Analysis of 1545 Fractures of Facial Region—A Retrospective Study
Abstract
:Materials and Methods
Results
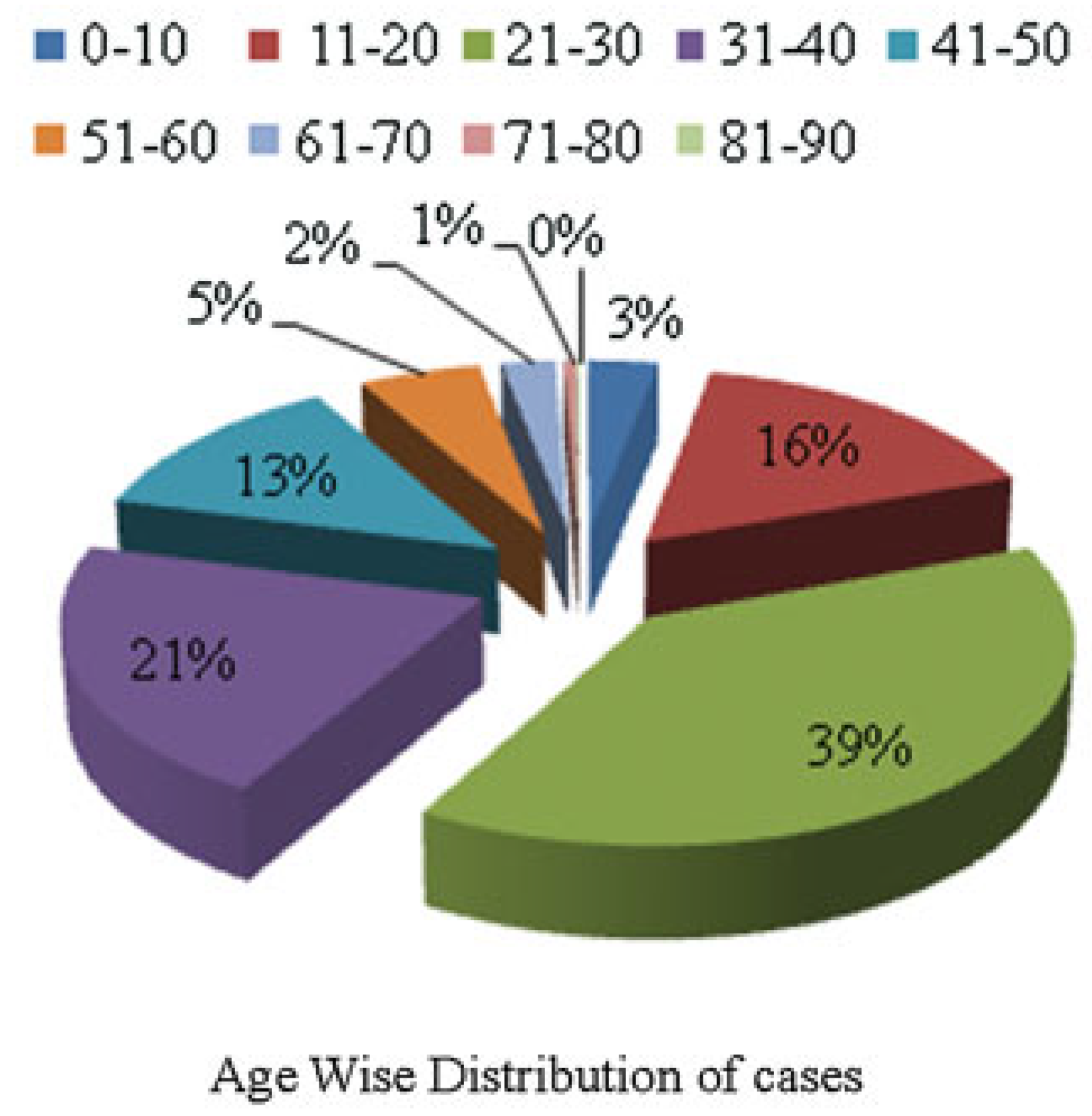
Age Distribution of Fractures
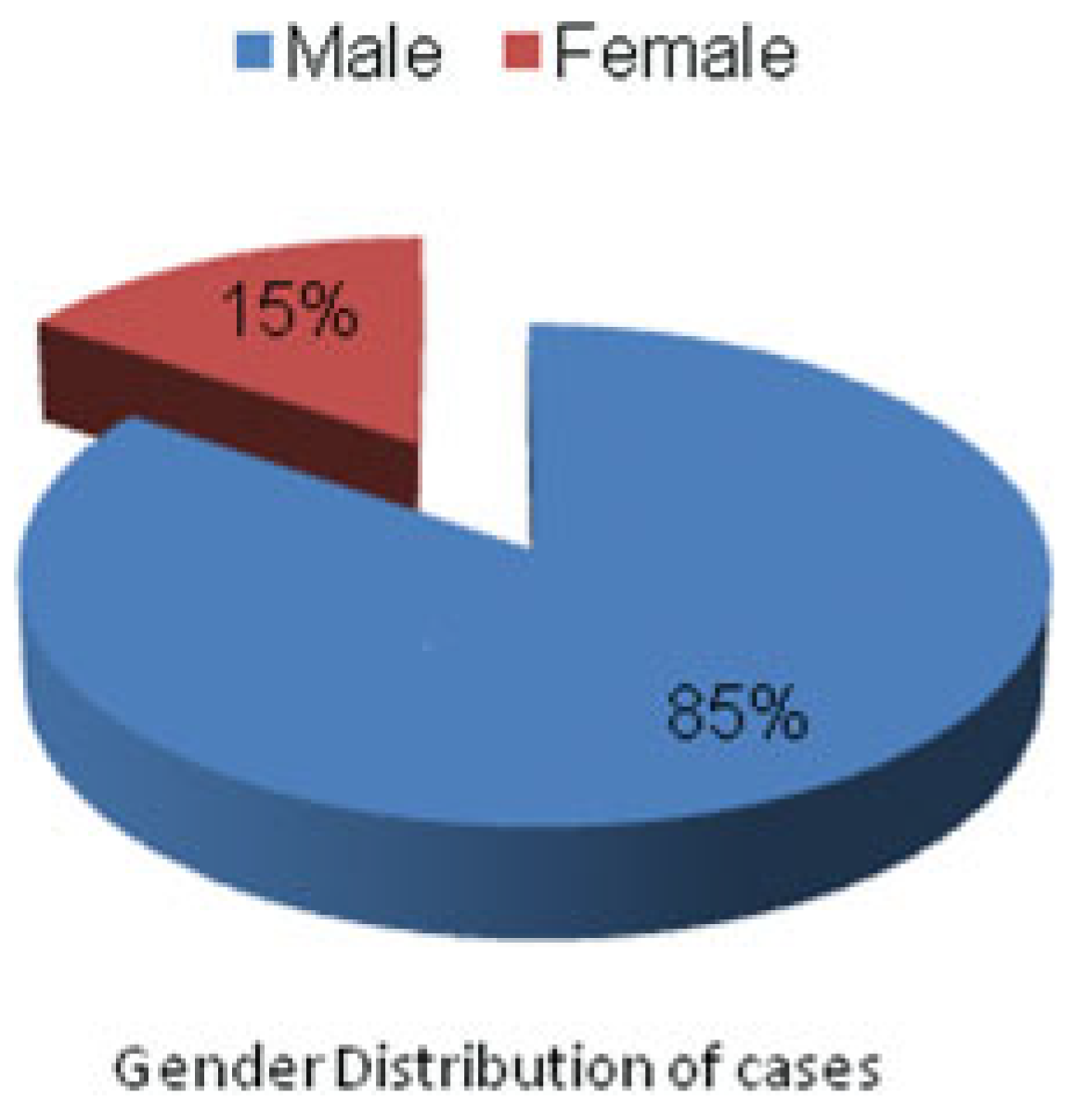
Gender Distribution
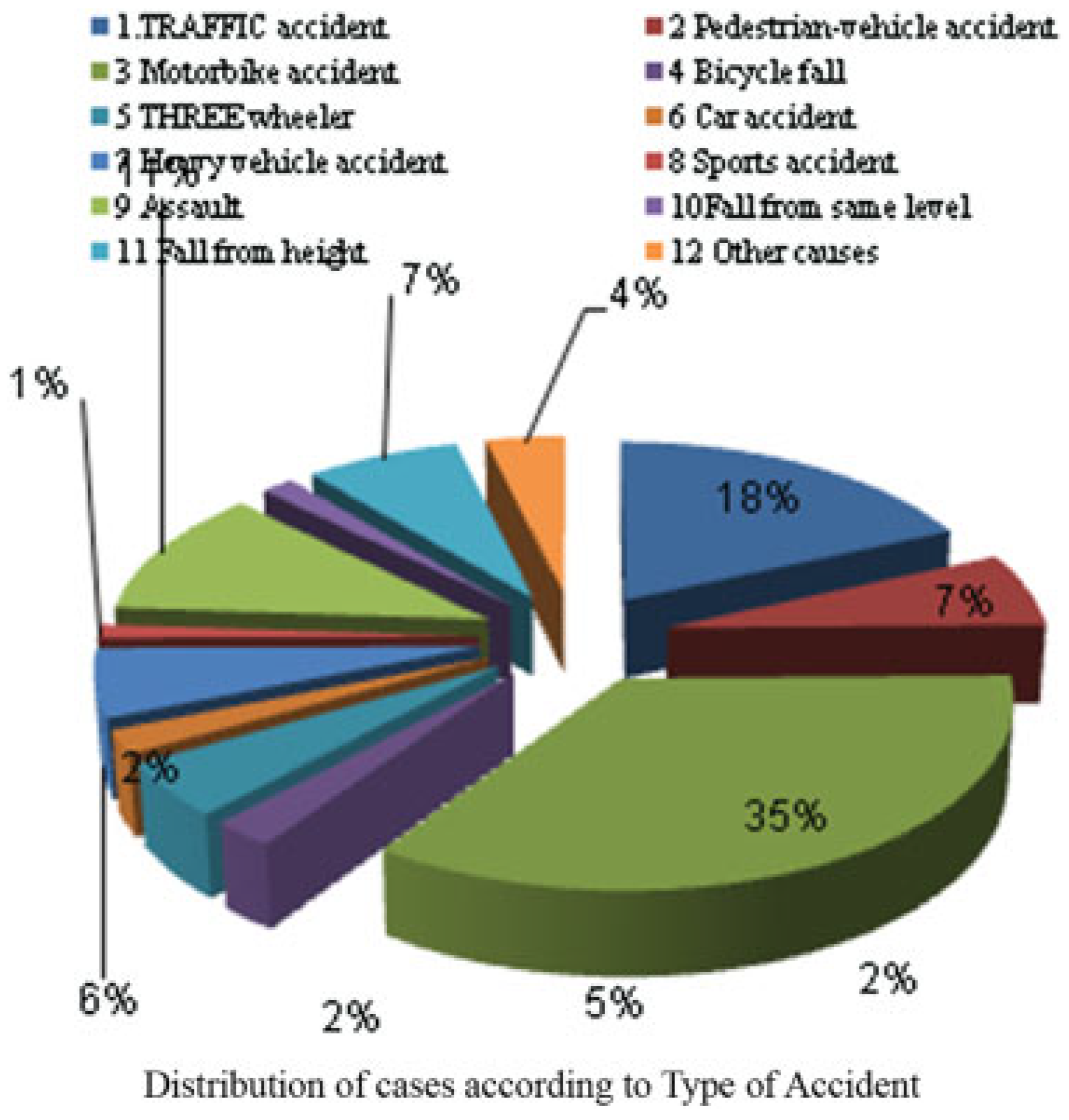
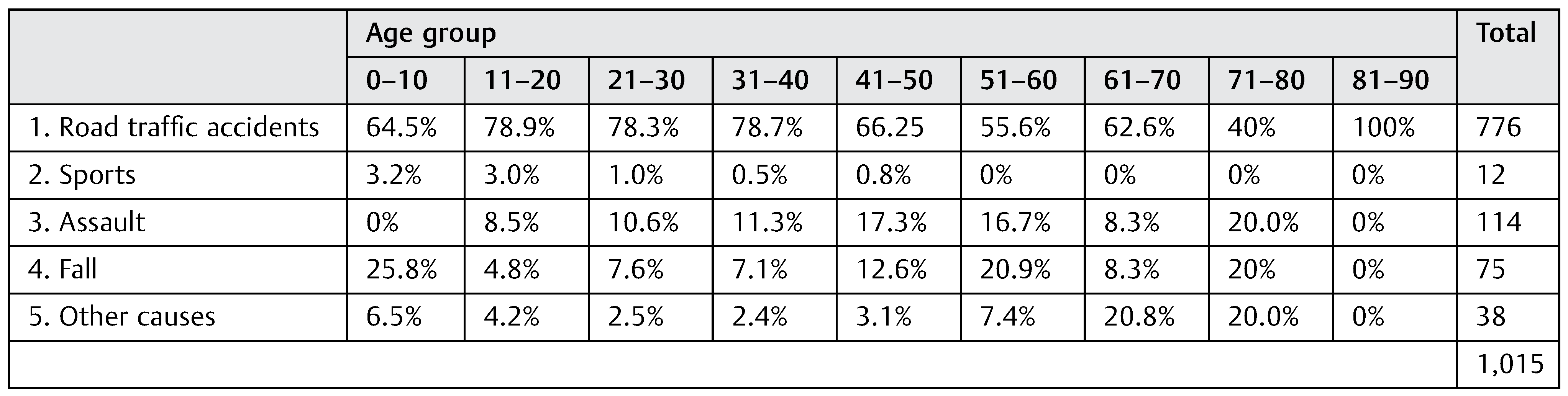
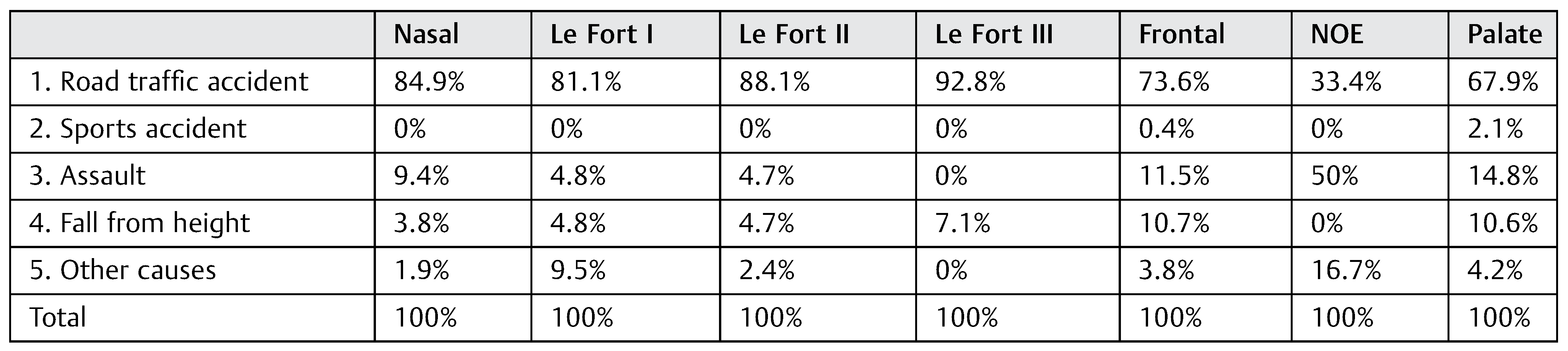
Etiology
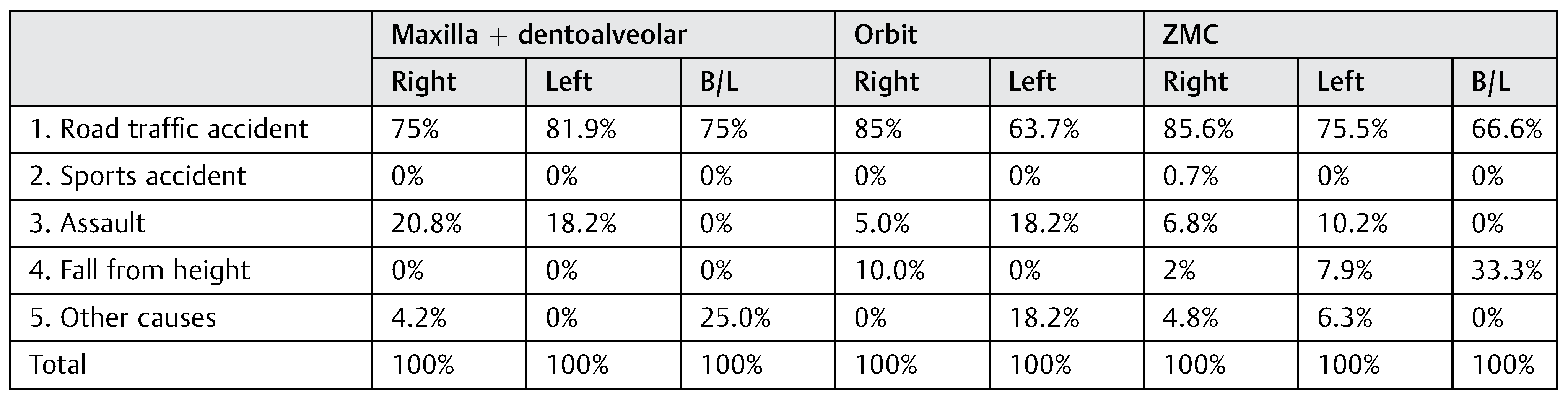
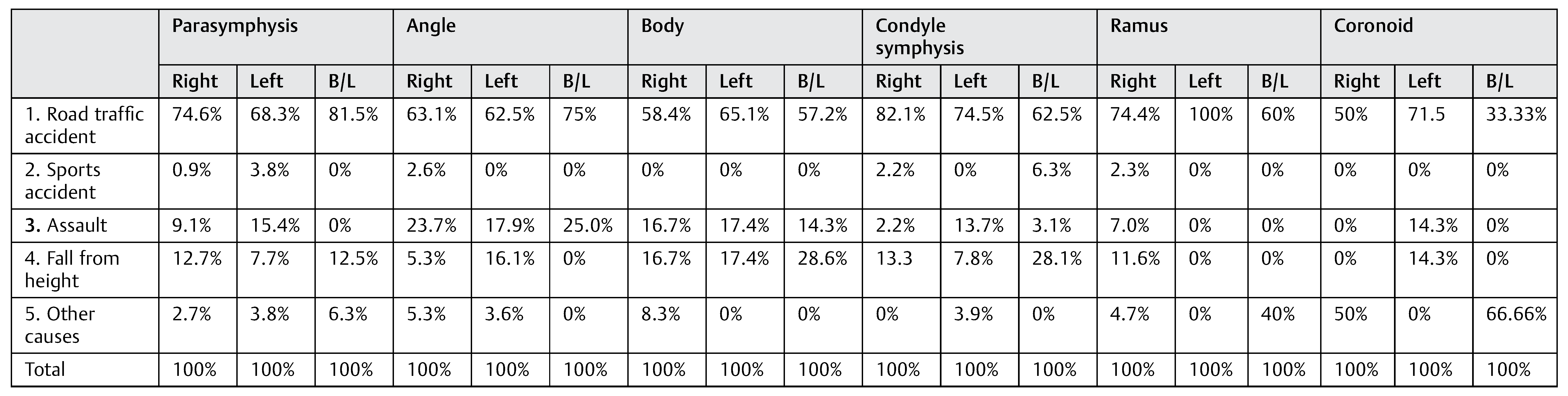
Distribution in Various Trauma Reasons
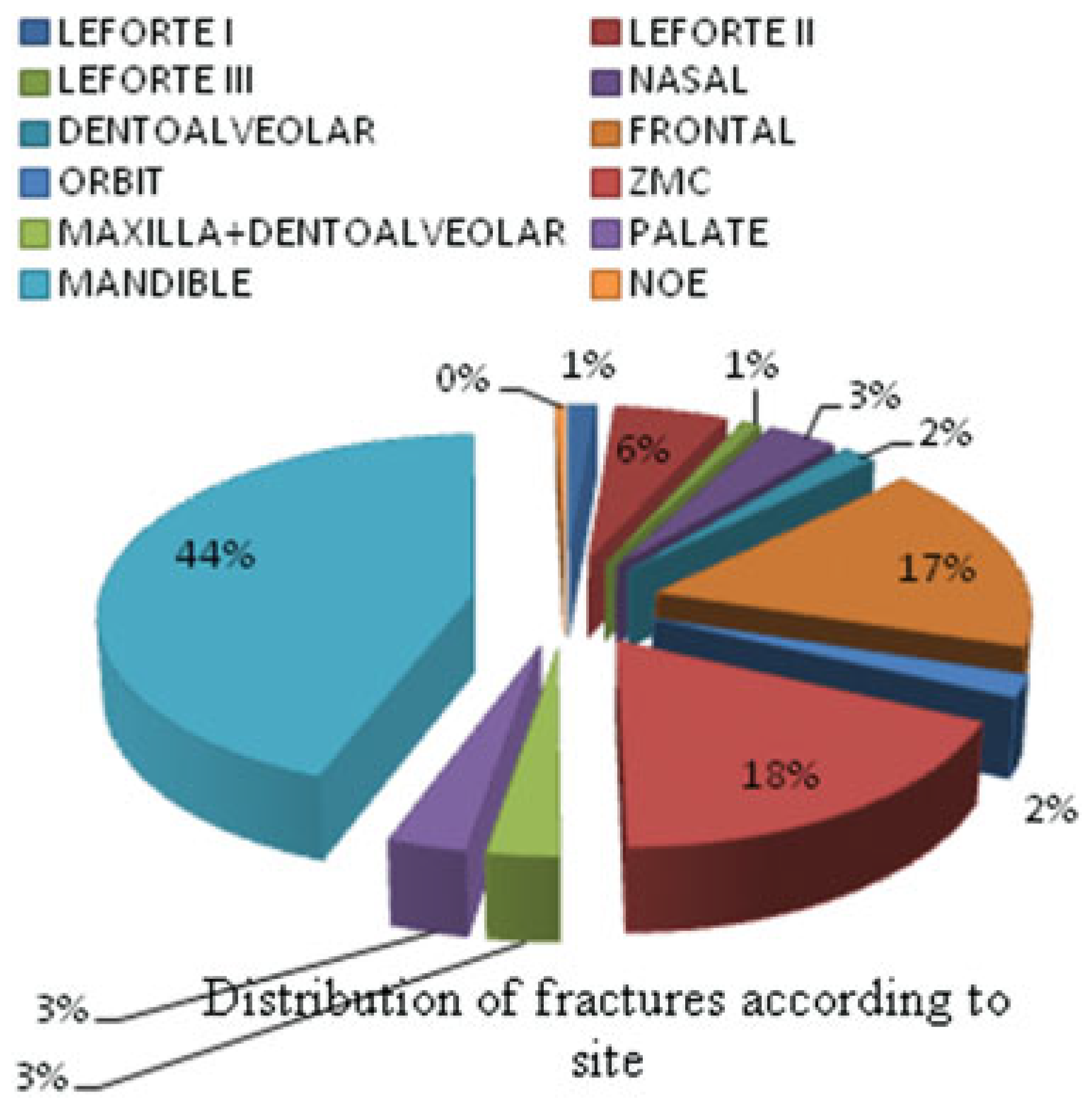
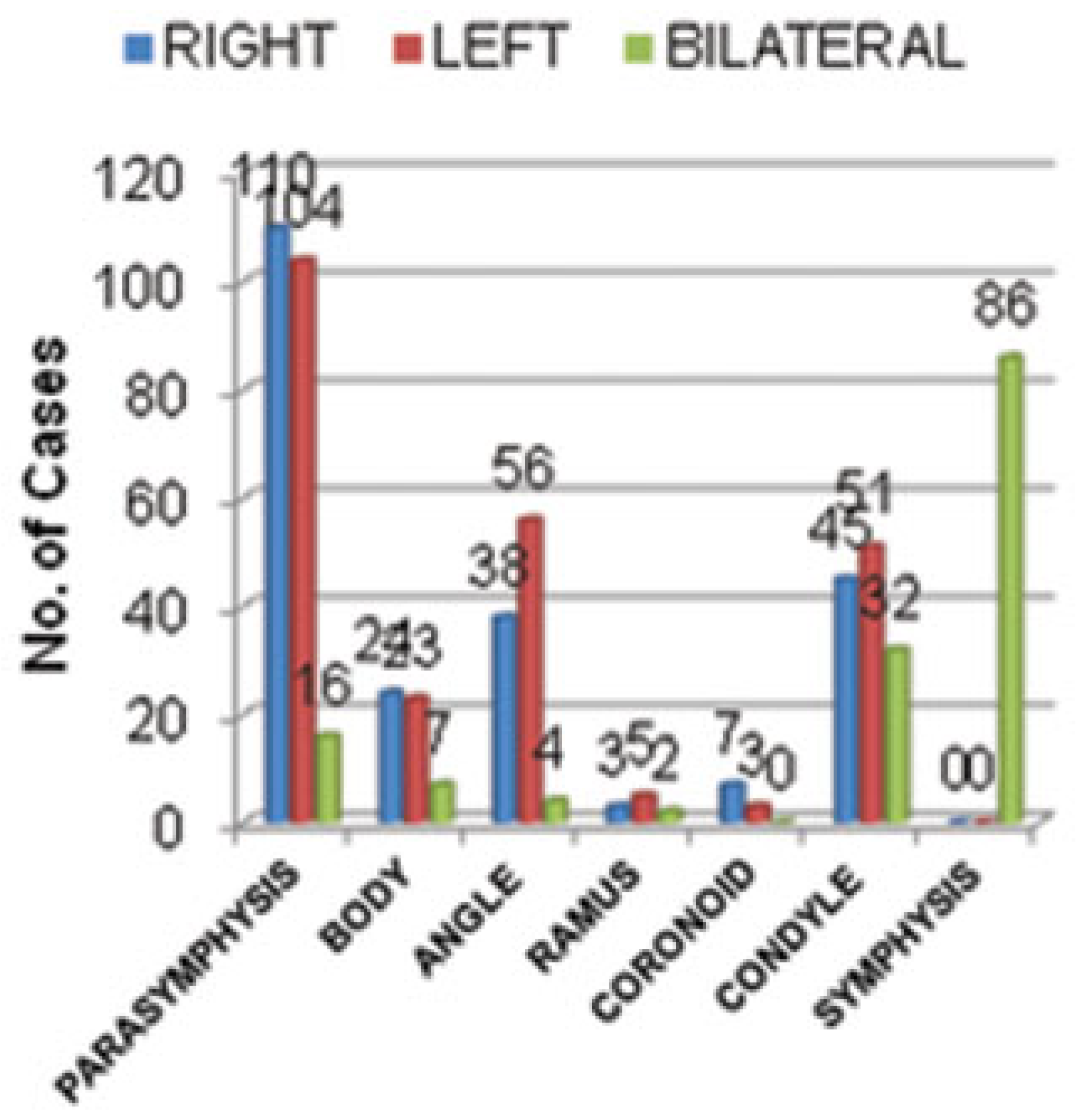
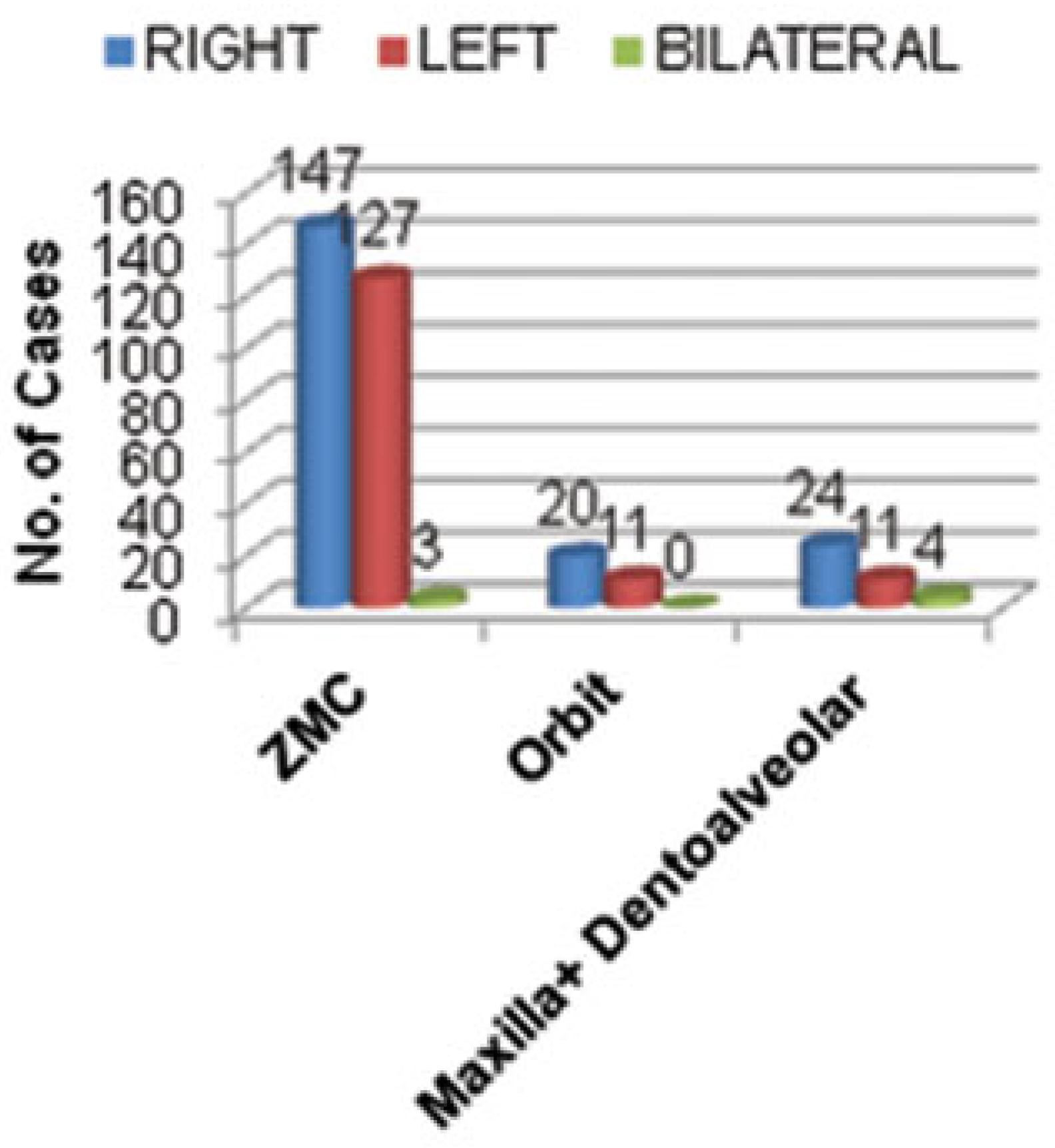
Fracture Site
Soft Tissue Injuries
Discussion
Conclusions
References
- Shayyab, M.; Alsoleihat, F.; Ryalat, S. Trends in the pattern of facial fractures in different countries of the world. Int. J. Morphol. 2012, 30, 745–756. [Google Scholar] [CrossRef]
- Ogundare, B.O.; Bonnick, A.; Bayley, N. Pattern of mandibular fractures in an urban major trauma center. J. Oral. Maxillofac. Surg. 2003, 61, 713–718. [Google Scholar]
