
Diagnostic Utility of N-Terminal Pro-B-Type Natriuretic Peptide in Identifying Atrial Fibrillation Post-Cryptogenic Stroke: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
- What is the diagnostic accuracy of NT-proBNP in detecting AF in patients with cryptogenic stroke? (As a secondary aim, we will investigate NT-proBNP accuracy in cohorts where the stroke’s etiology is established, thus formulating our secondary research question).
- What is the diagnostic accuracy of NT-proBNP in detecting AF in patients with stroke of known etiology?
2. Methods
2.1. Literature Search: Identification and Selection of Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Methodological Quality Assessment of Included Studies
2.5. Statistical Analyses
3. Results
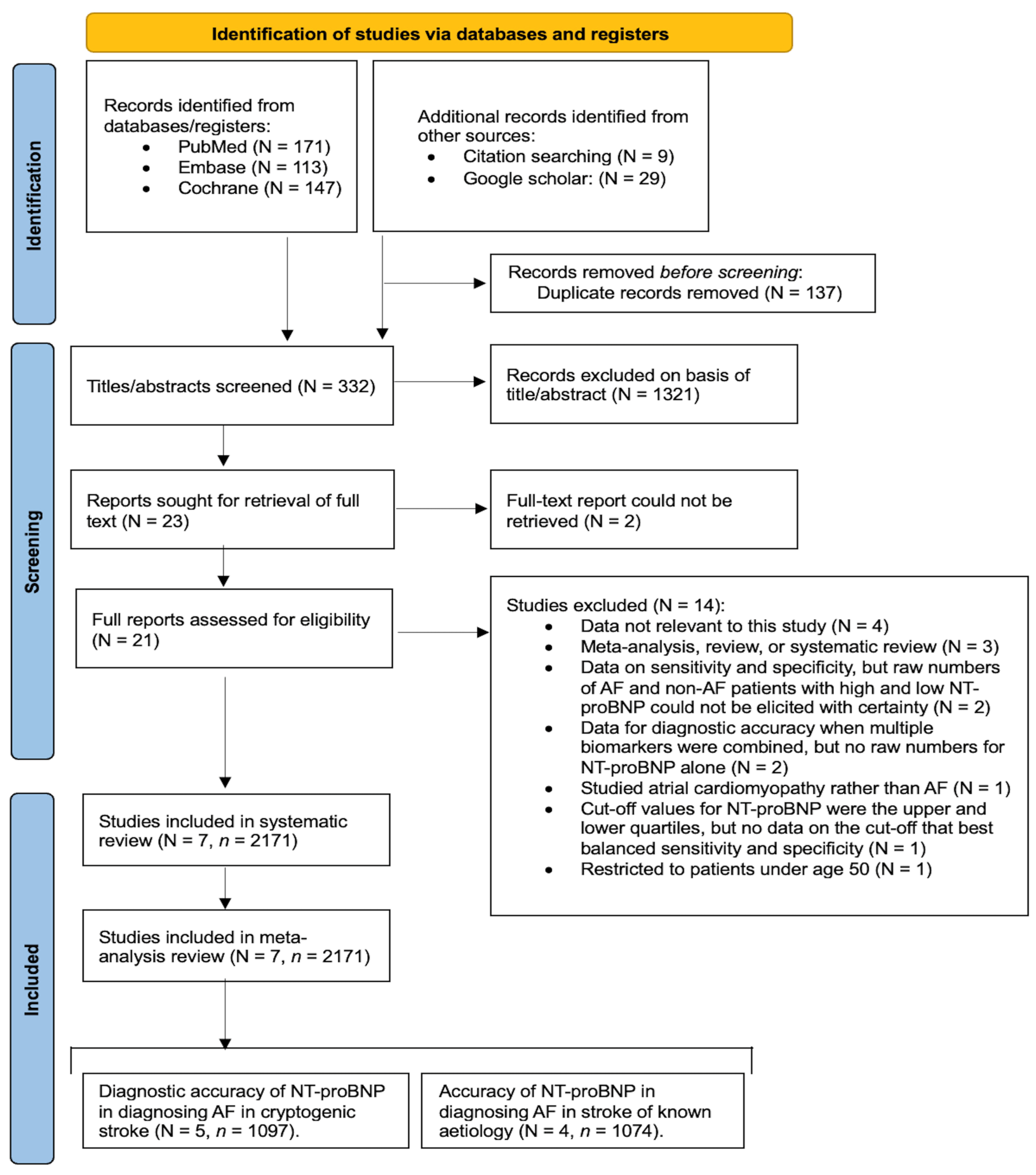
3.1. Results of the Search
3.2. Description of the Included Studies
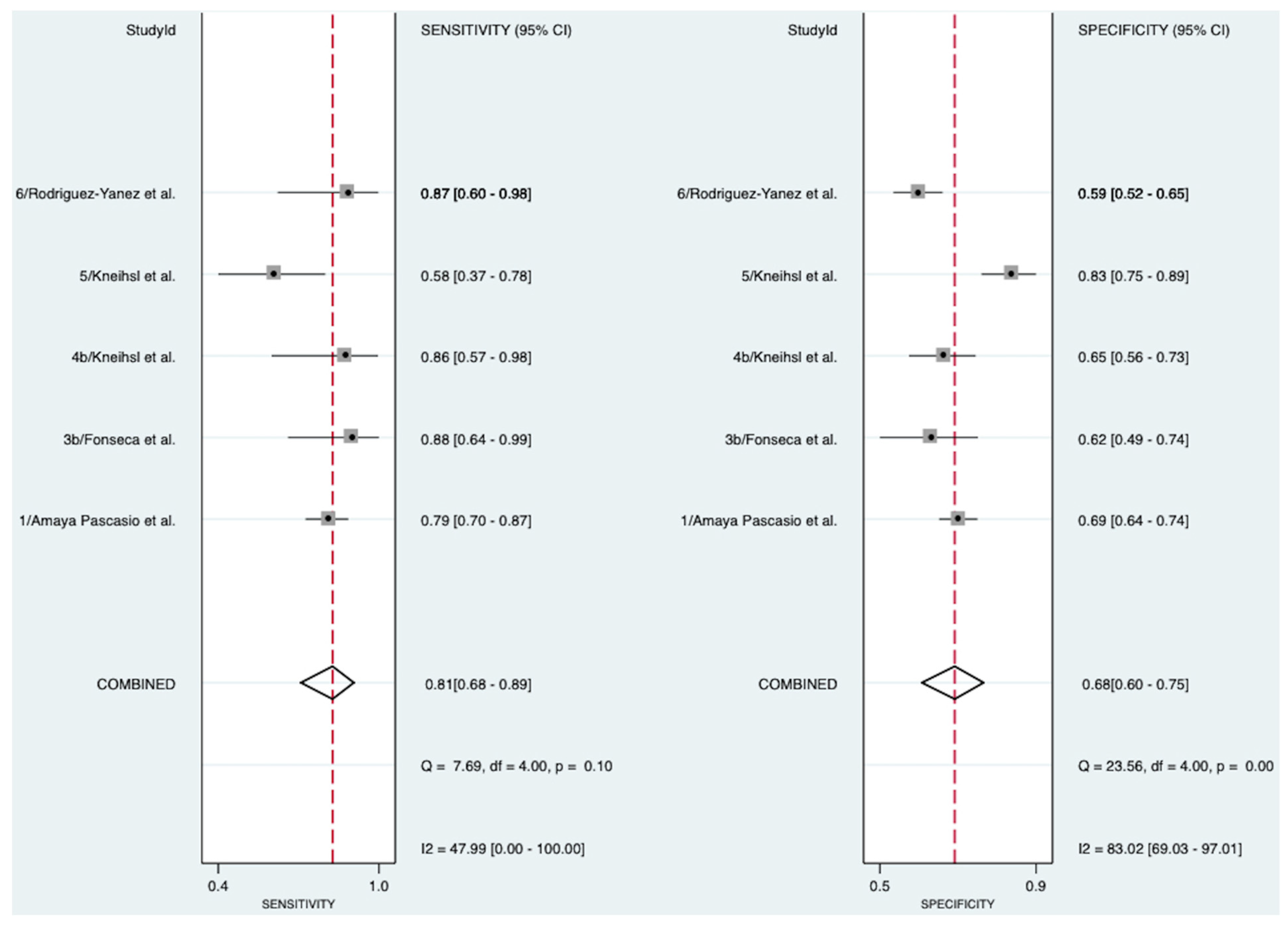
3.3. Diagnostic Accuracy of NT-proBNP in Detecting Atrial Fibrillation in Patients with Cryptogenic Stroke
3.4. Diagnostic Accuracy of NT-proBNP in Detecting Atrial Fibrillation in Patients with Stroke of Known Etiology
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| ECG | Electrocardiography |
| ICM | Implantable cardiac monitor |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| BNP | B-type natriuretic peptide |
| RAAS | Renin-angiotensin-aldosterone system |
| AUROC | Area Under the Receiver Operating Curve |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| MOOSE | Meta-analysis of Observational Studies in Epidemiology |
| STARD | Standards for Reporting Diagnostic Accuracy Studies |
| SROC | Summary receiver operating characteristic |
References
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Nesheiwat, Z.; Goyal, A.; Jagtap, M. Atrial Fibrillation. StatPearls 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK568719/ (accessed on 24 March 2024).
