This edition of Craniomaxillofacial Trauma and Reconstruction contains a special Supplement on the work of Audige, Cornelius, Di Leva, Prein and the AO CMF Classification Committee over a period greater than 10 years. They have authored a Classification scheme for facial fractures which is unique in that it is, like Craniomaxillofacial Trauma and Reconstruction, multispecialty in scope (Oral/Maxillofacial Surgery, Otolaryngology, Plastic and Reconstructive Surgery, Oculoplastic Surgery, Neurosurgery) and International in its inclusion of contributions from all the continents served by the AO Foundation, who sponsored the working group and the publication.
Also unique is the fact that the cranium and skull base are included in the fracture classification, in addition to including the standard areas of the mandible, midface, nose and orbits. Therefore, the classification is unique in three aspects: 1) International in the inclusion of contributions from continents served by the AO Foundation, 2) multispecialty in the recruitment of ideas from five specialties, and 3) geographic in its survey of the entire face, cranium and skull base in its classification.
The past 50 years have seen more progress in facial injury treatment than the past 3000 years, and particularly the use of modern imaging, and the techniques of open reduction, internal fixation and soft tissue replacement have contributed the progress witnessed by all of us fortunate to be interested in this challenging and rewarding discipline.
The AO is more than 55 years old, and was founded by visionary orthopedic pioneers who realized the challenge of trying to introduce a new system of fracture treatment which was opposed by the traditionalists of their day. The AO pioneers (Figure 1) realized that they must have proof of concept, and formulated the strategy of classification, instrumentation, documentation, research (both clinical and experimental) and education (Figure 2) as their method of proving that their proposals were safe, effective and were able to save careers by functional rehabilitation of previously devastating injuries. It did not take long for Veternarians, Craniomaxillofacial and Spine surgeons to realize the use of these concepts in their specialties, and to perceive the application of the concepts in both trauma and reconstructive surgery, and so the modern era of reconstructive facial and cranial surgery was born in the latter portion of the 20th century.
Figure 1.
The founders of the AO foundation, pioneers in orthopedic surgery and open reduction and internal fixation.
Figure 2.
The four “pillars” of the AO Foundation: Documentation, Research, Instrumentation and Teaching, achieved through international cooperation.
The AO pioneers developed concepts now fundamental to the progress achieved in modern medicine by the “Precision Medicine Cycle ” (Figure 3, courtesy of UCSF and Geoff Manley) of taxonomy, which provides for accurate diagnosis, and thereby the institution of targeted treatment, which leads to improved outcomes. Observational studies during the normal course of clinical care then collect “Medicine Based Evidence” which, when combined with Biomedical Research, validates a “Knowledge Network” which refines the taxonomy, creating and initiating a new cycle which constantly improves the entire process.
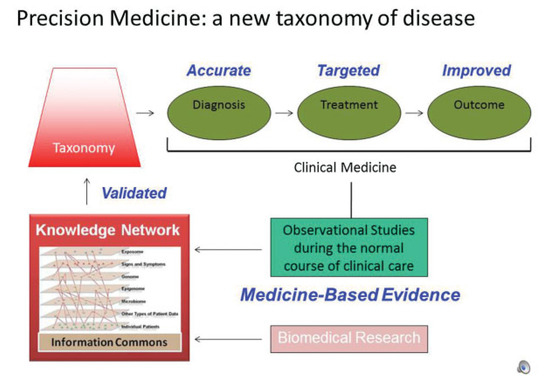
Figure 3.
The Cycle of “Precision Medicine,” courtesy of Geoff Manley and the University of California San Francisco. Taxonomy creates “clinical medicine” programs where accurate diagnosis, and the results of targeted treatment produce improved outcomes. Observational studies of these efforts in the normal course of clinical care create “Medicine Based Evidence”. When combined with Biomedical Research, these data generate a “knowledge network” which refines and improves the taxonomy, thereby improving the results of clinical medicine in a self perpetuating cycle.
Fundamental to the cycle of progress is the Classification of aspects of a particular problem, which creates the “Taxonomy” which allows for stratification of results, and thereby the collection of “Medicine Based Evidence.”
John Mulliken, MD, a Harvard Professor of Surgery at the Peter Bent Brigham Hospital, an individual who has made as many fundamental contributions to modern craniofacial surgery as has anyone, taught me the principles which have resulted in his perception of the ideas he has promulgated. His scientific investigation always begins with classification, the fundamental step in stratifying and collecting meaningful data, which allows the results to be categorized according to clinically useful criteria. Thereby, the results of treatment are able to be compared, best outcomes selected, and medicine is improved consistently by the process.
The steps taken by the authors and their Committee are fundamental in the three aspects described above. They represent an initial contribution in that they establish the taxonomy for a cycle of improvement which will constantly refine the medical and surgical treatment of cranial, skull base and facial fractures. The Classification will now begin to constantly evolve, and be improved by each process, and it is now up to each of us to employ the Classification in our publications, which will permit comparison of results across nations and continents making relevant communication possible.
We are justly proud of the important and detailed work done by the authors and their committee, which is typical of the work sponsored by the AO Foundation whose Mission “is to promote progress designed to foster and expand the network of healthcare professionals in education, research, development and clinical investigation to achieve more effective patient care worldwide.”
© 2014 by the author. The Author(s) 2014.