Abstract
The aim of this article is to evaluate the efficacy of a single second-generation headless compression screw along with a lower arch bar in the fixation of interforaminal mandible fractures. A total of seven patients were included in the study. An open approach was used either intraorally or extraorally. A second-generation 3.0 HCS (headless compression screw), 24 to 32 mm in length, diameter at the head of 3.5 mm, smooth shaft with 2.0 mm and at the leading edge 3.0 mm (Synthes, Paoli, PA) was used for the fixation along with a lower arch bar. Postoperative clinical and radiographic follow-up was performed at 3 weeks, 3 months, 6 months, and 1 year. A single, cannulated HCS was found to be effective in fixation of interforaminal mandible fractures except in one case where a miniplate had to be applied subapically. Clinical and radiographic follow-up revealed accurate reduction and fixation in all cases and no postoperative occlusal disturbances. A single, second-generation HCS along with a lower arch bar provides good results when used for the fixation of interforaminal mandible fractures. Headless compression screw fixation of interforaminal mandible fracture is a simple, quick, economic, and efficient method of rigid fixation with minimum complications.
The concept of bone plating has changed overtime, with the introduction of various modifications; sequentially, bone plates such as compression plate, dynamic compression plate (DCP), eccentric dynamic compression plate (EDCP), miniplates, and microplates have been introduced, but miniplates are the ones most commonly used [1]. The modalities for treatment of mandibular interforaminal fractures (fractures of mandible between the two mental foramina) have evolved based on the most recent scientific advances. Champy advised the use of two miniplates in the interforaminal region, one at inferior border and the other 5 mm above the lower plate [2]. This principle is still followed, but the need for two miniplates in the interforaminal region is questioned, when lower arch bar is also placed simultaneously for intra- or postoperative intermaxillary fixation. The lower arch bar placed for intraoperative or postoperative intermaxillary fixation itself acts as a tension band and the subapical miniplate (tension band plate) can be eliminated [3].
The installation of lag screw involves a greater surgical difficulty than the use of miniplates. On the other hand, lag screws have been associated with more technique sensitivity, lower complication rates, and more resistance to compression than miniplates in mechanical tests [3,4].
Filan and Herbert designed a single piece noncannulated headless compression screw (HCS) to provide internal compression and stability of the fracture while avoiding any prominence of metal on the bone surface. Initially, they were designed to internally fix displaced, small bone fractures like scaphoid [5]. Whipple modified the Herbert screw by developing a cannulated version for more accurate screw placement. Multiple manufactures are now offering newer or secondgeneration HCS (SG-HCS) [6]. HCSs were initially designed to internally fix displaced small bone fractures like scaphoid nonunion, capitellum, and also osteotomies of hallux valgus correction of tarsal bones [7]. These screws embody slight design modification that have been purported to improve biomechanical characteristics. The compression forces in the screw are generated by pitch difference between the narrow trailing thread and the wide leading thread. Fixation of fracture of the interforaminal region of mandible has been a long-standing topic of discussion in maxillofacial surgery and debate continues regarding the ideal treatment method [3].
The use of cannulated bone screws has not been described in literature for the fixation of interforaminal fractures of the mandible till now. The absence of any important vascular or neural anatomical structures in this area makes it well suited for placement of a screw. The curvature of the interforaminal region of the mandible allows for the accommodation of the entire length of the screw in the bone, which holds true for sagittal and oblique fractures. Thick bony cortex in this region ensures secure subcortical placement and rigid fixation of the screw [8].
In the maxillofacial region, cannulated screws have been used to fix intracapsular dicapitular fractures of the mandibular condyle [9,10]. In a mechanical and photoelastic study performed by Falci et al, cannulated bone screws were used and results were comparable to those achieved by lag screws for the fixation of interforaminal mandible fractures [11]. Ellis and Ghali treated seven patients with interforaminal mandible fractures using a singlelag screwalong with lower arch bar and bridle wire with no complications [8]. According to a study by Emam and Stevens, a single lag screw used along with lower arch bar was enough to provide rigidity and to oppose rotational forces in interforaminal mandible fractures [12].
The purpose of this study was to assess the efficacy of a single SG-HCS along with a lower arch bar in the fixation of mandibular interforaminal fractures.
Patients and Methods
This study was undertaken in the Department of Oral and Maxillofacial Surgery between August 2014 to May 2015 and follow-up was done till May 2016 after approval from the institutional ethical committee. All the patients were operated by a single surgeon with an experience of 9 years postresidency.
A total of seven patients aged between 21 and 32 years were included in the study. Postoperative clinical and radiographic follow-up was performed at 3 weeks, 3 months, 6 months, and 1 year in all the patients and there were no dropouts from the study. All the patients were explained about the procedure and written consents were obtained prior to surgery.
All the patients included in the study had sustained an interforaminal fracture of mandible with a clearly perceptible step deformity. Patients with associated facial fractures (mandibular condyle, mandibular angle, or midface) were also included in the study, provided they were managed by open reduction and internal fixation. Patients were excluded from the study if they had an (1) atrophic, edentulous mandible, (2) severely comminuted interforaminal fracture of the mandible, (3) infected fractures of the interforaminal region of mandible, and (4) systemic conditions which would interfere with soft-tissue and bone healing (AIDS, diabetes mellitus, etc.), as well as (5) who are unwilling/unable to come for follow-up.
