Two Miniplates Versus Three Dimensional Plate in Management of Mandibular Condylar Fractures: A Systematic Review and Meta-Analysis

Abstract
Introduction
Methodology
Search Strategy
Translations
Study Selection
Inclusion and Exclusion Criteria
Data Extraction
Data Synthesis and Meta-Analysis
Heterogeneity Assessment
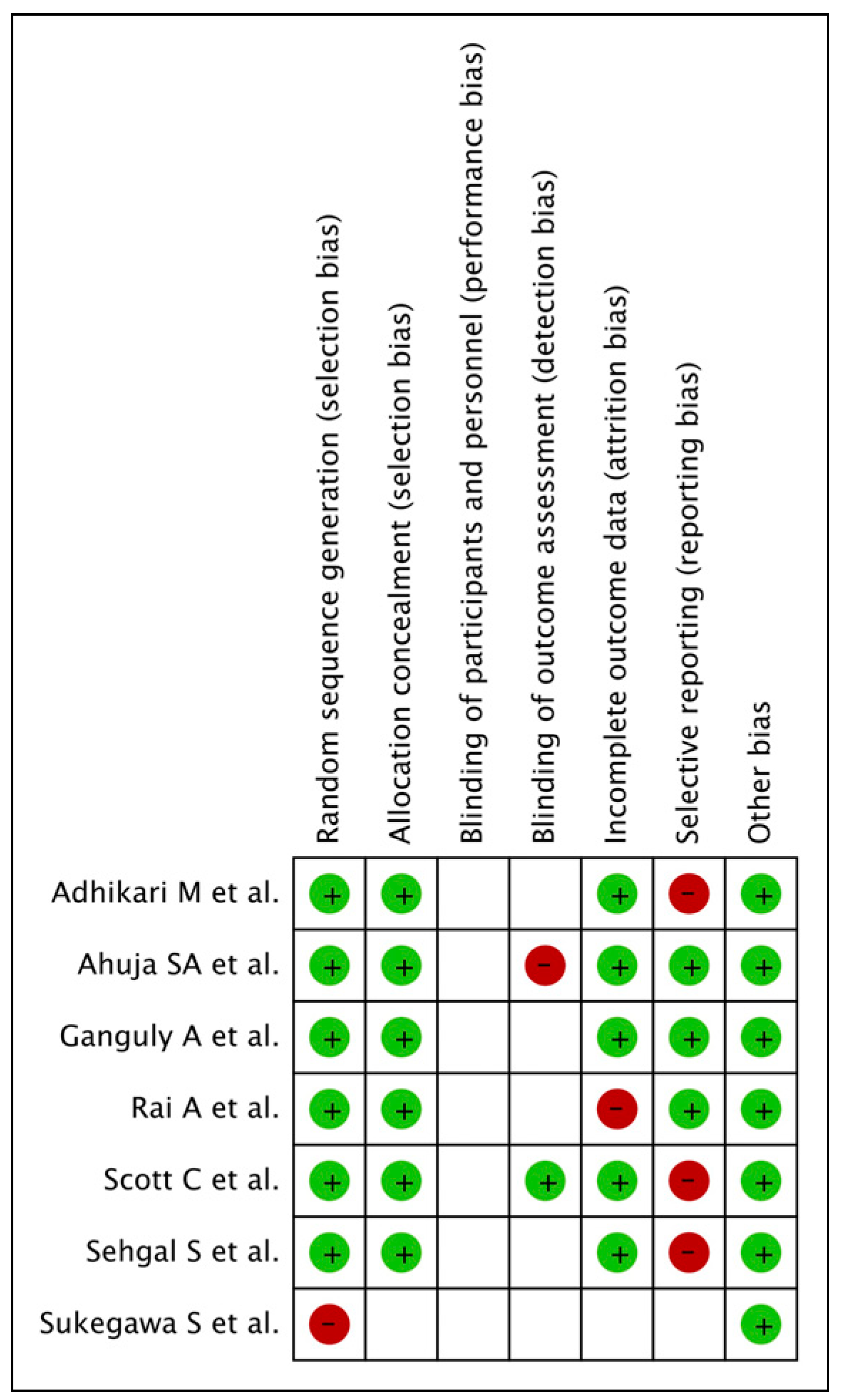
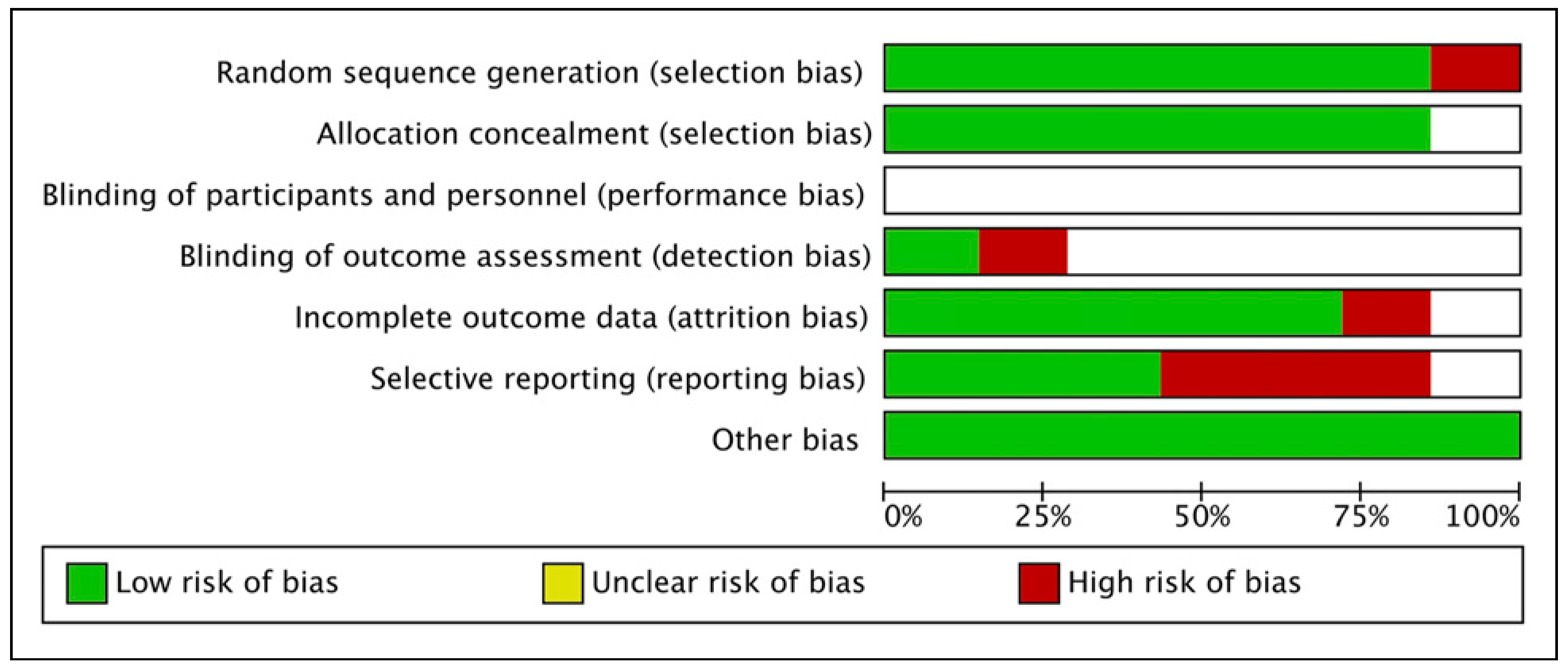
Risk of Bias Assessment
Results
Search Results
Characteristics of Included Studies
Results Pertaining to Various Parameters Assessed
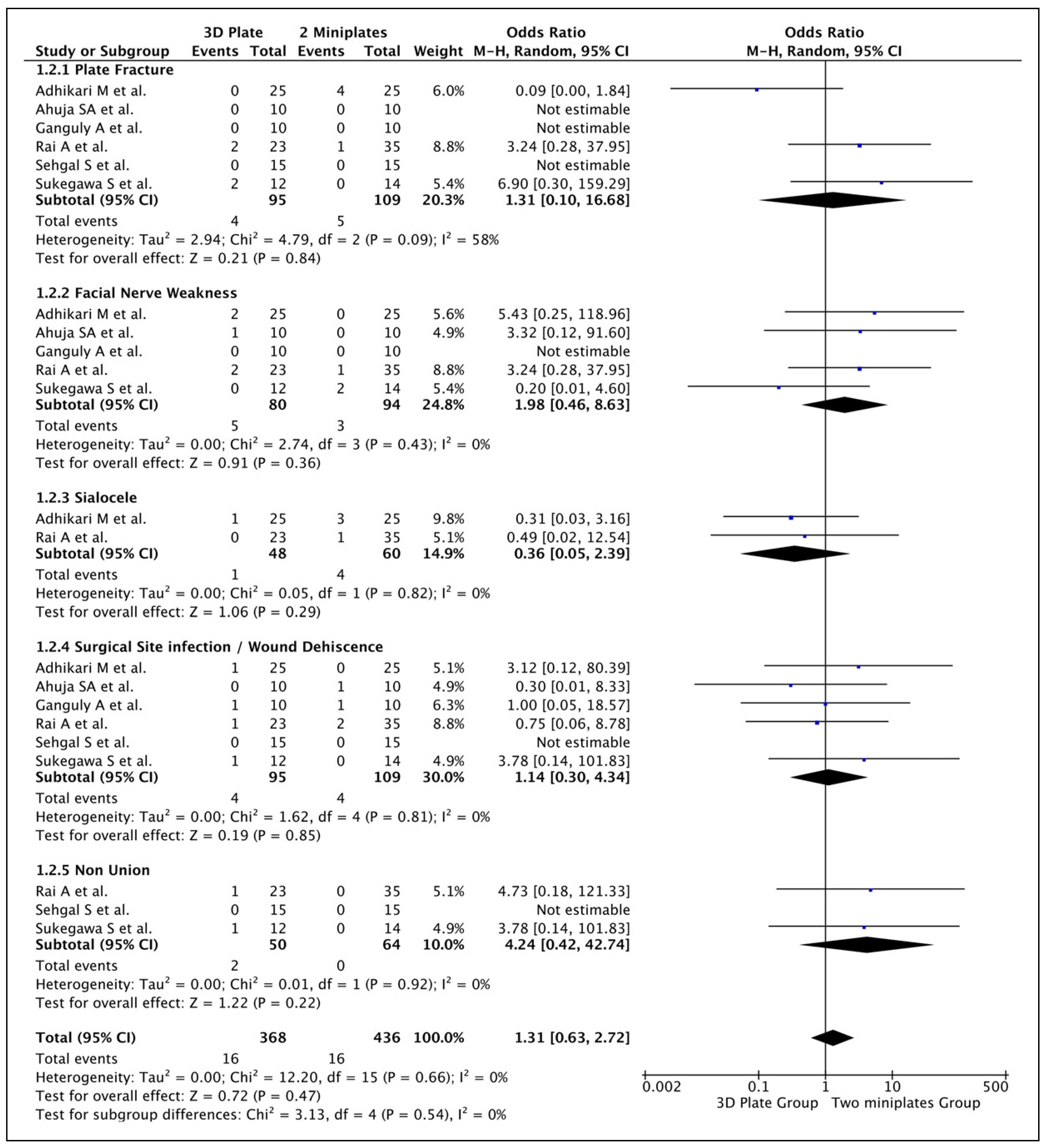
Meta-Analysis Results
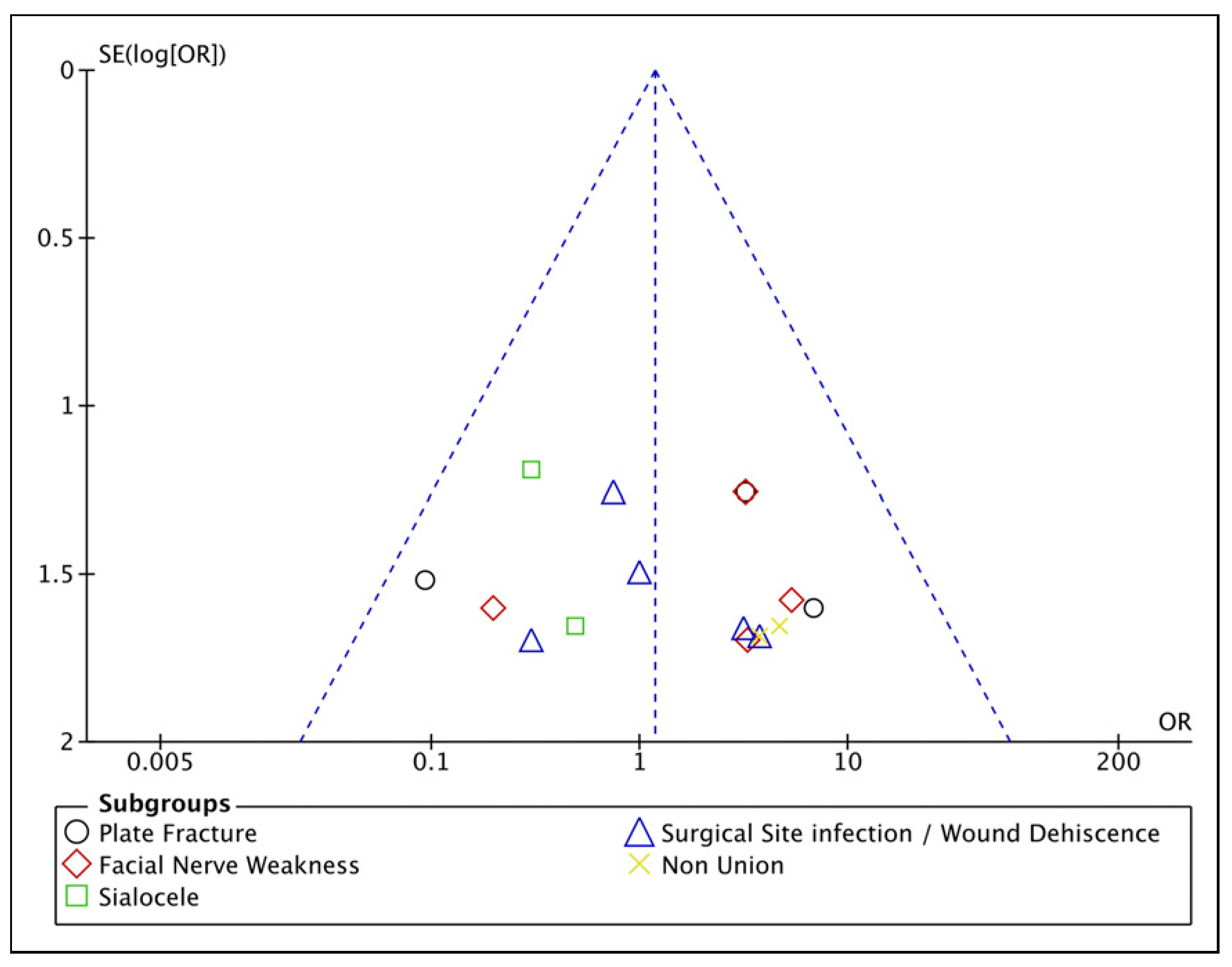
Risk of Bias Assessment
Discussion
Conclusion
Funding
Conflicts of Interest
References
- Stacey, D.H.; Doyle, J.F.; Mount, D.L.; Snyder, M.C.; Gutowski, K.A. Management of mandible fractures. Plast Reconstr Surg. 2006, 117, 48e–60e. [Google Scholar] [CrossRef]
- Morris, C.; Bebeau, N.P.; Brockhoff, H.; Tandon, R.; Tiwana, P. Mandibular fractures: an analysis of the epidemiology and patterns of injury in 4,143 fractures. J Oral Maxillofac Surg. 2015, 73, 951.e1–951.e12. [Google Scholar] [CrossRef]
- MacLennan, W.D. Fractures of the mandibular condylar process. Br J Oral Surg. 1969, 7, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Smets, M.H.; van Damme, P.A.; Stoelinga, P.J.W. Non-surgical treatment of condylar fractures in adults: a retrospective analysis. J Cranio-Maxillo-Fac Surg. 2003, 31, 162–167. [Google Scholar] [CrossRef]
- Villareal, P.M.; Monje, F.; Junquera, L.M.; Mateo, J.; Morillo, A.J.; Gonzalez, C. Mandibular condyle fractures: determinants of treatment and outcome. J Oral Maxillofac Surg. 2004, 62, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Ellis, E. Surgical treatment of adult mandibular condylar fractures provides better outcomes than closed treatment: a systematic review and meta-analysis. J Oral Maxillofac Surg. 2015, 73, 482–493. [Google Scholar] [CrossRef]