- Chamberlain, A.M.; Agarwal, S.K.; Folsom, A.R.; Duval, S.; Soliman, E.Z.; Ambrose, M.; Eberly, L.E.; Alonso, A. Smoking and incidence of atrial fibrillation: Results from the Atherosclerosis Risk in Communities (ARIC) study. Heart Rhythm. 2011, 8, 1160–1166. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Elkind, M.S.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke: Time for a New Model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, J.D.; Seeher, K.M.; Schiess, N.; Nichols, E.; Cao, B.; Servili, C.; Cavallera, V.; Cousin, E.; Hagins, H.; Moberg, M.E.; et al. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024, 23, 344–381. [Google Scholar] [CrossRef] [PubMed]
- Wasser, K.; Weber-Krüger, M.; Jürries, F.; Liman, J.; Hamann, G.F.; Kermer, P.; Uphaus, T.; Protsenko, E.; Seegers, J.; Mende, M.; et al. The cardiac diagnostic work-up in stroke patients-A subanalysis of the Find-AFRANDOMISED trial. PLoS ONE 2019, 14, e0216530. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Mac Grory, B.; Flood, S.P.; Apostolidou, E.; Yaghi, S. Cryptogenic Stroke: Diagnostic Workup and Management. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 77. [Google Scholar] [CrossRef]
- Xu, J.; Sethi, P.; Biby, S.; Allred, J.; Seiler, A.; Sabir, R. Predictors of atrial fibrillation detection and features of recurrent strokes in patients after cryptogenic stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104934. [Google Scholar] [CrossRef]
- Skrebelyte-Strøm, L.; Rønning, O.M.; Dahl, F.A.; Steine, K.; Kjekshus, H. Prediction of occult atrial fibrillation in patients after cryptogenic stroke and transient ischaemic attack: PROACTIA. Europace 2022, 24, 1881–1888. [Google Scholar] [CrossRef]
- Acampa, M.; Lazzerini, P.E.; Lattanzi, S.; Rubiera, M. Cryptogenic stroke as a working diagnosis: The need for an early and comprehensive diagnostic work-up. BMC Neurol. 2023, 23, 153. [Google Scholar] [CrossRef] [PubMed]
- Kneihsl, M.; Gattringer, T.; Bisping, E.; Scherr, D.; Raggam, R.; Mangge, H.; Enzinger, C.; Fandler-Höfler, S.; Eppinger, S.; Hermetter, C.; et al. Blood Biomarkers of Heart Failure and Hypercoagulation to Identify Atrial Fibrillation–Related Stroke. Stroke 2019, 50, 2223–2226. [Google Scholar] [CrossRef]
- Novack, M.L.; Zubair, M. Natriuretic Peptide B Type Test. StatPearls 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK556136/ (accessed on 24 March 2024).
- Weber, M.; Hamm, C. Role of B-type natriuretic peptide (BNP) and NT-proBNP in clinical routine. Heart 2006, 92, 843–849. [Google Scholar] [CrossRef]
- Zhang, K.; Kamtchum-Tatuene, J.; Li, M.; Jickling, G.C. Cardiac natriuretic peptides for diagnosis of covert atrial fibrillation after acute ischaemic stroke: A meta-analysis of diagnostic accuracy studies. Stroke Vasc. Neurol. 2021, 6, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Amaya Pascasio, L.; Quesada Lopez, M.; Garcia-Torrecillas, J.M.; Arjona-Padillo, A.; Martinez Sanchez, P. Development of a Score to Predict the Paroxysmal Atrial Fibrillation in Stroke Patients: The Screening for Atrial Fibrillation Scale. Front. Neurol. 2022, 13, 900582. [Google Scholar] [CrossRef]
- Fonseca, A.C.; Matias, J.S.; Pinho e Melo, T.; Falcao, F.; Canhao, P.; Ferro, J.M. N-terminal probrain natriuretic peptide as a biomarker of cardioembolic stroke. Int. J. Stroke 2011, 6, 398–403. [Google Scholar] [CrossRef]
- Fonseca, A.C.; Brito, D.; Pinho e Melo, T.; Geraldes, R.; Canhao, P.; Caplan, L.R.; Ferro, J.M. N-terminal pro-brain natriuretic peptide shows diagnostic accuracy for detecting atrial fibrillation in cryptogenic stroke patients. Int. J. Stroke 2014, 9, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Kneihsl, M.; Bisping, E.; Scherr, D.; Mangge, H.; Fandler-Hofler, S.; Colonna, I.; Haidegger, M.; Eppinger, S.; Hofer, E.; Fazekas, F.; et al. Predicting atrial fibrillation after cryptogenic stroke via a clinical risk score-a prospective observational study. Eur. J. Neurol. 2022, 29, 149–157. [Google Scholar] [CrossRef]
- Rodriguez-Yanez, M.; Arias-Rivas, S.; Santamaria-Cadavid, M.; Sobrino, T.; Castillo, J.; Blanco, M. High pro-BNP levels predict the occurrence of atrial fibrillation after cryptogenic stroke. Neurology 2013, 81, 444–447. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, Y.; Yuan, F.; Song, C.; Jiang, Y.; Gao, Q.; Leng, X.; Jiang, W. Diagnostic value of N-terminal pro B-type natriuretic peptide for nonvalvular atrial fibrillation in acute ischemic stroke patients: A retrospective multicenter case-control study. J. Neurol. Sci. 2020, 414, 116822. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Simundic, A.-M. Measures of Diagnostic Accuracy: Basic Definitions. Med. Biol. Sci. 2008, 22. Available online: https://www.researchgate.net/publication/267722807_Measures_of_Diagnostic_Accuracy_Basic_Definitions (accessed on 24 March 2024).