- Gassner, R.; Tuli, T.; Hächl, O.; Rudisch, A.; Ulmer, H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J. Craniomaxillofac Surg. 2003, 31, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Girotto, J.A.; MacKenzie, E.; Fowler, C.; Redett, R.; Robertson, B.; Manson, P.N. Long-term physical impairment and functional outcomes after complex facial fractures. Plast. Reconstr. Surg. 2001, 108, 312–327. [Google Scholar]
- Meyer, U.; Benthaus, S.; Du Chesne, A.; Wannhof, H.; Zöllner, B.; Joos, U. Examining patients with facial skull fractures from an etiological and legal perspective. Mund. Kiefer Gesichtschir 1999, 3, 152–157. [Google Scholar] [PubMed]
- Mesgarzadeh, A.H.; Shahamfar, M.; Azar, S.F.; Shahamfar, J. Analysis of the pattern of maxillofacial fractures in north western of Iran: a retrospective study. J. Emerg. Trauma. Shock. 2011, 4, 48–52. [Google Scholar] [CrossRef]
- Ugboko, V.I.; Odusanya, S.A.; Fagade, O.O. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. A review of 442 cases. Int. J. Oral. Maxillofac. Surg. 1998, 27, 286–289. [Google Scholar] [CrossRef]
- Tanaka, N.; Tomitsuka, K.; Shionoya, K.; et al. Aetiology of maxillofacial fracture. Br. J. Oral. Maxillofac. Surg. 1994, 32, 19–23. [Google Scholar] [CrossRef]
- Abiose, B.O. Maxillofacial skeleton injuries in the western states of Nigeria. Br. J. Oral. Maxillofac. Surg. 1986, 24, 31–39. [Google Scholar] [CrossRef]
- Bataineh, A.B. Etiology and incidence of maxillofacial fractures in the north of Jordan. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 1998, 86, 31–35. [Google Scholar]
- Iida, S.; Kogo, M.; Sugiura, T.; Mima, T.; Matsuya, T. Retrospective analysis of 1502 patients with facial fractures. Int. J. Oral. Maxillofac. Surg. 2001, 30, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, T.; Motozawa, Y.; Sasaki, T.; Hitosugi, M. A retrospective analysis of oral and maxillofacial injuries in motor vehicle accidents. J. Oral. Maxillofac. Surg. 2006, 64, 1731–1735. [Google Scholar]
- Elhammali, N.; Bremerich, A.; Rustemeyer, J. Demographical and clinical aspects of sports-related maxillofacial and skull base fractures in hospitalized patients. Int. J. Oral. Maxillofac. Surg. 2010, 39, 857–862. [Google Scholar] [PubMed]