- Wagner, A.; Krach, W.; Schicho, K.; Undt, G.; Ploder, O.; Ewers, R. A 3-dimensional finite- element analysis investigating the bio- mechanical behavior of the mandible and plate osteosynthesis in cases of fractures of the condylar process. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002, 94, 678–686. [Google Scholar] [CrossRef]
- Kanno, T.; Sukegawa, S.; Tatsumi, H.; et al. The retromandibular transparotid approach for reduction and rigid internal fixation using two locking miniplates in mandibular condylar neck fractures. Int J Oral Maxillofac Surg. 2014, 43, 177–184. [Google Scholar] [CrossRef]
- Kisnisci, R. Management of fractures of the condyle, condylar neck, and coronoid process. Oral Maxillofac Surg Clin North Am. 2013, 25, 573–590. [Google Scholar] [CrossRef]
- Farmand, M. Experiences with the 3-D miniplate osteosynthesis in mandibular fractures. Fortschr Kiefer Gesichtschir. 1996, 41, 85. [Google Scholar]
- Hammer, B.; Schier, P.; Prein, J. Osteosynthesis of condylar neck fractures: a review of 30 patients. Br J Oral Maxillofac Surg. 1997, 35, 288–291. [Google Scholar] [CrossRef]
- Cortelazzi, R.; Altacera, M.; Turco, M.; Antonicelli, V.; De Benedittis, M. Development and clinical evaluation of MatrixMANDIBLE subcondylar plates system (synthes). Craniomaxillofacial Trauma Reconstr. 2015, 8, 94–99. [Google Scholar] [CrossRef]
- Murakami, K.; Yamamoto, K.; Sugiura, T.; Horita, S.; Matsusue, Y.; Kirita, T. Computed tomography-based 3-dimensional finite element analyses of various types of plates placed for a virtually reduced unilateral condylar fracture of the mandible of a patient. J Oral Maxillofac Surg. 2017, 75, 1239.e1–1239.e11. [Google Scholar] [CrossRef]
