Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience
 , and
, and
Abstract
:Introduction
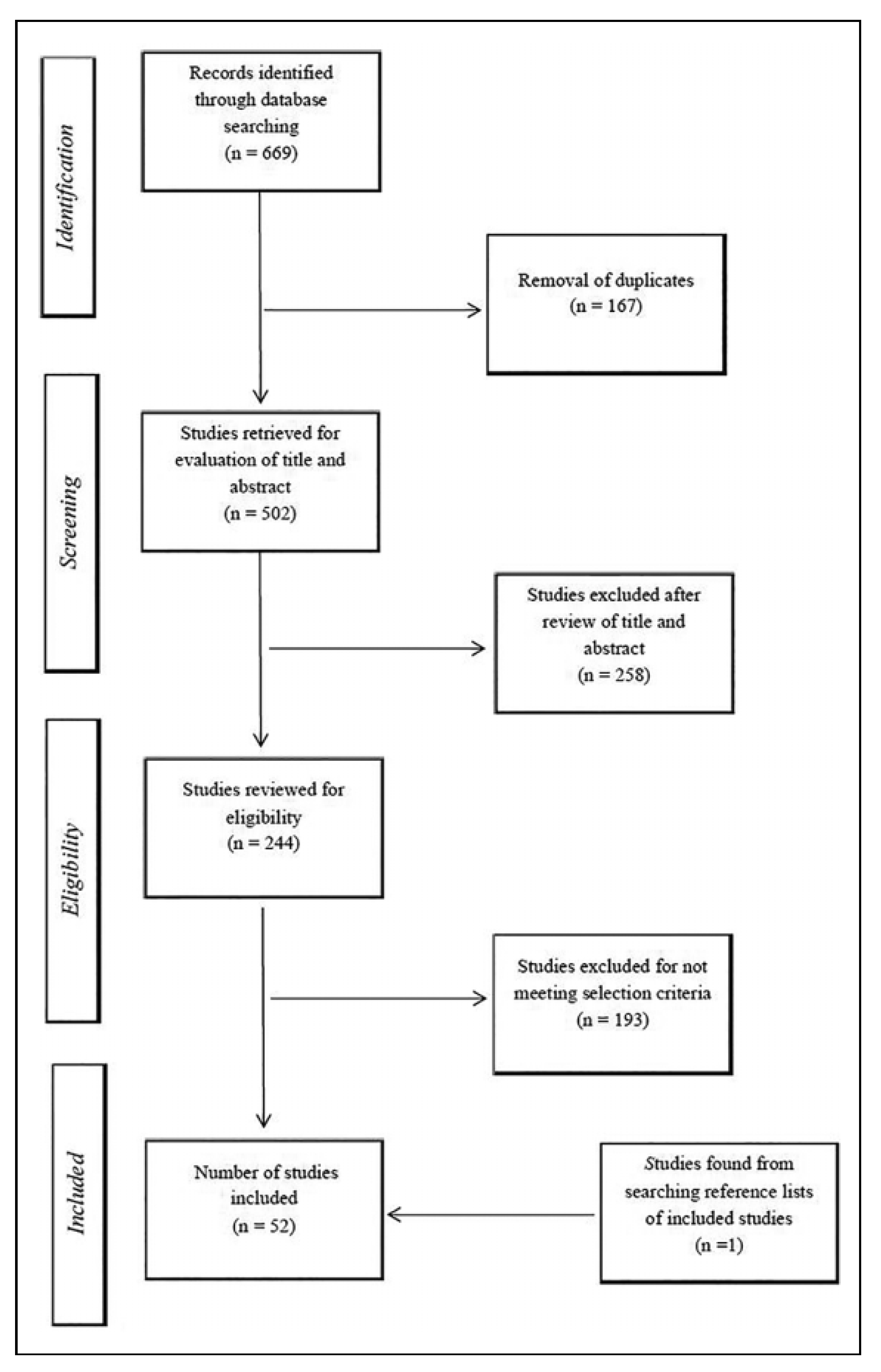
Methods
Inclusion and Exclusion Criteria
Data Evaluation and Extraction
Results
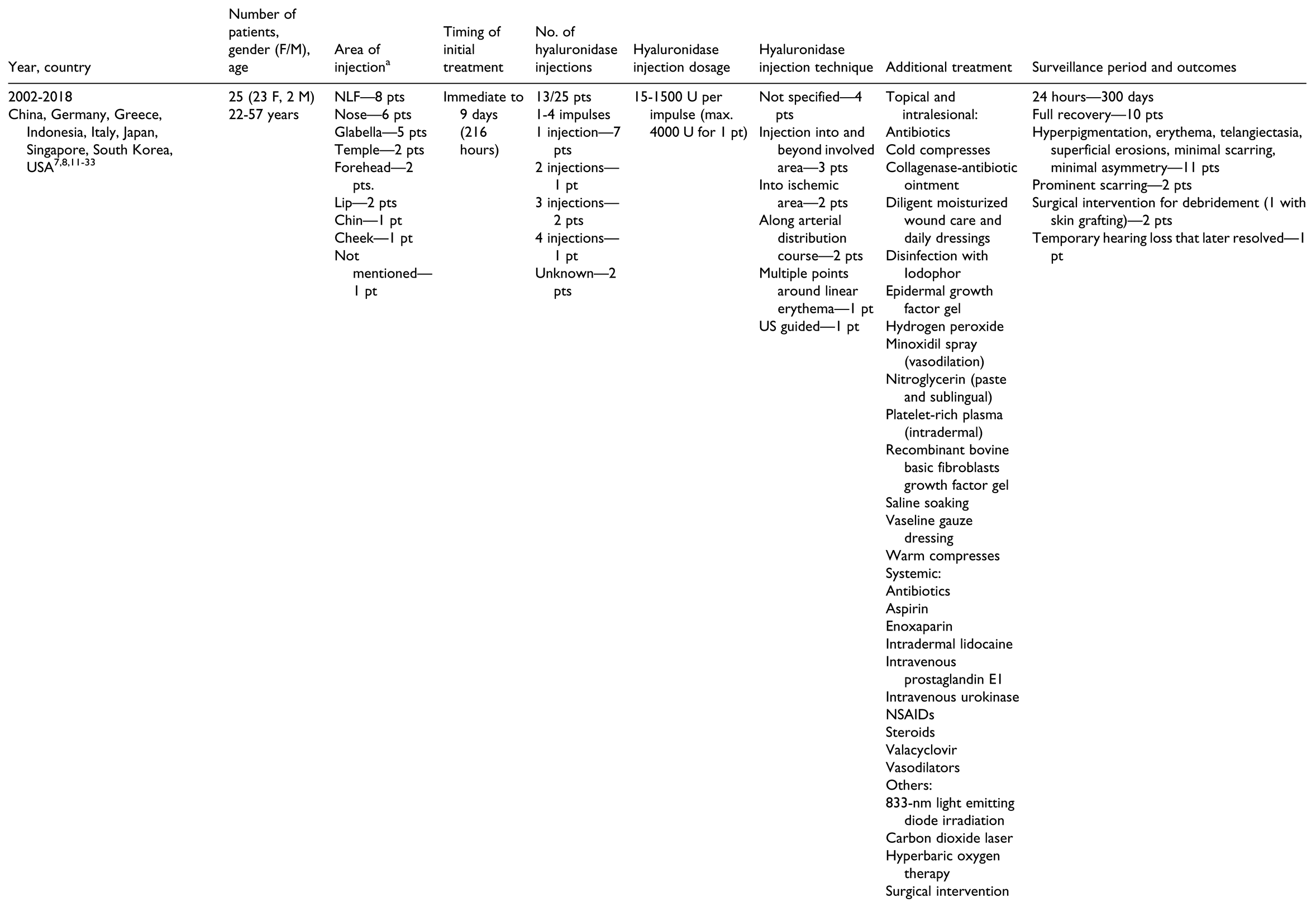
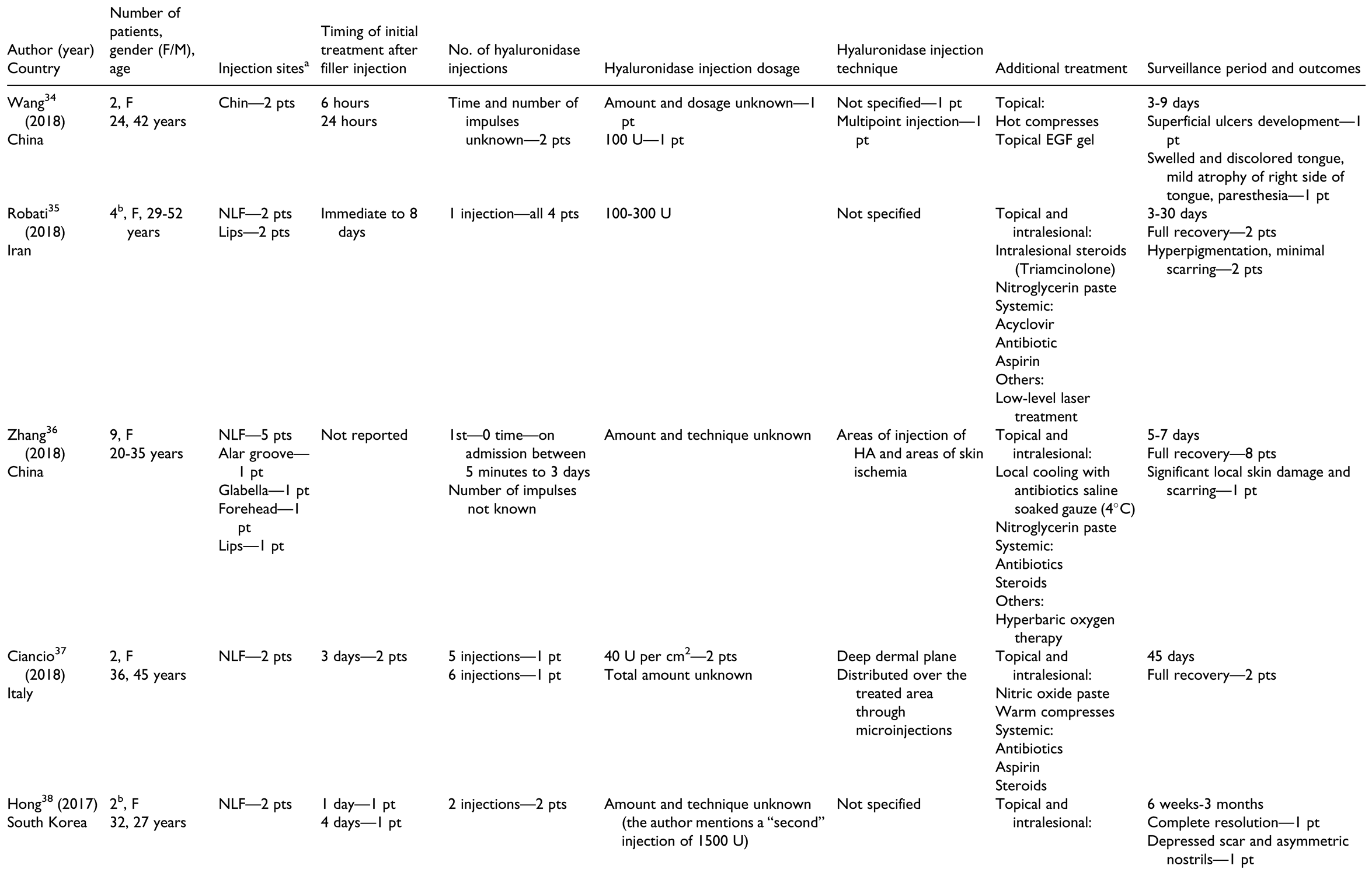
Characteristics of Included Studies
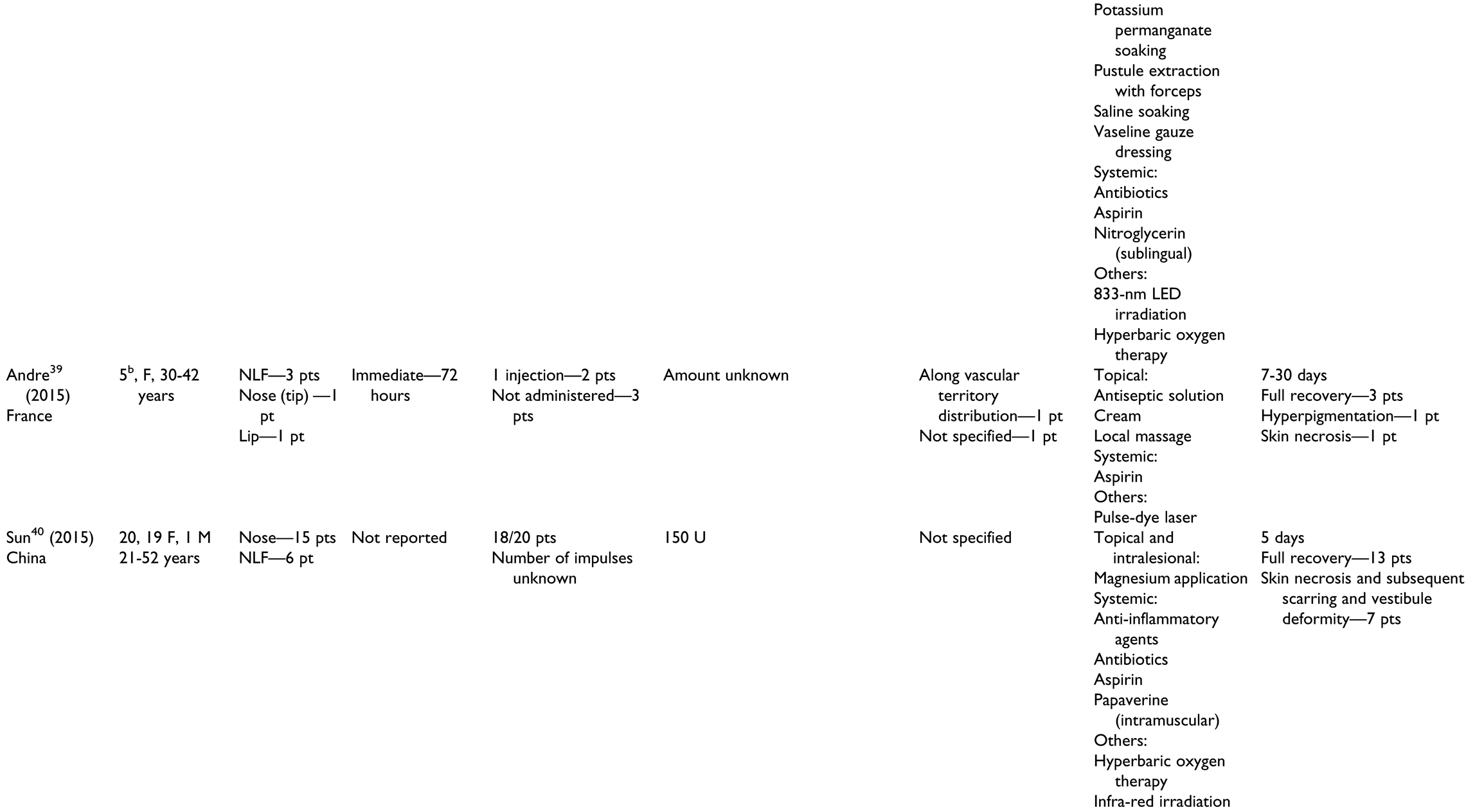
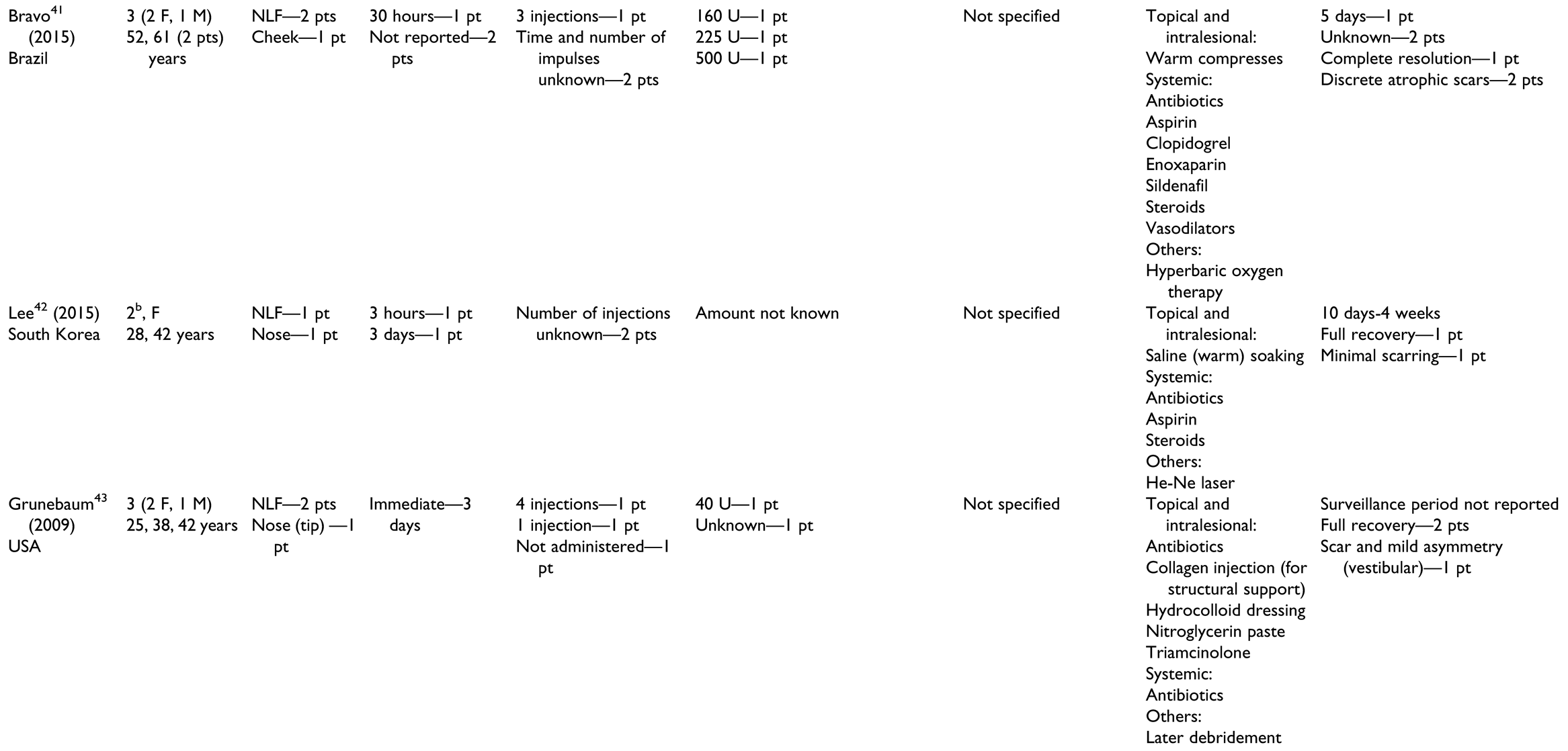
Non-Ophthalmic-Related Vascular Obstruction
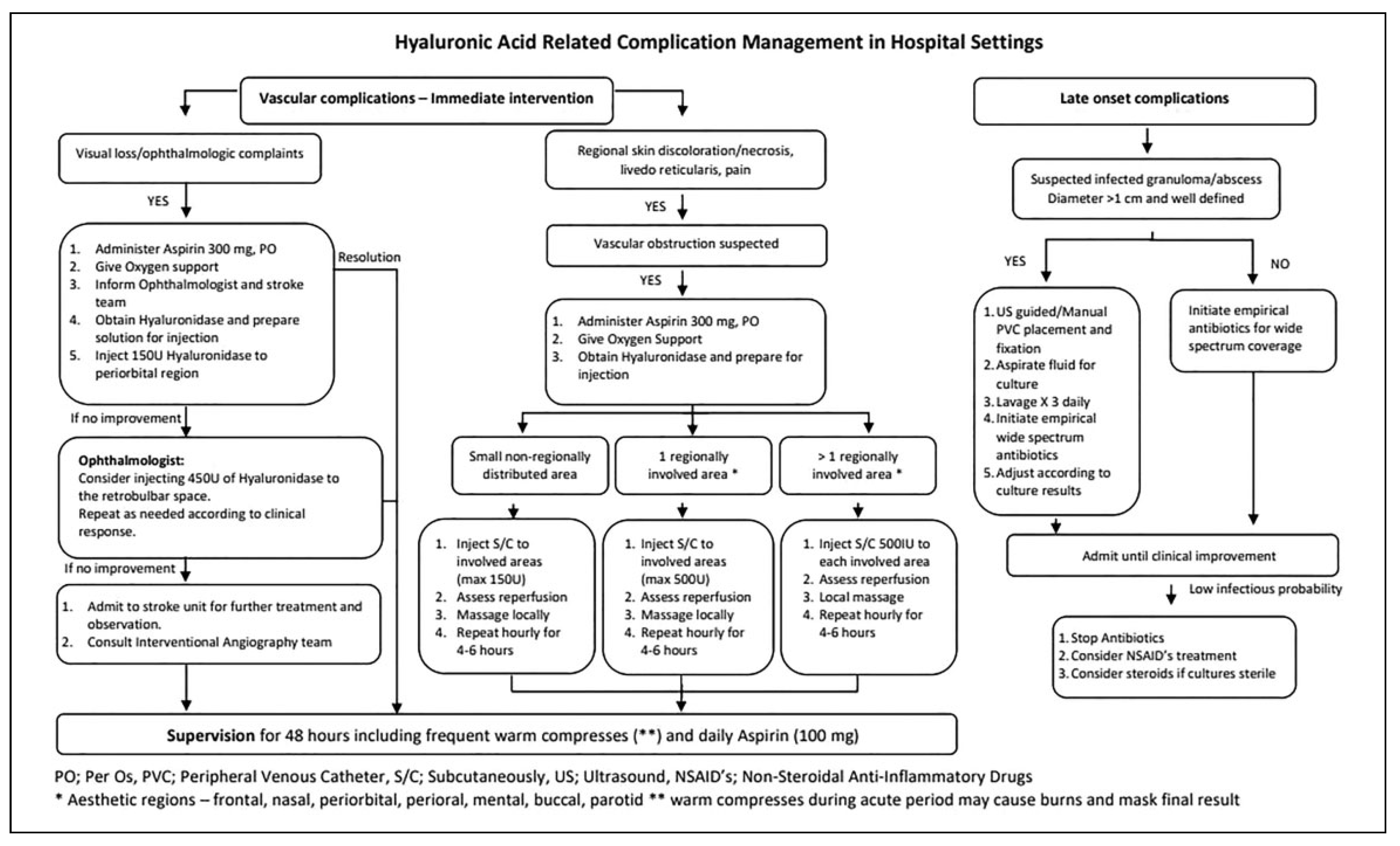
Proposed Algorithm
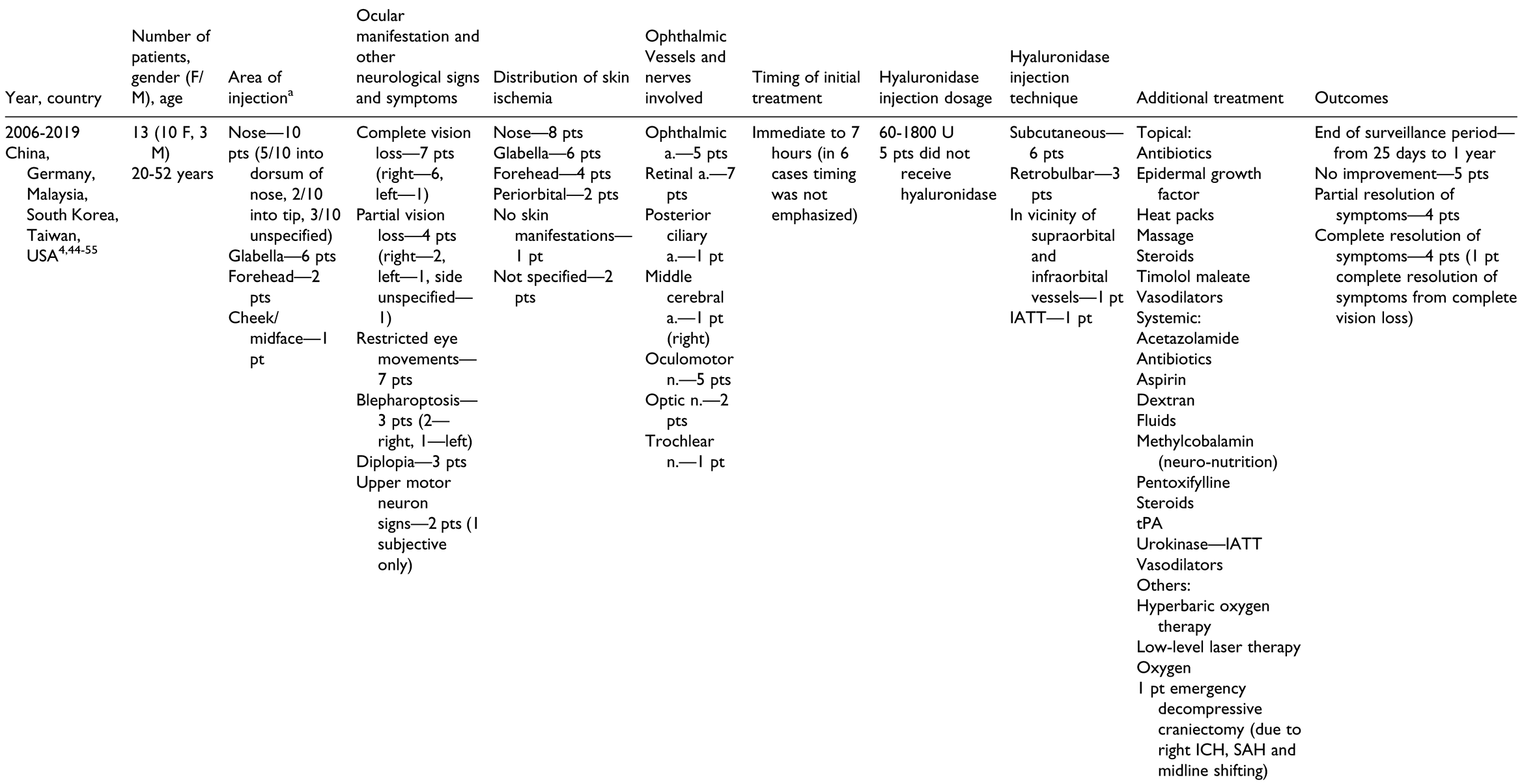
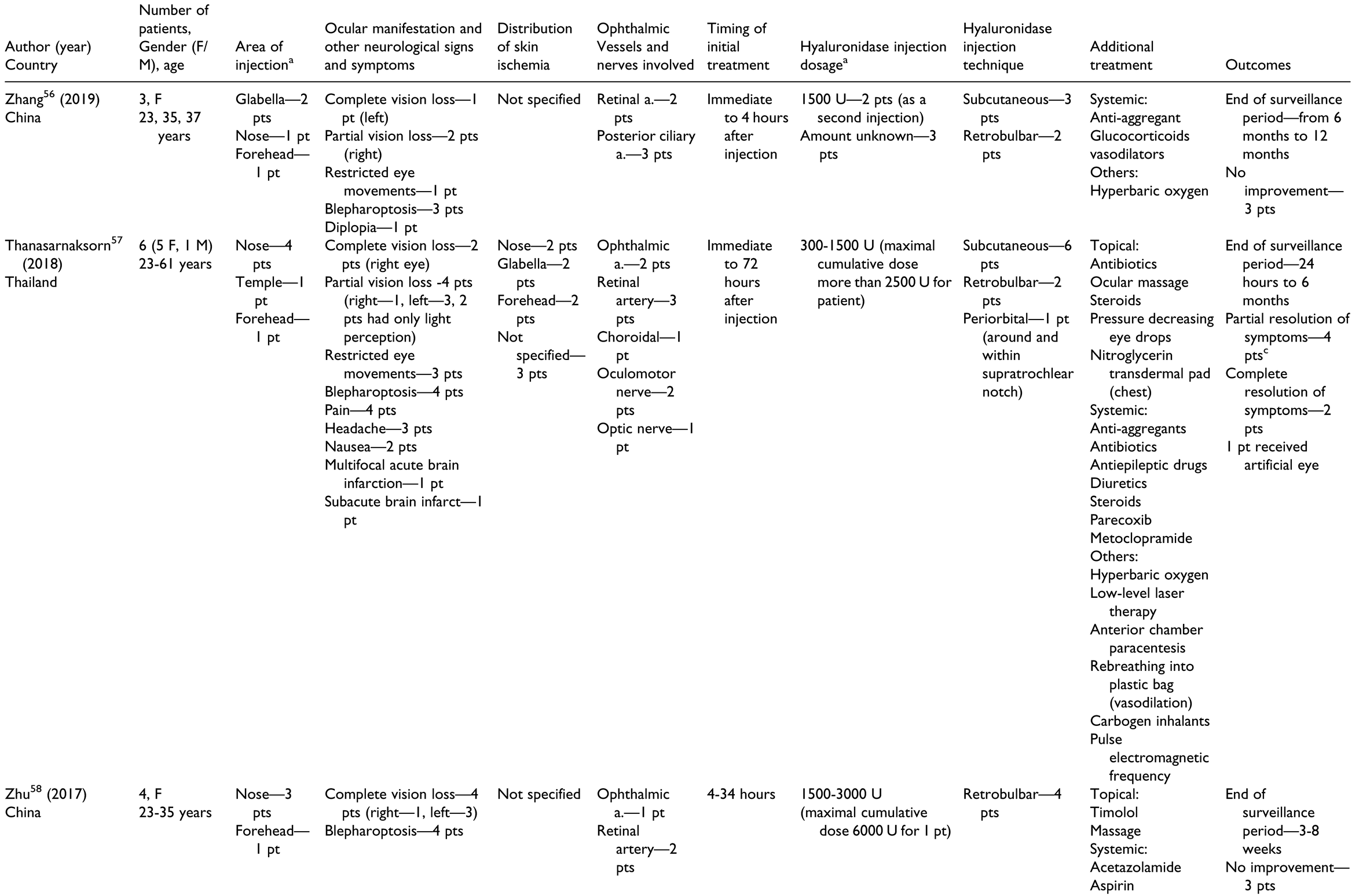
Ophthalmic Vascular Obstruction
Abscesses and Infected Granulomas
Discussion
Limitations
Conclusions
Funding
Conflicts of Interest
References
- Park, T.H.; Seo, S.W.; Kim, J.K.; Chang, C.H. Clinical experience with hyaluronic acid-filler complications. J Plast Reconstr Aesthet Surg. 2011, 64, 892–896. [Google Scholar] [PubMed]
- Bailey, S.H.; Fagien, S.; Rohrich, R.J. Changing role of hyaluronidase in plastic surgery. Plast Reconstr Surg. 2014, 133, 127e–132e. [Google Scholar]
- Landau, M. Hyaluronidase caveats in treating filler complications. Dermatol Surg. 2015, 41, S347–S353. [Google Scholar]
- Bae, I.H.; Kim, M.S.; Choi, H.; Na, C.H.; Shin, B.S. Ischemic oculomotor nerve palsy due to hyaluronic acid filler injection. J Cosmet Dermatol. 2018, 17, 1016–1018. [Google Scholar]
- Cohen, J.L.; Biesman, B.S.; Dayan, S.H.; et al. Treatment of hyaluronic acid filler-induced impending necrosis with hyaluronidase: consensus recommendations. Aesthet Surg J. 2015, 35, 844–849. [Google Scholar]
- Urdiales-Galvez, F.; Delgado, N.E.; Figueiredo, V.; et al. Treatment of soft tissue filler complications: expert consensus recommendations. Aesthetic Plast Surg. 2018, 42, 498–510. [Google Scholar] [PubMed]
