Arthroscopic Eminoplasty of Temporomandibular Joint: Surgical Technique
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
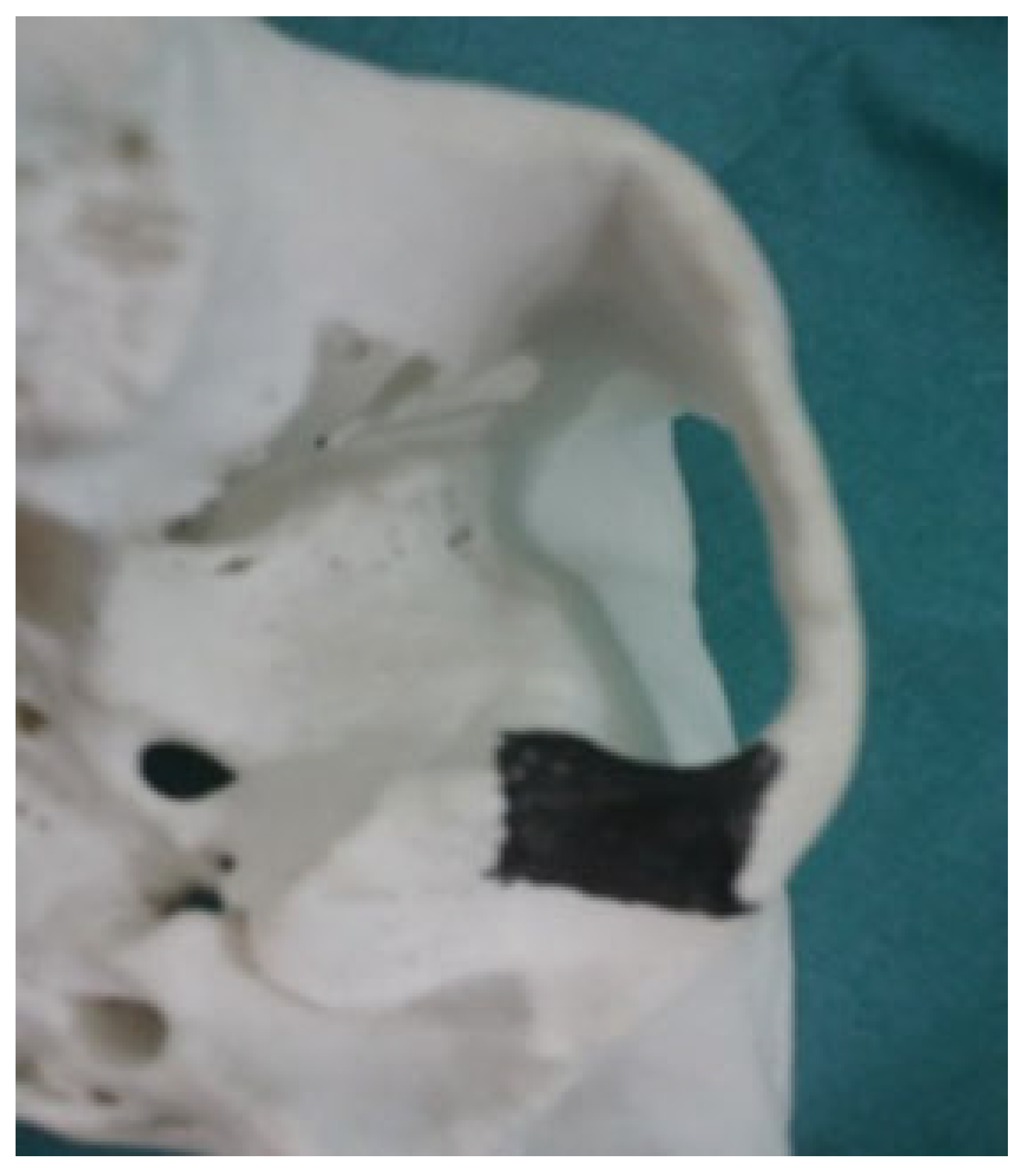
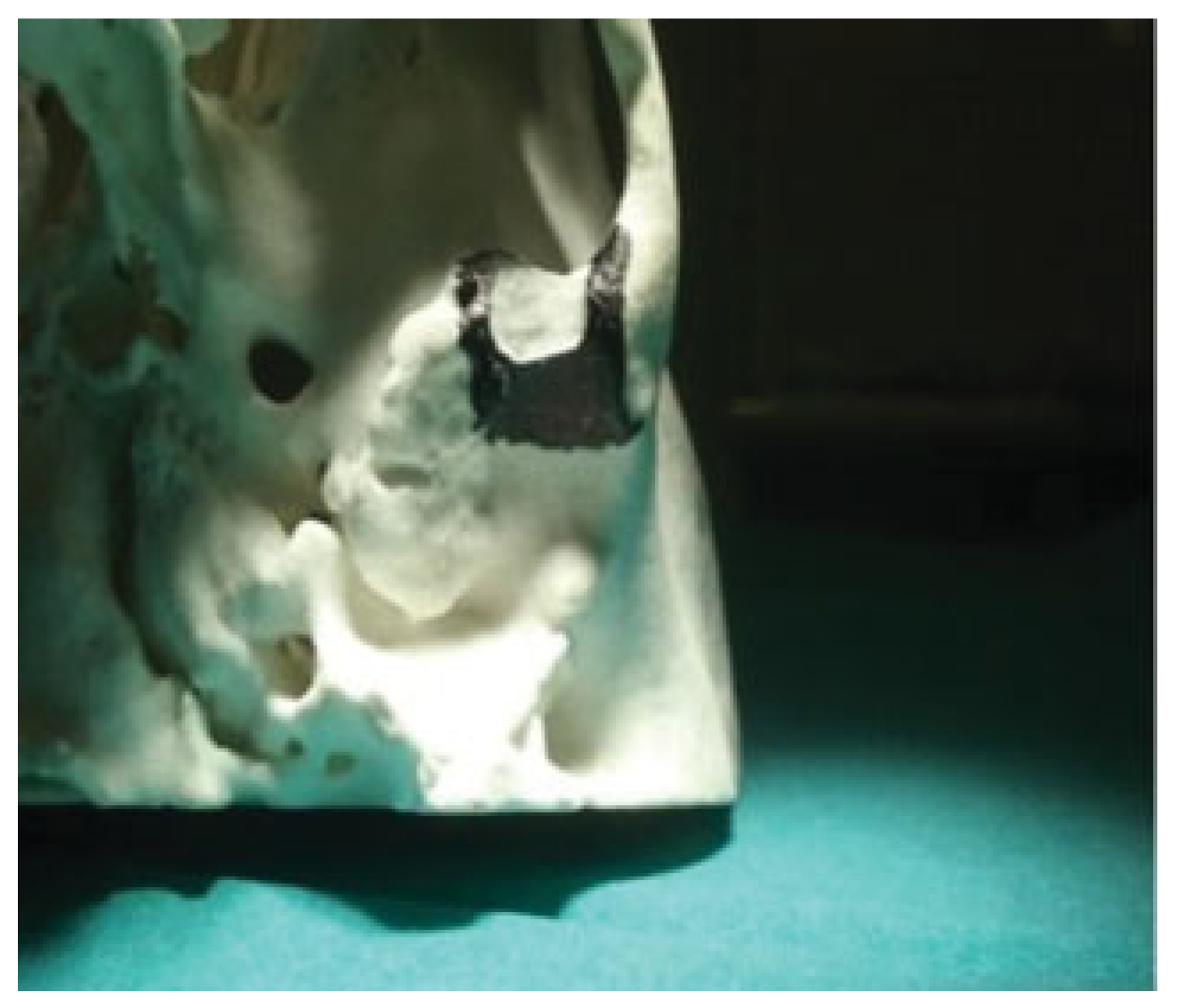
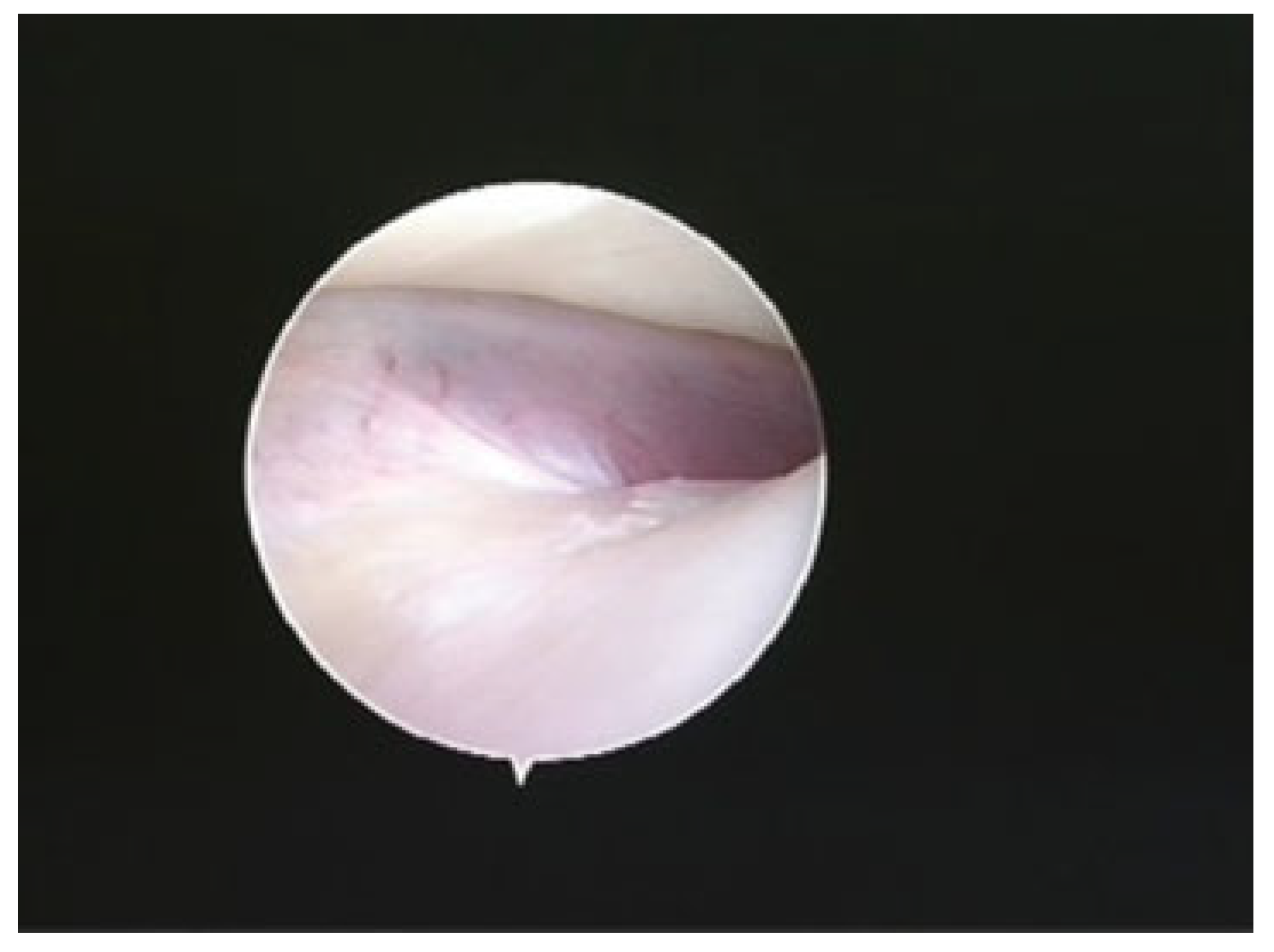
:Surgical Technique
Discussion
Funding
Conflicts of Interest
Ethical Standards
Authors’ Contributions
Informed Consent
References
- Ingawalé, S.; Goswami, T. Temporomandibular joint: Disorders, treatments, and biomechanics. Ann Biomed Eng 2009, 37, 976–996. [Google Scholar] [CrossRef] [PubMed]
- Segami, N.; Kaneyama, K.; Tsurusako, S.; Suzuki, T. Arthroscopic eminoplasty for habitual dislocation of the temporomandibular joint: Preliminary study. J Craniomaxillofac Surg 1999, 27, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Moses, J.J. Current concepts, rationale and techniques in TMJ arthroscopic surgery. J Oral Maxillofac Surg 2007, 65, 96. [Google Scholar] [CrossRef]