- Adhikari, M.; Bhatt, K.; Yadav, R.; Mandal, J.; Bhutia, O.; Roychoudhury, A. Fixation of subcondylar fractures of the mandible: a randomized clinical trial comparing one trapezoidal plate with two miniplates. Int J Oral Maxillofac Surg. 2021, 50, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.A.; Galinde, J.; Asnani, U.; Mistry, Y.A. Comparative evaluation of clinical outcomes using delta plates and conventional miniplates for internal fixation of mandibular condylar fractures in adults. J Oral Maxillofac Surg. 2018, 76, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, A.; Mittal, G.; Garg, R. Comparison between 3D delta plate and conventional miniplate in treatment of condylar fracture: a randomised clinical trial. J Cranio-Maxillo-Fac Surg. 2021, 49, 1026–1034. [Google Scholar] [CrossRef]
- Rai, A.; Jain, A.; Thukral, R. Two miniplates versus 3- dimensional plate in the management of mandibular subcondylar fractures: a retrospective analysis. Oral Maxillofac Surg. 2021, 25, 457–461. [Google Scholar] [CrossRef]
- Scott, C.; Ramakrishnan, K.; Vivek, N.; Saravanan, C.; Prashanthi, G. Does three-dimensional plate offer better outcome and reduce the surgical time following open reduction and internal fixation of adult mandibular unilateral subcondylar fractures. A randomized clinical study. J Oral Maxillofac Surg. 2021, 79, 1330.e1–1330.e12. [Google Scholar] [CrossRef]
- Sehgal, S.; Ramanujam, L.; Prasad, K.; Krishnappa, R. Three- dimensional v/s standard titanium miniplate fixation in the management of mandibular fractures--a randomized clinical study. J Cranio-Maxillo-Fac Surg. 2014, 42, 1292–1299. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Masui, M.; et al. Which fixation methods are better between three-dimensional anatomical plate and two miniplates for the mandibular subcondylar fracture open treatment? J Cranio-Maxillo-Fac Surg. 2019, 47, 771–777. [Google Scholar] [CrossRef]