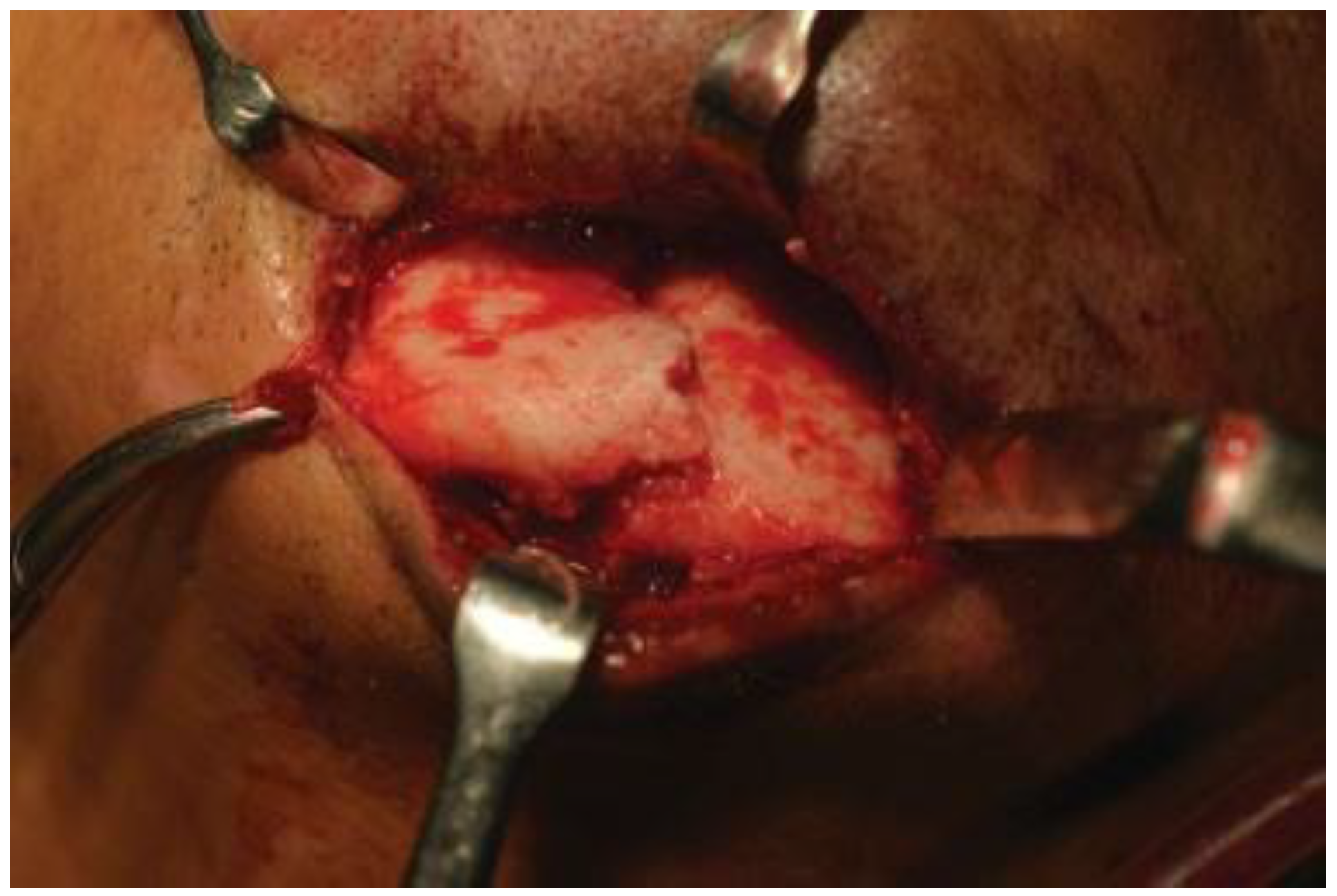
We used a second-generation 3.0 HCS, 24 to 32 mm in length, diameter at the trailing edge of 3.5 mm, smooth shaft with 2.0 mm and at the leading edge 3.0 mm (Synthes Paoli, PA; Figure 1). Patients were operated under local anesthesia or general anesthesia according to the extent of associated injuries and need for their fixation. Part to be operated was prepared with betadine solution and was infiltrated with lignocaine and adrenaline (1:80,000) concentration. An intraoral gingivobuccal/gingivolabial approach or extraoral approach through an existing laceration was taken and careful dissection was done to expose the fracture site (Figure 2 and Figure 3). Fracture segments were reduced along with performing intraoperative intermaxillary fixation to ensure accurate occlusion. The next step is to carefully drill a guiding hole with a 2.5-mm drill bit in the distal fracture fragment. Hand drilling is now commenced with a hollow 2.5-mm drill bit while maintaining the coaxiality in the distal and proximal fragment with the help of a K-wire. The HCS is inserted into the guiding hole along the K-wire with the help of a cannulated T8 StarDrive screwdriver. The screwdriver is engaged and the screw is inserted into the bone using the compression sleeve construct. Both ends of the screw are accommodated in the buccal cortical plate which is necessary to gain interfragmentary compression. When the tip of the compression sleeve contacts the bone, the fracture gap is closed and compressed, and the countersink is performed by holding the compression sleeve stationary and advancing the screw into the bone (Figure 4 and Figure 5). Clinical stability of fixation of fracture was checked intraoperatively by performing labiolingual and superior–inferior movements between the two fracture fragments.
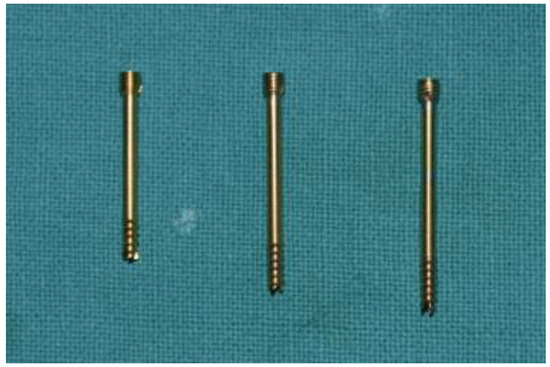
Figure 1.
Second-generation 3.0 headless compression screw 24, 28, and 32 mm in length.
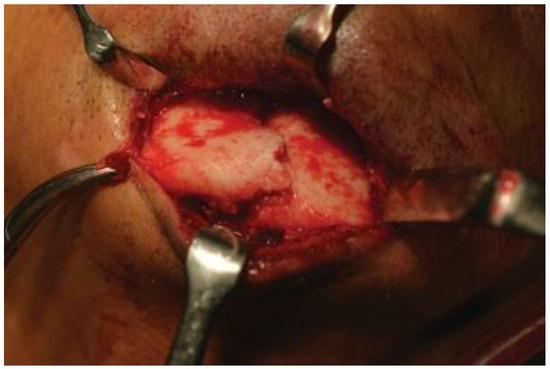
Figure 2.
Case 1: Intraoperative photograph of interforaminal mandible fracture exposed extraorally through an existing laceration.

Figure 3.
Case 2: Intraoperative photograph of interforaminal mandible fracture exposed extraorally through an existing laceration.

Figure 4.
Case 1: Intraoperative photograph of interforaminal mandible fracture reduced and fixed with a headless compression screw.

Figure 5.
Case 2: Intraoperative photograph of interforaminal mandible fracture reduced and fixed with a headless compression screw.
Postoperative intermaxillary was not done in any of the cases. The lower arch bar was left in situ for a period of 6 weeks in all patients. Postoperative clinical and radiographic follow-up was done in all patients for a period of 1 year (Figure 13b).
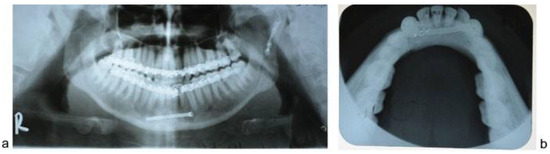
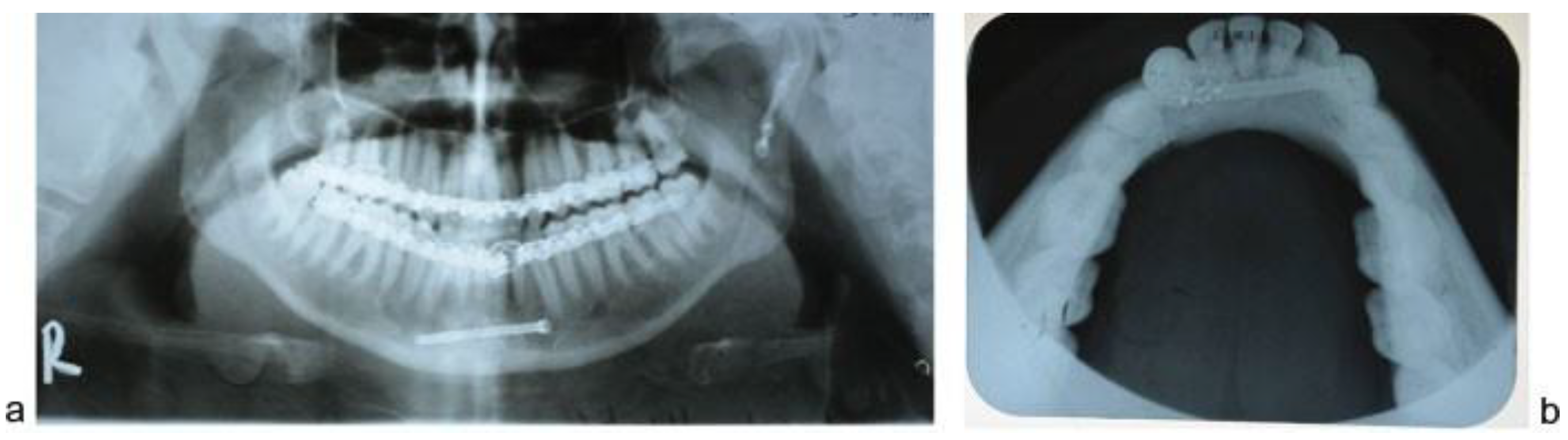
Figure 13.
