Abstract
Aim Acceptable facial aesthetics is a common desire among patients presenting with dentofacial deformities planning to undergo orthognathic surgeries. Thus, professionals must be alert to their patients’ complaints as well as their desires regarding facial morphology, because this is quite subjective and personal. This research aimed at evaluating the different views of orthodontists and oral maxillofacial surgeons regarding the facial analysis of patients who undergo orthognathic surgery. Methods Thirty individuals were selected with a minimum postoperative period of 6 months and photographed in the frontal and profile norm. Facial morphology characteristics were recorded to observe the agreement of the assessments of four professionals (two orthodontists and two surgeons). Results A significant agreement was seen between the orthodontists regarding the nasolabial angle (80%). In the frontal analysis, the agreement percentage (60%) between orthodontists and surgeons was considerable regarding facial asymmetry assessment. Conclusions Professionals must keep alert to facial analysis, especially in terms of tegumental harmony, for the orthognathic surgery to reestablish, satisfactorily, the facial aesthetics in all parameters set.
Perception of beauty in the human face is inherent to the knowledge of individuals, with cultural and socioeconomic influences. It brings intense pleasure to the senses and to the intellectual and moral faculties [1].
Several studies have identified the characteristics responsible for pleasant facial aesthetics, which are associated with the harmony and balance among the parts constituting the facial profile [2,3].
Most people seeking dental assistance wish to improve their facial aesthetics and their smile to better integrate in their societies. Thus, the orthodontist must be skilled to recognize the therapeutic goals, individually, so as to reestablish the patients’ facial harmony within their expectations. With the great advances of orthodontics and the classification of malocclusions [4], the identification of dental position alterations has had a remarkable impact on the orthodontic treatment of sagittal and inter- and intra-arches. Thus, through the knowledge of orthodontic limitations, in relation to changes of the facial profile, orthognathic surgery is recommended.
With the advent of orthognathic procedures, the search for facial balance has increased, as well as the need to study aesthetically pleasant faces, both for those presenting with dentofacial deformities to be corrected and those who have already undergone surgery, aiming at reestablishing the harmonious facial characteristics [5]. Thus, a subjective facial analysis must be accomplished, which represents the key to the diagnosis, following the clinical dental exam [6].
The morphological assessment of the face consists, basically, on the observance of parameters by frontal and profile views. The patient is kept in an erect position, looking forward at the horizon line, with a natural head position and a relaxed labial posture [7]. The frontal analysis allows one to notice the facial symmetry, the relation of the lips and labial seal, the proportion of facial structures, as well as the presence of excess or skeletal vertical reduction. For the parameters of patient profile, the facial pattern [7], the pleasantness of the nasolabial angle, the chin-neck line, as well as the labial seal must be observed.
Taking into account that facial harmony is an individual characteristic, this research questioned the differences in relation to the facial analysis of patients who had orthognathic surgery, as regarded by professional orthodontists and oral maxillofacial surgeons who did not know that the patients had undergone such procedures.
The present work aimed at answering the following question: What are the differences, in the view of orthodontists and oral maxillofacial surgeons, regarding facial analysis, in frontal and profile views, of patients who had orthognathic surgery?
Materials and Methods
The research project was approved by the Human Beings Research Ethics Committee. Thirty patients who had undergone orthognathic surgery, with a minimum postoperative period of 6 months, were selected consecutively, corresponding to the period from March 2009 to March 2010 all by the same surgeon. All patients were photographed using the same camera (Nikon® D-40X, Tokyo, Japan). Only one researcher was in charge of the photographic recording; exposures were standardized, with a distance of 1.5 meters from the patient. The images were accomplished in the frontal, profile, and three-quarters aspects, in which the individuals were positioned with the Frankfurt’s plane parallel to the ground, keeping a slightly sealed relaxed lip position, for thorough tegumental analysis. Afterward, the photos were stored and standardized in the Adobe Photoshop CS software (Figure 1 and Figure 2).

Figure 1.
Patient’s image in the frontal aspect.

Figure 2.
Patient’s image in profile.
Two forms were used in the subjective tegumental assessment, with questions on the different characteristics pertaining to a pleasant face, in frontal and profiles analyses (Appendix 1 and Appendix 2).
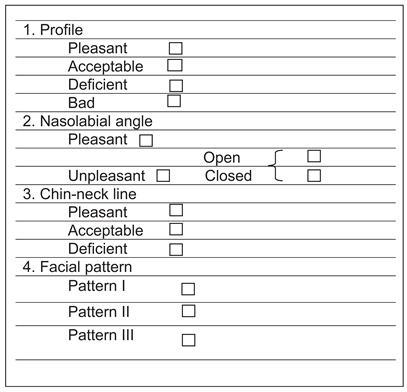
The parameters of a pleasant face consisted of the observation of facial symmetry, correct proportion of facial thirds, good relationship of the lips, soft nasolabial angle, and good mandibular projection.
