
Long-Term Effectiveness of Hepatitis B Vaccination in the Protection of Healthcare Students in Highly Developed Countries: A Systematic Review and Meta-Analysis
 , and
, and 
Abstract
:1. Introduction
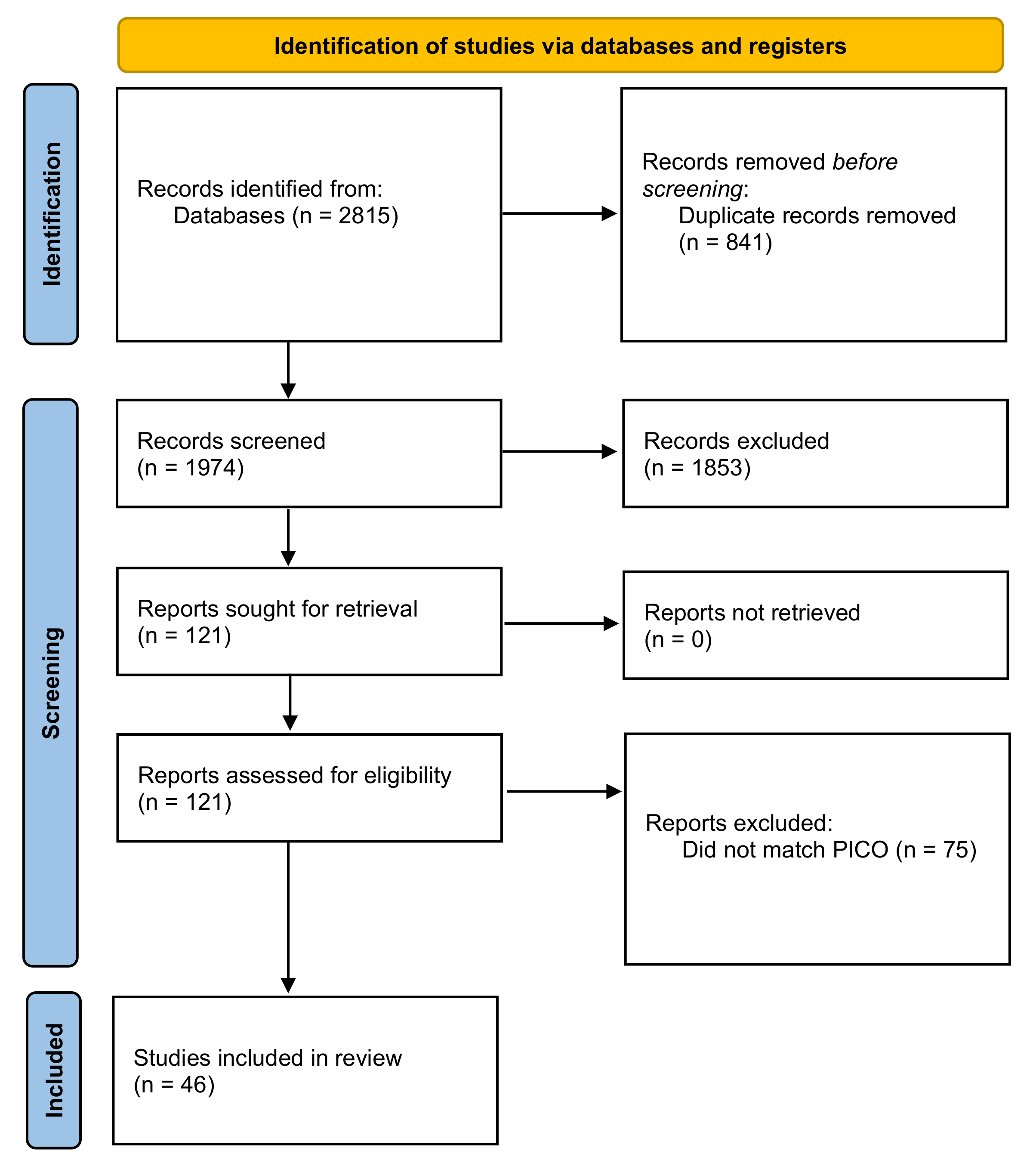
2. Materials and Methods
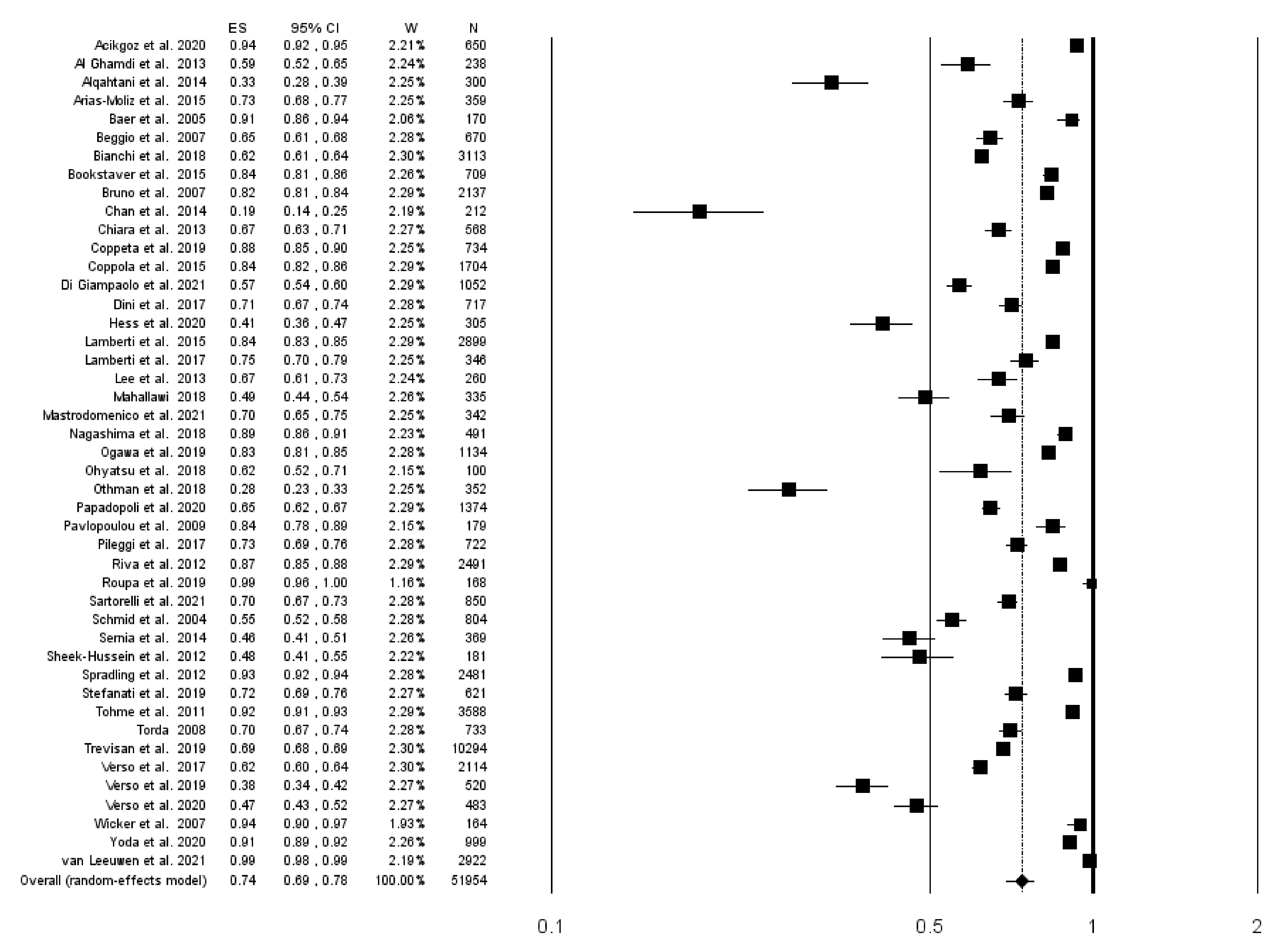
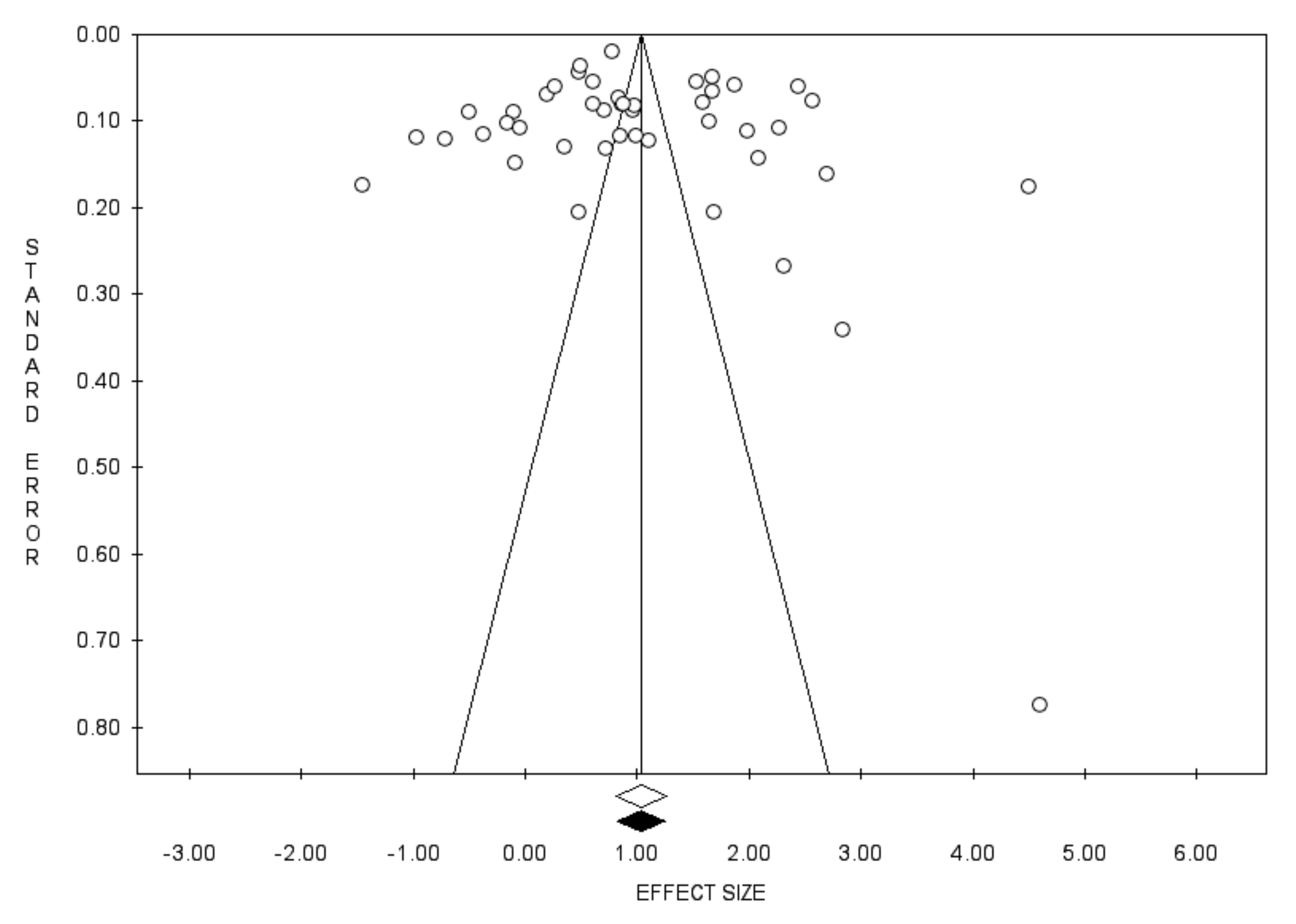
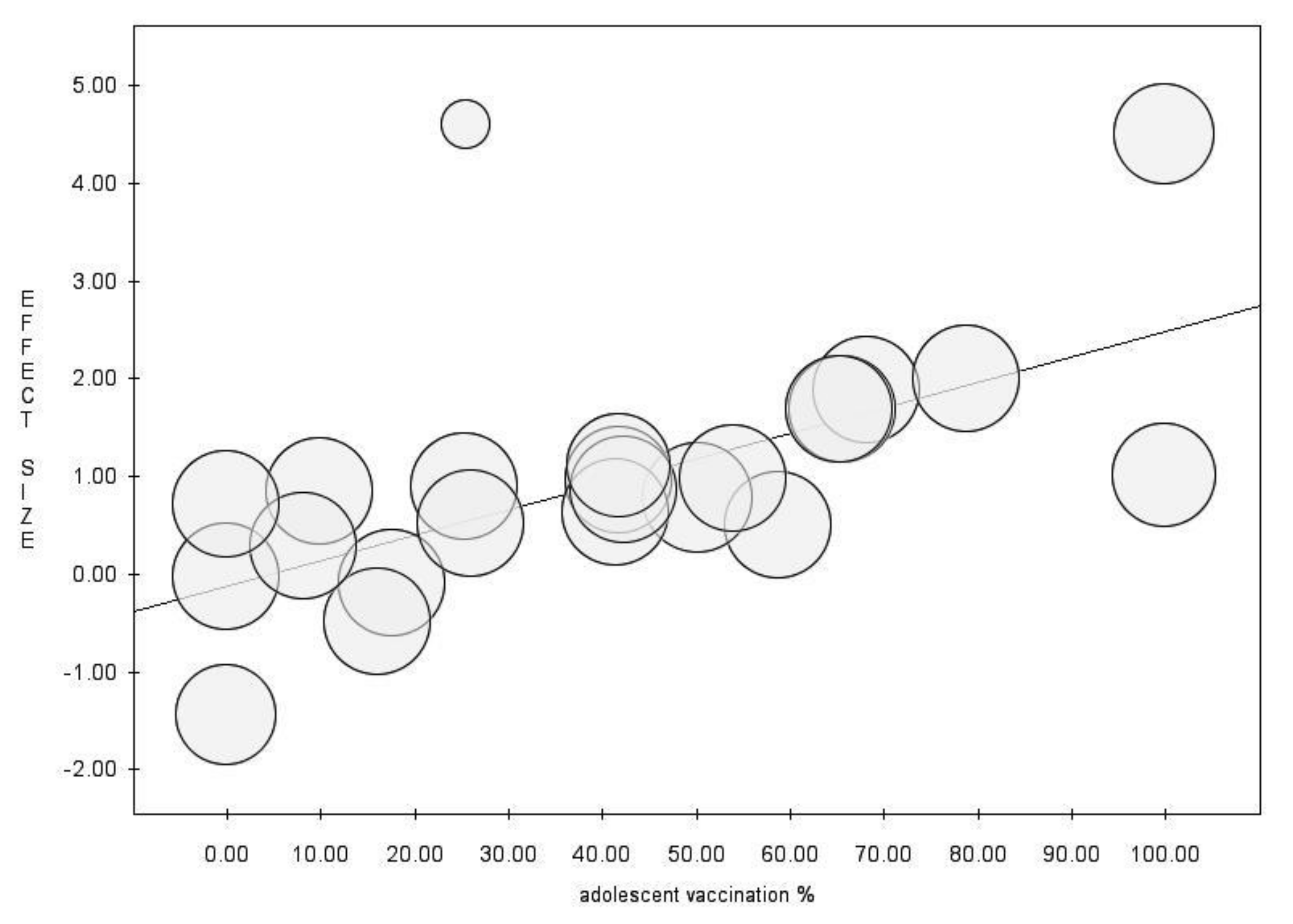
2.1. Data Analysis
2.2. Registration and Protocol
3. Results
Systematic Review
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report. 2017. Available online: https://apps.who.int/iris/rest/bitstreams/1082592/retrieve (accessed on 1 October 2022).
- European Centre for Disease Prevention and Control. Hepatitis B. In Annual Epidemiological Report for 2019; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Prüss-Ustün, A.; Rapiti, E.; Hutin, Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am. J. Ind. Med. 2005, 48, 482–490. [Google Scholar] [CrossRef]
