Multi-Institutional Analysis of Surgical Management and Outcomes of Mandibular Fracture Repair in Adults
Abstract
:Methods
Statistics
Results
Discussion
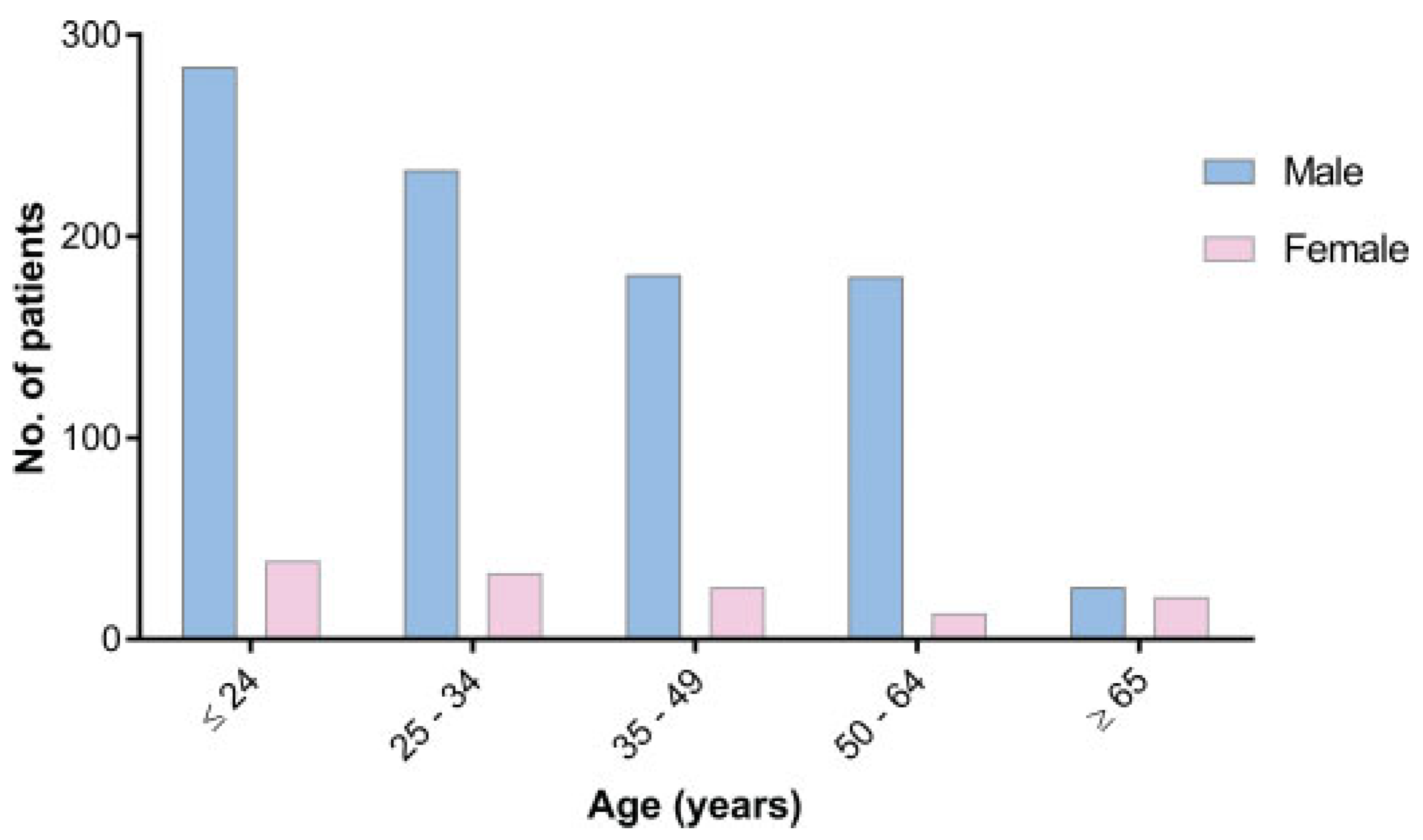
Which Patients Present with Mandibular Fractures?
Treatment of Open versus Closed Fracture: Does It Make a Difference?
