An Interesting Case of Gunshot Injury to the Temporomandibular Joint
{kind=link}
{kind=link}
{kind=link}
Abstract
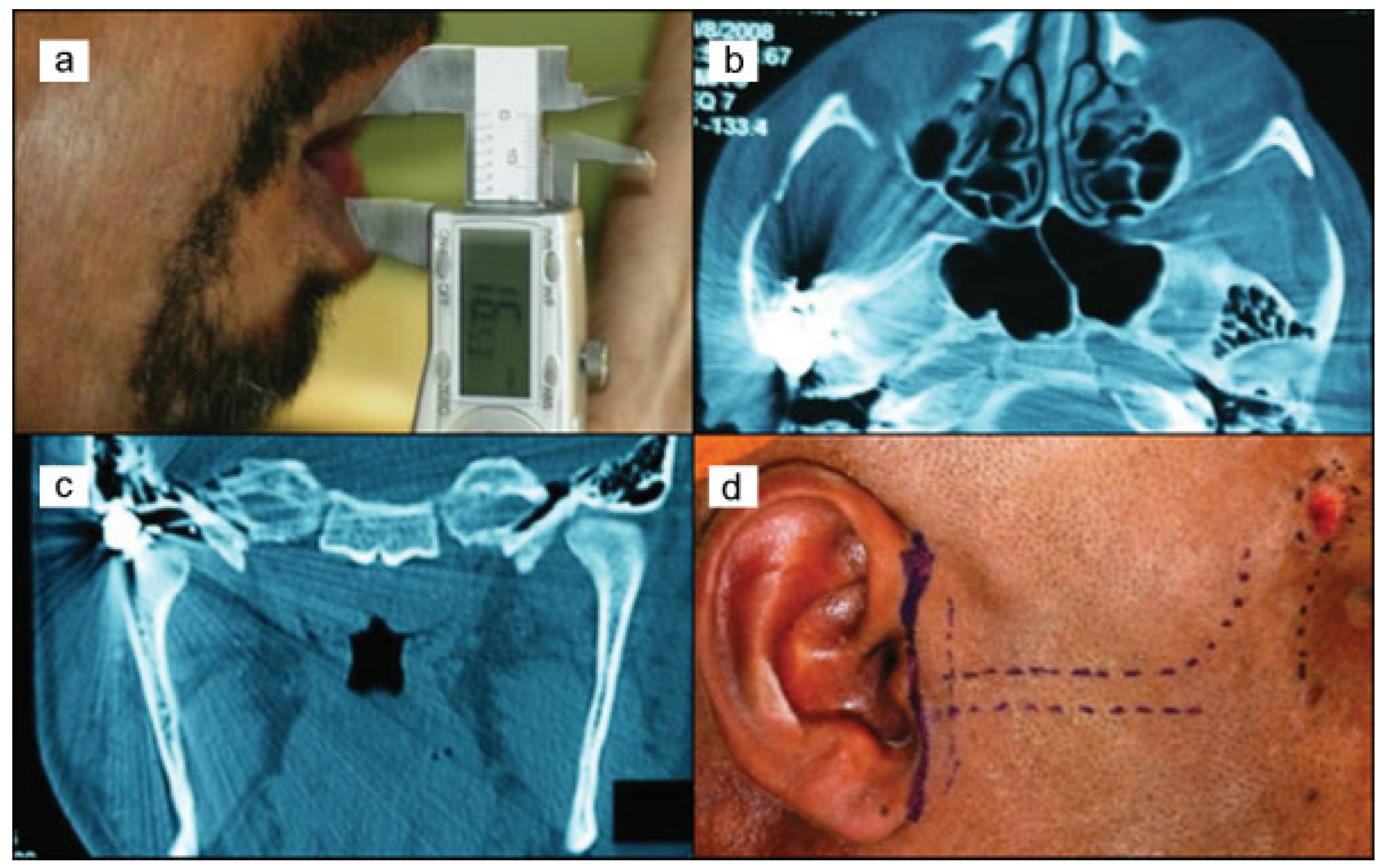
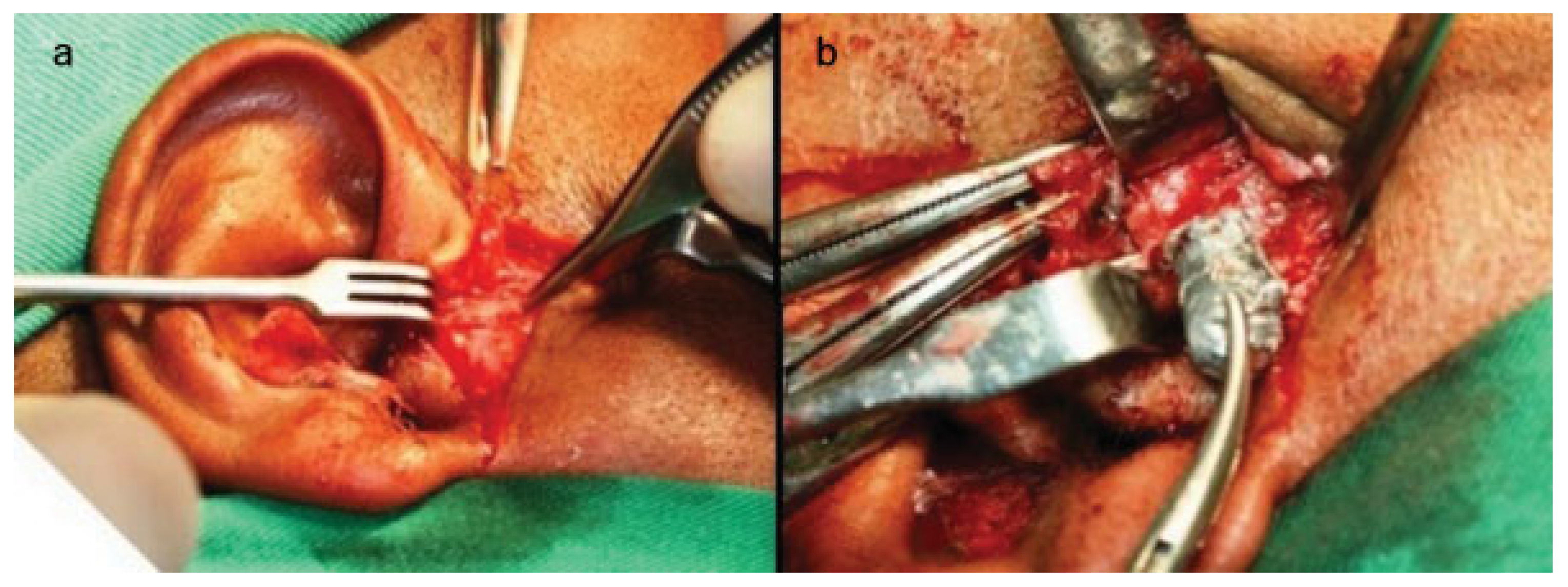
:Case Report
Discussion
Conclusion
References
- Pereira, C.C.S.; Jacob, R.J.; Takahashi, A.; Shinohara, E.H. Mandibular fracture by projectile from a firearm. Rev Cir Traumatol Bucomaxilofac 2006, 6, 39–46. [Google Scholar]
- He, D.; Zhang, Y.; Ellis, E., III. Panfacial fractures: analysis of 33 cases treated late. J Oral Maxillofac Surg 2007, 65, 2459–2465. [Google Scholar] [PubMed]
- Pinna, B.R.; Testa, J.R.G.; Fukuda, Y. Estudo de paralisias faciais traumáticas: análise de casos clínicos e cirúrgicos. Rev Bras Otorrinolaringol (Engl Ed) 2004, 70, 479–482. [Google Scholar] [CrossRef]
- Zachariades, N.; Mezitis, M.; Mourouzis, C.; Papadakis, D.; Spanou, A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment and proposals. J Craniomaxillofac Surg 2006, 34, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., III; Zide, M. Acessos cirúrgicos ao esqueleto facial, 2nd ed.; Santos: São Paulo, 2006; pp. 193–199. [Google Scholar]
- Osborn, D.B.; Bays, R.A. Pathophysiology and management of gunshot wounds to the face. In Oral Maxillofacial trauma; Fonseca, R.W., Ed.; Saunders Co: Philadelphia, 1991; pp. 672–701. [Google Scholar]
- Akhlaghi, F.; Aframian-Farnad, F. Management of maxillofacial injuries in the Iran-Iraq War. J Oral Maxillofac Surg 1997, 55, 927–930, discussion 930–931. [Google Scholar] [PubMed]