- Higgins, J.P.T.T.J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). 2022. Available online: https://training.cochrane.org/handbook/archive/v6.3 (accessed on 24 March 2024).
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Suissa, L.; Bertora, D.; Lachaud, S.; Mahagne, M.H. Score for the targeting of atrial fibrillation (STAF): A new approach to the detection of atrial fibrillation in the secondary prevention of ischemic stroke. Stroke 2009, 40, 2866–2868. [Google Scholar] [CrossRef] [PubMed]
- Sanak, D.; Hutyra, M.; Kral, M.; Bartkova, A.; Zapletalova, J.; Fedorco, M.; Veverka, T.; Vindis, D.; Dornak, T.; Skala, T.; et al. Paroxysmal atrial fibrillation in young cryptogenic ischemic stroke: A 3-week ECG Holter monitoring study. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc Czech Repub. 2015, 159, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.; Vail, A.; Cameron, A.; Katan, M.; Lip, G.Y.; Dawson, J.; Smith, C.J.; Kishore, A.K. Molecular biomarkers predicting newly detected atrial fibrillation after ischaemic stroke or TIA: A systematic review. Eur. Stroke J. 2022, 8, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.Y.; Diederichsen, S.Z.; Højberg, S.; Krieger, D.W.; Graff, C.; Frikke-Schmidt, R.; Olesen, M.S.; Brandes, A.; Køber, L.; Haugan, K.J.; et al. Effects of Atrial Fibrillation Screening According to N-Terminal Pro-B-Type Natriuretic Peptide: A Secondary Analysis of the Randomized LOOP Study. Circulation 2023, 147, 1788–1797. [Google Scholar] [CrossRef]
- Shi, M.; Liu, L.; Wafa, H.; Curcin, V.; Wang, Y. Effectiveness and safety of non-vitamin K oral anticoagulants versus warfarin in patients with atrial fibrillation and previous stroke: A systematic review and meta-analysis. Neuroepidemiology 2023, 58, 1–14. [Google Scholar] [CrossRef]
- Patel, J.; Bhaskar, S. Atrial Fibrillation and Reperfusion Therapy in Acute Ischaemic Stroke Patients: Prevalence and Outcomes-A Comprehensive Systematic Review and Meta-Analysis. Neurol. Int. 2023, 15, 1014–1043. [Google Scholar] [CrossRef] [PubMed]
- Ludhwani, D.; Wieters, J.S. Paroxysmal Atrial Fibrillation. StatPearls 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK535439/ (accessed on 24 March 2024).
- Ratajczak-Tretel, B.; Lambert, A.T.; Al-Ani, R.; Arntzen, K.; Bakkejord, G.K.; Bekkeseth, H.M.O.; Bjerkeli, V.; Eldøen, G.; Gulsvik, A.K.; Halvorsen, B.; et al. Underlying causes of cryptogenic stroke and TIA in the nordic atrial fibrillation and stroke (NOR-FIB) study—The importance of comprehensive clinical evaluation. BMC Neurol. 2023, 23, 115. [Google Scholar] [CrossRef] [PubMed]
- Hariri, E.; Hachem, A.; Sarkis, G.; Nasr, S. Optimal Duration of Monitoring for Atrial Fibrillation in Cryptogenic Stroke: A Nonsystematic Review. Biomed. Res. Int. 2016, 2016, 5704963. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, H.; Liu, C.; Ren, Y.; Sun, C. NT Pro-BNP can be used as a risk predictor of clinical atrial fibrillation with or without left atrial enlargement. Clin. Cardiol. 2022, 45, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Nasab Mehrabi, E.; Toupchi-Khosroshahi, V.; Athari, S.S. Relationship of atrial fibrillation and N terminal pro brain natriuretic peptide in heart failure patients. ESC Heart Fail. 2023, 10, 3250–3257. [Google Scholar] [CrossRef] [PubMed]
- Didier, R.; Garnier, L.; Duloquin, G.; Meloux, A.; Sagnard, A.; Graber, M.; Dogon, G.; Benali, K.; Pommier, T.; Laurent, G.; et al. Distribution of atrial cardiomyopathy markers and association with atrial fibrillation detected after ischaemic stroke in the SAFAS study. Stroke Vasc. Neurol. 2023, 9, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Armoundas, A.A.; Narayan, S.M.; Arnett, D.K.; Spector-Bagdady, K.; Bennett, D.A.; Celi, L.A.; Friedman, P.A.; Gollob, M.H.; Hall, J.L.; Kwitek, A.E.; et al. Use of Artificial Intelligence in Improving Outcomes in Heart Disease: A Scientific Statement From the American Heart Association. Circulation 2024, 149, e1028–e1050. [Google Scholar] [CrossRef]
- Tancin Lambert, A.; Ratajczak-Tretel, B.; Al-Ani, R.; Arntzen, K.; Bakkejord, G.K.; Bekkeseth, H.M.O.; Bjerkeli, V.; Eldøen, G.; Gulsvik, A.K.; Halvorsen, B.; et al. Biomarkers predictive of atrial fibrillation in patients with cryptogenic stroke. Insights from the Nordic Atrial Fibrillation and Stroke (NOR-FIB) study. Eur. J. Neurol. 2023, 30, 1352–1363. [Google Scholar] [CrossRef]