- Sato, J.; Segami, N.; Nishimura, M.; Suzuki, T.; Kaneyama, K.; Fujimura, K. Clinical evaluation of arthroscopic eminoplasty for habitual dislocation of the temporomandibular joint: Comparative study with conventional open eminectomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003, 95, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Tsuyama, M.; Kondoh, T.; Seto, K.; Fukuda, J. Complications of temporomandibular joint arthroscopy: A retrospective analysis of 301 lysis and lavage procedures performed using the triangulation technique. J Oral Maxillofac Surg 2000, 58, 500–505, discussion 505–506. [Google Scholar] [CrossRef] [PubMed]
- Undt, G. Temporomandibular joint eminectomy for recurrent dislocation. Atlas Oral Maxillofac Surg Clin North Am 2011, 19, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.M.; Chiaravalloti, G.; Iwasaki, L.R.; Nickel, J.C.; Palla, S. Mechanical work during stress-field translation in the human TMJ. J Dent Res 2006, 85, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Cascone, P.; Ungari, C.; Paparo, F.; Marianetti, T.M.; Ramieri, V.; Fatone, M. A new surgical approach for the treatment of chronic recurrent temporomandibular joint dislocation. J Craniofac Surg 2008, 19, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Wolford, L.M. Clinical indications for simultaneous TMJ and orthognathic surgery. Cranio 2007, 25, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Garcia Medina, B.; Cariati, P.; Galvez, P.; Cabello Serrano, A.; Garcia Martin, M. Arthroscopic eminoplasty: A new choice of treatment for TMJ internal derangement. Minerva Stomatol 2017, 66, 141–147. [Google Scholar] [CrossRef] [PubMed]

© 2018 by the author. The Author(s) 2018.
Share and Cite
Cariati, P.; Garcia Medina, B.; Galvez, P.; Cabello Serrano, A.; Garcia Martin, M.; Valencia Moya, G. Arthroscopic Eminoplasty of Temporomandibular Joint: Surgical Technique. Craniomaxillofac. Trauma Reconstr. 2018, 11, 161-164. https://doi.org/10.1055/s-0038-1639349
Cariati P, Garcia Medina B, Galvez P, Cabello Serrano A, Garcia Martin M, Valencia Moya G. Arthroscopic Eminoplasty of Temporomandibular Joint: Surgical Technique. Craniomaxillofacial Trauma & Reconstruction. 2018; 11(2):161-164. https://doi.org/10.1055/s-0038-1639349
Chicago/Turabian StyleCariati, Paolo, Blas Garcia Medina, Pablo Galvez, Almudena Cabello Serrano, Miguel Garcia Martin, and Guillermo Valencia Moya. 2018. "Arthroscopic Eminoplasty of Temporomandibular Joint: Surgical Technique" Craniomaxillofacial Trauma & Reconstruction 11, no. 2: 161-164. https://doi.org/10.1055/s-0038-1639349
APA StyleCariati, P., Garcia Medina, B., Galvez, P., Cabello Serrano, A., Garcia Martin, M., & Valencia Moya, G. (2018). Arthroscopic Eminoplasty of Temporomandibular Joint: Surgical Technique. Craniomaxillofacial Trauma & Reconstruction, 11(2), 161-164. https://doi.org/10.1055/s-0038-1639349