A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma

Abstract
:Introduction
Materials and Methods
Study Design and Population
Measurements
Statistical Analysis
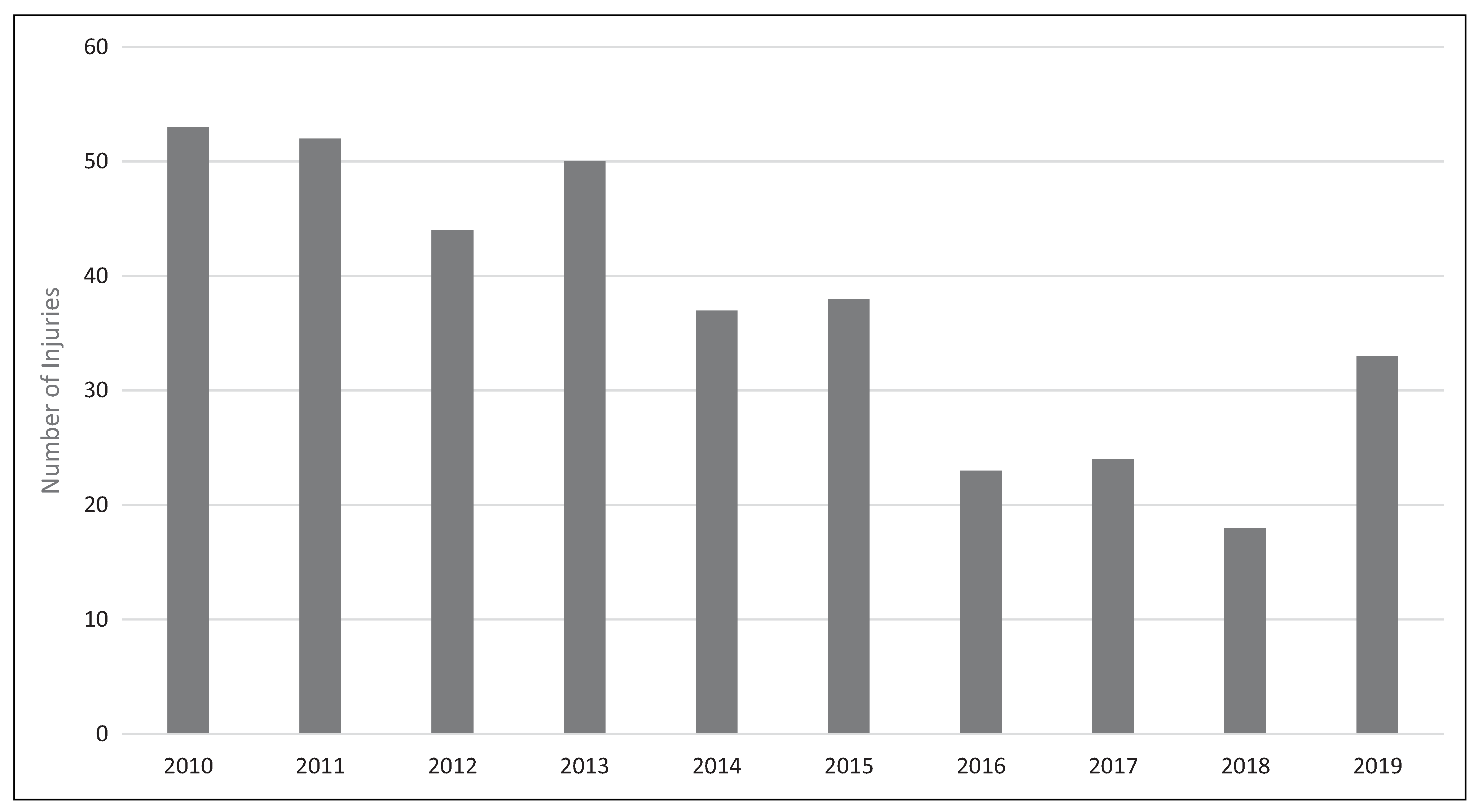
Results
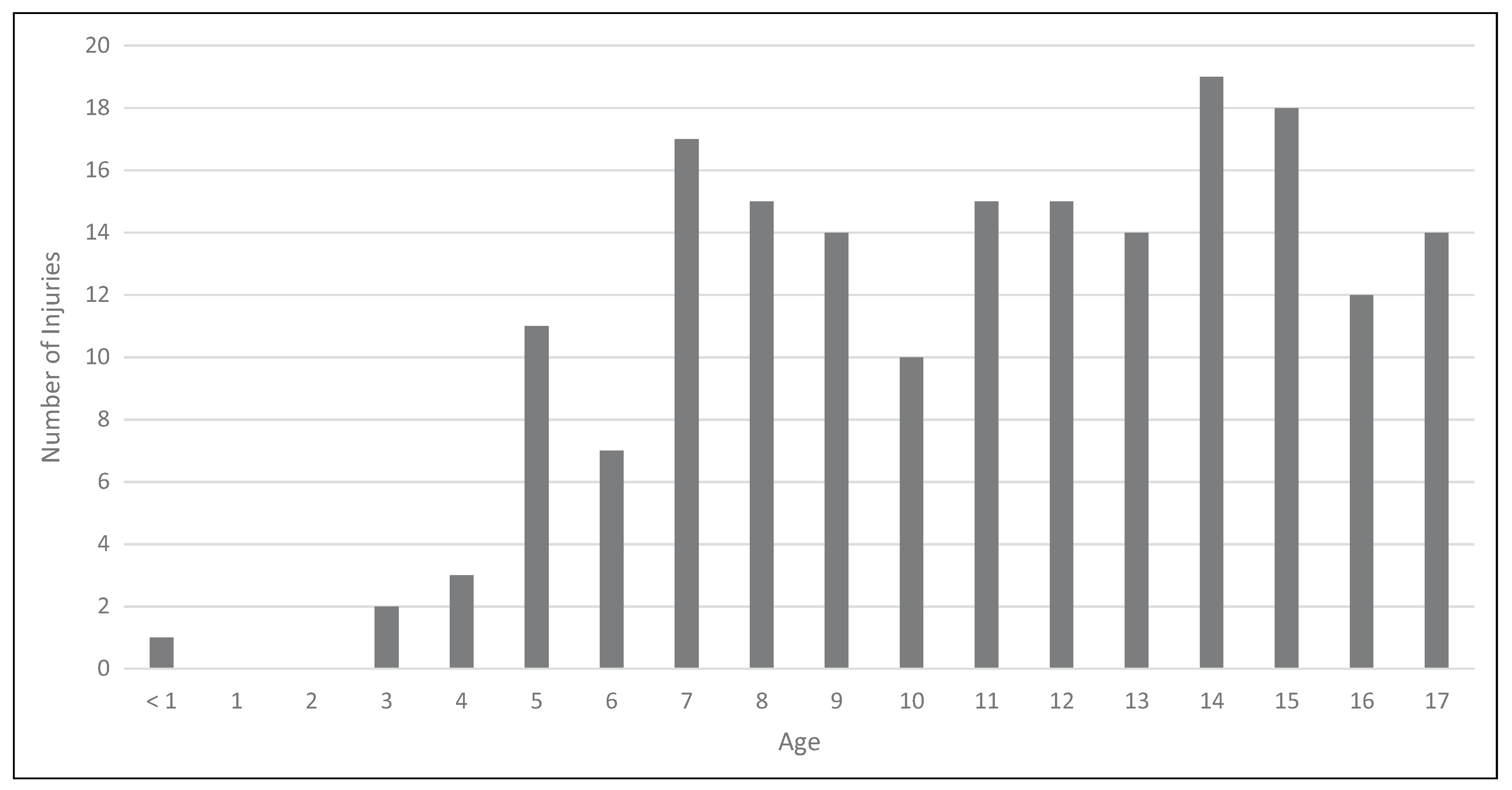
Age-Related Trends
Sex-Related Trends
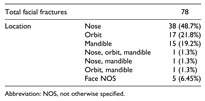
Facial Fractures
Discussion
Conclusions
Declaration of Conflicting Interests
Funding
References
- Physical Activity Council. 2020 physical activity council’s overview report on U.S. participation. Published 2021. Accessed , 2020. https://eb6d91a4-d249-47b8- a5cb-933f7971db54.filesusr.com/ugd/286de6_c28995b76cf 94de2a22ac7a0a4d5264d. 14 December.