- Pena, E.O.; Marzola, C.; Campos, C.R.N.; Toledo Filho, J.L.; Zorzetto, D.L.G.; Pastori, C.M. Tratamento de lesões faciais causadas por armas de fogo – Considerações gerais e apresentação de casos cirúrgicos. Rev Ass Maringaense Odont 2000, 1, 8–18. [Google Scholar]
- Shinohara, E.H.; Shigeto, E.B.; Mitsuda, S.T.; Carvalho Júnior, J.P. Tratamento de fratura mandibular por projétil de arma de fogo. Rev Assoc Paul Cir Dent; Escola de Aperfeiçoamento Profissional: São Paulo, 1999; pp. 363–365. [Google Scholar]
- Hollier, L.; Grantcharova, E.P.; Kattash, M. Facial gunshot wounds: a 4-year experience. J Oral Maxillofac Surg 2001, 59, 277–282. [Google Scholar] [PubMed]
- Holmes, J.D. Decker, B.C., Ed.; Gunshot injuries. In Peterson’s principles of oral and maxillofacial surgery, 2nd ed.; B.C. Decker, 2004; pp. 509–524. [Google Scholar]
- Alper, M.; Totan, S.; Cankayali, R.; Songür, E. Gunshot wounds of the face in attempted suicide patients. J Oral Maxillofac Surg 1998, 56, 930–933, discussion 933–934. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, M.H. Primary management of maxillofacial hard and soft tissue gunshot and shrapnel injuries. J Oral Maxillofac Surg 2003, 61, 1390–1398. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.J.; Ellis, E.E.; Hupp, J.R.; Tucker, M.R. Contemporary oral and maxillofacial surgery, 3nd edMosby: Saint Louis, 2000. [Google Scholar]
- Ellis, H. A history of surgery; Greenwich Medical Media Limited: London, 2001; p. 264. [Google Scholar]
- Ogata, E.; Ono, H.Y.; Leandro, L.F.L. Fraturas mandibulares por projétil de arma de fogo. Rev Internacional de Cirurgia e Traumatologia Bucomaxilofacial; Dental Tribune International: Curitiba, 2003; pp. 212–217. [Google Scholar]