- Loh, K.T.D.; Phoon, Y.S.; Phua, V.; Kapoor, K.M. Successfully managing impending skin necrosis following hyaluronic acid filler injection, using high-dose pulsed hyaluronidase. Plast Reconstr Surg Glob Open. 2018, 6, e1639. [Google Scholar]
- Hirsch, R.J.; Cohen, J.L.; Carruthers, J.D. Successful management of an unusual presentation of impending necrosis following a hyaluronic acid injection embolus and a proposed algorithm for management with hyaluronidase. Dermatol Surg. 2007, 33, 357–360. [Google Scholar]
- Humzah, M.D.; Ataullah, S.; Chiang, C.; Malhotra, R.; Goldberg, R. The treatment of hyaluronic acid aesthetic interventional induced visual loss (AIIVL): a consensus on practical guidance. J Cosmet Dermatol. 2019, 18, 71–76. [Google Scholar] [PubMed]
- Signorini, M.; Liew, S.; Sundaram, H.; et al. Global aesthetics consensus: avoidance and management of complications from hyaluronic acid fillers—evidence-and opinion-based review and consensus recommendations. Plast Reconstr Surg. 2016, 137, 961. [Google Scholar]
- Yang, Q.; Qiu, L.; Yi, C.; et al. Reversible alopecia with localized scalp necrosis after accidental embolization of the parietal artery with hyaluronic acid. Aesthetic Plast Surg. 2017, 41, 695–699. [Google Scholar] [PubMed]
- Fang, M.; Rahman, E.; Kapoor, K.M. Managing complications of submental artery involvement after hyaluronic acid filler injection in chin region. Plast Reconstr Surg Glob Open. 2018, 6, e1789. [Google Scholar] [PubMed]
- Pavlidis, L.; Spyropoulou, G.A.; Deliligka, A.; Demiri, E. Intravenous hyaluronidase with urokinase as treatment for arterial hyaluronic acid embolism. Plast Reconstr Surg. 2016, 138, 370e–371e. [Google Scholar] [PubMed]
- Kang, M.S.; Park, E.S.; Shin, H.S.; Jung, S.G.; Kim, Y.B.; Kim, D.W. Skin necrosis of the nasal ala after injection of dermal fillers. Dermatol Surg. 2011, 37, 375–380. [Google Scholar]
- Chen, Q.; Liu, Y.; Fan, D. Serious vascular complications after nonsurgical rhinoplasty: a case report. Plast Reconstr Surg Glob Open. 2016, 4, e683. [Google Scholar]