(a) Case 2: Postoperative orthopantomograph showing interforaminal mandible fracture reduced and fixed with a single headless compression screw. (b) Case 1: Mandibular occlusal radiograph taken at 6 months follow-up showing the position of headless compression screw and healed fracture of the interforaminal region of the mandible.
The objectives of the study were to clinically assess fixation and reduction of fracture fragments radiographically, discrepancy in the occlusion, mental nerve injury, evidence of infection at the operated site, intraoperative time taken for the procedure, and lower border malalignment. Clinical assessment of fixation was done intraoperatively by performing labiolingual and superior–inferior movements in opposite directions between the two fracture fragments. Clinical intraoperative assessment was performed by the operating surgeon and was graded as good, moderate, or poor. Radiographic assessment of reduction was done on orthopantomograph and CT scan by a surgeon with an experience of 11 years postresidency from the Department of Plastic Surgery who was blinded to the identity of the operating surgeon to avoid bias. It was also graded as good, moderate, or poor.
We used cotton wisp test to determine mental nerve injury. The patient was asked to sit up straight and keep both their eyes closed. The cotton wisp was contacted to the lower lip and chin on the concerned side to check function of mental nerve on that side. Mental nerve injury was noted as present or absent. Intraoperative time taken was calculated as the time taken for incision, exposure, reduction, fixation, and closure of the interforaminal mandible fracture. Lower border malalignment was noted as present or absent as observed on the orthopantomograph.
Results
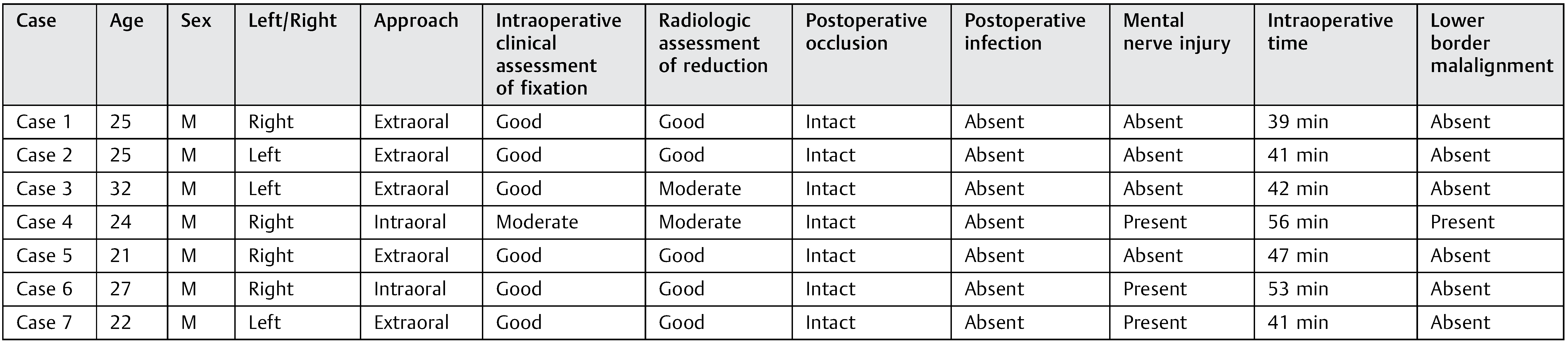
All the patients enrolled in the study were males aged 21 to 32 years with an average of 25.14 years (Table 1). All cases were approached extraorally through an existing laceration except two, which were approached through a gingivobuccal incision intraorally. Average intraoperative time taken was 45.57 minutes.

Table 1.
Details of patients and results obtained.
Intraoperative clinical stability was achieved in all patients and was graded as good except one in which a single miniplate was used subapically to counteract tension forces and was graded as moderate. Postoperative dental occlusion was achieved in all the patients and no intermaxillary fixation required postoperatively. Postoperative wound healing was uneventful in all the patients. Evidence of mental nerve injury was present in three cases postoperatively but was transient in nature and disappeared on the third week follow-up in one case and after 3 months postoperatively in two cases.
