Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Case Presentation
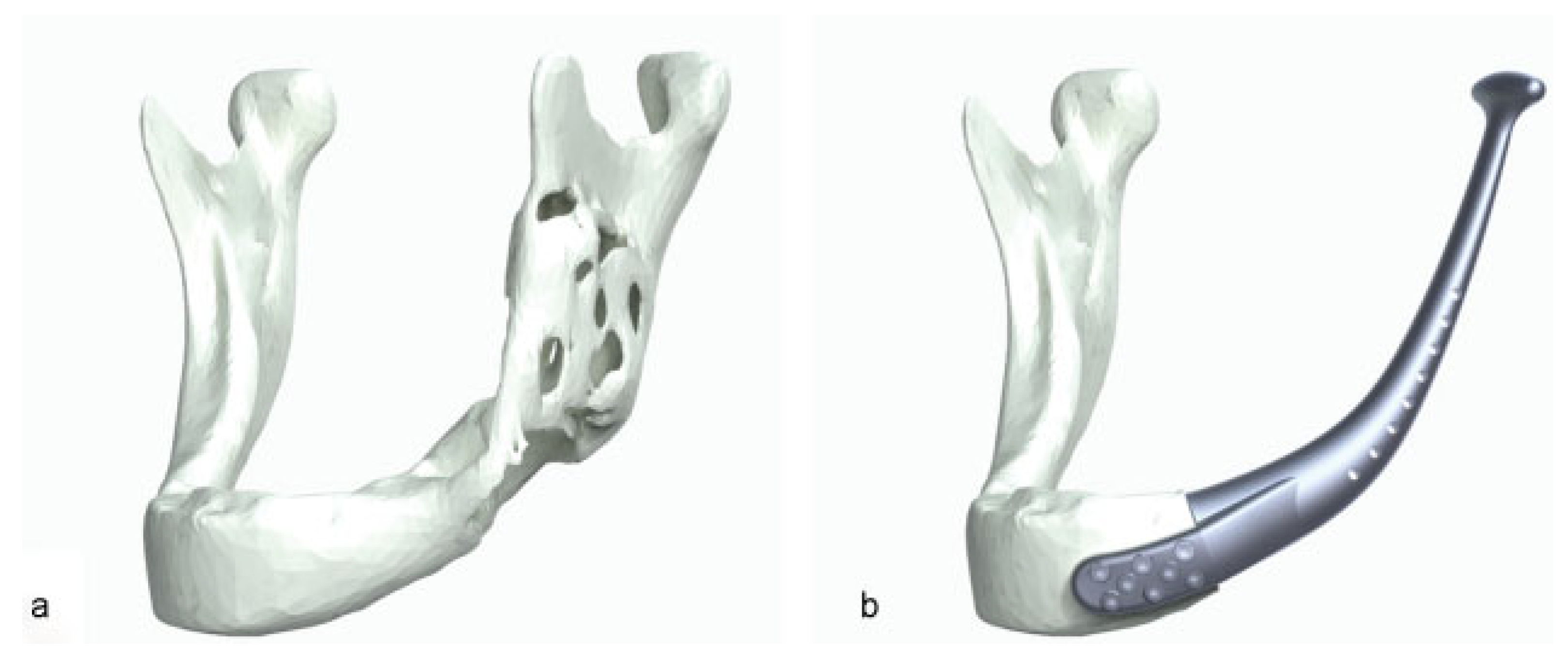
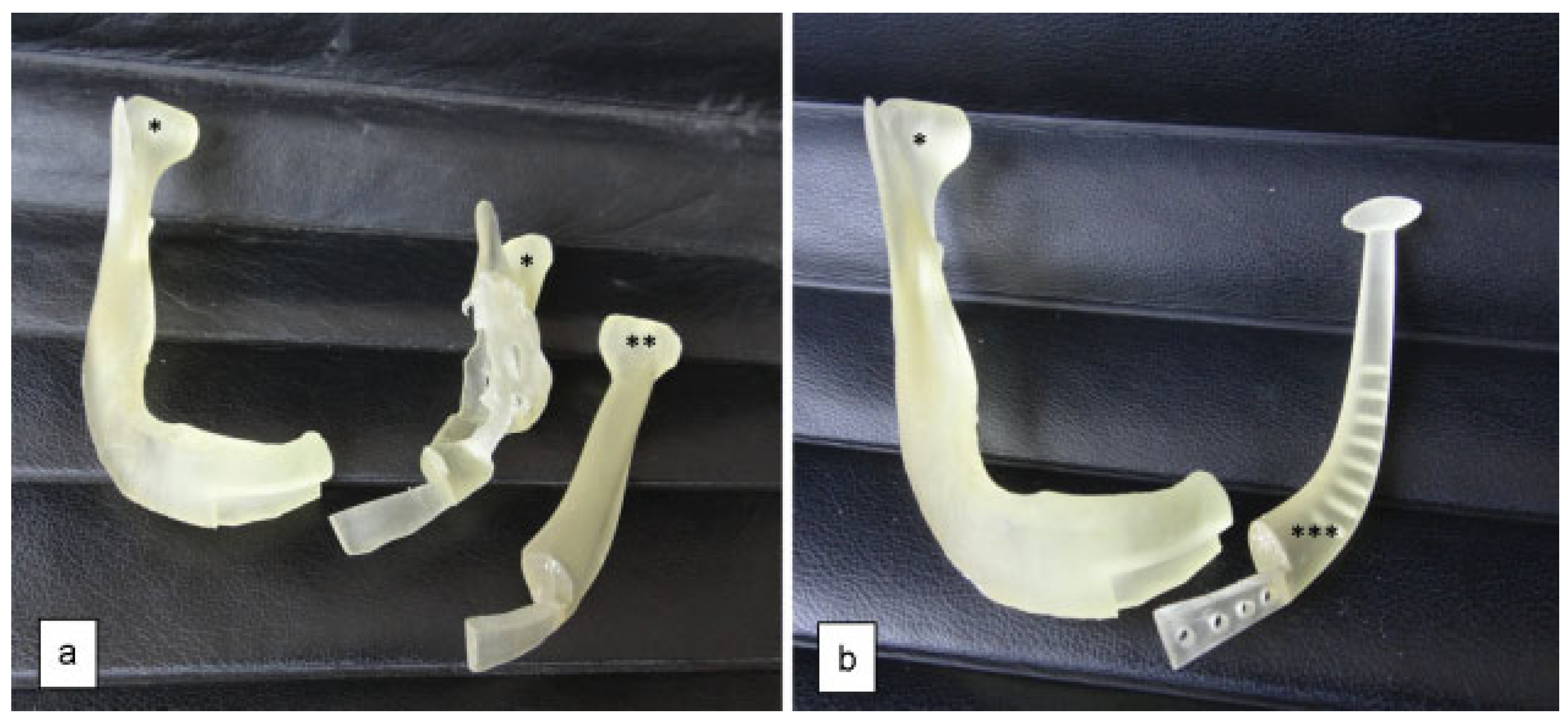
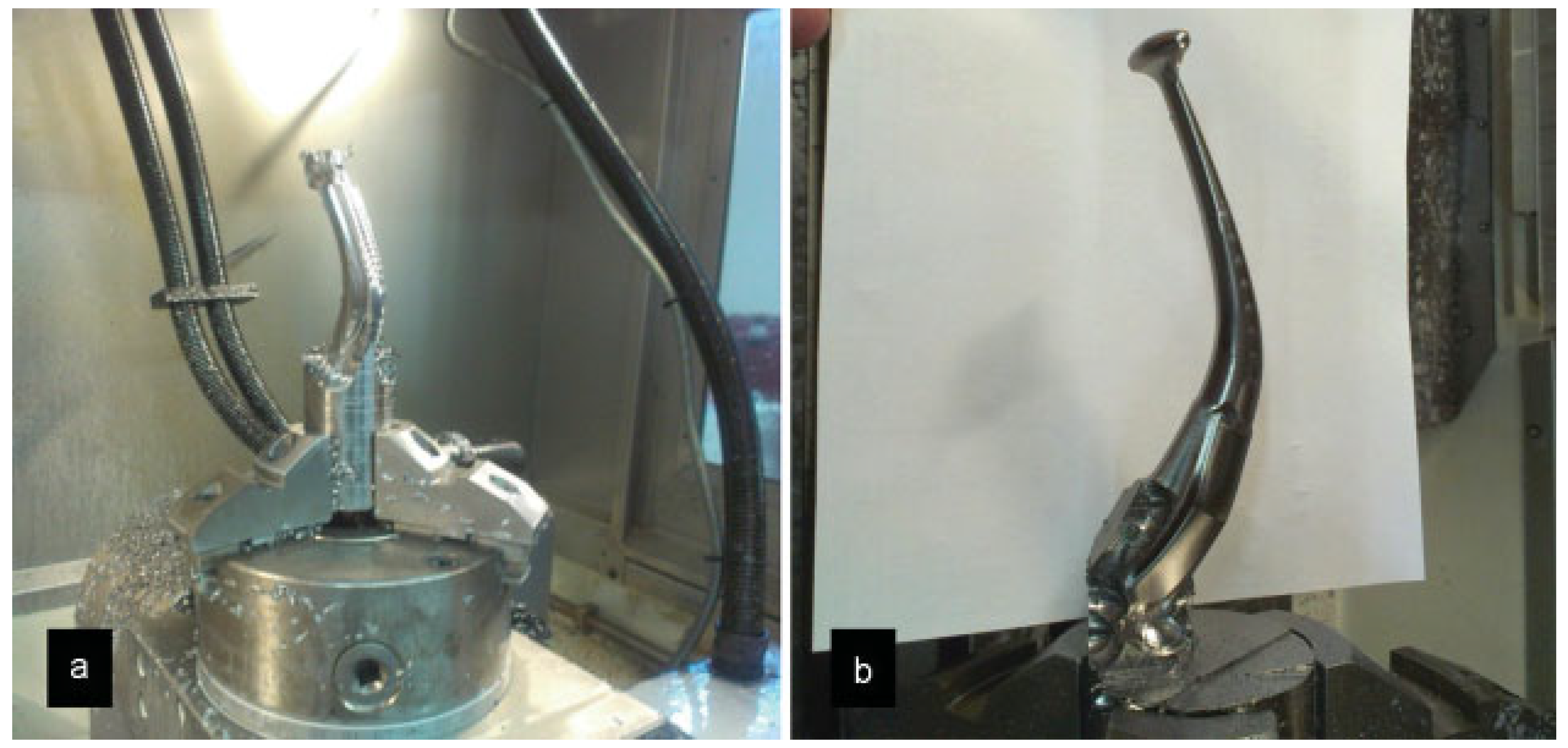
Design Sequence
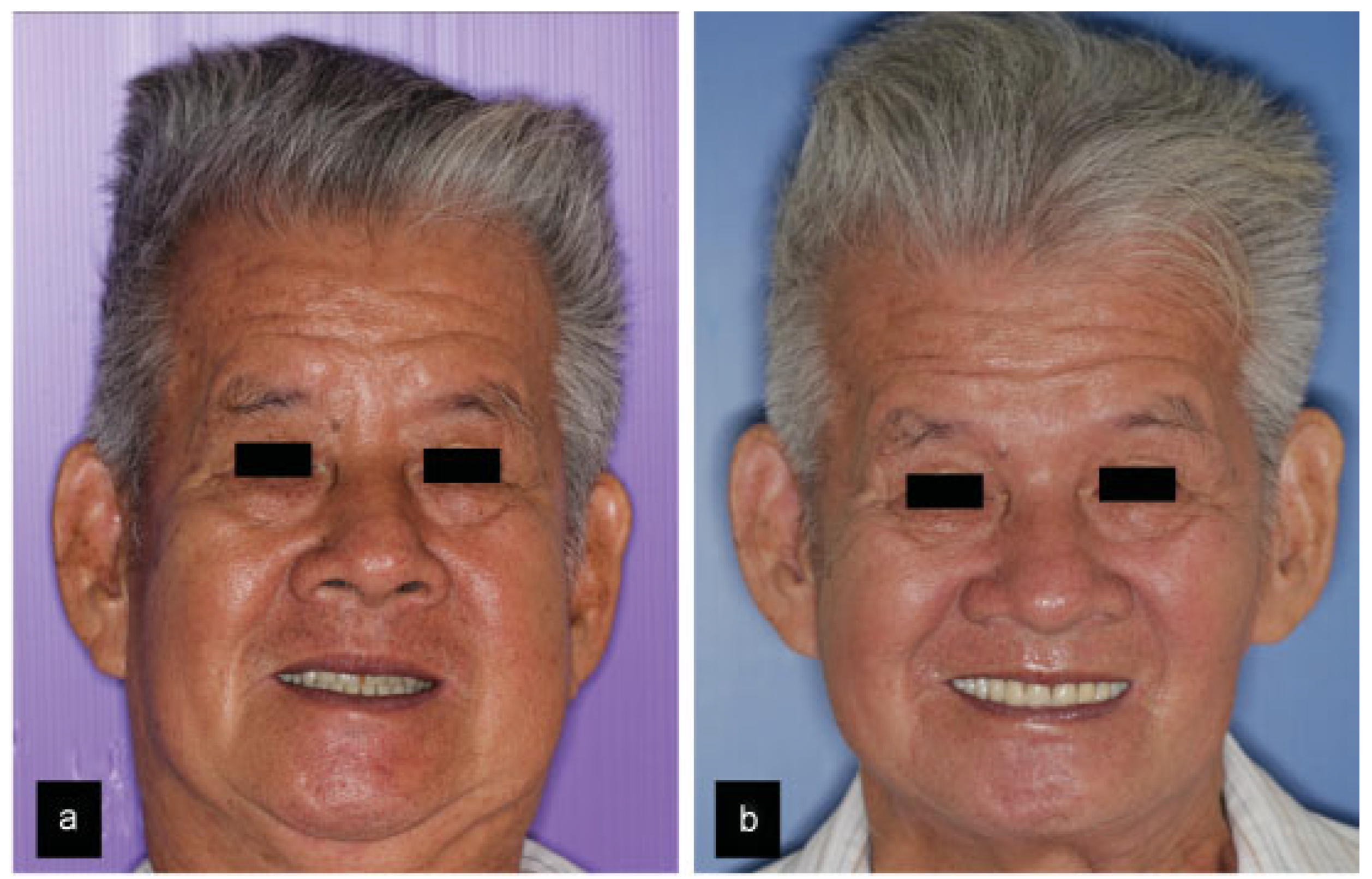
Surgical Sequence
Discussion
Funding
References
- Disa, J.J.; Cordeiro, P.G. Mandible reconstruction with microvascular surgery. Semin Surg Oncol 2000, 19, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Mertens, C.; Decker, C.; Engel, M.; Sander, A.; Hoffmann, J.; Freier, K. Early bone resorption of free microvascular reanastomized bone grafts for mandibular reconstruction—A comparison of iliac crest and fibula grafts. J Craniomaxillofac Surg 2014, 42, e217–e223. [Google Scholar] [CrossRef] [PubMed]
- Handschel, J.; Hassanyar, H.; Depprich, R.A.; et al. Nonvascularized iliac bone grafts for mandibular reconstruction—Requirements and limitations. In Vivo 2011, 25, 795–799. [Google Scholar] [PubMed]