- Kim, J.L.; Shin, J.Y.; Roh, S.G.; Lee, N.H. Demarcative necrosis along previous laceration line after filler injection. J Craniofac Surg. 2017, 28, e481–e482. [Google Scholar]
- Henderson, R.; Reilly, D.A.; Cooper, J.S. Hyperbaric oxygen for ischemia due to injection of cosmetic fillers: case report and issues. Plast Reconstr Surg Glob Open. 2018, 6, e1618. [Google Scholar]
- Grzybinski, S.; Temin, E. Vascular occlusion after hyaluronic acid filler injection. Clin Pract Cases Emerg Med. 2018, 2, 167–168. [Google Scholar]
- Han, J.; He, Y.; Liu, K.; Yang, Q. Necrosis of the glabella after injection with hyaluronic acid into the forehead. J Craniofac Surg. 2018, 29, e726–e727. [Google Scholar]
- Maruyama, S. A histopathologic diagnosis of vascular occlusion after injection of hyaluronic acid filler: findings of intravascular foreign body and skin necrosis. Aesthet Surg J. 2017, 37, NP102–NP108. [Google Scholar]
- Salval, A.; Ciancio, F.; Margara, A.; Bonomi, S. Impending facial skin necrosis and ocular involvement after dermal filler injection: a case report. Aesthetic Plast Surg. 2017, 41, 1198–1201. [Google Scholar] [PubMed]
- Kwon, H.J.; Kim, B.J.; Ko, E.J.; Choi, S.Y. The utility of color Doppler ultrasound to explore vascular complications after filler injection. Dermatol Surg. 2017, 43, 1508–1510. [Google Scholar]
- Fan, X.; Dong, M.; Li, T.; Ma, Q.; Yin, Y. Two cases of adverse reactions of hyaluronic acid-based filler injections. Plast Reconstr Surg Glob Open. 2016, 4, e1112. [Google Scholar]
- Kang, B.K.; Kang, I.J.; Jeong, K.H.; Shin, M.K. Treatment of glabella skin necrosis following injection of hyaluronic acid filler using platelet-rich plasma. J Cosmet Laser Ther. 2016, 18, 111–112. [Google Scholar] [PubMed]
- Kurkjian, T.J.; Ahmad, J.; Rohrich, R.J. Soft-tissue fillers in rhinoplasty. Plast Reconstr Surg. 2014, 133, 121e–126e. [Google Scholar]