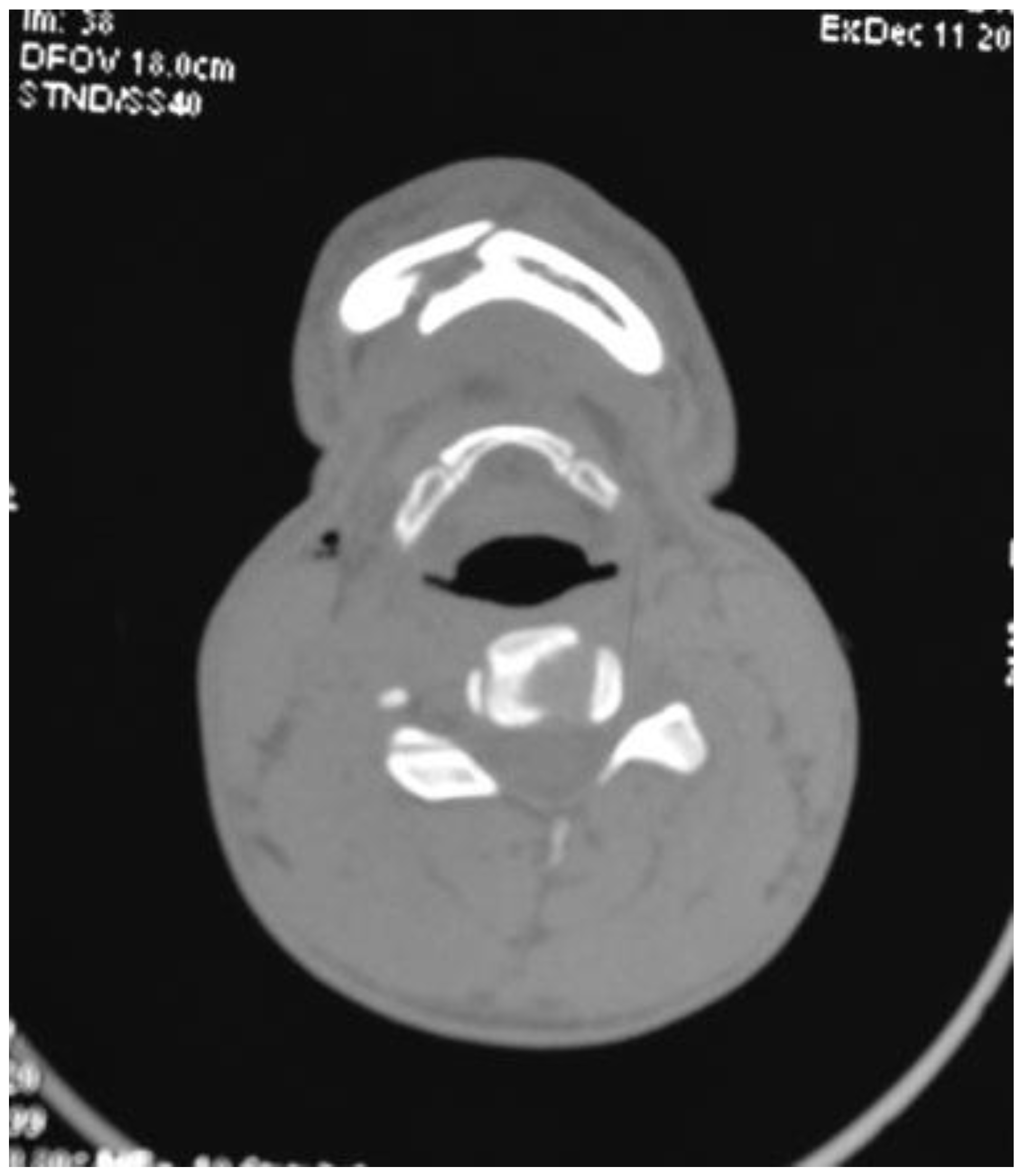
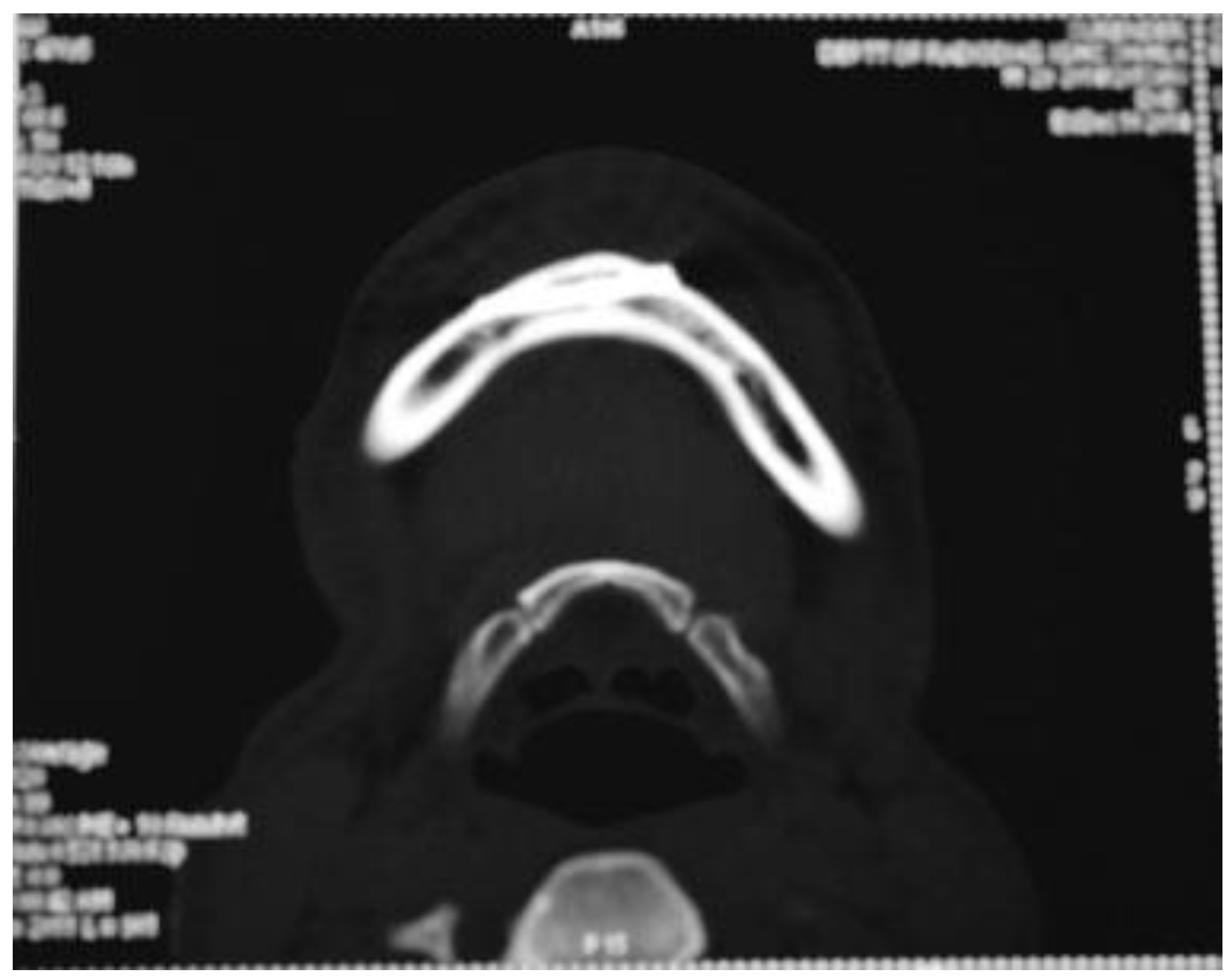
Six out of seven patients showed good anatomical reduction on postoperative CT scans (Figure 6, Figure 7, Figure 8 and Figure 9) and orthopan-tomograph (Figure 10, Figure 11, Figure 12 and Figure 13). On regular follow-up at 3 weeks, 3 months, and 6 months, and 1 year, no evidence of wound dehiscence, discrepancy in occlusion, or lower border malalignment was seen (Figure 14).