- Mahamat, G.; Kenmoe, S.; Akazong, E.W.; Ebogo-Belobo, J.T.; Mbaga, D.S.; Bowo-Ngandji, A.; Foe-Essomba, J.R.; Amougou-Atsama, M.; Monamele, C.G.; Mbongue Mikangue, C.A.; et al. Global prevalence of hepatitis B virus serological markers among healthcare workers: A systematic review and meta-analysis. World J. Hepatol. 2021, 13, 1190–1202. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fact sheets: Hepatitis B. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 1 October 2022).
- Pattyn, J.; Hendrickx, G.; Vorsters, A.; Van Damme, P. Hepatitis B Vaccines. J. Infect. Dis. 2021, 224, S343–S351. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Hepatitis B. In Epidemiology and Prevention of Vaccine-Preventable Diseases, 14th ed.; Hall, E., Wodi, A.P., Hamborsky, J., Morelli, V., Schillie, S., Eds.; Public Health Foundation: Washington, DC, USA, 2021. [Google Scholar]
- Ministero Della Salute. Il Piano Nazionale Prevenzione Vaccinale. 2017–2019. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 1 October 2022).
- Bagnasco, A.; Zanini, M.; Catania, G.; Watson, R.; Hayter, M.; Dasso, N.; Dini, G.; Agodi, A.; Pasquarella, C.; Zotti, C.M.; et al. Predicting needlestick and sharps injuries in nursing students: Development of the SNNIP scale. Nurs. Open 2020, 7, 1578–1587. [Google Scholar] [CrossRef] [PubMed]
- Black Thomas, L.M. Underreporting of Bloodborne Pathogen Exposures in Nursing Students. Nurse Educ. 2020, 45, 78–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
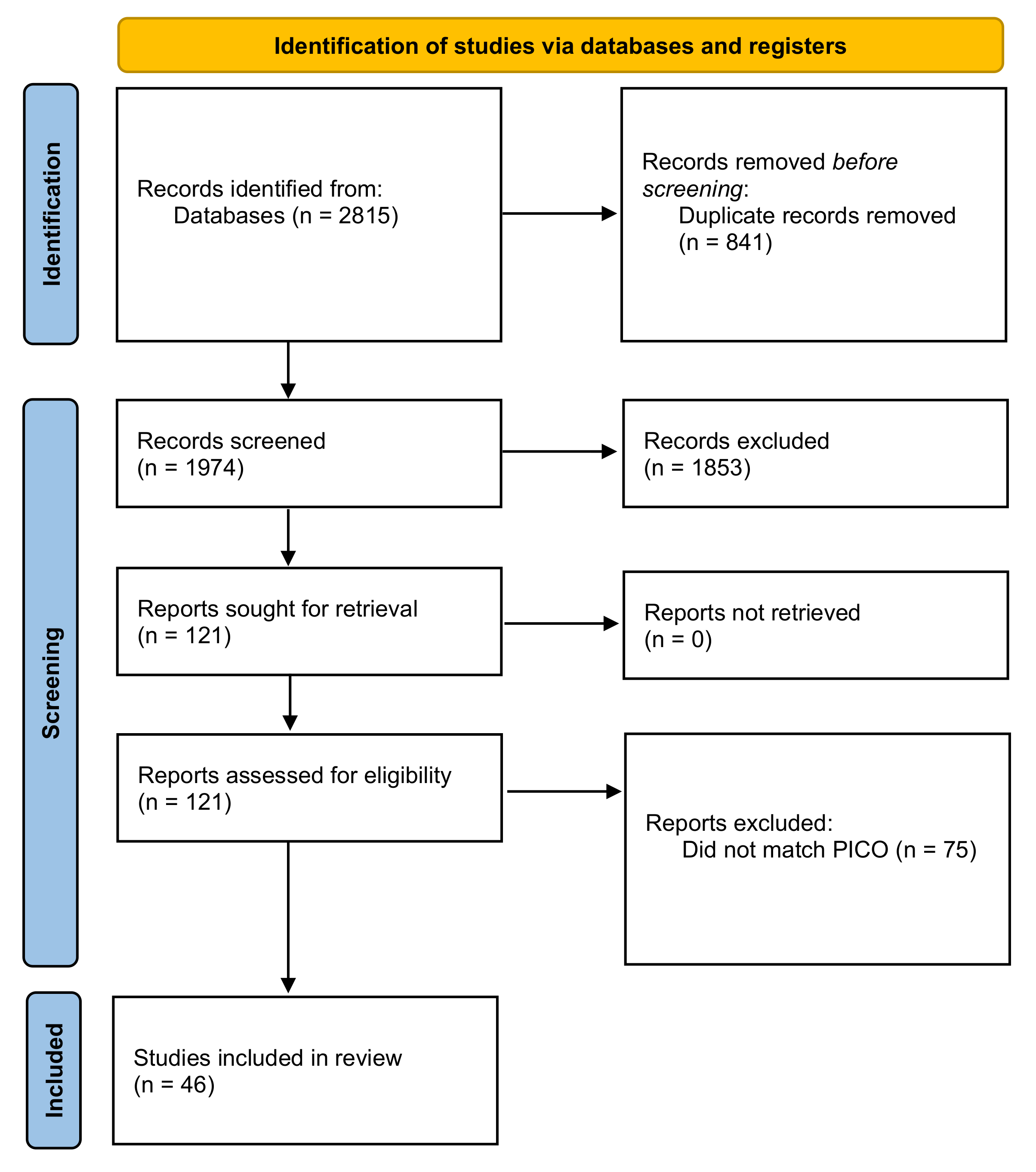
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- United Nations Development Programme. Human Development Report 2020. The Next Frontier Human Development and the Anthropocene; United Nations Development Programme: New York, NY, USA, 2021. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021; Available online: https://www.training.cochrane.org/handbook (accessed on 1 October 2022).