The same photos (n = 30) were stored in the Microsoft Office PowerPoint 2007 software and displayed in 30 slides, according to the forms (1 to 30). The images were printed in gloss paper and sent to four referees (two professional orthodontists and two oral maxillofacial surgeons) for their assessments, without being told whether or not the patients had undergone orthognathic surgeries.
The data were described by absolute (n) and relative (%) frequencies. Agreement percentage and kappa statistics were used to verify the interevaluators’ agreement, and all calculations were performed in the 13.0 SPSS software. Statistics were used to verify the interevaluators’ frontal and profiles analyses.
Results
The results are shown in the tables. For the main parameters related to perception of facial harmony, see Table 1 and Table 2 for analysis of the facial profile, Table 3 and Table 4 for frontal analysis, and Table 5 and Table 6 for facial symmetry. The other evaluations described previously will be presented throughout the text.

Table 1.
Profile Assessment by the Two Surgeons.
Table 2.
Profile Assessment by the Two Orthodontists.
Table 3.
Frontal Assessment by the Two Surgeons.
Table 4.
Frontal Assessment by the Two Orthodontists.
Table 5.
Symmetry Assessment by the Two Surgeons.
Table 6.
Symmetry Evaluation by the Two Orthodontists.
Profile Analysis
The profile analysis of the 30 individuals involved in this research was classified by the first examiner. Only 1 patient presented a pleasant profile (3.3%), 22 patients presented acceptable profiles (73.35), 6 presented deficient profiles (20%), and 1 had a bad profile (3.3%). Surgeon 2 considered 5 patients to have a pleasant profile (16.7%), 7 to have an acceptable profile (23.3%), 15 to have a deficient profile (50%), and 3 to have a bad profile (3.3%). Thus, the agreement percentage between surgeons in this evaluation was 40% (Table 1).
In relation to facial profile assessment by the orthodontists, the first evaluator classified the profile of 9 patients as pleasant (30%), 15 as acceptable (50%) and 6 as deficient (20%). The second surgeon identified 21 with a pleasant profile (70%), 7 with an acceptable profile (23.3%), and 2 with a deficient facial profile (6.7%). The agreement between them was 36.67% (Table 2).
As for the facial pattern of the individuals studied, surgeon 1 identified 16 patients with facial pattern I (53.3%), 8 with pattern II (26.7%), and 6 with pattern III (20%). On the other hand, the second evaluator classified 30 patients with facial pattern I (30%), 11 with pattern II (36.7%), and 10 with pattern III (33.3%), corresponding to an agreement percentage of 26.67% between the professionals.
As for the facial pattern, orthodontist 1 identified 12 patients with pattern I (40%), 6 with pattern II (20%), and 12 individuals with pattern III (40%). On the other hand, the second evaluator classified 25 patients with facial pattern I (83.3%), 2 with pattern II (6.7%), and 3 with pattern III (10%). Thus, the professionals agreed in only 36.67%.
The nasolabial angle was evaluated by the surgeons, and according to the first evaluator, it was pleasant in 13 individuals (43.3%), 1 patient presented an open angle (3.3%), and 16 presented a closed nasolabial angle (30%). The second surgeon considered 16 patients to have a pleasant nasolabial angle (53.3%), 8 to have an open angle (26.7%), and 6 to have a closed nasolabial angle (20%). The agreement between the professionals was 33.33%.
Orthodontist 1 considered the nasolabial angle as pleasant in 21 patients (70%), open in 1 (3.3%), and closed in 8 (26.7%). The second referee identified 23 patients with a pleasant nasolabial angle (76.7%), 1 with an open angle (3.3%), and 6 individuals with a closed angle (30%). This time, the agreement percentage between these professionals was 80%.
For the distance of the chin-neck line, the first surgeon classified 7 patients with a pleasant line (23.3%), 13 with an acceptable line (43.3%), and 10 with a deficient chin-neck line (33.3%), and surgeon 2 also considered 7 patients to have a pleasant line (23.3%), 9 to have an acceptable line (30%), and 14 to have a deficient chin-neck line (30%). The agreement percentage was 30%.
The chin-neck line was defined as pleasant by the first orthodontist in 10 patients (33.3%), as acceptable in 15 patients (50%), and as deficient in 5 patients (16.7%). However, orthodontist 2 classified 16 individuals with a pleasant chin-neck line (53.3%), 13 with an acceptable line (43.3%), and 1 with a deficient one (3.3%). The agreement between the professionals was 43.33%.