- Darling, M.D.; Peterson, J.D.; Fabi, S.G. Impending necrosis after injection of hyaluronic acid and calcium hydroxylapatite fillers: report of 2 cases treated with hyperbaric oxygen therapy. Dermatol Surg. 2014, 40, 1049–1052. [Google Scholar] [PubMed]
- Banh, K. Facial ischemia after hyaluronic acid injection. J Emerg Med. 2013, 44, 169–170. [Google Scholar] [PubMed]
- Kim, S.G.; Kim, Y.J.; Lee, S.I.; Lee, C.J. Salvage of nasal skin in a case of venous compromise after hyaluronic acid filler injection using prostaglandin E. Dermatol Surg. 2011, 37, 1817–1819. [Google Scholar]
- Kassir, R.; Kolluru, A.; Kassir, M. Extensive necrosis after injection of hyaluronic acid filler: case report and review of the literature. J Cosmet Dermatol. 2011, 10, 224–231. [Google Scholar]
- Cox, S.E. Clinical experience with filler complications. Dermatol Surg. 2009, 35, 1661–1666. [Google Scholar]
- Hirsch, R.J.; Lupo, M.; Cohen, J.L.; Duffy, D. Delayed presentation of impending necrosis following soft tissue augmentation with hyaluronic acid and successful management with hyaluronidase. J Drugs Dermatol. 2007, 6, 325–328. [Google Scholar]
- Bellman, B.; Bellman, B. Complication following suspected intra-arterial injection of Restylane. Aesthet Surg J. 2006, 26, 304–305. [Google Scholar]
- Schanz, S.; Schippert, W.; Ulmer, A.; Rassner, G.; Fierlbeck, G. Arterial embolization caused by injection of hyaluronic acid (Restylane). Br J Dermatol. 2002, 146, 928–929. [Google Scholar] [CrossRef]
- Wang, Q.; Zhao, Y.; Li, H.; Li, P.; Wang, J. Vascular complications after chin augmentation using hyaluronic acid. Aesthetic Plast Surg. 2018, 42, 553–559. [Google Scholar] [CrossRef]
- Robati, R.M.; Moeineddin, F.; Almasi-Nasrabadi, M. The risk of skin necrosis following hyaluronic acid filler injection in patients with a history of cosmetic rhinoplasty. Aesthet Surg J. 2018, 38, 883–888. [Google Scholar]