- Allan, B.P.; Daly, C.G. Fractures of the mandible. A 35-year retrospective study. Int. J. Oral. Maxillofac. Surg. 1990, 19, 268–271. [Google Scholar] [PubMed]
- Bakardjiev, A.; Pechalova, P. Maxillofacial fractures in Southern Bulgaria a retrospective study of 1706 cases. J Craniomaxillofac Surg 2007, 35, 147–150. [Google Scholar]
- King, R.E.; Scianna, J.M.; Petruzzelli, G.J. Mandible fracture patterns: a suburban trauma center experience. Am. J. Otolaryngol. 2004, 25, 301–307. [Google Scholar]
- Adebayo, E.T.; Ajike, O.S.; Adekeye, E.O. Analysis of the pattern of maxillofacial fractures in Kaduna, Nigeria. Br. J. Oral. Maxillofac. Surg. 2003, 41, 396–400. [Google Scholar]
- Thorn, J.J.; Møgeltoft, M.; Hansen, P.K. Incidence and aetiological pattern of jaw fractures in Greenland. Int. J. Oral. Maxillofac. Surg. 1986, 15, 372–379. [Google Scholar]
- Güven, O.; Keskin, A. Remodelling following condylar fractures in children. J. Craniomaxillofac Surg. 2001, 29, 232–237. [Google Scholar]