Frontal Analysis
In relation to the frontal aspect, the first surgeon classified 5 patients with a pleasant frontal facial aspect (16.7%), 17 with an acceptable frontal facial aspect (56.7%), 1 with a deficient frontal facial aspect (3.3%), and 7 with a bad frontal facial aspect (23.3%). Surgeon 2, however, considered 4 patients to have a pleasant frontal aspect (13.3%), 14 to have an acceptable frontal aspect (46.7%), 10 to have a deficient frontal aspect (33.3%), and 2 to have a bad frontal aspect (6.7%). The agreement percentage was 40% (Table 3).
In relation to the frontal aspect analysis, orthodontist 1 did not classify any face as pleasant, but classified 23 patients with an acceptable frontal aspect (76.7%) and 7 with a deficient frontal aspect (23.3%). The second evaluator cited 22 patients with a pleasant frontal facial aspect (73.3%), 7 with an acceptable frontal aspect (23.3%), and 1 with a deficient frontal aspect (3.3%). Thus, the agreement percentage was 13.3% between the orthodontists (Table 4).
Facial symmetry was evaluated and surgeon 1 classified 3 patients with asymmetric faces (10%), 6 with vertical excess (20%), 1 with vertical reduction (3.3%), and 20 with symmetric faces (66.7%). The second evaluator classified 10 patients with asymmetric faces (33.3%), 10 with vertical excess (33.33%), 3 with vertical reduction (10%), and 7 with symmetric faces (23.3%). The agreement between these professionals was 33.3% (Table 5).
Assessing the symmetry, orthodontist 1 classified 4 faces as asymmetric (13.3%), 8 as having vertical excess (26.7%), and 18 as symmetric (60%). The second referee considered 3 patients to have asymmetric faces (10%), 2 to have vertical excess (6.7%), and 25 to have symmetric faces (83.3%). The agreement percentage between these professionals was 60% (Table 6).
Discussion
The literature unanimously states that professionals in the fields of orthodontics and oral maxillofacial surgery must be thorough regarding the facial analysis of patients presenting with dentofacial deformities who should be intensively questioned about their complaints, which must corroborate with the professionals’ clinical exams, for the surgical plan to be successful [6,8,9]. This assessment is quite subjective, taking into account the facial harmony and beauty standards imposed by society with its cultural and economic relevances [10]. A statistically significant discrepancy was seen both between the oral maxillofacial surgeons, with an agreement percentage of 40%, and the orthodontists, with a percentage of 36.67% (Table 1 and Table 2), when analyzing the facial profile of the 30 individuals participating in this research. The agreement between the surgeons was maintained in the frontal analysis (40%), and between the orthodontists, the agreement percentage was 13.3% (Table 3 and Table 4).
Still, in this aspect, the surgeries presented good results concerning the facial profile and frontal aspect of the patients, because for most referees of this research, a considerable percentage of the patterns evaluated were classified as acceptable and pleasant. Nevertheless, only surgeon 2 in the facial profile analysis identified 60% of the patients with a deficient or bad profile, which confirms the great divergence of opinions on facial tegumental analysis.
Facial morphology is the most precise resource for the evaluation and diagnosis of facial patterns. Profile views are classified as follows: pattern I, tegumental normality of the face; pattern II, a convex profile; and pattern III, a concave profile [5,7]. In the present work, the professionals did not obtain considerable agreement, which was only 26.67% between the surgeons and 36.67% between the orthodontists, denoting the great discrepancy among the professionals as far as facial profile classification is concerned. Only a surgeon and an orthodontist identified most pattern I patients; the other professionals classified most pattern II and III patients. Thus, it is extremely important that patients be thoroughly evaluated for the surgical plan to provide a harmonious face postoperatively.
Another essential point to be assessed in the facial profile of patients is the nasolabial angle, intimately related to upper lip projection and reflecting the position of upper incisors and the thickness of the soft tissue that covers the teeth. This angle may be altered, perceptively, with orthodontic and surgical procedures that modify the anteroposterior position or tipping of the frontal teeth in the maxilla [8,11]. It is a consensus among authors that the dental discompensation of anterosuperior teeth as well as the surgical movement of the maxilla possess a certain degree of limitation. Thus, depending on this limitation, with the surgical procedure many times the nasolabial angle might not be within normal standards, remaining open or closed, a fact that justified the results accomplished in this work, with an agreement rate of 33.33% between the surgeons and 80% between the orthodontists in this study. Furthermore, a judgment constancy was not seen among the evaluators.
A generally observed peculiarity in patients with mandibular horizontal excess is the increase in the distance of the neck junction up to the mentum (chin-neck line). On the other hand, in the mandible’s horizontal deficiencies, this line is reduced, thus this distance should be considered in physical exams, because the planning is crucial for the decision of mandibular movements and for a satisfactory postoperative result [6,12,13]. Therefore, in this research, the patients were considered to have a pleasant or acceptable chin-neck distance in more than 50% among the two groups of referees; however, a great agreement difference was seen between the surgeons (30%) and the orthodontists (43.33%).