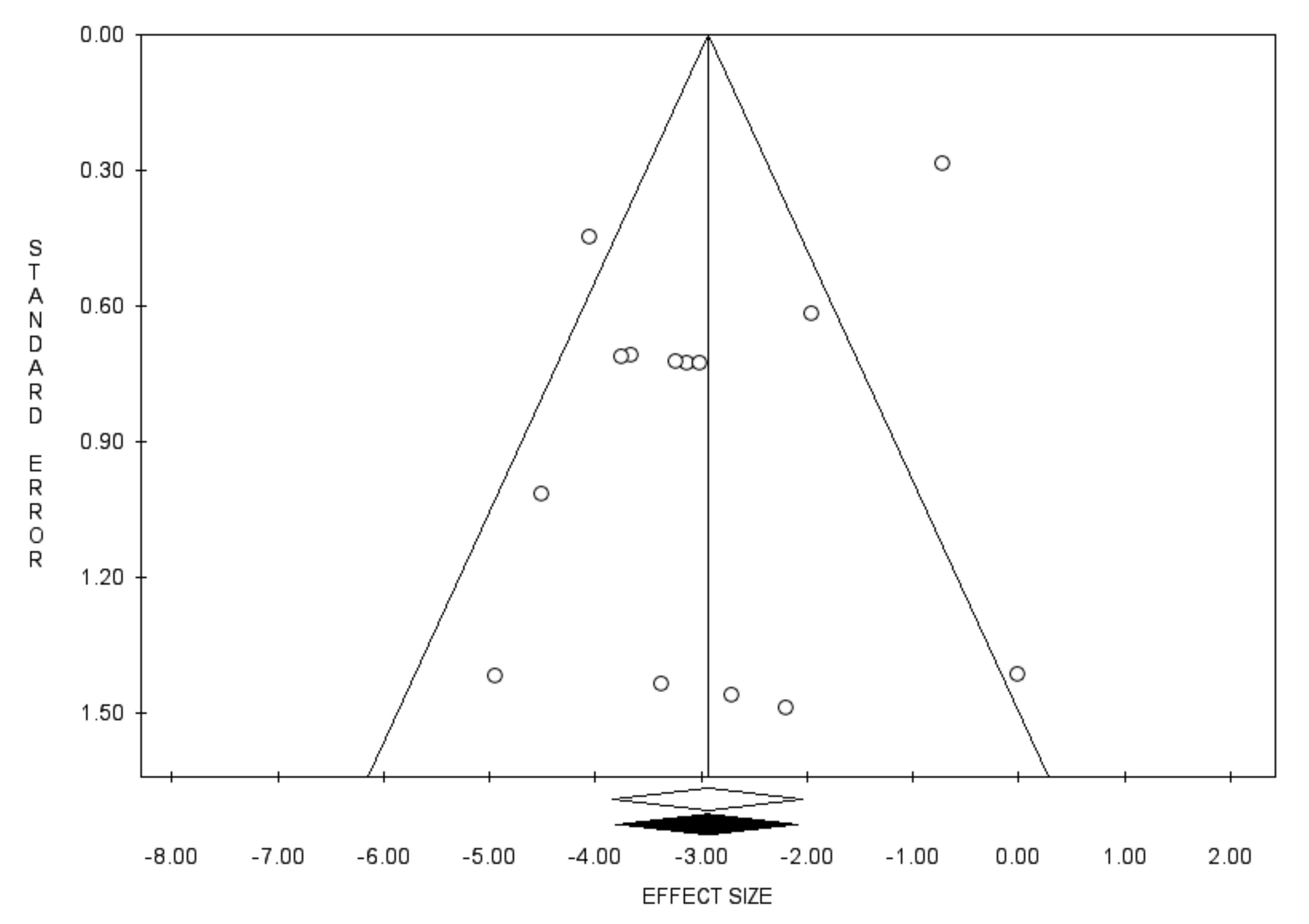
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Acikgoz, A.; Cimrin, D.; Kizildag, S.; Esen, N.; Balci, P.; Sayiner, A.A. Hepatitis A, B and C seropositivity among first-year healthcare students in western Turkey: A seroprevalence study. BMC Infect. Dis. 2020, 20, 529. [Google Scholar] [CrossRef]
- Al Ghamdi, S.S.; Fallatah, H.I.; Fetyani, D.M.; Al-Mughales, J.A.; Gelaidan, A.T. Long-term efficacy of the hepatitis B vaccine in a high-risk group. J. Med. Virol. 2013, 85, 1518–1522. [Google Scholar] [CrossRef]
- Alqahtani, J.M.; Abu-Eshy, S.A.; Mahfouz, A.A.; El-Mekki, A.A.; Asaad, A.M. Seroprevalence of hepatitis B and C virus infections among health students and health care workers in the Najran region, southwestern Saudi Arabia: The need for national guidelines for health students. BMC Public Health 2014, 14, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arias-Moliz, M.T.; Rojas, L.; Liébana-Cabanillas, F.; Bernal, C.; Castillo, F.; Rodríguez-Archilla, A.; Castillo, A.; Liébana, J. Serologic control against hepatitis B virus among dental students of the University of Granada, Spain. Med. Oral. Patol. Oral. Cir. Bucal. 2015, 20, e566–e571. [Google Scholar] [CrossRef] [PubMed]
- Baer, G.; Bonhoeffer, J.; Schaad, U.B.; Heininger, U. Seroprevalence and immunization history of selected vaccine preventable diseases in medical students. Vaccine 2005, 23, 2016–2020. [Google Scholar] [CrossRef] [PubMed]
- Beggio, M.; Giraldo, M.; Borella-Venturini, M.; Mongillo, M.; Zanetti, E.; Bruno, A.; Davanzo, E.; Trevisan, A. Prevalenza dei marcatori dell’epatite (A, B e C) in relazione alla provenienza geografica degli studenti dei corsi di laurea in medicina [Prevalence of hepatitis virus A, B, and C markers according to the geographic origin of medical students]. G. Ital. Med. Lav. Ergon. 2007, 29, 745–747. (In Italian) [Google Scholar]
- Bianchi, F.P.; Gallone, M.S.; Gallone, M.F.; Larocca, A.M.V.; Vimercati, L.; Quarto, M.; Tafuri, S. HBV seroprevalence after 25 years of universal mass vaccination and management of non-responders to the anti-Hepatitis B vaccine: An Italian study among medical students. J. Viral. Hepat. 2019, 26, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Bookstaver, P.B.; Foster, J.L.; Lu, Z.K.; Mann, J.R.; Ambrose, C.; Grant, A.; Burgess, S. Hepatitis B virus seroconversion rates among health sciences students in the southeastern United States. J. Am. Coll. Health 2016, 64, 69–73. [Google Scholar] [CrossRef]
- Bruno, A.; Borella-Venturini, M.; Giraldo, M.; Mongillo, M.; Zanetti, E.; Beggio, M.; Davanzo, E.; Trevisan, A. Prevalenza dei marcatori dell’epatite B negli studenti dei corsi di laurea in medicina [Prevalence of virus hepatitis B markers among medical students]. G. Ital. Med. Lav. Ergon. 2007, 29, 752–754. (In Italian) [Google Scholar]
- Chan, P.K.; Ngai, K.L.; Lao, T.T.; Wong, M.C.; Cheung, T.; Yeung, A.C.; Chan, M.C.; Luk, S.W. Response to booster doses of hepatitis B vaccine among young adults who had received neonatal vaccination. PLoS ONE 2014, 9, e107163. [Google Scholar] [CrossRef]
- Chiara, F.; Bartolucci, G.B.; Mongillo, M.; Ferretto, L.; Nicolli, A.; Trevisan, A. Hepatitis B vaccination at three months of age: A successful strategy? Vaccine 2013, 31, 1696–1700. [Google Scholar] [CrossRef]
- Coppeta, L.; Pompei, A.; Balbi, O.; Zordo, L.M.; Mormone, F.; Policardo, S.; Lieto, P.; Pietroiusti, A.; Magrini, A. Persistence of Immunity for Hepatitis B Virus among Heathcare Workers and Italian Medical Students 20 Years after Vaccination. Int. J. Environ. Res. Public Health 2019, 16, 1515. [Google Scholar] [CrossRef] [Green Version]
- Coppola, N.; Corvino, A.R.; De Pascalis, S.; Signoriello, G.; Di Fiore, E.; Nienhaus, A.; Sagnelli, E.; Lamberti, M. The long-term immunogenicity of recombinant hepatitis B virus (HBV) vaccine: Contribution of universal HBV vaccination in Italy. BMC Infect. Dis. 2015, 15, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Giampaolo, L.; Costantini, E.; Di Nicola, M.; Porreca, A.; D’Amore, G.; Coppeta, L.; Mangifesta, R. Titer of anti-HBs in health professions trainees: Prevalence of antibody coverage in a University of Central Italy. Hum. Vaccines Immunother. 2022, 18, 1886805. [Google Scholar] [CrossRef] [PubMed]