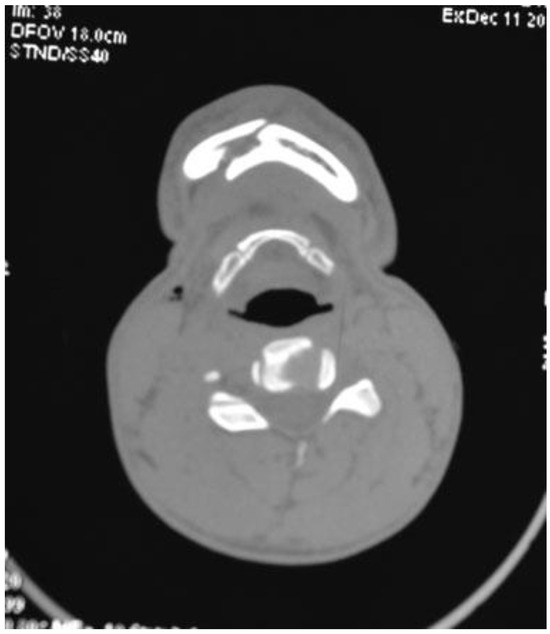
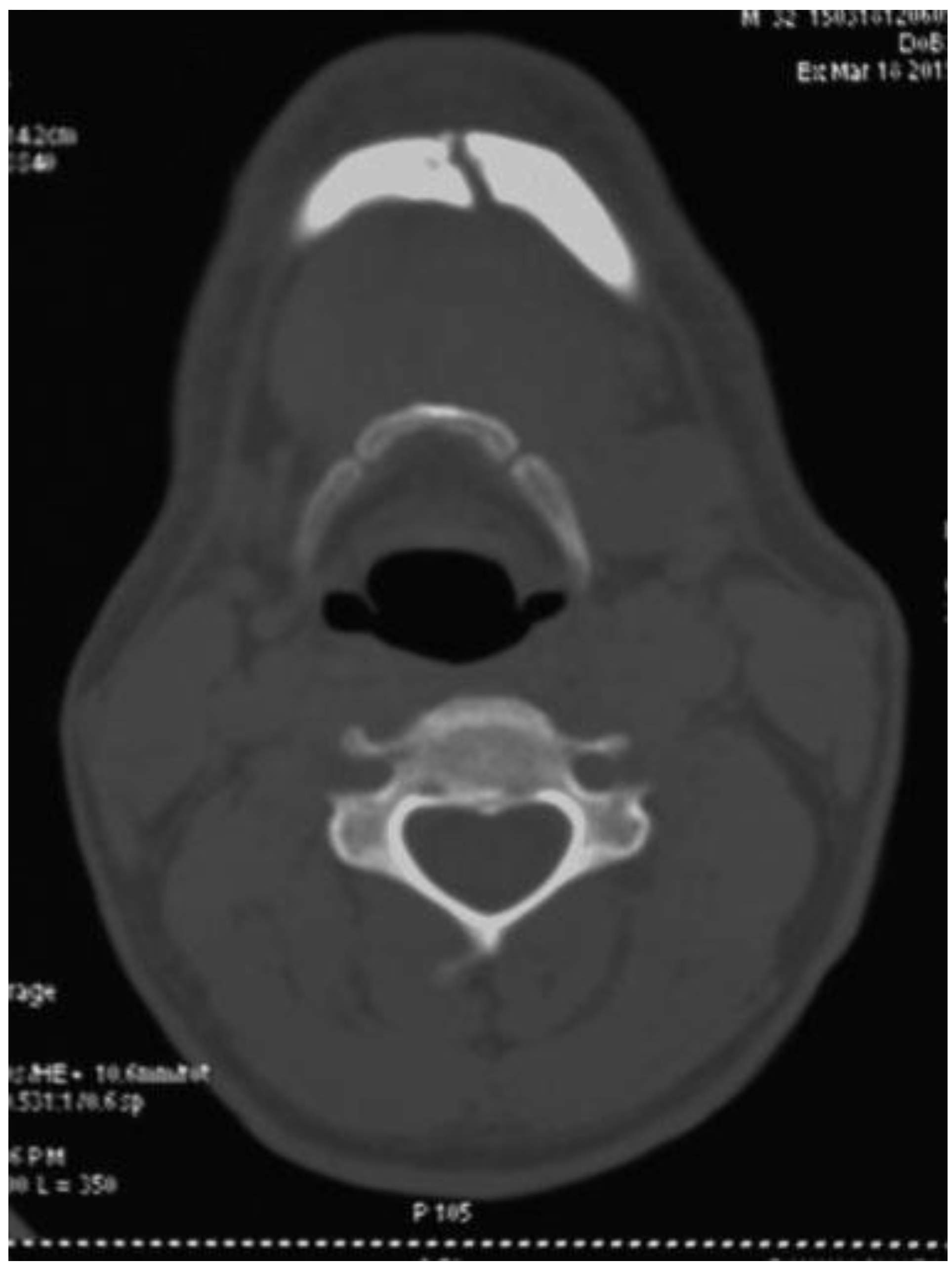
Figure 6.
Case 1: Preoperative CT scan of axial section showing interforaminal fracture of right side mandible.
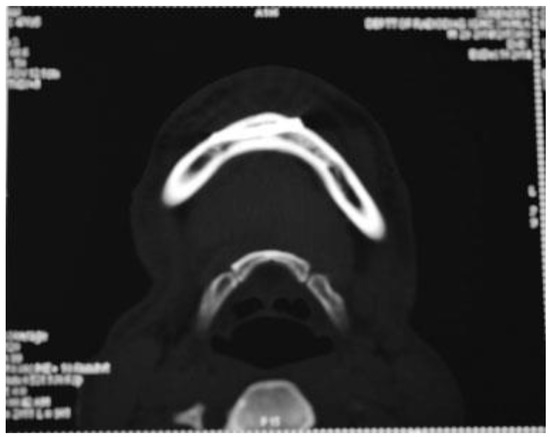
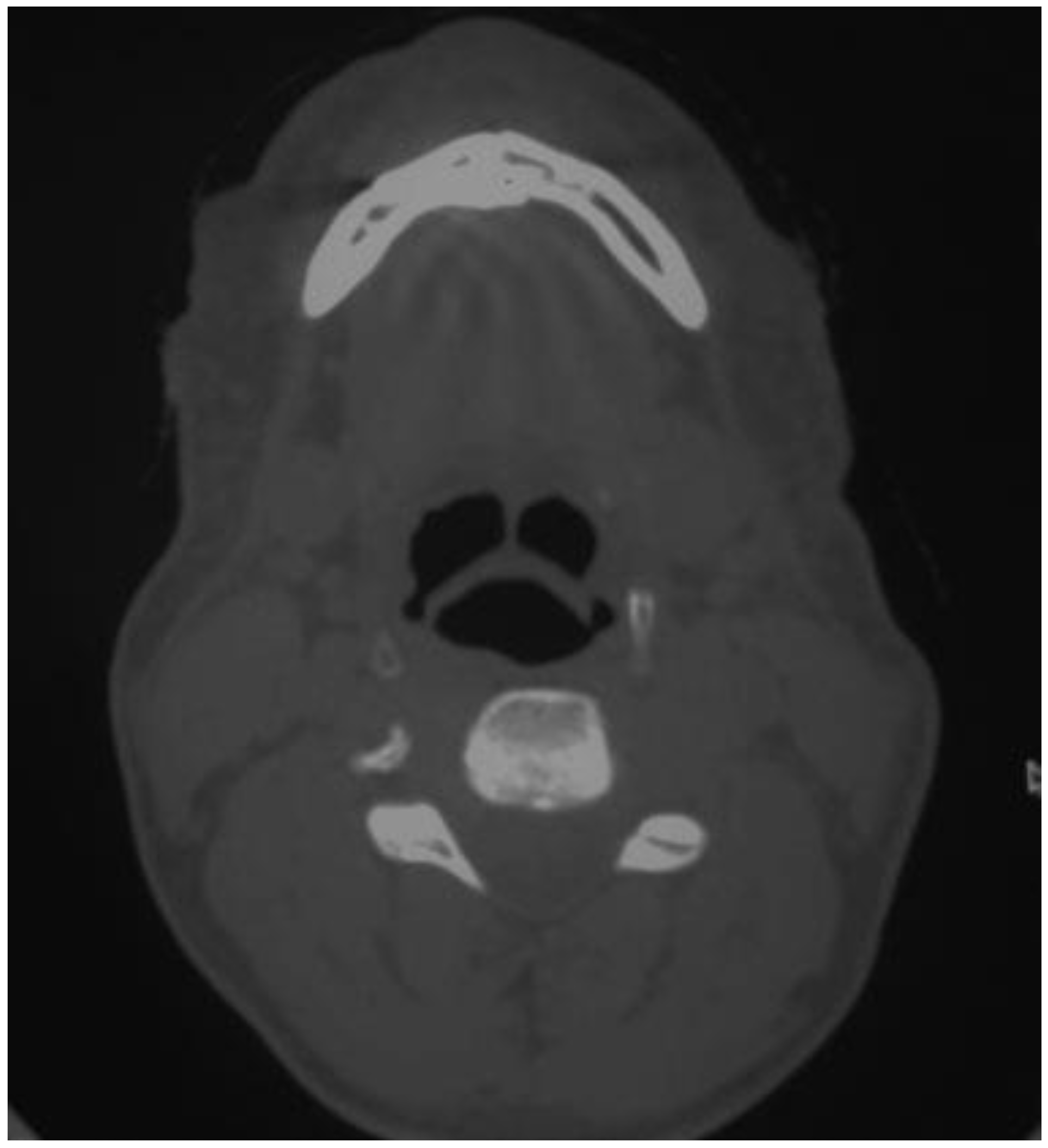
Figure 7.