- Demetriades, D.; Chahwan, S.; Gomez, H.; Falabella, A.; Velmahos, G.; Yamashita, D. Initial evaluation and management of gunshot wounds to the face. J Trauma 1998, 45, 39–41. [Google Scholar] [PubMed]
- Cunningham, L.L.; Haug, R.H.; Ford, J. Firearm injuries to the maxillofacial region: an overview of current thoughts regarding demographics, pathophysiology, and management. J Oral Maxillofac Surg 2003, 61, 932–942. [Google Scholar] [PubMed]

© 2014 by the author. The Author(s) 2014.
Share and Cite
Pires, M.S.M.; Giongo, C.C.; de Marco Antonello, G.; do Couto, R.T.; de Oliveira Veras Filho, R.; Junior, O.L.C. An Interesting Case of Gunshot Injury to the Temporomandibular Joint. Craniomaxillofac. Trauma Reconstr. 2015, 8, 79-82. https://doi.org/10.1055/s-0034-1390244
Pires MSM, Giongo CC, de Marco Antonello G, do Couto RT, de Oliveira Veras Filho R, Junior OLC. An Interesting Case of Gunshot Injury to the Temporomandibular Joint. Craniomaxillofacial Trauma & Reconstruction. 2015; 8(1):79-82. https://doi.org/10.1055/s-0034-1390244
Chicago/Turabian StylePires, Mário Sergio Medeiros, Caroline Comis Giongo, Guilherme de Marco Antonello, Ricardo Torres do Couto, Ruy de Oliveira Veras Filho, and Otacílio Luiz Chagas Junior. 2015. "An Interesting Case of Gunshot Injury to the Temporomandibular Joint" Craniomaxillofacial Trauma & Reconstruction 8, no. 1: 79-82. https://doi.org/10.1055/s-0034-1390244
APA StylePires, M. S. M., Giongo, C. C., de Marco Antonello, G., do Couto, R. T., de Oliveira Veras Filho, R., & Junior, O. L. C. (2015). An Interesting Case of Gunshot Injury to the Temporomandibular Joint. Craniomaxillofacial Trauma & Reconstruction, 8(1), 79-82. https://doi.org/10.1055/s-0034-1390244