin. Biochem. Rev. 2012, 33, 49–75. [Google Scholar] [PubMed]
- IEEE Std. 644. IEEE Standard Procedures for Measurements of Power Frequency Electric and Magnetic Fields from AC Power Lines; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar]
- Carobbi, C.F.M.; Lallechere, S.; Arnaut, L.R. Review of Uncertainty Quantification of Measurement and Computational Modeling in EMC Part I: Measurement Uncertainty. IEEE Trans. Electromagn. Compat. 2019, 61, 1690–1698. [Google Scholar] [CrossRef]
- Wavecontrol, WP400 Probe Datasheet. Available online: https://www.wavecontrol.com/rfsafety/en/products/probes#WP400 (accessed on 29 September 2021).
- Narda, ELT 400 Exposure Level Tester. Available online: https://www.narda-sts.com/en/wideband-emf/elt-400/ (accessed on 29 September 2021).
- Aaronia, Spectran 5030/5035 Datasheet. Available online: https://testequipmentconnection.com/specs/Aaronia_Spectran_NF_5035.PDF (accessed on 29 September 2021).
- Mohamed, A.A.S.; Meintz, A.; Schrafel, P.; Calabro, A. In-Vehicle Assessment of Human Exposure to EMFs from 25-kW WPT System Based on Near-Field Analysis. In Proceedings of the IEEE Vehicle Power and Propulsion Conference (VPPC), Chicago, IL, USA, 27–30 August 2018. [Google Scholar] [CrossRef]
- IEC 61980-1. Electric Vehicle Wireless Power Transfer (WPT) Systems—Part 1: General Requirements; IEC: Geneva, Switzerland, 2021. [Google Scholar]
- IEC 62764-1. Measurement Procedures of Magnetic Field Levels Generated by Electronic and Electrical Equipment in the Automotive Environment with Respect to Human Exposure—Part 1: Low Frequency Magnetic Fields; IEC: Geneva, Switzerland, 2019. [Google Scholar]




| Freq. Range [kHz] | Power Level [kW] | Application |
|---|---|---|
| 19–21 | >20 | S. Korea, UK, Germany |
| 59–61 | >20 | S. Korea, UK, Germany |
| 79–90 | 3.7–20 | Worldwide |
| 100–119 119–135 135–140 140–148.5 148.5–300 | <0.15 | Worldwide |
| 36–40 | — | under disc. CISPR |
| 55–65 | — | under disc. CISPR |
| Standard | Distance from Source [m] | Height above Ground [m] |
|---|---|---|
| IEC 62110 [77] (AC power systems) | — 0.2 (1) | 1 0.5, 1.0, 1.5 |
| IEC 62597 [28] (2) (Rolling stock) | 0.3 | 1.0, 1.5 (wrk in rsk) 0.3, 1.0, 1.5 (pub in rsk) 0.5, 1.5, 2.5 (wrk/pub out rsk) 0.5, 1.0, 1.5 (platforms) |
| IEC 62493 [79] (Lighting) | 0.5–2.0 (3) | — |
| ISO 19363 [71] (4) (WPT) | 0.2 | up to height of vehicle three points midway on seat, back, and headrest |
| IEC 62905 [80] (WPT) | 0.2 | 0.5, 1.0, 1.5 |
| Frequency Range | Criterion A Test Level | Criterion B Test Level | Modulation |
|---|---|---|---|
| 16–40 Hz | 240 A/m (301 μT) | 340 A/m (427 μT) | CW sin. |
| 50–100 Hz | 210 Am (301 μT) | 850 A/m (1068 μT) | CW sin. |
| 200–400 Hz | 210 A/m (301 μT) | 540 A/m (678 μT) | CW sin. |
| 0.5–3 kHz | 30 A/m (37.7 μT) | 106 A/m (133 μT) | CW sin. |
| 4–9 kHz | 30 A/m (37.7 μT) | 106 A/m (133 μT) | CW sin. |
| 10–150 kHz | 30 A/m (37.7 μT) | 106 A/m (133 μT) | 1 kHz, PM |
| 0.2–3 MHz | 4 A/m (5.0 μT) | 21 A/m (26.5 μT) | 1 kHz, PM |
| 4–10 MHz | 2 A/m (2.5 μT) | 21 A/m (26.5 μT) | 1 kHz, PM |
| Frequency Range | Criterion A Test Level | Modulation |
|---|---|---|
| 1–3 kHz | 84/f A/m (105.6/f μT) | 2 Hz, AM 95% |
| 3–150 kHz | 28 Am (35 μT) | 2 Hz, AM 95% |