- Zhang, C.; Ge, C.; Du, C.; Li, J. Local cooling as a step of treatment for tissue ischemia caused by hyaluronic acid injectioninduced embolism—a report of 9 cases. Plast Reconstr Surg Glob Open. 2018, 6, e1824. [Google Scholar] [CrossRef]
- Ciancio, F.; Tarico, M.S.; Giudice, G.; Perrotta, R.E. Early hyaluronidase use in preventing skin necrosis after treatment with dermal fillers: report of two cases. F1000 Res. 2018, 7, 1388. [Google Scholar]
- Hong, J.Y.; Seok, J.; Ahn, G.R.; Jang, Y.J.; Li, K.; Kim, B.J. Impending skin necrosis after dermal filler injection: a “golden time” for first-aid intervention. Dermatol Ther. 2017, 30, 1–4. [Google Scholar] [CrossRef]
- Andre, P.; Haneke, E. Nicolau syndrome due to hyaluronic acid injections. J Cosmet Laser Ther. 2016, 18, 239–244. [Google Scholar] [CrossRef]
- Sun, Z.S.; Zhu, G.Z.; Wang, H.B.; et al. Clinical outcomes of impending nasal skin necrosis related to nose and nasolabial fold augmentation with hyaluronic acid fillers. Plast Reconstr Surg. 2015, 136, e434–e441. [Google Scholar]
- Bravo, B.S.F.; De Almeida Balassiano, L.K.; Da Rocha, C.R.M.; et al. Delayed-type necrosis after soft-tissue augmentation with hyaluronic acid. J Clin Aesthet Dermatol. 2015, 8, 42–47. [Google Scholar]
- Lee, S.K.; Kim, S.M.; Cho, S.H.; Lee, J.D.; Kim, H.S. Adverse reactions to injectable soft tissue fillers: memorable cases and their clinico-pathological overview. J Cosmet Laser Ther. 2015, 17, 102–108. [Google Scholar]
- Grunebaum, L.D.; Bogdan Allemann, I.; Dayan, S.; Mandy, S.; Baumann, L. The risk of alar necrosis associated with dermal filler injection. Dermatol Surg. 2009, 35, 1635–1640. [Google Scholar]
- Kim, E.G.; Eom, T.K.; Kang, S.J. Severe visual loss and cerebral infarction after injection of hyaluronic acid gel. J Craniofac Surg. 2014, 25, 684–686. [Google Scholar]
- Chesnut, C. Restoration of visual loss with retrobulbar hyaluronidase injection after hyaluronic acid filler. Dermatol Surg. 2018, 44, 435–437. [Google Scholar]