- Costabel, J.; Burgos, L.; Trivi, M. The Significance Of Troponin Elevation in Atrial Fibrillation. J. Atr. Fibrillation 2017, 9, 1530. [Google Scholar] [CrossRef]
- Ward, F.; McGovern, R.; Cotter, P. Troponin-I Is a Predictor of a Delayed Diagnosis of Atrial Fibrillation in Acute Ischemic Stroke and Transient Ischemic Attack. J. Stroke Cerebrovasc. Dis. 2014, 24, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Palà, E.; Pagola, J.; Juega, J.; Francisco-Pascual, J.; Bustamante, A.; Penalba, A.; Comas, I.; Rodriguez, M.; De Lera Alfonso, M.; Arenillas, J.F.; et al. B-type natriuretic peptide over N-terminal pro-brain natriuretic peptide to predict incident atrial fibrillation after cryptogenic stroke. Eur. J. Neurol. 2021, 28, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Ederhy, S.; Meuleman, C.; Di Angelantonio, E.; Dufaitre, G.; Boccara, F. d-dimers in atrial fibrillation: A further step in risk stratification of thrombo-embolism? Eur. Heart J. 2007, 28, 2179–2180. [Google Scholar] [CrossRef]
- Li, X.; Peng, S.; Wu, X.; Guan, B.; Tse, G.; Chen, S.; Zhou, G.; Wei, Y.; Gong, C.; Lu, X.; et al. C-reactive protein and atrial fibrillation: Insights from epidemiological and Mendelian randomization studies. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Gong, M.; Cheung, A.; Wang, Q.S.; Li, G.; Goudis, C.; Bazoukis, G.; Lip, G.; Baranchuk, A.; Korantzopoulos, P.; Letsas, K.; et al. Galectin-3 and risk of atrial fibrillation: A systematic review and meta-analysis. J. Clin. Lab. Anal. 2020, 34, e23104. [Google Scholar] [CrossRef] [PubMed]
- Garnier, L.; Duloquin, G.; Meloux, A.; Benali, K.; Sagnard, A.; Graber, M.; Dogon, G.; Didier, R.; Pommier, T.; Vergely, C.; et al. Multimodal Approach for the Prediction of Atrial Fibrillation Detected After Stroke: SAFAS Study. Front. Cardiovasc. Med. 2022, 9, 949213. [Google Scholar] [CrossRef] [PubMed]
- Pauklin, P.; Zilmer, M.; Eha, J.; Tootsi, K.; Kals, M.; Kampus, P. Markers of Inflammation, Oxidative Stress, and Fibrosis in Patients with Atrial Fibrillation. Oxid. Med. Cell Longev. 2022, 2022, 4556671. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, K.; Zhao, L.; Guo, J.; Hu, X.; Chen, Z. Increased serum HMGB1 is related to oxidative stress in patients with atrial fibrillation. J. Int. Med. Res. 2013, 41, 1796–1802. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Killingsworth, M.; Bhaskar, S. Is Composition of Brain Clot Retrieved by Mechanical Thrombectomy Associated with Stroke Aetiology and Clinical Outcomes in Acute Ischemic Stroke?—A Systematic Review and Meta-Analysis. Neurol. Int. 2022, 14, 748–770. [Google Scholar] [CrossRef]
- Bhaskar, S.; Cordato, D.; Cappelen-Smith, C.; Cheung, A.; Ledingham, D.; Celermajer, D.; Levi, C. Clarion call for histopathological clot analysis in “cryptogenic” ischemic stroke: Implications for diagnosis and treatment. Ann. Clin. Transl. Neurol. 2017, 4, 926–930. [Google Scholar] [CrossRef]
- Bhaskar, S.; Saab, J.; Cappelen-Smith, C.; Killingsworth, M.; Wu, X.; Cheung, A.; Manning, N.; Aouad, P.; McDougall, A.; Hodgkinson, S.; et al. Clot Histopathology in Ischemic Stroke with Infective Endocarditis. Can. J. Neurol. Sci. J. Can. Des. Sci. Neurol. 2019, 46, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, D.; Bajpai, R.; Ng, G.J.L.; Soljak, M.; Marks, R.S.; Cheung, C.; Arumugam, T.V.; Quek, A.M.L.; Tok, A.I.Y.; Seet, R.C.S. Blood biomarkers to detect new-onset atrial fibrillation and cardioembolism in ischemic stroke patients. Heart Rhythm. 2021, 18, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, K.; Watanabe, K.; Zeniya, S.; Ito, Y.; Hizume, M.; Kanazawa, T.; Tomita, M.; Ishibashi, S.; Miake, H.; Tanaka, H.; et al. A Score for Predicting Paroxysmal Atrial Fibrillation in Acute Stroke Patients: iPAB Score. J. Stroke Cerebrovasc. Dis. 2015, 24, 2263–2269. [Google Scholar] [CrossRef] [PubMed]