- Gassner, R.; Tuli, T.; H€achl, O.; et al. Cranio-maxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J Cranio-Maxillo-Fac Surg. 2003, 31, 51. [Google Scholar] [CrossRef] [PubMed]
- Eckelt, U.; Schneider, M.; Erasmus, F.; et al. Open versus closed treatment of fractures of the mandibular condylar process – a prospective randomized multi-centre study. J Cranio-Maxillo-Fac Surg. 2006, 34, 306–314. [Google Scholar] [CrossRef]
- Worsaae, N.; Thorn, J.J. Surgical versus non- surgical treatment of unilateral dislocated low subcondylar frac- tures: a clinical study of 52 cases. J Oral Maxillofac Surg. 1994, 52, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E.; Simon, P.; Throckmorton, G.S. Occlusal results after open or closed treatment of fractures of the mandibular condylar process. J Oral Maxillofac Surg. 2000, 58, 260–268. [Google Scholar] [CrossRef]
- Ellis, E.; Throckmorton, G.S.; Palmieri, C. Open treatment of condylar process fractures: assessment of adequacy of repositioning and maintenance of stability. J Oral Maxillofac Surg. 2000, 58, 27. [Google Scholar] [CrossRef]
- Haug, R.H.; Assael, L.A. Outcomes of open versus closed treatment of mandibular subcondylar fractures. J Oral Maxillofac Surg. 2001, 59, 370. [Google Scholar] [CrossRef]
- Hyde, N.; Manisali, M.; Aghabeigi, B.; et al. The role of open reduction and internal fixation in unilateral fractures of the mandibular condyle: a prospective study. Br J Oral Maxillofac Surg. 2002, 40, 19. [Google Scholar] [CrossRef]
- Meyer, C.; Kahn, J.L.; Boutemi, P.; Wilk, A. Photoelastic analysis of bone deformation in the region of the mandibular condyle during mastication. J Cranio-Maxillo-Fac Surg. 2002, 30, 160. [Google Scholar] [CrossRef]