Case 1: Postoperative CT scan of axial section showing interforaminal mandible fracture reduced and fixed with a headless compression screw.
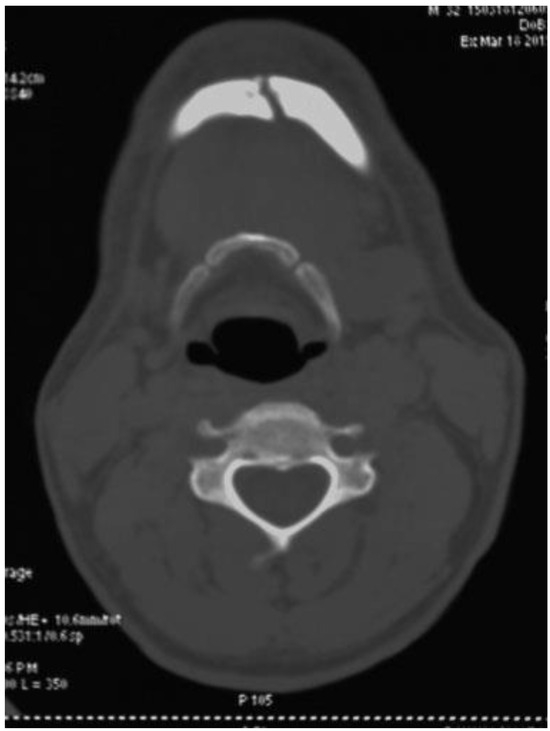
Figure 8.
Case 2: Preoperative CT scan of axial section showing interforaminal fracture of left side mandible.
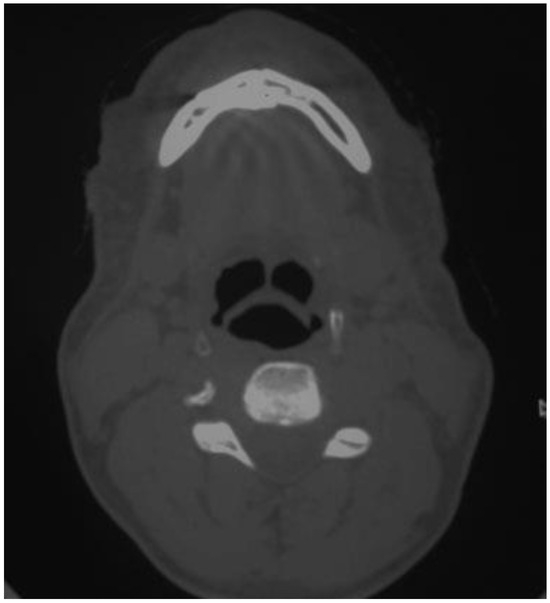
Figure 9.
Case 2: Postoperative CT scan of axial section showing interforaminal mandible fracture reduced and fixed with a headless compression screw.

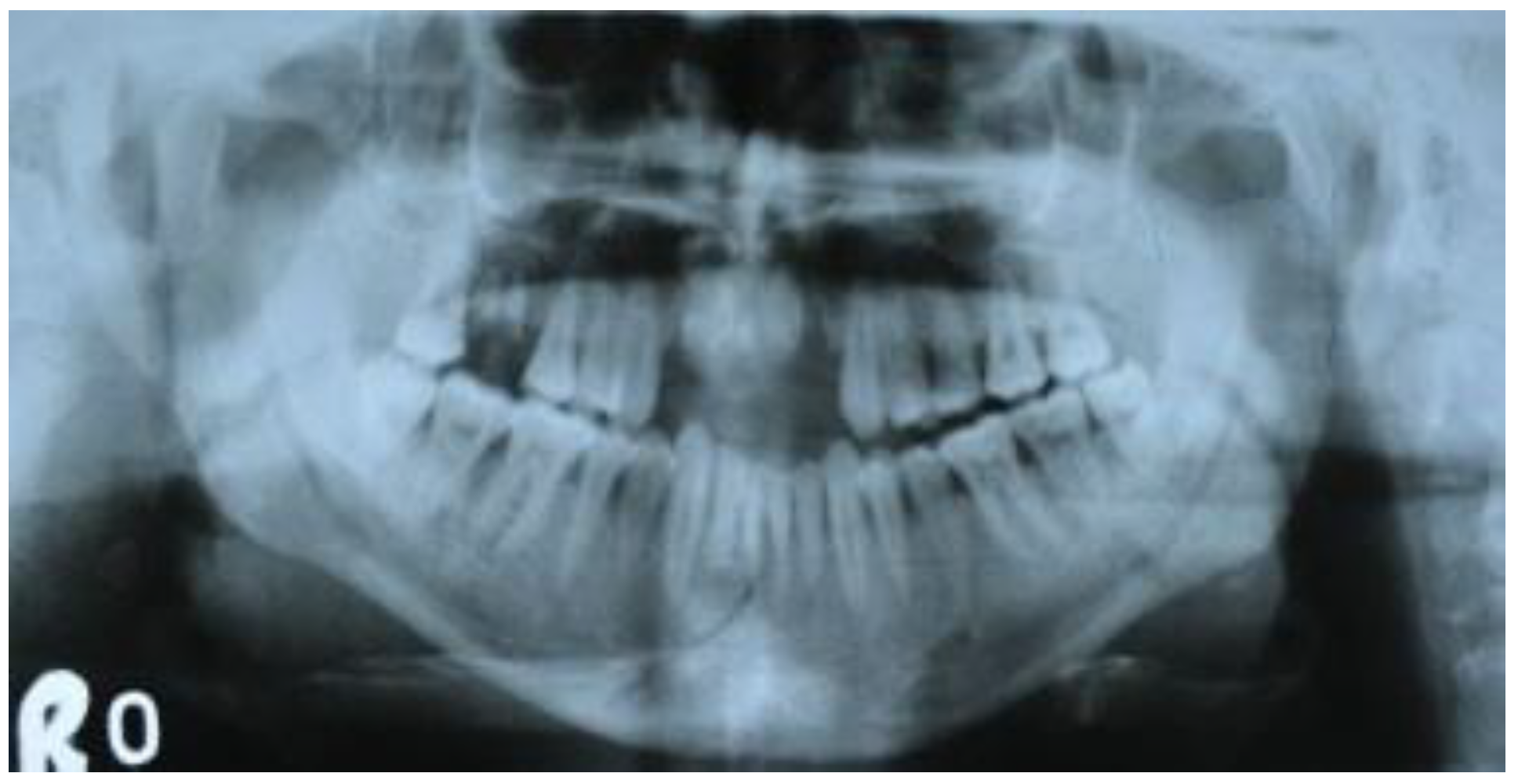
Figure 10.