- Kishore, A.K.; Hossain, M.J.; Cameron, A.; Dawson, J.; Vail, A.; Smith, C.J. Use of risk scores for predicting new atrial fibrillation after ischemic stroke or transient ischemic attack-A systematic review. Int. J. Stroke 2022, 17, 608–617. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Pagola, J.; Juega, J.; Francisco-Pascual, J.; Bustamante, A.; Penalba, A.; Pala, E.; Rodriguez, M.; De Lera-Alfonso, M.; Arenillas, J.F.; Cabezas, J.A.; et al. Predicting Atrial Fibrillation with High Risk of Embolization with Atrial Strain and NT-proBNP. Transl. Stroke Res. 2021, 12, 735–741. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| StudyID | Author | Year | Country | Study Type | Stroke Cohort | Number of Patients (n) | Male (n, %) | Age (Mean, SD) | AF Detection Method | Cryptogenic Stroke Diagnosis Method | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | AF | Non-AF | ||||||||||
| 1 | Amaya Pascasio et al. [17] | 2022 | Spain | Prospective a | Cryptogenic stroke | 460 | 308 (66.96) | 65.0 (13.4) | 74.7 (9.0) | 62.0 (13.4) | Measured for at least 72 h with telemetry or Holter monitoring during hospitalization (and additional Holter monitoring was at the discretion of the neurologist). Additionally, a TTE was conducted during hospitalization or within 3 months. | Cryptogenic stroke was diagnosed where previously known AF, AF found at the emergency ECG, and other major cardioembolic causes were excluded. Patients with incomplete etiological investigations (e.g., missing TTE) were also excluded. |
| 2 | Fonseca et al. [18] | 2011 | Portugal | Prospective | Known etiology b | 66 | 40 (60.61) | - | 63 (16) | 59 (14) | At least two ECGs during hospitalization and 24-h Holter monitoring if the stroke cause remained undetermined. Additionally, TTE was performed in all patients, and TOE was performed in all patients aged < 55 years. | - |
| 3a | Fonseca et al. [19] | 2014 | Portugal | Prospective | Known etiology | 184 | 105 (57.07) | - | 70.3 (7.8) | 58.6 (12.7) | At least two ECGs and one 24 h Holter within the first week of presentation. Additionally, TTE was performed in all patients, and TOE was performed in all patients aged < 55 years. | - |
| 3b | Fonseca et al. [19] | 2014 | Portugal | Prospective | Cryptogenic stroke | 80 | 42 (52.50) | - | 74 (7) c | 68 (15) c | As stated above, with additional serial 24-h Holter monitoring conducted during follow-ups between 3 and 6 months. | Diagnosis of cryptogenic stroke was made using the TOAST criteria [27]. If a patient had a history of AF and no other findings were disclosed, then they were classified as cardioembolic rather than cryptogenic. |
| 4a | Kneihsl et al. [13] | 2019 | Austria | Prospective | Known etiology | 274 | 157 (57.30) | - | 77.4 (9.5) | 68.0 (12.6) | ECG on admission, ECG monitoring in the stroke unit, medical history. TTE was performed in all patients who did not have evidence of large- or small-vessel disease. TOE was performed in all patients aged < 55 or those with clinical and/or imaging signs of cardioembolism. | - |
| 4b | Kneihsl et al. [13] | 2019 | Austria | Prospective | Cryptogenic stroke | 143 | 77 (53.85) | - | 74.4 (6.7) | 66.9 (14.7) | As above, with additional stroke unit ECG monitoring of at least 48 h, regular pulse controls, and a further 24 h Holter monitoring during hospitalization. | Cryptogenic stroke was diagnosed by excluding patients with known AF or AF known immediately on admission, those with other known cardioembolic sources, those with large-vessel disease, patients with small-vessel disease, and those with specific stroke etiologies such as arterial dissection. |
| 5 | Kneihsl et al. [20] | 2022 | Austria | Prospective | Cryptogenic stroke | 150 | 85 (56.67) | 66.7 (15.3) | 75.0 (6.3) | 65.1 (15.9) | ECG on admission, continuous ECG in stroke unit, additional 24-h Holter monitoring, ECG during follow-up, and ILR offered to some patients at the discretion of the treating physicians. Additionally, echocardiography was performed for each patient. | Patients were classified as having cryptogenic stroke if there was no evidence of AF on initial ECG and 24-h Holter monitoring. |