Choice of Operative Technique
Complications from Mandibular Fractures
Conclusions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Ferreira, P.C.; Amarante, J.M.; Silva, P.N.; et al. Retrospective study of 1251 maxillofacial fractures in children and adolescents. Plast Reconstr Surg 2005, 115, 1500–1508. [Google Scholar]
- Moura, L.B.; Gabrielli, M.F.; Gabrielli, M.A.; Filho, V.A. Pathologic mandibular fracture as first sign of multiple myeloma. J Craniofac Surg 2016, 27, e138–e139. [Google Scholar]
- Afrooz, P.N.; Bykowski, M.R.; James, I.B.; Daniali, L.N.; Clavijo-Alvarez, J.A. The epidemiology of mandibular fractures in the United States, Part 1: A review of 13,142 cases from the US National Trauma Data Bank. J Oral Maxillofac Surg 2015, 73, 2361–2366. [Google Scholar] [PubMed]
- Morris, C.; Bebeau, N.P.; Brockhoff, H.; Tandon, R.; Tiwana, P. Mandibular fractures: An analysis of the epidemiology and patterns of injury in 4,143 fractures. J Oral Maxillofac Surg 2015, 73, 951.e1–951.e12. [Google Scholar] [PubMed]
- Murray, J.M. Mandible fractures and dental trauma. Emerg Med Clin North Am 2013, 31, 553–573. [Google Scholar] [PubMed]
- Kruger, E.; Tennant, M. Fractures of the mandible and maxilla: A 10-year analysis. Australas Med J 2016, 9, 17–24. [Google Scholar]
- Atilgan, S.; Erol, B.; Yaman, F.; Yilmaz, N.; Ucan, M.C. Mandibular fractures: A comparative analysis between young and adult patients in the southeast region of Turkey. J Appl Oral Sci 2010, 18, 17–22. [Google Scholar]
- Banks, P.; Brown, A. Fractures of the Facial Skeleton; Wright: Oxford, UK, 2001. [Google Scholar]
- Infante Cossio, P.; Espin Galvez, F.; Gutierrez Perez, J.L.; Garcia-Perla, A.; Hernandez Guisado, J.M. Mandibular fractures in children. A retrospective study of 99 fractures in 59 patients. Int J Oral Maxillofac Surg 1994, 23 Pt 1, 329–331. [Google Scholar]
- Cole, P.; Kaufman, Y.; Izaddoost, S.; Hatef, D.A.; Hollier, L. Principles of pediatric mandibular fracture management. Plast Reconstr Surg 2009, 123, 1022–1024. [Google Scholar]
- Goth, S.; Sawatari, Y.; Peleg, M. Management of pediatric mandible fractures. J Craniofac Surg 2012, 23, 47–56. [Google Scholar]
- Hackenberg, B.; Lee, C.; Caterson, E.J. Management of subcondylar mandible fractures in the adult patient. J Craniofac Surg 2014, 25, 166–171. [Google Scholar] [PubMed]
- Alpert, B.; Kushner, G.M.; Tiwana, P.S. Contemporary management of infected mandibular fractures. Craniomaxillofac Trauma Reconstr 2008, 1, 25–29. [Google Scholar] [PubMed]
- Burm, J.S.; Hansen, J.E. The use of microplates for internal fixation of mandibular fractures. Plast Reconstr Surg 2010, 125, 1485–1492. [Google Scholar] [PubMed]
- Rémi, M.; Christine, M.C.; Gael, P.; Soizick, P.; Joseph-André, J. Mandibular fractures in children: Long term results. Int J Pediatr Otorhinolaryngol 2003, 67, 25–30. [Google Scholar]
- American College of Surgeons. ACS NSQIP Participant Use Data File. 2014. Available online: https://www.facs.org/~/media/files/quality%20programs/nsqip/nsqip_puf_userguide_2014.ashx (accessed on 13 November 2016).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 9th ed.; World Health Organization: New York, NY, USA, 1977. [Google Scholar]
- American Association of Medical Colleges. Physician Specialty Data Book. 2014. Available online: https://members.aamc.org/eweb/upload/Physician%20Specialty%20Databook%202014.pdf (accessed on 13 November 2016).