Case 1: Preoperative orthopantomograph showing interforaminal mandible fracture of right side.
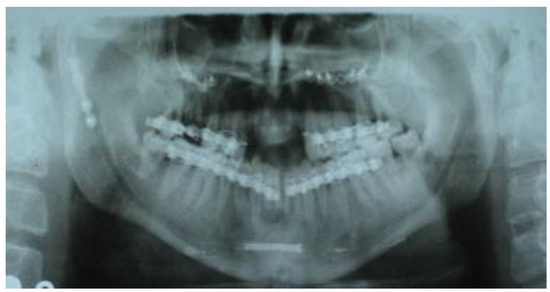
Figure 11.
Case 1: Postoperative orthopantomograph showing interforaminal mandible fracture reduced and fixed with a single headless compression screw.

Figure 12.
Case 2: Preoperative orthopantomograph showing interforaminal mandible fracture of left side.
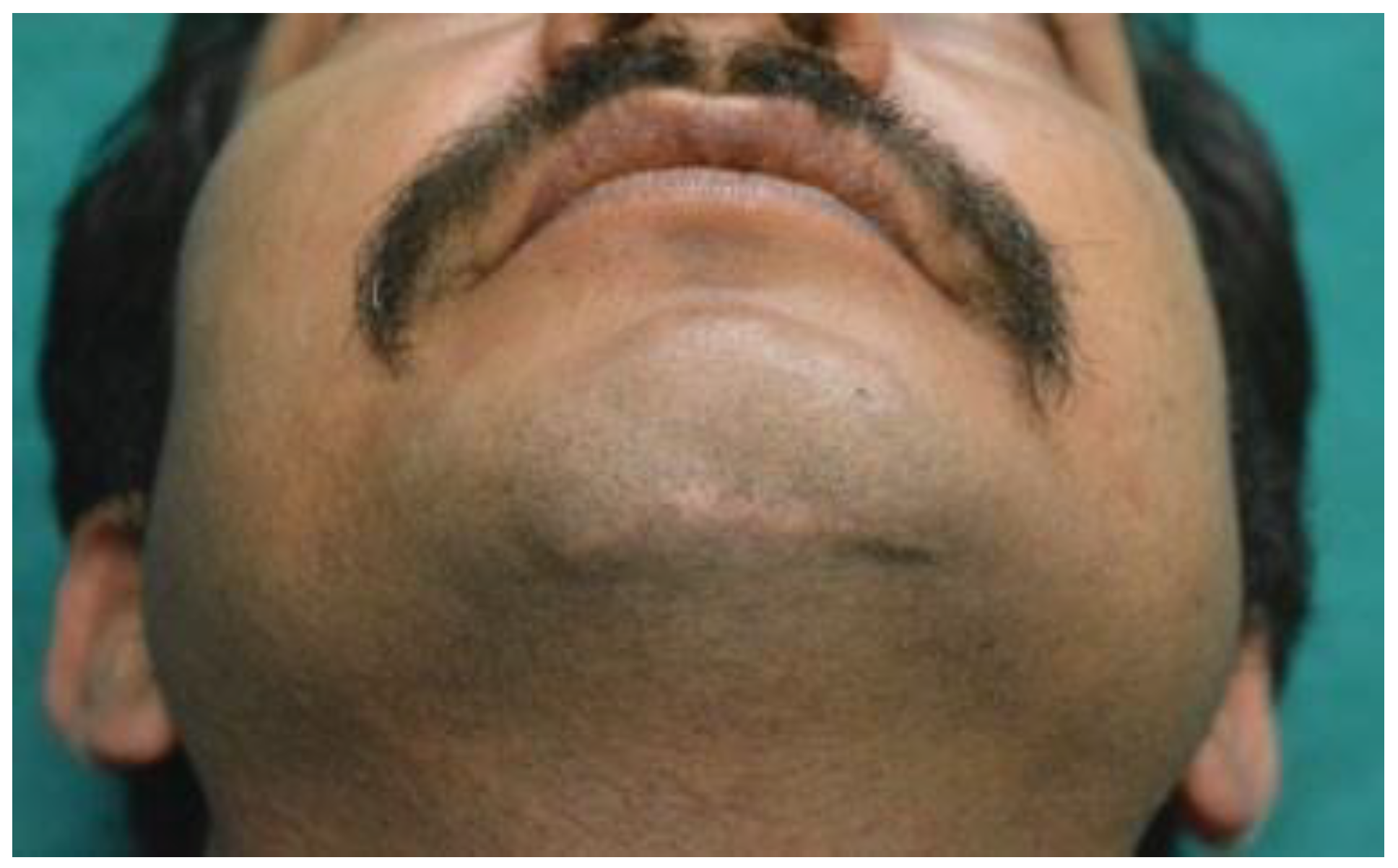
Figure 14.
Case 2: Extraoral scar on 1-year follow-up.
Discussion
Cannulated bone screws have been used in the past for small bones of the extremities, most notably the scaphoid [5]. HCS 3.0 has threads at the distal and proximal ends and a smooth central shank. It is designed to provide interfragmentary compression. HCSs are favored because they are embedded below the surface of the bone, which reduces tissue irritation and immobilization [7].
Conventionally, the use of two hardwares (two miniplates or two lag screws) has been suggested for the fixation of interforaminal fractures of mandible. However, numerous studies have suggested that the use of two miniplates or two lag screws is not absolutely necessary [1,12].
Champy et al. introduced the concept of ideal osteosynthesis lines by using a multidisciplinary approach considering anatomical, biomechanical, and clinical factors [2]. The directions of forces that are distributed through the interforaminal region of mandible vary with the activity of the mandible. This means that the classic zones of tension on the superior and compression on the inferior surfaces of the mandible are not absolute [8].
In this study, we have used a single HCS and the lower arch bar as a tension band eliminating the need for hardware subapically. The only resistance to rotation about one screw is the compaction (friction) of the fragments into one another by virtue of the compression imparted from the HCS. Application of an arch bar to the teeth may prohibit the rotational force.