Facial symmetry is a very important aspect for individuals presenting with dentofacial deformities, mainly because in cases of asymmetry, they suffer a great psychological impact, showing, in many cases, a deficit in their learning process and in their daily lives [14,15,16]. Quite frequently, the upper labial filter is a reliable midline structure for facial symmetry evaluation. A vertical line is traced through the middle point of the filter and the middle dental and skeletal lines are assessed. In addition, the face may present a vertical excess or reduction compared by the proportions of the facial thirds [6,15]. In this study, only surgeon 2 classified 23.3% of the patients evaluated as having symmetric faces. The other professionals classified most individuals to have symmetric faces (Table 5 and Table 6). This highlights the importance of facial analysis and the correction of asymmetries and vertical alterations of the thirds, for facial harmony to be accomplished through orthognathic surgeries, boosting the patient’s self-esteem.
Therefore, this disagreement shows that facial analysis is rather subjective and personal and above all influenced by community characteristics. Moreover, for the aesthetic and functional result of orthognathic surgeries to be accomplished, the professionals involved must be thorough while examining the patients, thus performing a satisfactory surgical plan.
Appendix 1. Form for Frontal Facial Analysis
| frontal aspect |
| Pleasant □ |
| Acceptable □ |
| Deficient □ |
| Bad □ |
| frontal aspect |
| Symmetric □ |
| Asymmetric □ |
| Vertical excess □ |
| Vertical reduction □ |
Appendix 2. Form for Facial Profile Analysis
References
- Giddon, D.B. Aplicações ortodônticas de estudos psicológicos e perceptuais da estética facial. In Atualidades em Ortodontia; Sadowsky, P.L., Peck, S., King, G., Eds.; Premier: São Paulo, Brazil, 1997. [Google Scholar]
- Herzberg, B.L. Facial esthetics in relation to orthodontics treatment. Angle Orthod 1952, 22, 3–22. [Google Scholar]
- Brons, R. Facial Harmony: Standards for Orthognathic Surgery and Orthodontics; Quintessence: London, UK, 1998. [Google Scholar]
- Angle, E.H. Classification of malocclusion. Dent Cosmos. 1899, 41, 248–265. [Google Scholar]
- Braga Reis, S.A.; Abrão, J.; Capelozza Filho, L.; Claro, C.A.A. Estudo comparativo do perfil facial de indivíduos Padrões I, II e III portadores de selamento labial passivo. Rev Dent Press Ortodon Ortop Facial 2006, 11, 36–45. [Google Scholar]
- Suguino, R.; Ramos, Q.L.; Terada, H.B. Análise facial. Rev Dent Press Ortodon Ortop Facial 1996, 1, 87–105. [Google Scholar]
- Capelozza Filho, L. Diagnóstico em Ortodontia; Dent Press: Maringá,, 2004. [Google Scholar]
- Arnett, W.G.; McLaughlin, R.P. Planejamento facial e dentário para ortodontistas e cirurgiões bucomaxilofaciais; Artes Médicas: São Paulo, Brazil, 2004. [Google Scholar]
- Braga Reis, S.A.; Capelozza Filho, L.; Claro, C.A.A. Análise facial subjetiva. Rev Dent Press Ortodon Ortop Facial 2006, 11, 159–172. [Google Scholar] [CrossRef]
- Sarver, D.; Jacobson, R.S. The aesthetic dentofacial analysis. Clin Plast Surg 2007, 34, 369–394. [Google Scholar] [CrossRef] [PubMed]
- Sarver, D.M. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop 2001, 120, 98–111. [Google Scholar] [PubMed]
- Sarver, D.M.; Johnston, M.W. Orthognathic surgery and aesthetics: planning treatment to achieve functional and aesthetic goals. Br J Orthod 1993, 20, 93–100. [Google Scholar] [PubMed]
- Sarver, D.M. Esthetic Orthodontics and Orthognathic Surgery; CV Mosby Co.: St. Louis, MO, 1997. [Google Scholar]
- Bell, W.H.; Proffit, W.P.; White, R.P. Surgical Correction of Dentofacial Deformities; W. B. Saunders Co.: Philadelphia, PA, 1980; Volume 1. [Google Scholar]
- Goiato, M.C.; Nicolau, E.I.; Mazaro, J.V.Q.; et al. Mobility, aesthetic, implants, and satisfaction of the ocular prostheses wearers. J Craniofac Surg 2010, 21, 160–164. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, D.M.; Goiato, M.C.; Pesqueira, A.A.; et al. Prosthesis auricular with osseointegrated implants and quality of life. J Craniofac Surg 2010, 21, 94–96. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2013 by the author. The Author(s) 2013.