- Zimmermann, C.E.; Troulis, M.J.; Kaban, L.B. Pediatric facial fractures: recent advances in prevention, diagnosis and management. Int. J. Oral. Maxillofac. Surg. 2005, 34, 823–833. [Google Scholar]
- Subhashraj, K.; Nandakumar, N.; Ravindran, C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral Maxillofac Surg 2007, 45, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Iida, S.; Hassfeld, S.; Reuther, T.; et al. Maxillofacial fractures resulting from falls. J. Craniomaxillofac Surg. 2003, 31, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Maliska, M.C.; Lima Júnior, S.M.; Gil, J.N. Analysis of 185 maxillofacial fractures in the state of Santa Catarina, Brazil. Braz. Oral. Res. 2009, 23, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Simsek, S.; Simsek, B.; Abubaker, A.O.; Laskin, D.M. A comparative study of mandibular fractures in the United States and Turkey. Int. J. Oral. Maxillofac. Surg. 2007, 36, 395–397. [Google Scholar] [CrossRef]
- Gopalakrishna, G.; Peek-Asa, C.; Kraus, J.F. Epidemiologic features of facial injuries among motorcyclists. Ann. Emerg. Med. 1998, 32, 425–430. [Google Scholar] [CrossRef]
- McDade, A.M.; McNicol, R.D.; Ward-Booth, P.; Chesworth, J.; Moos, K.F. The aetiology of maxillo-facial injuries, with special reference to the abuse of alcohol. Int. J. Oral. Surg. 1982, 11, 152–155. [Google Scholar] [CrossRef]
- Andersson, L.; Hultin, M.; Nordenram, A.; Ramström, G. Jaw fractures in the county of Stockholm (1978–1980) (I). General survey. Int. J. Oral. Surg. 1984, 13, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.P.; Shapland, M.; Pearce, N.X.; Scully, C. Pattern, severity and aetiology of injuries invictims of assault. J. R. Soc. Med. 1990, 83, 75–78. [Google Scholar] [CrossRef]
- Lee, K.H. Interpersonal violence and facial fractures. J. Oral. Maxillofac. Surg. 2009, 67, 1878–1883. [Google Scholar] [CrossRef]
- Yamamoto, K.; Kuraki, M.; Kurihara, M.; et al. Maxillofacial fractures resulting from falls. J. Oral. Maxillofac. Surg. 2010, 68, 1602–1607. [Google Scholar] [CrossRef]