- Kelley, P.; Crawford, M.; Higuera, S.; Hollier, L.H. Two hundred ninetyfour consecutive facial fractures in an urban trauma center: Lessons learned. Plast Reconstr Surg 2005, 116, 42e–49e. [Google Scholar]
- Azevedo, A.B.; Trent, R.B.; Ellis, A. Population-based analysis of 10,766 hospitalizations for mandibular fractures in California, 1991 to 1993. J Trauma 1998, 45, 1084–1087. [Google Scholar]
- Nasser, M.; Pandis, N.; Fleming, P.S.; Fedorowicz, Z.; Ellis, E.; Ali, K. Interventions for the management of mandibular fractures. Cochrane Database Syst Rev 2013, 2013, CD006087. [Google Scholar]
- Boffano, P.; Kommers, S.C.; Roccia, F.; Forouzanfar, T. Mandibular trauma treatment: A comparison of two protocols. Med Oral Patol Oral Cir Bucal 2015, 20, e218–e223. [Google Scholar]
- Boffano, P.; Kommers, S.C.; Karagozoglu, K.H.; Gallesio, C.; Forouzanfar, T. Mandibular trauma: A two-centre study. Int J Oral Maxillofac Surg 2015, 44, 998–1004. [Google Scholar]
- Serena-Gómez, E.; Passeri, L.A. Complications of mandible fractures related to substance abuse. J Oral Maxillofac Surg 2008, 66, 2028–2034. [Google Scholar]
- Boffano, P.; Roccia, F.; Zavattero, E.; et al. European Maxillofacial Trauma (EURMAT) project: A multicentre and prospective study. J Craniomaxillofac Surg 2015, 43, 62–70. [Google Scholar] [PubMed]
- Le, B.T.; Holmgren, E.P.; Holmes, J.D.; Ueeck, B.A.; Dierks, E.J. Referral patterns for the treatment of facial trauma in teaching hospitals in the United States. J Oral Maxillofac Surg 2003, 61, 557–560. [Google Scholar]
- Kanno, T.; Sukegawa, S.; Nariai, Y.; et al. Surgical treatment of comminuted mandibular fractures using a low-profile locking mandibular reconstruction plate system. Ann Maxillofac Surg 2014, 4, 144–149. [Google Scholar] [PubMed]
- Furr, A.M.; Schweinfurth, J.M.; May, W.L. Factors associated with longterm complications after repair of mandibular fractures. Laryngoscope 2006, 116, 427–430. [Google Scholar] [PubMed]
- Gokkulakrishnan, S.; Singh, S.; Sharma, A.; Shahi, A.K. An analysis of postoperative complications and efficacy of 3D miniplates in fixation of mandibular fractures. Dent Res J 2012, 9, 414–421. [Google Scholar]
- Plaisier, B.R.; Punjabi, A.P.; Super, D.M.; Haug, R.H. The relationship between facial fractures and death from neurologic injury. J Oral Maxillofac Surg 2000, 58, 708–712, Discussion 712–713. [Google Scholar]

{kind=link}
| Variable | Total Fractures (n = 940) Cases, % Of Total | Closed Fractures (n = 750) Cases, % of Total | Open Fractures (n = 190) Cases, % of Total | p-Value |
|---|---|---|---|---|
| Age (mean ± SD) | 34.0 ± 14.8 | 34.5 ± 15.0 | 32.1 ± 13.8 | 0.050 |
| Sex | ||||
| Male | 805 (85.7) | 644 (85.9) | 161 (84.7) | 0.800 |
| Female | 134 (14.3) | 105 (14.0) | 29 (15.3) | 0.800 |
| BMI (mean ± SD) | 23.6 ± 8.2 | 23.3 ± 8.3 | 24.6 ± 7.5 | 0.063 |