- Dini, G.; Toletone, A.; Barberis, I.; Debarbieri, N.; Massa, E.; Paganino, C.; Bersi, F.; Montecucco, A.; Alicino, C.; Durando, P. Persistence of protective anti-HBs antibody levels and anamnestic response to HBV booster vaccination: A cross-sectional study among healthcare students 20 years following the universal immunization campaign in Italy. Hum. Vaccines Immunother. 2017, 13, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Grazzini, M.; Arcangeli, G.; Mucci, N.; Bonanni, P.; Bini, C.; Bechini, A.; Boccalini, S.; Tiscione, E.; Paolini, D. High chance to overcome the non-responder status to hepatitis B vaccine after a further full vaccination course: Results from the extended study on healthcare students and workers in Florence, Italy. Hum. Vaccines Immunother. 2020, 16, 949–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, L.; Riesenberg, K.; Rolston, K.V.I.; Nesher, L. Administering an additional hepatitis B vaccination dose after 18 years maintains adequate long-term protection levels in healthcare workers. Infect. Dis. 2020, 52, 330–335. [Google Scholar] [CrossRef]
- Lamberti, M.; De Rosa, A.; Garzillo, E.M.; Corvino, A.R.; Sannolo, N.; De Pascalis, S.; Di Fiore, E.; Westermann, C.; Arnese, A.; Gabriella, D.G.; et al. Vaccination against hepatitis b virus: Are Italian medical students sufficiently protected after the public vaccination programme? J. Occup. Med. Toxicol. 2015, 10, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamberti, M.; Garzillo, E.; Muoio, M.; Arnese, A.; Nienhaus, A.; Abbondante, E.; Giuseppe, G.; Pedata, P.; Rosado, A. Seropositivity for Hepatitis B Virus, Vaccination Status and Response to Vaccine in a Cohort of Dental Students. Open J. Prev. Med. 2017, 7, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Song, H.; Lee, J.M.; Cho, J. Seroprevalence of hepatitis A and B viruses in medical school students planning for medical clerkships. Am. J. Infect. Control 2014, 42, 89–90. [Google Scholar] [CrossRef]
- Mahallawi, W. Persistence of hepatitis B surface antibody and immune memory to hepatitis B vaccine among medical college students in Madinah. Ann. Saudi. Med. 2018, 38, 413–419. [Google Scholar] [CrossRef]
- Mastrodomenico, M.; Muselli, M.; Provvidenti, L.; Scatigna, M.; Bianchi, S.; Fabiani, L. Long-term immune protection against HBV: Associated factors and determinants. Hum. Vaccines Immunother. 2021, 17, 2268–2272. [Google Scholar] [CrossRef]
- Nagashima, S.; Yamamoto, C.; Ko, K.; Chuon, C.; Sugiyama, A.; Ohisa, M.; Akita, T.; Katayama, K.; Yoshihara, M.; Tanaka, J. Acquisition rate of antibody to hepatitis B surface antigen among medical and dental students in Japan after three-dose hepatitis B vaccination. Vaccine 2019, 37, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Akine, D.; Sasahara, T. Comparison of hepatitis B vaccine efficacy in Japanese students: A retrospective study. Environ. Health Prev. Med. 2019, 24, 80. [Google Scholar] [CrossRef] [PubMed]
- Ohyatsu, M.; Ishikawa, Y.; Chibana, Y.; Watanabe, N.; Ohrui, M.; Tsuchida, K.; Tominaga, K.; Murohisa, T.; Iijima, M.; Hiraishi, H. Results of Hepatitis B Vaccination 3 Years After a Primary Vaccine Series in Medical Students. Dokkyo J. Med. Sci. 2018, 45, 1–8. [Google Scholar]
- Othman, S.N.; Zainol Rashid, Z.; Abdul Wahab, A.; Abdul Samat, M.N.; Ding, C.H.; Ali, U.K. Hepatitis B seroepidemiology and booster vaccination in pre-clinical medical students in a Malaysian university. Malays. J. Pathol. 2018, 40, 295–302. [Google Scholar] [PubMed]
- Papadopoli, R.; De Sarro, C.; Torti, C.; Pileggi, C.; Pavia, M. Is There Any Opportunity to Provide an HBV Vaccine Booster Dose Before Anti-Hbs Titer Vanishes? Vaccines 2020, 8, 227. [Google Scholar] [CrossRef] [PubMed]
- Pavlopoulou, I.D.; Daikos, G.L.; Tzivaras, A.; Bozas, E.; Kosmidis, C.; Tsoumakas, C.; Theodoridou, M. Medical and nursing students with suboptimal protective immunity against vaccine-preventable diseases. Infect. Control. Hosp. Epidemiol. 2009, 30, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Pileggi, C.; Papadopoli, R.; Bianco, A.; Pavia, M. Hepatitis B vaccine and the need for a booster dose after primary vaccination. Vaccine 2017, 35, 6302–6307. [Google Scholar] [CrossRef]
- Riva, M.A.; Madotto, F.; Conti, S.; Fornari, C.; Patronella, G.; Sormani, M.; D'Orso, M.I.; De Vito, G.; Latocca, R.; Cesana, G. Copertura vaccinale anti-epatite B e dose di rinforzo: Risultati di uno studio su una popolazione universitaria [Hepatitis B vaccination coverage and booster dose: Results from a survey on healthcare students]. G. Ital. Med. Lav. Ergon. 2012, 34, 283–285. (In Italian) [Google Scholar]
- Roupa, Z.; Noula, M.; Farazi, E.; Stylianides, A.; Papaneophytou, C. Vaccination Coverage and Awareness of Hepatitis B Virus Among Healthcare Students at a University in Cyprus. Mater. Sociomed. 2019, 31, 190–196. [Google Scholar] [CrossRef]