- Hu, X.Z.; Hu, J.Y.; Wu, P.S.; Yu, S.B.; Kikkawa, D.O.; Lu, W. Posterior ciliary artery occlusion caused by hyaluronic acid injections into the forehead: a case report. Medicine (Baltimore). 2016, 95, e3124–e3124. [Google Scholar]
- Kwon, S.G.; Hong, J.W.; Roh, T.S.; Kim, Y.S.; Rah, D.K.; Kim, S.S. Ischemic oculomotor nerve palsy and skin necrosis caused by vascular embolization after hyaluronic acid filler injection: a case report. Ann Plast Surg. 2013, 71, 333–334. [Google Scholar]
- Lee, J.I.; Kang, S.J.; Sun, H. Skin necrosis with oculomotor nerve palsy due to a hyaluronic acid filler injection. Arch Plast Surg. 2017, 44, 340–343. [Google Scholar]
- Peter, S.; Mennel, S. Retinal branch artery occlusion following injection of hyaluronic acid (Restylane). Clin Exp Ophthalmol. 2006, 34, 363–364. [Google Scholar]
- Sharudin, S.N.; Ismail, M.F.; Mohamad, N.F.; Vasudevan, S.K. Complete recovery of filler-induced visual loss following subcutaneous hyaluronidase injection. Neuroophthalmology. 2019, 43, 102–106. [Google Scholar] [PubMed]
- Chen, Y.C.; Wu, H.M.; Chen, S.J.; et al. Intra-arterial thrombolytic therapy is not a therapeutic option for filler-related central retinal artery occlusion. Facial Plast Surg. 2018, 34, 325–329. [Google Scholar] [CrossRef]
- Chen, W.; Wu, L.; Jian, X.L.; et al. Retinal branch artery embolization following hyaluronic acid injection: a case report. Aesthet Surg J. 2016, 36, 219–224. [Google Scholar] [CrossRef]
- Ramesh, S.; Fiaschetti, D.; Goldberg, R.A. Orbital and ocular ischemic syndrome with blindness after facial filler injection. Ophthalmic Plast Reconstr Surg. 2018, 34, e108–e110. [Google Scholar] [CrossRef]
- He, M.-S.; Sheu, M.-M.; Huang, Z.-L.; Tsai, C.-H.; Tsai, R.-K. Sudden bilateral vision loss and brain infarction following cosmetic hyaluronic acid injection. JAMA Ophthalmol. 2013, 131, 1234–1235. [Google Scholar]