- Magesh, D.P.; Kumaravelu, C.; Maheshwari, G.U. Efficacy of PRP in the reconstruction of mandibular segmental defects using iliac bone grafts. J Maxillofac Oral Surg 2013, 12, 160–167. [Google Scholar] [PubMed]
- Samman, N.; Luk, W.K.; Chow, T.W.; Cheung, L.K.; Tideman, H.; Clark, R.K. Custom-made titanium mandibular reconstruction tray. Aust Dent J 1999, 44, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Tideman, H.; Samman, N.; Cheung, L.K. Functional reconstruction of the mandible: A modified titanium mesh system. Int J Oral Maxillofac Surg 1998, 27, 339–345. [Google Scholar] [PubMed]
- He, Y.; Zhu, H.G.; Zhang, Z.Y.; He, J.; Sader, R. Three-dimensional model simulation and reconstruction of composite total maxillectomy defects with fibula osteomyocutaneous flap flow-through from radial forearm flap. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009, 108, e6–e12. [Google Scholar] [PubMed]
- Hou, J.S.; Chen, M.; Pan, C.B.; et al. Immediate reconstruction of bilateral mandible defects: Management based on computer-aided design/ computer-aided manufacturing rapid prototyping technology in combination with vascularized fibular osteomyocutaneous flap. J Oral Maxillofac Surg 2011, 69, 1792–1797. [Google Scholar] [PubMed]
- Lethaus, B.; Poort, L.; Böckmann, R.; Smeets, R.; Tolba, R.; Kessler, P. Additive manufacturing for microvascular reconstruction of the mandible in 20 patients. J Craniomaxillofac Surg 2012, 40, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Modabber, A.; Legros, C.; Rana, M.; Gerressen, M.; Riediger, D.; Ghassemi, A. Evaluation of computer-assisted jaw reconstruction with free vascularized fibular flap compared to conventional surgery: A clinical pilot study. Int J Med Robot 2012, 8, 215–220. [Google Scholar] [PubMed]
- Rodby, K.A.; Turin, S.; Jacobs, R.J.; et al. Advances in oncologic head and neck reconstruction: Systematic review and future considerations of virtual surgical planning and computer aided design/computer aided modeling. J Plast Reconstr Aesthet Surg 2014, 67, 1171–1185. [Google Scholar] [PubMed]