- Sartorelli, P.; Occhialini, F.; Miceli, R.; Pietronigro, A.; Bianciardi, L.; Salini, C.; Messina, G. The seroprevalence of the hepatitis B virus in Italian medical students after 3 decades since the introduction of universal vaccination. Int. J. Occup. Med. Environ. Health 2022, 35, 75–80. [Google Scholar] [CrossRef]
- Schmid, K.; Wallaschofski, H.; Drexler, H. Student health policy of a German medical school—Results of a cross sectional study concerning students’ immunity to vaccine-preventable diseases. Int. J. Hyg. Environ. Health 2004, 207, 595–600. [Google Scholar] [CrossRef]
- Sernia, S.; Ortis, M.; Antoniozzi, T.; Maffongelli, E.; La Torre, G. Levels of anti-HBs antibody in HBV-vaccinated students enrolled in the faculty of medicine, dentistry and health professions of a large Italian University. Biomed. Res. Int. 2015, 2015, 712020. [Google Scholar] [CrossRef] [PubMed]
- Sheek-Hussein, M.; Hashmey, R.; Alsuwaidi, A.R.; Al Maskari, F.; Amiri, L.; Souid, A.K. Seroprevalence of measles, mumps, rubella, varicella-zoster and hepatitis A–C in Emirati medical students. BMC Public Health 2012, 12, 1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spradling, P.R.; Williams, R.E.; Xing, J.; Soyemi, K.; Towers, J. Serologic testing for protection against hepatitis B virus infection among students at a health sciences university in the United States. Infect. Control Hosp. Epidemiol. 2012, 33, 732–736. [Google Scholar] [CrossRef]
- Stefanati, A.; Bolognesi, N.; Sandri, F.; Dini, G.; Massa, E.; Montecucco, A.; Lupi, S.; Gabutti, G. Long-term persistency of hepatitis B immunity: An observational cross-sectional study on medical students and resident doctors. J. Prev. Med. Hyg. 2019, 60, E184–E190. [Google Scholar] [CrossRef] [PubMed]
- Tohme, R.A.; Ribner, B.; Huey, M.J.; Spradling, P.R. Hepatitis B vaccination coverage and documented seroprotection among matriculating healthcare students at an academic institution in the United States. Infect. Control Hosp. Epidemiol. 2011, 32, 818–821. [Google Scholar] [CrossRef] [PubMed]
- Torda, A.J. Vaccination and screening of medical students: Results of a student health initiative. Med. J. Aust. 2008, 189, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, A.; Frasson, C.; De Nuzzo, D.; Nicolli, A.; Scapellato, M.L. Significance of anti-HB levels below 10 IU/L after vaccination against hepatitis B in infancy or adolescence: An update in relation to sex. Hum. Vaccines Immunother. 2020, 16, 460–464. [Google Scholar] [CrossRef]
- van Leeuwen, L.P.M.; Doornekamp, L.; Goeijenbier, S.; de Jong, W.; de Jager, H.J.; van Gorp, E.C.M.; Goeijenbier, M. Evaluation of the Hepatitis B Vaccination Programme in Medical Students in a Dutch University Hospital. Vaccines 2021, 9, 69. [Google Scholar] [CrossRef]
- Verso, M.G.; Lo Cascio, N.; Noto Laddeca, E.; Amodio, E.; Currieri, M.; Giammanco, G.; Ferraro, D.; De Grazia, S.; Picciotto, D. Predictors of Hepatitis B Surface Antigen Titers two decades after vaccination in a cohort of students and post-graduates of the Medical School at the University of Palermo, Italy. Ann. Agric. Environ. Med. 2017, 24, 303–306. [Google Scholar] [CrossRef] [Green Version]
- Verso, M.G.; Costantino, C.; Vitale, F.; Amodio, E. Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback. Vaccines 2019, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verso, M.G.; Costantino, C.; Marrella, A.; Immordino, P.; Vitale, F.; Amodio, E. Kinetics of Anti-Hepatitis B Surface Antigen Titers in Nurse Students after a Two-Year Follow-Up. Vaccines 2020, 8, 467. [Google Scholar] [CrossRef] [PubMed]
- Wicker, S.; Rabenau, H.F.; Gottschalk, R.; Doerr, H.W.; Allwinn, R. Seroprevalence of vaccine preventable and blood transmissible viral infections (measles, mumps, rubella, polio, HBV, HCV and HIV) in medical students. Med. Microbiol. Immunol. 2007, 196, 145–150. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Analysis of antibody-negative medical students after hepatitis B vaccination in Japan. Hum. Vaccines Immunother. 2021, 17, 852–856. [Google Scholar] [CrossRef]
- Rovenský, J.; Payer, J. (Eds.) Lymphocytes—Circulation. In Dictionary of Rheumatology; Springer: Vienna, Austria, 2009. [Google Scholar] [CrossRef]
- Palm, A.E.; Henry, C. Remembrance of Things Past: Long-Term B Cell Memory After Infection and Vaccination. Front. Immunol. 2019, 10, 1787. [Google Scholar] [CrossRef] [Green Version]
- European Consensus Group on Hepatitis B Immunity. Are booster immunisations needed for lifelong hepatitis B immunity? Lancet 2000, 355, 561–565. [Google Scholar] [CrossRef]