- Kim, Y.J.; Kim, S.S.; Song, W.K.; Lee, S.Y.; Yoon, J.S. Ocular ischemia with hypotony after injection of hyaluronic acid gel. Ophthalmic Plast Reconstr Surg. 2011, 27, e152–e155. [Google Scholar]
- Zhang, L.; Pan, L.; Xu, H.; et al. Clinical observations and the anatomical basis of blindness after facial hyaluronic acid injection. Aesthetic Plast Surg. 2019, 43, 1054–1060. [Google Scholar] [CrossRef]
- Thanasarnaksorn, W.; Cotofana, S.; Rudolph, C.; Kraisak, P.; Chanasumon, N.; Suwanchinda, A. Severe vision loss caused by cosmetic filler augmentation: case series with review of cause and therapy. J Cosmet Dermatol. 2018, 17, 712–718. [Google Scholar]
- Zhu, G.Z.; Sun, Z.S.; Liao, W.X.; et al. Efficacy of retrobulbar hyaluronidase injection for vision loss resulting from hyaluronic acid filler embolization. Aesthet Surg J. 2017, 38, 12–22. [Google Scholar]
- Kim, Y.K.; Jung, C.; Woo, S.J.; Park, K.H. Cerebral angiographic findings of cosmetic facial filler-related ophthalmic and retinal artery occlusion. J Korean Med Sci. 2015, 30, 1847–1855. [Google Scholar] [CrossRef]
- DeLorenzi, C. Transarterial degradation of hyaluronic acid filler by hyaluronidase. Dermatol Surg. 2014, 40, 832–841. [Google Scholar] [CrossRef]
- DeLorenzi, C. New high dose pulsed hyaluronidase protocol for hyaluronic acid filler vascular adverse events. Aesthet Surg J. 2017, 37, 814–825. [Google Scholar] [CrossRef]
- Kim, J.H.; Ahn, D.K.; Jeong, H.S.; Suh, I.S. Treatment algorithm of complications after filler injection: based on wound healing process. J Korean Med Sci. 2014, 29, S176–S182. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.I.; Palmer, J.H. The vascular territories (angiosomes) of the body: experimental study and clinical applications. Br J Plast Surg. 1987, 40, 113–141. [Google Scholar] [PubMed]
- Cavallini, M.; Gazzola, R.; Metalla, M.; Vaienti, L. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013, 33, 1167–1174. [Google Scholar]