- Ciocca, L.; Mazzoni, S.; Fantini, M.; et al. A CAD/CAM-prototyped anatomical condylar prosthesis connected to a custom-made bone plate to support a fibula free flap. Med Biol Eng Comput 2012, 50, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Sun, J.; Li, J.; et al. Using computer simulation and stereomodel for accurate mandibular reconstruction with vascularized iliac crest flap. Oral Surg Oral Med Oral Pathol Oral Radiol 2012, 114, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Metzler, P.; Geiger, E.J.; Alcon, A.; Ma, X.; Steinbacher, D.M. Threedimensional virtual surgery accuracy for free fibula mandibular reconstruction: Planned versus actual results. J Oral Maxillofac Surg 2014, 72, 2601–2612. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.B.; Shang, H.T.; He, L.S.; et al. Accurate reconstruction of discontinuous mandible using a reverse engineering/computeraided design/rapid prototyping technique: A preliminary clinical study. J Oral Maxillofac Surg 2010, 68, 2115–2121. [Google Scholar] [CrossRef] [PubMed]


© 2016 by the author. The Author(s) 2016.
Share and Cite
Ow, A.; Tan, W.; Pienkowski, L. Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing. Craniomaxillofac. Trauma Reconstr. 2016, 9, 246-250. https://doi.org/10.1055/s-0036-1581060
Ow A, Tan W, Pienkowski L. Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing. Craniomaxillofacial Trauma & Reconstruction. 2016; 9(3):246-250. https://doi.org/10.1055/s-0036-1581060
Chicago/Turabian StyleOw, Andrew, Winston Tan, and Lukasz Pienkowski. 2016. "Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing" Craniomaxillofacial Trauma & Reconstruction 9, no. 3: 246-250. https://doi.org/10.1055/s-0036-1581060
APA StyleOw, A., Tan, W., & Pienkowski, L. (2016). Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing. Craniomaxillofacial Trauma & Reconstruction, 9(3), 246-250. https://doi.org/10.1055/s-0036-1581060