- Erol, B.; Tanrikulu, R.; Görgün, B. Maxillofacial fractures. Analysis of demographic distribution and treatment in 2901 patients (25-year experience). J Craniomaxillofac Surg 2004, 32, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Paes, J.V.; de Sá Paes, F.L.; Valiati, R.; de Oliveira, M.G.; Pagnoncelli, R.M. Retrospective study of prevalence of face fractures in southern Brazil. Indian. J. Dent. Res. 2012, 23, 80–86. [Google Scholar] [PubMed]
- Marker, P.; Nielsen, A.; Bastian, H.L. Fractures of the mandibular condyle. Part 1: patterns of distribution of types and causes of fractures in 348 patients. Br. J. Oral. Maxillofac. Surg. 2000, 38, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., III; Moos, K.F.; el-Attar, A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral. Surg. Oral. Med. Oral. Pathol. 1985, 59, 120–129. [Google Scholar] [CrossRef]
- Obuekwe, O.N.; Ojo, M.A.; Akpata, O.; Etetafia, M. Maxillofacial trauma due to road traffic accidents in Benin City, Nigeria: a prospective study. Ann. African Med. 2003, 2, 58–63. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
© 2015 by the author. The Author(s) 2015.
Share and Cite
Gaddipati, R.; Ramisetti, S.; Vura, N.; Reddy, K.R.; Nalamolu, B. Analysis of 1545 Fractures of Facial Region—A Retrospective Study. Craniomaxillofac. Trauma Reconstr. 2015, 8, 307-314. https://doi.org/10.1055/s-0035-1549015
Gaddipati R, Ramisetti S, Vura N, Reddy KR, Nalamolu B. Analysis of 1545 Fractures of Facial Region—A Retrospective Study. Craniomaxillofacial Trauma & Reconstruction. 2015; 8(4):307-314. https://doi.org/10.1055/s-0035-1549015
Chicago/Turabian StyleGaddipati, Rajasekhar, Sudhir Ramisetti, Nandagopal Vura, K. Rajiv Reddy, and Bhargav Nalamolu. 2015. "Analysis of 1545 Fractures of Facial Region—A Retrospective Study" Craniomaxillofacial Trauma & Reconstruction 8, no. 4: 307-314. https://doi.org/10.1055/s-0035-1549015
APA StyleGaddipati, R., Ramisetti, S., Vura, N., Reddy, K. R., & Nalamolu, B. (2015). Analysis of 1545 Fractures of Facial Region—A Retrospective Study. Craniomaxillofacial Trauma & Reconstruction, 8(4), 307-314. https://doi.org/10.1055/s-0035-1549015