| 6 | Rodriguez-Yanez et al. [21] | 2013 | Spain | Prospective | Cryptogenic stroke | 264 | 150 (56.82) | - | 81 (6) | 72 (9) | ECG on admission and upon any arrhythmic pulse, 24 h Holter ECG in patients with a history of palpitations. In patients aged < 50, TOE and microbubble Doppler investigations were additionally conducted to detect right-to-left shunts. | Diagnosis of cryptogenic stroke was made using the TOAST criteria [27]. Cryptogenic stroke was diagnosed when no etiological sources were found. Cases with two co-existing causes of stroke were classified as undetermined rather than cryptogenic. |
| 7 | Zhao et al. [22] | 2020 | China | Retrospective | Known etiology | 550 d | 236 (42.91) | 71 (9) | 72 (9) | 71 (9) | ECG in all patients. In those with cardioembolic stroke, ECG, and 24-h Holter after admission. This was repeated within seven days in patients with STAF ≥5, where AF was still not found [28]. Additionally, either a TEE or TOE was conducted on each patient. | - |
| Study ID | Author | Year | Stroke Cohort | Number of Patients (n) | Hypertension (n, %) | Diabetes (n, %) | Dyslipidemia (n, %) | Smoking (n, %) |
|---|---|---|---|---|---|---|---|---|
| 1 | Amaya Pascasio et al. [17] | 2022 | Cryptogenic stroke | 460 | 276 (60.00) | 114 (24.78) | 191 (41.52) | 240 (52.17) |
| 2 | Fonseca et al. [18] | 2011 | Known etiology | 66 | 33 (50.00) | 8 (12.12) | 20 (30.30) | 26 (39.39) |
| 3a | Fonseca et al. [19] | 2014 | Known etiology | 184 | 127 (69.02) | 47 (25.54) | 83 (45.11) | 43 (23.37) |
| 3b | Fonseca et al. [19] | 2014 | Cryptogenic stroke | 80 | 57 (71.25) | 23 (28.75) | 26 (32.50) | 7 (8.75) |
| 4a | Kneihsl et al. [13] | 2019 | Known etiology | 274 | 236 (86.13) | 35 (12.77) | 162 (59.12) | 86 (31.39) |
| 4b | Kneihsl et al. [13] | 2019 | Cryptogenic stroke | 143 | 111 (77.62) | 30 (20.98) | 71 (49.65) | 40 (27.97) |
| 5 | Kneihsl et al. [20] | 2022 | Cryptogenic stroke | 150 | 100 (66.67) | 24 (16.00) | 72 (48.00) | 36 (24.00) |
| 6 | Rodriguez-Yanez et al. [21] | 2013 | Cryptogenic stroke | 264 | 138 (52.27) | 68 (25.76) | 78 (29.55) | 53 (20.08) |
| 7 | Zhao et al. [22] | 2020 | Known etiology | 550 | 417 (75.82) | 119 (21.64) | - | 75 (13.64) |
| Study ID | Author | Year | Stroke Cohort | Sensitivity (%) | Specificity (%) | NT-proBNP Cut-Off (pg/mL) |
|---|---|---|---|---|---|---|
| 1 | Amaya Pascasio et al. [17] | 2022 | Cryptogenic stroke | 81/102 (79.4) | 247/358 (69.0) | 250 |
| 2 | Fonseca et al. [18] | 2011 | Known etiology | 17/18 (94.4) | 35/48 (72.9) | 265.5 |
| 3a | Fonseca et al. [19] | 2014 | Known etiology | 55/55 (100.0) | 91/129 (70.5) | 265.5 |
| 3b | Fonseca et al. [19] | 2014 | Cryptogenic stroke | 15/17 (88.2) | 39/63 (61.9) | 265.5 |
| 4a | Kneihsl et al. [13] | 2019 | Known etiology | 96/103 (93.2) | 123/171 (71.9) | 505 |
| 4b | Kneihsl et al. [13] | 2019 | Cryptogenic stroke | 12/14 (85.7) | 84/129 (65.1) | 505 |
| 5 | Kneihsl et al. [20] | 2022 | Cryptogenic stroke | 14/24 (58.3) | 104/126 (82.5) | 505 |
| 6 | Rodriguez-Yanez et al. [21] | 2013 | Cryptogenic stroke | 13/15 (86.7) | 146/249 (58.6) | 360 |
| 7 | Zhao et al. [22] | 2020 | Known etiology | 252/275 (91.6) | 222/275 (80.7) | 431 |
| Cryptogenic Stroke (95% CI) | Stroke of Known Etiology (95% CI) | |
|---|---|---|
| Number of studies | 5 | 4 |
| Number of patients | 1097 | 1074 |
| AUROC | 0.80 (0.76–0.83) | 0.91 (0.88–0.93) |
| Sensitivity | 0.81 (0.68–0.89) | 0.95 (0.90–0.97) |
| Specificity | 0.68 (0.60–0.75) | 0.75 (0.69–0.80) |
| PLR | 2.5 (2.1–3.0) | 3.7 (3.1–4.5) |
| NLR | 0.28 (0.18–0.45) | 0.07 (0.04–0.14) |
| Diagnostic odds ratio | 9 (6–14) | 52 (27–98) |
| Pre-test probability of disease | 172/1097 ≈ 0.16 | 451/1074 ≈ 0.42 |
| Deviance | 57.5 | 43.1 |
| AIC | 67.5 | 53.1 |
| BIC | 69.0 | 53.5 |
| BICdiff | 9.7 | −2.6 |
| Correlation (mixed model) | −1.00 | −1.00 |
| Proportion of heterogeneity likely due to the threshold effect | 1.00 | 1.00 |
| ICC_SEN | 0.09 (0.00–0.25) | 0.04 (0.00–0.16) |
| MED_SEN | 0.63 (0.55–0.82) | 0.58 (0.51–0.88) |
| ICC_SPE | 0.04 (0.00–0.10) | 0.01 (0.00–0.04) |
| MED_SPE | 0.59 (0.54–0.69) | 0.55 (0.51–0.65) |
| Heterogeneity (I2) | Sensitivity: 47.99 (0.00–100.00) | Sensitivity: 40.67 (0.00–100.00) |
| Specificity: 83.02 (69.03–97.01) | Specificity: 57.99 (11.72–100.00) |
| Biomarker | Definition in the Context of AF | Diagnostic Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|