- Chiara, F.; Bartolucci, G.B.; Cattai, M.; Piazza, A.; Nicolli, A.; Buja, A.; Trevisan, A. Hepatitis B vaccination of adolescents: Significance of non-protective antibodies. Vaccine 2013, 32, 62–68. [Google Scholar] [CrossRef]
- Trevisan, A.; Giuliani, A.; Scapellato, M.L.; Anticoli, S.; Carsetti, R.; Zaffina, S.; Brugaletta, R.; Vonesch, N.; Tomao, P.; Ruggieri, A. Sex Disparity in Response to Hepatitis B Vaccine Related to the Age of Vaccination. Int. J. Environ. Res. Public Health 2020, 17, 327. [Google Scholar] [CrossRef] [Green Version]
- Cook, I.F. Sexual dimorphism of humoral immunity with human vaccines. Vaccine 2008, 26, 3551–3555. [Google Scholar] [CrossRef]
- Fish, E.N. The X-files in immunity: Sex-based differences predispose immune responses. Nat. Rev. Immunol. 2008, 8, 737–744. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Systematic Review on Hepatitis B and C Prevalence in the EU/EEA; ECDC: Stockholm, Sweden, 2016. [Google Scholar]
- Decree-Law 9 April 2008, Coordinated Text with Legislative Decree 3 August 2009, n. 106, Consolidated Law on Occupational Health and Safety. [Testo Coordinato con il D.Lgs. 3 Agosto 2009, n. 106, Testo Unico Sulla Salute e Sicurezza sul Lavoro]. Available online: https://www.ispettorato.gov.it/it-it/in-evidenza/Documents/Testo-unico-salute-sicurezza-gennaio-2020.pdf (accessed on 1 October 2022).
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Year | Country | Field of Study | Sample Size | Age (y) | Female (%) | Foreigner (%) | Vaccinated with 3-Dose Primary Cycle (%) | Time Since Primary Cycle Vaccination (y) | Primary Cycle during Infancy (%) | Primary Cycle during Adolescence (%) | HBsAb ≥ 10 mIU/mL (ratio) | Anamnestic Response Following Challenge Dose (ratio) | Non-Response Following Completion of Second Cycle n (ratio) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Acikgoz et al. [16] | 2020 | Turkey | healthcare | 650 | 19.8 | 66.5 | NA | NA | NA | NA | NA | 0.937 | NA | NA |
| Al Ghamdi et al. [17] | 2013 | Saudi Arabia | medical | 238 | 22.2 | 76.5 | NA | 100.0 | 19.8 | 80.3 | NA | 0.588 | NA | NA |
| Alqahtani et al. [18] | 2014 | Saudi Arabia | healthcare | 300 | 20.9 | 33.7 | NA | 52.0 | NA | NA | NA | 0.33 | NA | NA |
| Arias-Moliz et al. [19] | 2015 | Spain | dental | 359 | 20.1 | 72.9 | NA | 100.0 | 7.0 | 0.0 | 100.0 | 0.73 | NA | 2 (0.023) |
| Baer et al. [20] | 2005 | Switzerland | medical | 170 | 26.0 | 61.0 | 19.0 | 85.0 | NA | NA | NA | 0.91 | NA | NA |
| Beggio et al. [21] | 2007 | Italy | healthcare | 670 | 23.9 | 69.3 | 33.0 | 71.2 | NA | NA | NA | 0.647 | NA | NA |
| Bianchi et al. [22] | 2018 | Italy | medical (including residents) | 3113 | 24.0 | 66.3 | NA | 100.0 | NA | 74.0 | 26.0 | 0.623 | 0.909 | 2 (0.038) |
| Bookstaver et al. [23] | 2015 | USA | healthcare | 709 | 24.0 | 62.0 | NA | 95.5 | 9.8 | NA | NA | 0.839 | 0.963 | 2 (missing denominator) |
| Bruno et al. [24] | 2007 | Italy | healthcare | 2137 | 22.9 | 70.8 | NA | 70.5 | NA | NA | NA | 0.823 | NA | NA |
| Chan et al. [25] | 2014 | Hong Kong—China SAR | medical and nursing | 212 | 19.0 | 67.7 | NA | 100.0 | NA | 100.0 | 0.0 | 0.189 | 0.855 | 0 (0) |
| Chiara et al. [26] | 2013 | Italy | medical | 568 | 21.0 | 69.5 | NA | 100.0 | 18.0 | 53.3 | 0.0 | 0.67 | 0.966 | 1 (0.011) |
| Coppeta et al. [27] | 2019 | Italy | healthcare (including workers) | 734 | 29.9 | 65.5 | NA | 100.0 | 20.5 | 21.1 | 78.9 | 0.880 | 0.897 | NA |
| Coppola et al. [28] | 2015 | Italy | healthcare | 1704 | 26.0 | 60.6 | 1.1 | 100.0 | 17.7 | 34.6 | 65.4 | 0.842 | NA | NA |
| Di Giampaolo et al. [29] | 2021 | Italy | healthcare | 1052 | 21.2 | 66.3 | NA | 100.0 | NA | 91.7 | 8.3 | 0.568 | NA | NA |
| Dini et al. [30] | 2017 | Italy | healthcare | 717 | 24.8 | 67.2 | NA | 100.0 | 21.4 | 74.6 | 25.4 | 0.707 | 0.952 | NA |
| Grazzini et al. [31] | 2019 | Italy | healthcare | 795 | NA | 64.4 | 0 | 100.0 | 19.6 | 81.6 | 18.4 | 0 | 0.878 | 2 (0.047) |
| Hess et al. [32] | 2020 | Israel | healthcare | 305 | 21.9 | 79.4 | NA | 100.0 | NA | 100.0 | NA | 0.41 | 0.934 | NA |
| Lamberti et al. [33] | 2015 | Italy | healthcare | 2899 | 26.0 | 60.1 | 1.1 | 100.0 | 18.2 | 34.3 | 65.7 | 0.842 | NA | NA |
| Lamberti et al. [34] | 2017 | Italy | dental | 346 | 26.5 | 47.1 | 0.28 | 100.0 | NA | 58.1 | 41.9 | 0.751 | NA | NA |
| Lee et al. [35] | 2013 | South Korea | medical and nursing | 260 | 22.8 | 60.4 | NA | NA | NA | NA | NA | 0.673 | NA | NA |
| Mahallawi [36] | 2018 | Saudi Arabia | medical | 335 | 22.8 | 73.1 | 0 | 100.0 | 21.3 | 100.0 | 0.0 | 0.49 | 0.973 | 5 (0.017) |