- Darwich, M.A.; Albogha, M.H.; Abdelmajeed, A.; Darwich, K. Assessment of the biomechanical performance of 5 plating techniques in fixation of mandibular subcondylar fracture using finite element analysis. J Oral Maxillofac Surg. 2016, 74, 794.e1–794.e8. [Google Scholar] [CrossRef]
- Ellis, E.; Throckmorton, G.S.; Palmieri, C. Treatment of mandibular condylar process fractures: biological consideration. J Oral Maxillofac Surg. 2005, 63, 115–134. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Evaluation |
| Population (P) | Patients requiring open reduction and internal fixation of mandibular subcondylar fractures |
| Intervention (I) | Three dimensional plate (3D plate) for fixation of mandibular subcondylar fractures |
| Comparison (C) | Conventional two miniplates for fixation of mandibular subcondylar fractures |
| Outcomes (O) | Operative time, stability, mouth opening and complications |
| No. Of Patients | |||||||
| Sr No. | Author, Publication Year & Country | Age Range | Male/Female | Two Miniplates Group | 3 D Plate Group | Parameters Assessed | Type of 3D Plate |
| 1. | Adhikari et al (2021) [14] India | 18+ years | 46/6 | 26 | 26 | 1. Intra-operative time taken for fixation 2. Ease of plate adaptation 3. Postoperative status of occlusion 4. Radiographic plate fracture 5. Maximum mouth opening 6. Protrusive, ipsilateral, and contralateral movements 7. Facial nerve status 8. Complications like development of a temporomandibular disorder, sialocele, infection, or hypertrophic scar. | Trapezoidal plate |
| 2. | Ahuja et al (2018) [15] India | 18 to 60 years | 17/3 | 10 | 10 | 1. Intra-operative time taken for fixation 2. Ease of plate adaptation 3. Postoperative status of occlusion 4. Need for intermaxillary Fixation 5. Maximum mouth opening 6. Lateral excursive and protrusive movements | Delta plate |