| Race | ||||
| White | 455 (48.4) | 366 (51.5) | 89 (47.8) | 0.403 |
| Black | 219 (23.3) | 171 (24.1) | 48 (25.8) | |
| Asian | 15 (1.6) | 11 (1.5) | 4 (2.2) | |
| Hawaiian or Pacific Islander | 11 (1.2) | 8 (1.1) | 3 (1.6) | |
| Native American | 9 (1.0) | 5 (0.7) | 4 (2.2) | |
| Unknown | 231 (24.6) | 189 (25.2) | 42 (22.1) | |
| Clinical factors | ||||
| Smoker | 480 (51.1) | 397 (52.9) | 83 (43.7) | 0.023 a |
| Regular alcohol use b | 51 (5.4) | 40 (5.3) | 11 (5.8) | 0.889 |
| Steroid use | 3 (0.3) | 2 (0.3) | 1 (0.5) | 0.571 |
| Comorbidities | ||||
| Diabetes | 32 (3.4) | 26 (3.5) | 6 (3.2) | 0.834 |
| Hypertension | 109 (11.6) | 89 (11.9) | 20 (10.5) | 0.606 |
| Bleeding disorder | 10 (1.1) | 9 (1.2) | 1 (0.5) | 0.419 |
| Pulmonary history | 9 (1.0) | 7 (0.9) | 2 (1.1) | 0.880 |
| Cardiac history | 8 (0.9) | 7 (0.9) | 1 (0.5) | 0.585 |
| Renal history | 3 (0.3) | 3 (0.4) | 0 (0.0) | 0.383 |
| Neurologic history | 8 (0.9) | 8 (1.1) | 0 (0.0) | 0.153 |
| Variable | Total fractures (n = 940) Cases, % of total | Closed fractures (n = 750) Cases, % of total | Open fractures (n = 190) Cases, % of total | p-Value |
|---|---|---|---|---|
| Procedure type (top 5) | ||||
| Open treatment of mandibular fracture, with interdental fixation | 431 (45.9) | 347 (46.3) | 84 (44.2) | 0.578 |
| Open treatment of complicated mandibular fracture by multiple surgical approaches including internal fixation, interdental fixation, and/or wiring of dentures or splints | 235 (25.0) | 178 (23.7) | 57 (30.0) | |
| Open treatment of mandibular fracture, without interdental fixation | 105 (11.2) | 86 (11.5) | 19 (10.0) | |
| Open treatment of mandibular fracture, with external fixation | 27 (2.9) | 24 (3.2) | 3 (1.6) | |
| Open treatment of mandibular or maxillary alveolar ridge fracture | 24 (2.6) | 18 (2.4) | 6 (3.2) | |
| Emergency case | 141 (15.0) | 99 (13.2) | 42 (22.1) | 0.002 a |
| Inpatient | 431 (45.9) | 328 (43.7) | 103 (54.2) | 0.010 a |
| ASA classification | ||||
| Class 1 | 265 (28.2) | 208 (27.7) | 57 (30.0) | 0.601 |
| Class 2 | 528 (56.2) | 421 (56.1) | 107 (56.3) | |
| Class 3 | 142 (15.1) | 116 (15.5) | 26 (13.7) | |
| Class 4 | 5 (0.5) | 5 (0.7) | 0 (0.0) | |
| Operative time, minutes (mean ± SD) | 126.9 ± 72.8 | 122.6 ± 68.8 | 143.72 ± 84.9 | <0.001 a |
| Hospitalization length of stay, days (mean ± SD, median) | 1.3 ± 4.2, 1.0 | 1.3 ± 2.4, 1.0 | 1.3 ± 8.0, 1.0 | 0.875 |
| Specialty | ||||
| Otolaryngology | 588 (62.6) | 464 (61.9) | 124 (65.3) | 0.849 |
| Plastic surgery | 321 (34.1) | 260 (34.7) | 61 (32.1) | |
| Other | 31 (3.3) | 26 (3.4) | 5 (2.6) | |
| Outcome | Total Fractures (n = 940) Cases, % of Total | Closed Fractures (n = 750) Cases, % of Total | Open Fractures (n = 190) Cases, % of Total | p-Value |
|---|---|---|---|---|