Tiwana et al. performed a retrospective study on 102 patients regarding analysis of intraoperative and postoperative complications of use of lag screws in the interforaminal fractures of the mandible. They observed that out of all the complications, broken drill bit represented the largest subgroup (5.9%) of patients [13]. Intraosseous drill bit fracture was reported while attempting to drill the traction hole in lag screw technique by Emam and Stevens [12] and Tiwana et al [13].
We did not encounter any instance of drill bit breakage probably because our method requires the use of only a single drill bit instead of two drill bits with different diameter.
According to Al-Moraissi and Ellis among all the treatment modalities for fixation of fractures of interforaminal region of mandible, the use of two miniplates had the highest incidence of complications. This meta-analysis also showed that the use of a single miniplate along with a lower arch bar (as a tension band) decreased the complication rate by 72% as compared with use of two miniplates and that the application of a single lag screw took minimum time among all the treatment modalities for interforaminal mandible fractures [3].
We found that the average time taken in using our technique was 45.57 minutes. The two cases which were operated intraorally took more time owing to careful dissection of mental nerve and exposure of lower border. In case of an existing laceration where an extraoral approach was used, it took lesser time for exposure of thefracture site. We also found that paraesthesia of the mental nerve was present postoperatively in both cases where an intraoral approach was taken which disappeared on 3 months of follow-up. One case that was managed extraorally presented with postoperative mental nerve paraesthesia which resolved on 3 weeks of follow-up.
A study conducted by Saluja et al concluded that a single implant at the lower border is sufficient for fixation of interforaminal mandible fractures, as they managed isolated parasymphysis fractures by placing a single miniplate at the inferior border and utilizing the arch bar as a tension band for 6 weeks [1].
Emam and Stevens found that single lag screw technique, when used in combination with a dental arch bar, provides sufficient fixation to counteract the rotational forces, in the interforaminal region of mandible. More superior the fixation of the lag screw was on the alveolus, the more effective the fixation biomechanics were in resisting the rotational forces [12].
In one case out of seven, reduction and fixationwas found to be inadequate intraoperatively and a miniplate was applied-subapically. Occlusion was intact postoperatively and at follow-up and none of the cases required guiding elastics.
We found that the headless compression screw provided many advantages over a lag screw. The need for using two drill bits of different diameter was obviated. Another advantage was that there was no need for countersinking, as it is a headless screw and it is completely embedded in the buccal cortex. In addition, possibility of microfractures and chipping near buccal cortex can occur near the head of the screw if countersinking is inadequate. This problem does not occur with HCS because they do not have a head. Another advantage of cannulated screws is the possibility of performing minimally invasive surgery, which is possible because the cannulated screw enables the insertion of a Kirschner wire, which can be guided based on visualization in an image-intensifying apparatus, minimizing the need to perform large incisions [11].
Direct trauma to the interforaminal region of mandible is often associated with a laceration which has been sutured in the emergency department giving an unsightly scar. Our technique is best suited for such cases, as we found that approach through an existing laceration required lesser time and lesser chance of injury to the mental nerve. Also it gives another opportunity to revise an extraoral skin scar.
The rationale for using a single HCS along with a lower arch bar in interforaminal fractures of the mandible was the need for a method which was neither time consuming and riddled with complications as two miniplates osteosynthesis [2] nor was it technique sensitive as in the case of lag screw osteosynthesis [8,13].
As this is a pilot study with a small sample size, further researchis required for determining the efficacyof a single HCS as a fixation device along with a lower arch bar for interforaminal fractures of the mandible. A prospective randomized control trial with comparative analysis with other treatment methods (two miniplates and/or two lag screws) for isolated interforaminal fractures of the mandible with a larger sample size would be an ideal study design for this purpose.
We recommend the use of a single HCS along with lower arch bar for fixation of interforaminal fractures of the mandible, as it is less time consuming, does not require a steep learning curve, and provides rigid fixation with minimum complications.
References
- Saluja, H.; Kini, Y.; Mahindra, U.; Kharkar, V.; Rudagi, B.M.; Dehane, V. A comparative evaluation of different treatment modalities for parasymphysis fractures: A pilot study. Int. J. Oral. Maxillofac. Surg. 2012, 41, 906–911. [Google Scholar] [CrossRef]
- Champy, M.; Lodde, J.P.; Schmitt, R. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J. Maxillofac. Surg. 1978, 6, 14–21. [Google Scholar] [PubMed]
- Al-Moraissi, E.A.; Ellis, E. Surgical management of anterior mandibular fractures: A systematic review and meta-analysis. J. Oral. Maxillofac. Surg. 2014, 72, 2507.e1–2507.e11. [Google Scholar] [PubMed]
- Madsen, M.J.; McDaniel, C.A.; Haug, R.H. A biomechanical evaluation of plating techniques used for reconstructing mandibular symphysis/parasymphysis fractures. J. Oral. Maxillofac. Surg. 2008, 66, 2012–2019. [Google Scholar] [CrossRef] [PubMed]
- Filan, S.L.; Herbert, T.J. Herbert screw fixation of scaphoid fractures. J. Bone Jt. Surg. Br. 1996, 78, 519–529. [Google Scholar] [CrossRef]
- Whipple, T.L.; Ellis, F.D. Arthroscopic management of the athlete part I: Internal fixation of scaphoid fractures. J. Hand Ther. 1991, 4, 57–60. [Google Scholar] [CrossRef]
- Assari, S.; Darvish, K.; Ilyas, A.M. Biomechanical analysis of second-generation headless compression screws. Injury 2012, 43, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., III.; Ghali, G.E. Lag screw fixation of anterior mandibular fractures. J. Oral. Maxillofac. Surg. 1991, 49, 13–21. [Google Scholar] [PubMed]
- Pilling, E.; Schneider, M.; Mai, R.; Loukota, R.A.; Eckelt, U. Minimally invasive fracture treatment with cannulated lag screws in intracapsular fractures of the condyle. J. Oral. Maxillofac. Surg. 2006, 64, 868–872. [Google Scholar] [PubMed]
- Loukota, R.A. Fixation of dicapitular fractures of the mandibular condyle with a headless bone screw. Br. J. Oral. Maxillofac. Surg. 2007, 45, 399–401. [Google Scholar] [PubMed]
- Falci, S.G.; Rodrigues, D.C.; Marchiori, E.C.; Brancher, G.; Makyama, A.; Fernandes Moreira, R.W. Assessment of the fixation of mandibular symphysis fractures using conical cannulated screws: Mechanical and photoelastic tests. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 118, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Emam, H.A.; Stevens, M.R. Can an arch bar replace a second lag screw in management of anterior mandibular fractures? J. Oral. Maxillofac. Surg. 2012, 70, 378–383. [Google Scholar] [PubMed]
- Tiwana, P.S.; Kushner, G.M.; Alpert, B. Lag screw fixation of anterior mandibular fractures: A retrospective analysis of intraoperative and postoperative complications. J. Oral. Maxillofac. Surg. 2007, 65, 1180–1185. [Google Scholar]






© 2017 by the author. The Author(s) 2017.