| 3. | Ganguly et al (2021) [16] India | 16+ years | 18/2 | 10 | 10 | 1. Complications like pain, wound dehiscence, infection 2. Mouth opening and lateral deviation while mouth opening 3. Biting efficiency 4. Need for postoperative intermaxillary fixation 5. Radiographic assessment of fracture reduction 6. Bite force | Delta plate |
| 4. | Rai et al (2021) [17] India | 21 to 59 years | 43/15 | 35 | 23 | 1. Occlusal stability 2. Postoperative complications like plate fracture, non-union, plate or screw loosening, plate or screw infection leading to implant removal, wound dehiscence, salivary fistula, and facial nerve paralysis. 3. Radiographic evaluation of fracture reduction | Rectangular plate |
| 5. | Scott et al (2020) [18] India | 18 to 53 years | 40/4 | 22 | 22 | 1. Time taken for fixation 2. Maximum mouth opening 3. Occlusal stability 4. Radiographic evaluation of fracture reduction 5. Jaw movements | Trapezoidal plate |
| 6. | Sehgal et al (2014) [19] India | 18 to 60 years | 26/4 | 15 | 15 | 1. Intraoperative assessment of reduction of fracture 2. Stability of occlusion 3. Need for intermaxillary fixation 4. Post-operative complications like tissue dehiscence and infection. 5. Bone Union 6. Plate Fracture | Rectangular plate |
| 7. | Sukegawa et al (2019) [20] Japan | Not reported | 16/10 | 14 | 12 | 1. Complications like postoperative infection, facial nerve paralysis, nonunion, malunion, and occlusal insufficiency, foreign body sensation by an osteosynthesis plate, and plate removal 2. Postoperative stability and occlusion | MatrixMANDIBLE subcondylar plate |
| Parameter Assessed | |||||||
| Sr No. | Author, Publication Year & Country | Intra-operative Time | Occlusion | Ease of Adaptation of Plate | Mouth Opening | Jaw Movements | Any Other |
| 1. | Adhikari et al (2021) [14] | Yes | Yes | Yes | Yes | Yes | Not reported |
