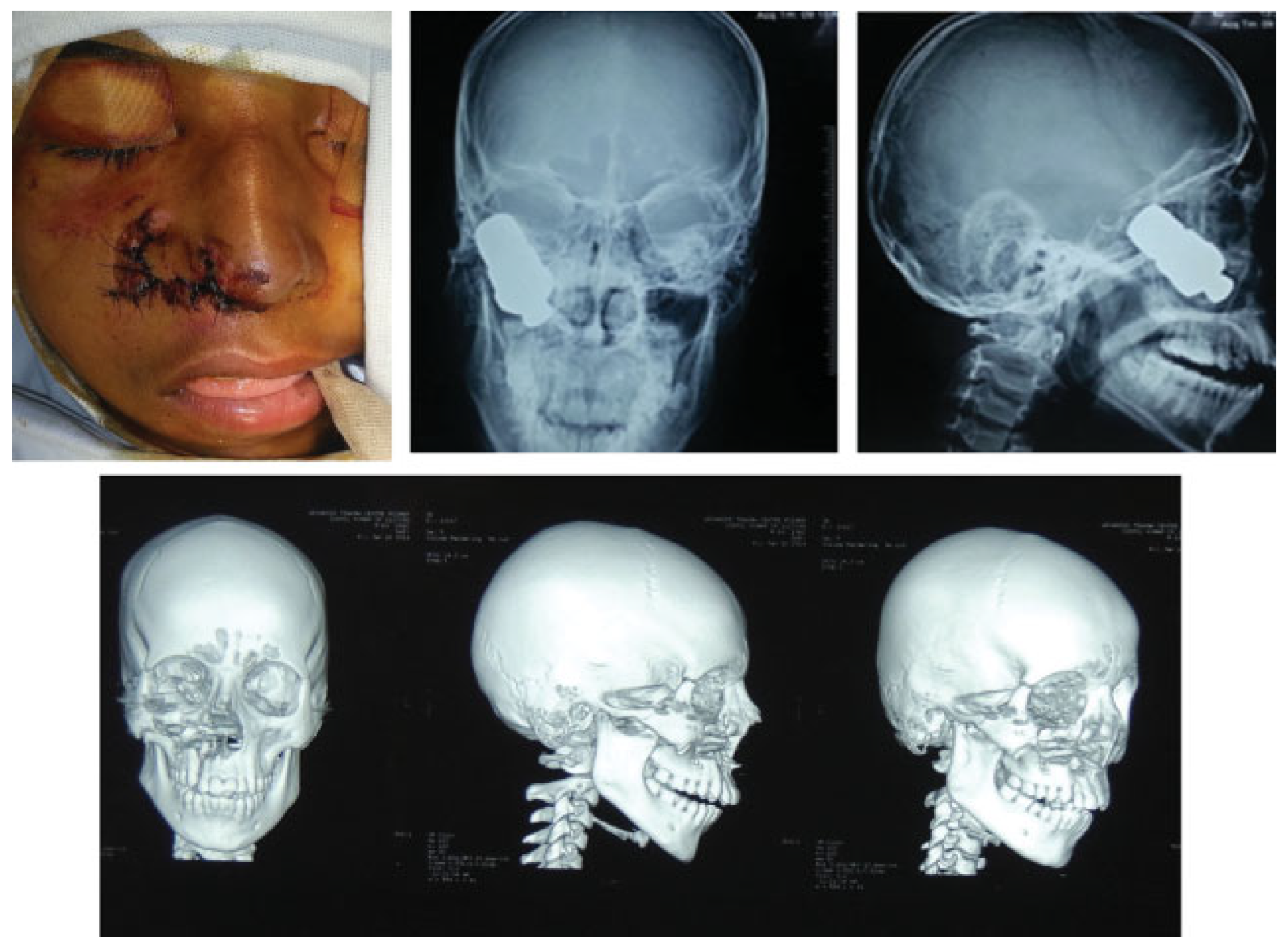
Bolt from the Blue: A Large Foreign Body in the Maxillary Antrum Necessitating Delayed Primary Reconstruction with Split Cranial Bone Graft
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Case Report
Discussion
References
- Jagannathan, M.; Nayak, B.B.; Baliarsing, A.S.; Babu, N.D. An unusual case of orbital trauma with a large foreign body in the maxilla. Br J Plast Surg 1999, 52, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Akdogan, O.; Ozcan, I.; Selcuk, A.; Bilal, N.; Saricaoğlu, S.; Ensari, S. Orbital foreign body penetrating from the cheek. J Craniofac Surg 2008, 19, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Lee, H.Y. A case of retained wooden foreign body in orbit. Korean J Ophthalmol 2002, 16, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Kharel Sitaula, R.; Gautam, V.; Kc, K.; Shah, D.N. Impacted iron nail in the orbit and maxillary sinus through a corneo-scleral perforation: a case report. Nepal J Ophthalmol 2013, 5, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.; Singh, A.; Karthikeyan, A. Unusual foreign body in the maxillary antrum: a case report. The Internet J Otorhinolaryngol 2009, 12, 1–3. [Google Scholar]
- Frodel, J.L. Calvarial bone graft harvesting techniques: considerations for their use with rigid fixation techniques in the craniomaxillofacial region. In Craniomaxillofacial Reconstructive and Corrective Bone Surgery; Greenberg A, Prein J, Ed.; Springer-Verlag: New York, 2002; pp. 700–712. [Google Scholar]
- Elsalanty, M.E.; Genecov, D.G. Bone grafts in craniofacial surgery. Craniomaxillofac Trauma Reconstr 2009, 2, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Tessier, P. Autogenous bone grafts taken from the calvarium for facial and cranial applications. Clin Plast Surg 1982, 9, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.W.; Muschler, G.F. Bone graft materials. An overview of the basic science. Clin Orthop Relat Res 2000, 10–27. [Google Scholar] [CrossRef]
- Hayward, R.D. Cranioplasty: don’t forget the patient’s own bone is cheaper than titanium. Br J Neurosurg 1999, 13, 490–491. [Google Scholar] [CrossRef] [PubMed]



© 2015 by the author. The Author(s) 2015.
Share and Cite
Sharma, R.K.; Vemula, G.K.; John, J.R. Bolt from the Blue: A Large Foreign Body in the Maxillary Antrum Necessitating Delayed Primary Reconstruction with Split Cranial Bone Graft. Craniomaxillofac. Trauma Reconstr. 2016, 9, 242-245. https://doi.org/10.1055/s-0035-1563699
Sharma RK, Vemula GK, John JR. Bolt from the Blue: A Large Foreign Body in the Maxillary Antrum Necessitating Delayed Primary Reconstruction with Split Cranial Bone Graft. Craniomaxillofacial Trauma & Reconstruction. 2016; 9(3):242-245. https://doi.org/10.1055/s-0035-1563699
Chicago/Turabian StyleSharma, Ramesh K., Guru Karna Vemula, and Jerry R. John. 2016. "Bolt from the Blue: A Large Foreign Body in the Maxillary Antrum Necessitating Delayed Primary Reconstruction with Split Cranial Bone Graft" Craniomaxillofacial Trauma & Reconstruction 9, no. 3: 242-245. https://doi.org/10.1055/s-0035-1563699
APA StyleSharma, R. K., Vemula, G. K., & John, J. R. (2016). Bolt from the Blue: A Large Foreign Body in the Maxillary Antrum Necessitating Delayed Primary Reconstruction with Split Cranial Bone Graft. Craniomaxillofacial Trauma & Reconstruction, 9(3), 242-245. https://doi.org/10.1055/s-0035-1563699