- Skokan EG, Junkins EP, Kadish H. Serious winter sport injuries in children and adolescents requiring hospitalization. Am J Emerg Med. [CrossRef]
- U.S. Consumer Product Safety Commission Division of Hazard and Injury Data Systems. The National Electronic Injury Surveillance System: a tool for researchers. Published 2021. Accessed , 2020. https://www.cpsc.gov/ Research–Statistics/NEISS-Injury-Data. 14 December.
- U.S. Consumer Product Safety Commission Division of Hazard and Injury Data Systems NEISS coding manual. Published 2021. Accessed , 2020. https:// www.cpsc.gov/s3fs-public/2019_NEISS_Coding_Manual. pdf. 14 December.
- Schroeder T, Ault K, U.S. Consumer Product Safety Com- mission Division of Hazard and Injury Data Systems. The NEISS sample (design and implementation) 1997 to present. Published 2021. Accessed , 2020. https://www. cpsc.gov/s3fs-public/pdfs/blk_media_2001d011-6b6.pdf. 14 December.
- Svider PF, Bobian M, Hojjat H, et al. A chilling reminder: pediatric facial trauma from recreational winter activities. Int J Pediatr Otorhinolaryngol. [CrossRef]
- Tuli T, Haechl O, Berger N, et al. Facial trauma: how dan- gerous are skiing and snowboarding? J Oral Maxillofac Surg. [CrossRef]
- Provance AJ, Daoud AK, Tagawa A, Rhodes J. Pediatric and adolescent injury in skiing. Res Sports Med, 1: 1). [CrossRef]
- Federiuk CS, Schlueter JL, Adams AL. Skiing, snowboard- ing, and sledding injuries in a northwestern state. Wilderness Environ Med.
- Døving M, Galteland P, Eken T, et al. Dentoalveolar injuries, bicycling accidents and helmet use in patients referred to a Norwegian trauma Centre: a 12-year prospective study. Dent Traumatol, 2020. [CrossRef]
- Frenkel B, Bahouth H, Abu Shqara F, Rachmiel A. Cranio- facial injuries seen among electric-motorized bicycle riders. J Craniofac Surg, 2: online. 2020;31(8), 2020. [CrossRef]
- Moshy JR, Msemakweli BS, Owibingire SS, Sohal KS. Pattern of mandibular fractures and helmet use among motor- cycle crash victims in Tanzania. Afr Health Sci. [CrossRef]
- Alfrey EJ, Tracy M, Alfrey JR, et al. Helmet usage reduces serious head injury without decreasing concussion after bicycle riders crash. J Surg Res. [CrossRef]
- Micieli JA, Zurakowski D, Ahmed IIK. Impact of visors on eye and orbital injuries in the National Hockey League. Can J Ophthalmol. [CrossRef]
- Benson BW, Mohtadi NG, Rose MS, Meeuwisse WH. Head and neck injuries among ice hockey players wearing full face shields vs half face shields. JAMA, 2328. [CrossRef]
- Murray TM, Livingston LA. Hockey helmets, face masks, and injurious behavior. Pediatrics.