- Kim, M.S.; Youn, S.; Na, C.H.; Shin, B.S. Allergic reaction to hyaluronidase use after hyaluronic acid filler injection. J Cosmet Laser Ther. 2015, 17, 283–285. [Google Scholar] [PubMed]
- Kim, D.W.; Yoon, E.S.; Ji, Y.H.; Park, S.H.; Lee, B.I.; Dhong, E.S. Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management. J Plast Reconstr Aesthet Surg. 2011, 64, 1590–1595. [Google Scholar]
- Goldan, O.; Georgiou, I.; Grabov-Nardini, G.; et al. Early and late complications after a nonabsorbable hydrogel polymer injection: a series of 14 patients and novel management. Dermatol Surg. 2007, 33, S199–S206. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
   |
 |
  |
© 2020 by the authors. The Authors 2020.
Share and Cite
Aviv, U.; Haik, J.; Weiss, N.; Berl, A.; Ofir, H.; Nardini, G.; Cleary, M.; Kornhaber, R.; Harats, M. Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience. Craniomaxillofac. Trauma Reconstr. 2020, 13, 313-328. https://doi.org/10.1177/1943387520952687
Aviv U, Haik J, Weiss N, Berl A, Ofir H, Nardini G, Cleary M, Kornhaber R, Harats M. Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience. Craniomaxillofacial Trauma & Reconstruction. 2020; 13(4):313-328. https://doi.org/10.1177/1943387520952687
Chicago/Turabian StyleAviv, Uri, Josef Haik, Nathaniel Weiss, Ariel Berl, Hagit Ofir, Gil Nardini, Michelle Cleary, Rachel Kornhaber, and Moti Harats. 2020. "Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience" Craniomaxillofacial Trauma & Reconstruction 13, no. 4: 313-328. https://doi.org/10.1177/1943387520952687
APA StyleAviv, U., Haik, J., Weiss, N., Berl, A., Ofir, H., Nardini, G., Cleary, M., Kornhaber, R., & Harats, M. (2020). Treatment Algorithm for Hyaluronic Acid-Related Complication Based on a Systematic Review of Case Reports, Case Series, and Clinical Experience. Craniomaxillofacial Trauma & Reconstruction, 13(4), 313-328. https://doi.org/10.1177/1943387520952687