| NT-proBNP | A prohormone that is released in response to myocardial stress and volume overload, which may be more likely to occur in patients with AF [14,15]. | Our investigation revealed a good-to-very-good diagnostic accuracy of NT-proBNP for detecting AF in cryptogenic stroke patients, with an AUROC of 0.80 [95% CI 0.76–0.83]. | Our findings show NT-proBNP has a very good sensitivity of 0.81 [95% CI 0.68–0.89] for detecting AF in cryptogenic stroke patients. | Our study demonstrated that NT-proBNP has a sufficient specificity of 0.68 [95% CI 0.60–0.75] for detecting AF in cryptogenic stroke patients. |
| Cardiac troponins | These cardiac enzymes are involved in myocyte contractility and may be released in greater quantities in AF patients due to myocyte damage and transient ischemia [42]. | A recent analysis reported an AUROC of 0.697 [95% CI 0.551–0.842] for hs-cTnT and an AUROC of 0.65 [95% CI 0.556–0.743] for hs-cTnI for detecting AF in cryptogenic stroke and TIA patients [41]. Comparatively, NT-proBNP had a greater AUROC of 0.725 [95% CI 0.642–0.808]. | Troponin elevations are a predictor of AF in cryptogenic stroke [43,44]; however, there is limited data on their sensitivity in this context. | Whilst troponins are associated with AF in cryptogenic stroke patients [43,44], there are limited data on their exact specificity. |
| D-dimer | A product of the degradation of fibrin, typically used in venous thromboembolism, may also be increased in patients with AF [45]. | A recent analysis reported an AUROC of 0.584 [95% CI 0.495–0.672] for detecting AF in cryptogenic stroke and TIA patients [41]. | Limited data with various indications. | Limited data with various indications. |
| CRP | CRP is a biomarker that reflects systemic inflammation, which may reflect underlying AF, though it is generally non-specific [46]. | Whilst cumulative exposure to CRP has been linked to AF, baseline CRP was shown not to be significantly associated with AF [46]. Moreover, there is a lack of data regarding the accuracy of CRP for diagnosing AF in cryptogenic stroke patients. | Limited data with various indications. | Limited data with various indications. |
| Galectin-3 | Galectin-3 is a biomarker associated with myocardial fibrosis, which can occur due to structural remodeling in AF [47]. | A prospective study reported that a galactin-3 level ≥ 9 ng/mL had a very good AUROC of 0.829 [95% CI 0.764–0.894] for detecting AF in stroke patients without previously known AF [48]. In the same study, NT-proBNP had a very good AUROC of 0.879 [95% CI 0.818–0.940]. | Limited data with various indications. | Limited data with various indications. |
| Markers of oxidative stress (MDA, 8-isoprostane) | Oxidative stress is a factor involved in the pathogenesis of AF, and there are numerous biomarkers of oxidative stress that may be elevated in AF patients [49]. | Whilst MDA activity is associated with AF [50], there are limited data on the diagnostic accuracy of oxidative stress biomarkers in the setting of cryptogenic stroke. | Limited data with various indications. | Limited data with various indications. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, J.; Bhaskar, S.M.M. Diagnostic Utility of N-Terminal Pro-B-Type Natriuretic Peptide in Identifying Atrial Fibrillation Post-Cryptogenic Stroke: A Systematic Review and Meta-Analysis. Pathophysiology 2024, 31, 331-349. https://doi.org/10.3390/pathophysiology31030024
Patel J, Bhaskar SMM. Diagnostic Utility of N-Terminal Pro-B-Type Natriuretic Peptide in Identifying Atrial Fibrillation Post-Cryptogenic Stroke: A Systematic Review and Meta-Analysis. Pathophysiology. 2024; 31(3):331-349. https://doi.org/10.3390/pathophysiology31030024
Chicago/Turabian StylePatel, Jay, and Sonu M. M. Bhaskar. 2024. "Diagnostic Utility of N-Terminal Pro-B-Type Natriuretic Peptide in Identifying Atrial Fibrillation Post-Cryptogenic Stroke: A Systematic Review and Meta-Analysis" Pathophysiology 31, no. 3: 331-349. https://doi.org/10.3390/pathophysiology31030024
APA StylePatel, J., & Bhaskar, S. M. M. (2024). Diagnostic Utility of N-Terminal Pro-B-Type Natriuretic Peptide in Identifying Atrial Fibrillation Post-Cryptogenic Stroke: A Systematic Review and Meta-Analysis. Pathophysiology, 31(3), 331-349. https://doi.org/10.3390/pathophysiology31030024