| India | 3D plate <2 miniplates | Satisfactory in all cases | Better in 3D plate group | No significant difference in both groups | Satisfactory in all cases | ||
| 2. | Ahuja et al (2018) [15] | Not reported | Yes | Yes | Yes | Yes | Not reported |
| India | No difference in both the groups | Faster in 3D plate group | No significant difference in both groups | No significant difference in both groups | |||
| 3. | Ganguly et al (2021) [16] | Yes | Not | Not | Yes | Not | Biting Efficiency |
| India | 3D plate <2 miniplates | 3D plate >2 miniplates | 3D plate >2 miniplates | ||||
| 4. | Rai et al (2021) [17] | Not reported | Yes | Not | Not reported | Not | Not reported |
| India | No difference in both the groups | ||||||
| 5. | Scott et al (2020) [18] | Yes | Yes | Not | Yes | Yes | Gap between fractured Segments 2 miniplates > 3D plate |
| India | 3D plate <2 miniplates | Satisfactory in all cases | 3 D plate >2 miniplates | No significant difference in both groups | |||
| 6. | Sehgal et al (2014) [19] | Not reported | Yes | Not reported | Not reported | Not reported | Not reported |
| India | Satisfactory in all cases | ||||||
| 7. | Sukegawa et al (2019) [20] | Not reported | Not reported | Not reported | Not reported | Not reported | Vertical height |
| Japan | Difference | ||||||
| No difference in both groups | |||||||
| Complications Reported | |||||||||||
| Plate Fracture | Facial Nerve Weakness | Sialocele | Surgical Site Infection/Wound Dehiscence | Non-Union | |||||||
| Sr No. | Author, Publication Year & Country | Miniplate Group | 3D Plate Group | Miniplate Group | 3D Plate Group | Miniplate Group | 3D Plate Group | Miniplate Group | 3D Plate Group | Miniplate Group | 3D Plate Group |
| 1. | Adhikari et al (2021) [14] | 4/25 | Zero | Zero | 2/25 | 3/25 | 1/25 | Zero | 1/25 | NR | NR |
| India | |||||||||||