{kind=link}
{kind=link}
| Values | ||
| Facial injuries | 361 | |
| Average age (SD) [years] | 21.1 (14.5) | |
| Sex (n ¼ 361) | Male | 244 (67.6%) |
| Female | 117 (32.4%) | |
| Race (n ¼ 361) | White | 259 (71.7%) |
| Black | 7 (1.9%) | |
| Other | 8 (2.2%) | |
| Asian | 11 (3.0%) | |
| American Indian/American native | 1 (0.28%) | |
| Native Hawaiian/Pacific Islander | 0 (0%) | |
| Not specified | 75 (20.8%) | |
| Type (n ¼ 361) | Lacerations | 165 (45.7%) |
| Contusions/Abrasions | 87 (24.0%) | |
| Fractures | 78 (21.6%) | |
| Bleeds | 3 (0.85%) | |
| All other | 28 (7.8%) | |
| Disposition from ED (n ¼ 361) | Treated and discharged | 340 (94.2%) |
| Treated and admitted | 11 (3.0%) | |
| Left without being seen | 3 (0.83%) | |
| Treated and transferred | 2 (0.55%) | |
| Held for observation | 5 (1.4%) | |
| Fatality incl. DOA or died in ED | 0 (0%) | |
| Abbreviations: DOA, dead on arrival; ED, emergency department. |
| Adult (n = 174) | Children (n =187) | ||
| Sex | Male | 117 (67.2%) | 127 (67.9%) |
| Female | 57 (32.8%) | 60 (32.1%) | |
| Injury type | Contusion | 40 (23.0%) | 47 (25.1%) |
| Fracture* | 52 (30.0%) | 26 (13.9%) | |
| Bleed | 2 (1.1%) | 1 (0.53%) | |
| Laceration% | 68 (39.1%) | 97 (51.9%) | |
| Other/Not specified | 12 (6.9%) | 16 (8.6%) | |
| Disposition | Treated and discharged | 166 (95.4%) | 174 (93.0%) |
| Treated and transferred | 2 (1.15%) | 0 (0%) | |
| Treated and admitted% | 2 (1.15%) | 9 (4.8%) | |
| Left without being seen | 2 (1.15%) | 1 (0.53%) | |
| Held for observation | 2 (1.15%) | 3 (1.6%) |
| Male (n ¼ 244) | Female (n ¼ 117) | ||
| Mean age (+ SD) [years] | 21.0 (14.4) | 21.4 (14.7) | |
| Injury time | Contusion% | 50 (20.5%) | 37 (31.6%) |
| Fracture | 50 (20.5%) | 28 (23.9%) | |
| Hemorrhage | 2 (0.8%) | 1 (0.9%) | |
| Laceration* | 126 (51.6%) | 39 (33.3%) | |
| Other/Not specified | 16 (6.6%) | 12 (10%) | |
| Disposition | Treated and discharged% | 235 (96.3%) | 105 (89.7%) |
| Treated and transferred | 0 (0%) | 2 (1.71%) | |
| Treated and admitted | 5 (2.1%) | 6 (5.1%) | |
| Left without being seen | 1 (0.4%) | 2 (1.71%) | |
| Held for observation | 3 (1.2%) | 2 (1.71%) | |
| Abbreviation: SD, standard deviation.*P < 0.01, %P < 0.05. | |||
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the AO Foundation. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorenson, T.J.; Borad, V.; Schubert, W. A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma. Craniomaxillofac. Trauma Reconstr. 2022, 15, 28-33. https://doi.org/10.1177/1943387521997237
Sorenson TJ, Borad V, Schubert W. A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma. Craniomaxillofacial Trauma & Reconstruction. 2022; 15(1):28-33. https://doi.org/10.1177/1943387521997237
Chicago/Turabian StyleSorenson, Thomas J., Vedant Borad, and Warren Schubert. 2022. "A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma" Craniomaxillofacial Trauma & Reconstruction 15, no. 1: 28-33. https://doi.org/10.1177/1943387521997237
APA StyleSorenson, T. J., Borad, V., & Schubert, W. (2022). A Nationwide Study of Skiing and Snowboarding-Related Facial Trauma. Craniomaxillofacial Trauma & Reconstruction, 15(1), 28-33. https://doi.org/10.1177/1943387521997237