| Mastrodomenico et al. [37] | 2021 | Italy | healthcare | 342 | 26.1 | 63.2 | NA | 100.0 | 20.5 | 57.6 | 42.4 | 0.699 | NA | NA |
| Nagashima et al. [38] | 2018 | Japan | medical and dental | 491 | 22.7 | 41.1 | NA | 100.0 | 0.4 | NA | NA | 0.89 | NA | NA |
| Ogawa et al. [39] | 2019 | Japan | medical and nursing | 1134 | 20.0 | 57.6 | 0 | 100.0 | 0.27 | 0 | 0 | 0.829 | NA | NA |
| Ohyatsu et al. [40] | 2018 | Japan | medical | 100 | 21.4 | 41.0 | NA | 100.0 | 2.0 | NA | NA | 0.62 | 0.972 | 1 (0.50) |
| Othman et al. [41] | 2018 | Malaysia | medical | 352 | NA | 69.0 | 26.8 | 100.0 | NA | NA | NA | 0.276 | 0.816 | 2 (0.042) |
| Papadopoli et al. [42] | 2020 | Italy | healthcare | 1374 | 24.8 | 67.1 | NA | 100.0 | 19.3 | 55.3 | 41.5 | 0.649 | 0.922 | 0 (0) |
| Pavlopoulou et al. [43] | 2009 | Greece | medical and nursing | 179 | 23.8 | 66.0 | 7.0 | 77.7 | NA | NA | NA | 0.844 | NA | NA |
| Pileggi et al. [44] | 2017 | Italy | healthcare (including residents) | 722 | 25.5 | 70.0 | NA | 100.0 | 18.3 | 41.3 | 54.0 | 0.726 | NA | NA |
| Riva et al. [45] | 2012 | Italy | healthcare (including residents) | 2491 | 21.5 | 70.9 | NA | 100.0 | NA | 15.8 | 68.3 | 0.867 | 0.909 | NA |
| Roupa et al. [46] | 2019 | Cyprus | healthcare | 168 | 23.6 | 69.0 | 14.9 | 40.5 | NA | 28.6 | 25.6 | 0.988 | NA | NA |
| Sartorelli et al. [47] | 2021 | Italy | healthcare | 850 | 24.0 | 62.1 | 4.6 | 98.6 | NA | 90.0 | 10.0 | 0.698 | 0.80 | 0 (0) |
| Schmid et al. [48] | 2004 | Germany | medical and dental | 804 | 22.4 | 63.4 | NA | 58.0 | NA | NA | NA | 0.55 | NA | NA |
| Sernia et al. [49] | 2014 | Italy | healthcare | 369 | 25.4 | 71.0 | NA | 84.8 | NA | NA | NA | 0.46 | NA | NA |
| Sheek-Hussein et al. [50] | 2012 | UAE | medical | 181 | 21.2 | 61.0 | NA | 40.3 | NA | 40.0 | NA | 0.48 | NA | NA |
| Spradling et al. [51] | 2012 | USA | healthcare | 2481 | 23.2 | 64.6 | 14.0 | 100.0 | 8.7 | NA | NA | 0.929 | NA | 2 (0.025) |
| Stefanati et al. [52] | 2019 | Italy | medical (including residents) | 621 | 24.6 | 60.7 | NA | 100.0 | 18.9 | 58.1 | 41.9 | 0.723 | 0.926 | 0 (0) |
| Tohme et al. [53] | 2011 | USA | healthcare | 3588 | NA | NA | NA | 59.7 | 0.81 | NA | NA | 0.92 | 0.633 | 18 (0.327) |
| Torda et al. [54] | 2008 | Australia | medical | 733 | NA | NA | 55.0 | 44.2 | NA | NA | NA | 0.705 | NA | NA |
| Trevisan et al. [55] | 2019 | Italy | healthcare | 10294 | 20.8 | 65.8 | 0 | 100.0 | 16.4 | 49.8 | 50.2 | 0.685 | 0.920 | NA |
| van Leeuwen et al. [56] | 2021 | Netherlands | medical | 2922 | 19.5 | 66.0 | NA | 100.0 | 0.08 | 0 | 100.0 | 0.989 | NA | 3 (0.125) |
| Verso et al. [57] | 2017 | Italy | medical (including residents) | 2114 | 26.6 | 39.7 | 0.1 | 100.0 | 19.5 | 41.1 | 58.9 | 0.619 | NA | NA |
| Verso et al. [58] | 2019 | Italy | nursing | 520 | 21.9 | 65.2 | NA | 100.0 | 20.0 | 83.8 | 16.2 | 0.377 | 0.94 | NA |
| Verso et al. [59] | 2020 | Italy | nursing | 483 | 21.7 | 66.9 | NA | 100.0 | NA | 82.4 | 17.6 | 0.474 | NA | NA |
| Wicker et al. [60] | 2007 | Germany | medical | 164 | NA | 65.5 | NA | 100.0 | NA | NA | NA | 0.945 | NA | NA |
| Yoda et al. [61] | 2021 | Japan | medical | 999 | 20.1 | 67.7 | NA | 97.7 | 0.25 | NA | NA | 0.906 | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahmani, A.; Montecucco, A.; Kusznir Vitturi, B.; Debarbieri, N.; Dini, G.; Durando, P. Long-Term Effectiveness of Hepatitis B Vaccination in the Protection of Healthcare Students in Highly Developed Countries: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1841. https://doi.org/10.3390/vaccines10111841
Rahmani A, Montecucco A, Kusznir Vitturi B, Debarbieri N, Dini G, Durando P. Long-Term Effectiveness of Hepatitis B Vaccination in the Protection of Healthcare Students in Highly Developed Countries: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(11):1841. https://doi.org/10.3390/vaccines10111841
Chicago/Turabian StyleRahmani, Alborz, Alfredo Montecucco, Bruno Kusznir Vitturi, Nicoletta Debarbieri, Guglielmo Dini, and Paolo Durando. 2022. "Long-Term Effectiveness of Hepatitis B Vaccination in the Protection of Healthcare Students in Highly Developed Countries: A Systematic Review and Meta-Analysis" Vaccines 10, no. 11: 1841. https://doi.org/10.3390/vaccines10111841
APA StyleRahmani, A., Montecucco, A., Kusznir Vitturi, B., Debarbieri, N., Dini, G., & Durando, P. (2022). Long-Term Effectiveness of Hepatitis B Vaccination in the Protection of Healthcare Students in Highly Developed Countries: A Systematic Review and Meta-Analysis. Vaccines, 10(11), 1841. https://doi.org/10.3390/vaccines10111841