| 2. | Ahuja et al (2018) [15] | Zero | Zero | Zero | 1/10 | NR | NR | 1/10 | Zero | NR | NR |
| India | |||||||||||
| 3. | Ganguly et al (2021) [16] | Zero | Zero | Zero | Zero | NR | NR | 1/10 | 1/10 | NR | NR |
| India | |||||||||||
| 4. | Rai et al (2021) [17] | 1/35 | 2/23 | 1/35 | 2/23 | 1/35 | Zero | 2/35 | 1/23 | Zero | 1/23 |
| India | |||||||||||
| 5. | Scott et al (2020) [18] | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| India | |||||||||||
| 6. | Sehgal et al (2014) [19] | Zero | Zero | NR | NR | NR | NR | Zero | Zero | Zero | Zero |
| India | |||||||||||
| 7. | Sukegawa et al (2019) [20] | Zero | 2/12 | 2/14 | Zero | NR | NR | Zero | 1/12 | Zero | 1/12 |
| Japan | |||||||||||
© 2024 by the authors. The Author(s) 2024.
Share and Cite
Kuna, S.K.; Jain, A.; Kuna, V. Two Miniplates Versus Three Dimensional Plate in Management of Mandibular Condylar Fractures: A Systematic Review and Meta-Analysis. Craniomaxillofac. Trauma Reconstr. 2024, 17, 72. https://doi.org/10.1177/19433875241252979
Kuna SK, Jain A, Kuna V. Two Miniplates Versus Three Dimensional Plate in Management of Mandibular Condylar Fractures: A Systematic Review and Meta-Analysis. Craniomaxillofacial Trauma & Reconstruction. 2024; 17(4):72. https://doi.org/10.1177/19433875241252979
Chicago/Turabian StyleKuna, Santhosh Kumar, Anuj Jain, and Vishala Kuna. 2024. "Two Miniplates Versus Three Dimensional Plate in Management of Mandibular Condylar Fractures: A Systematic Review and Meta-Analysis" Craniomaxillofacial Trauma & Reconstruction 17, no. 4: 72. https://doi.org/10.1177/19433875241252979
APA StyleKuna, S. K., Jain, A., & Kuna, V. (2024). Two Miniplates Versus Three Dimensional Plate in Management of Mandibular Condylar Fractures: A Systematic Review and Meta-Analysis. Craniomaxillofacial Trauma & Reconstruction, 17(4), 72. https://doi.org/10.1177/19433875241252979