| Frequency Range | Criterion A Test Level | Modulation |
|---|---|---|
| 1–100 kHz | 150 A/m (188.4/f μT) | CW sin. |
| 100–140 kHz | 15,000/f A/m (18.84/f mT) | CW sin. |
| Item | Source of Uncertainty | Distribution | Exemplified Tolerance/Range |
|---|---|---|---|
| 1 | Field amplitude (probe calibration uncertainty, possible use of flat gain; cannot be better than internal noise #10) | normal/ rectangular | often ambiguously specified as “accuracy”, typ. ±1% to ±3% |
| 2 | Field gradient (probe calibration uncertainty, spatially integrated gradient, see item #7 and #8) | normal | not available for all examined instruments |
| 3 | Probe anisotropy | rectangular (4) | declared often as ±5%, barely addressing compliance to standards |
| 4 | Probe linearity (relevant with large fundamental components) | rectangular | typ. ±1%, better for limited range |
| 5 | Probe frequency domain response (1) | rectangular | not fully specified, typ. ±1 dB at corner frequencies |
| 6 | Probe modulation response (e.g., with square pulse modulation) | rectangular | not available for all examined instruments |
| 7 | Probe spatial averaging (depends on probe area) (2) | rectangular | standard coil cross-sections of 100 and 3 cm2 |
| 8 | Gradient uncertainty | rectangular | not available for all examined instruments |
| 9 | Parasitic E-field sensitivity (applicable to magnetic field probe) | rectangular | negligible for shielded construction |
| 10 | Internal noise (to evaluate, e.g., at 1–10% of the general public exposure; includes thermal and quantization noise) | normal | typ. 1% of full scale; higher for large dynamic ranges and in overload |
| 11 | Additional shaping, filtering, signal conditioning | rectangular/normal | If digital implementation, uncertainty negligible. If analog implementation, variable but up to 0.3–0.5% |
| 12 | Spatial positioning and moving error (3) | rectangular | site dependent, must be evaluated case by case |
| 13 | Repeatability (dispersion for repeated measurements) | normal | not available for all examined instruments; replaced by a statement of total uncertainty typ. ±5% to ±7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mariscotti, A. Assessment of Human Exposure (Including Interference to Implantable Devices) to Low-Frequency Electromagnetic Field in Modern Microgrids, Power Systems and Electric Transports. Energies 2021, 14, 6789. https://doi.org/10.3390/en14206789
Mariscotti A. Assessment of Human Exposure (Including Interference to Implantable Devices) to Low-Frequency Electromagnetic Field in Modern Microgrids, Power Systems and Electric Transports. Energies. 2021; 14(20):6789. https://doi.org/10.3390/en14206789
Chicago/Turabian StyleMariscotti, Andrea. 2021. "Assessment of Human Exposure (Including Interference to Implantable Devices) to Low-Frequency Electromagnetic Field in Modern Microgrids, Power Systems and Electric Transports" Energies 14, no. 20: 6789. https://doi.org/10.3390/en14206789
APA StyleMariscotti, A. (2021). Assessment of Human Exposure (Including Interference to Implantable Devices) to Low-Frequency Electromagnetic Field in Modern Microgrids, Power Systems and Electric Transports. Energies, 14(20), 6789. https://doi.org/10.3390/en14206789