| Medical complication | 16 (1.7) | 11 (1.5) | 5 (2.6) | 0.267 |
| Pulmonary | 9 (1.0) | 6 (0.8) | 3 (1.6) | 0.325 |
| Reintubation | 3 (0.3) | 2 (0.3) | 1 (0.5) | 0.571 |
| Failure to wean off ventilator within 48 h | 5 (0.5) | 3 (0.4) | 2 (1.1) | 0.269 |
| Cardiovascular | 2 (0.2) | 2 (0.3) | 0 (0.0) | 0.476 |
| Renal | 5 (0.5) | 3 (0.4) | 2 (1.1) | 0.269 |
| Hematologic | 2 (0.2) | 1 (0.1) | 0 (0.0) | 0.615 |
| Infectious | 3 (0.3) | 2 (0.3) | 1 (0.5) | 0.571 |
| Surgical complication | 35 (3.7) | 30 (4.0) | 5 (2.6) | 0.374 |
| Wound class | ||||
| 1: Clean | 115 (12.2) | 98 (13.1) | 17 (8.9) | <0.001 |
| 2: Clean/Contaminated | 704 (74.9) | 570 (76.0) | 134 (70.5) | |
| 3: Contaminated | 81 (8.6) | 60 (8.0) | 21 (11.1) | |
| 4: Dirty/Infected | 40 (4.3) | 22 (2.9) | 18 (9.5) | |
| Readmission | 21 (2.2) | 17 (2.3) | 4 (2.1) | 0.893 |
| Reoperation | 12 (1.3) | 11 (1.5) | 1 (0.5) | 0.302 |
| Mortality | 1 (0.1) | 1 (0.1) | 0 (0.0) | 0.615 |
| Variable | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.02 | 0.99–1.06 | 0.240 |
| ASA 3 or higher | 8.65 | 2.19–34.14 | 0.002 a |
| Open | 1.93 | 0.60–6.26 | 0.273 |
| Operative time | 1.00 | 0.99–1.01 | 0.958 |
| Emergency case | 3.62 | 1.12–11.73 | 0.032 a |
| Smoker | 0.72 | 0.24–2.14 | 0.552 |
| Variable | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.02 | 0.99–1.04 | 0.188 |
| ASA 3 or higher | 0.90 | 0.34–2.61 | 0.907 |
| Open | 0.73 | 0.28–1.93 | 0.525 |
| Operative time | 1.00 | 0.99–1.00 | 0.709 |
| Emergency case | 0.51 | 0.18–1.95 | 0.383 |
| Smoker | 1.28 | 0.64–2.56 | 0.478 |
© 2017 by the author. The Author(s) 2017.
Share and Cite
Zavlin, D.; Jubbal, K.T.; Echo, A.; Izaddoost, S.A.; Friedman, J.D.; Olorunnipa, O. Multi-Institutional Analysis of Surgical Management and Outcomes of Mandibular Fracture Repair in Adults. Craniomaxillofac. Trauma Reconstr. 2018, 11, 41-48. https://doi.org/10.1055/s-0037-1603460
Zavlin D, Jubbal KT, Echo A, Izaddoost SA, Friedman JD, Olorunnipa O. Multi-Institutional Analysis of Surgical Management and Outcomes of Mandibular Fracture Repair in Adults. Craniomaxillofacial Trauma & Reconstruction. 2018; 11(1):41-48. https://doi.org/10.1055/s-0037-1603460
Chicago/Turabian StyleZavlin, Dmitry, Kevin T. Jubbal, Anthony Echo, Shayan A. Izaddoost, Jeffrey D. Friedman, and Olushola Olorunnipa. 2018. "Multi-Institutional Analysis of Surgical Management and Outcomes of Mandibular Fracture Repair in Adults" Craniomaxillofacial Trauma & Reconstruction 11, no. 1: 41-48. https://doi.org/10.1055/s-0037-1603460
APA StyleZavlin, D., Jubbal, K. T., Echo, A., Izaddoost, S. A., Friedman, J. D., & Olorunnipa, O. (2018). Multi-Institutional Analysis of Surgical Management and Outcomes of Mandibular Fracture Repair in Adults. Craniomaxillofacial Trauma & Reconstruction, 11(1), 41-48. https://doi.org/10.1055/s-0037-1603460