
Combination Therapy with Enalapril and Paricalcitol Ameliorates Streptozotocin Diabetes-Induced Testicular Dysfunction in Rats via Mitigation of Inflammation, Apoptosis, and Oxidative Stress

Abstract
:1. Introduction
2. Material and Methods
2.1. Animals and Experimental Design
2.2. Induction of Diabetes
2.3. Grouping and Drug Intervention
2.4. Blood Collection and Biochemical Assessment
2.5. Preparation of Testicular Tissue and Samples
2.6. Assessment of Testicular Oxidative Stress and Inflammatory Parameters
2.7. Assessment of Sperm Characteristics
2.8. Histopathological Examination
2.9. Immunohistochemical Studies
2.10. Statistical Analysis
3. Results
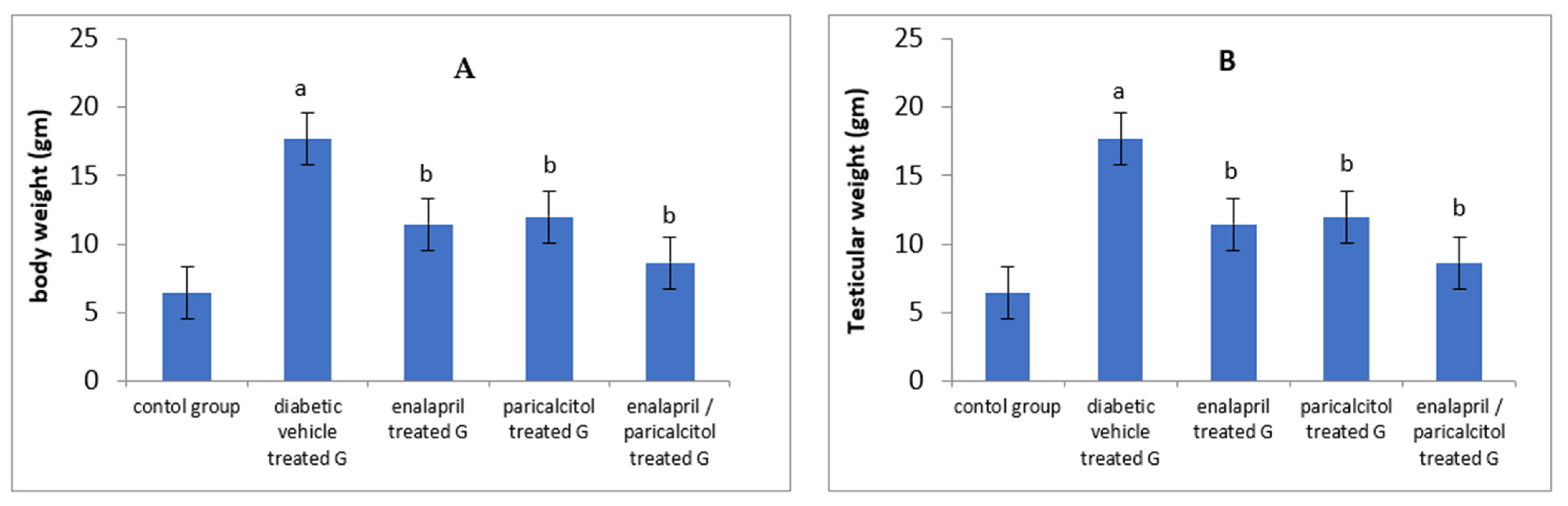
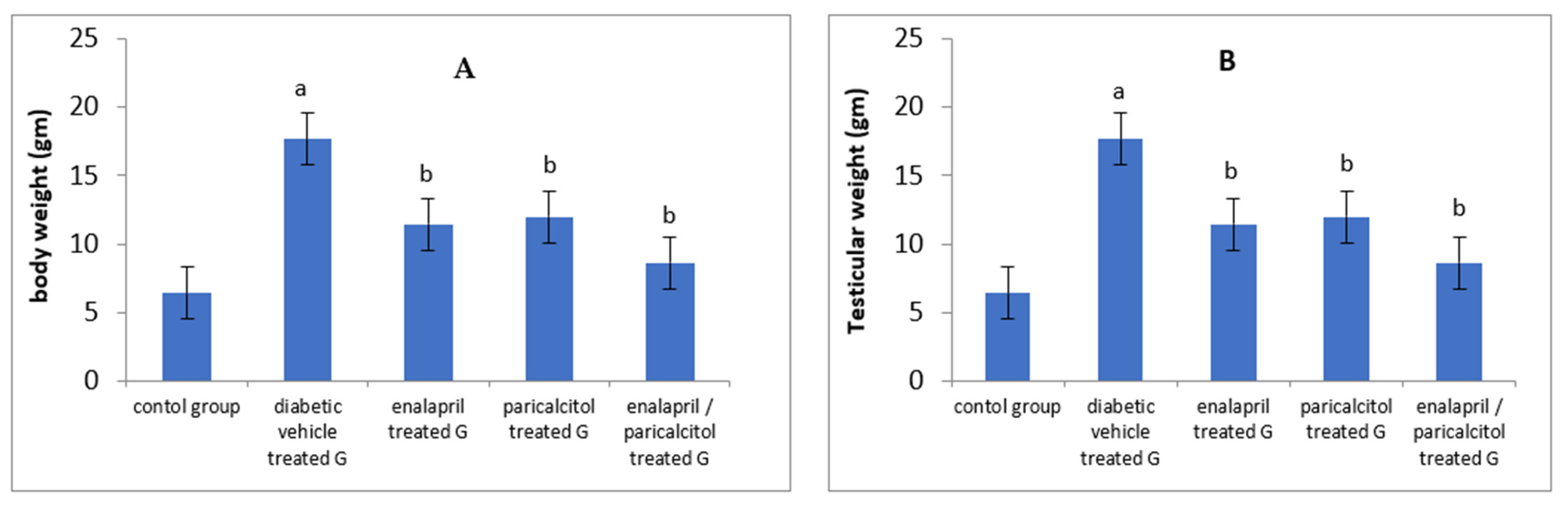
3.1. Effects of Different Treatments on Body Weight and Testicular Weight in Studied Groups
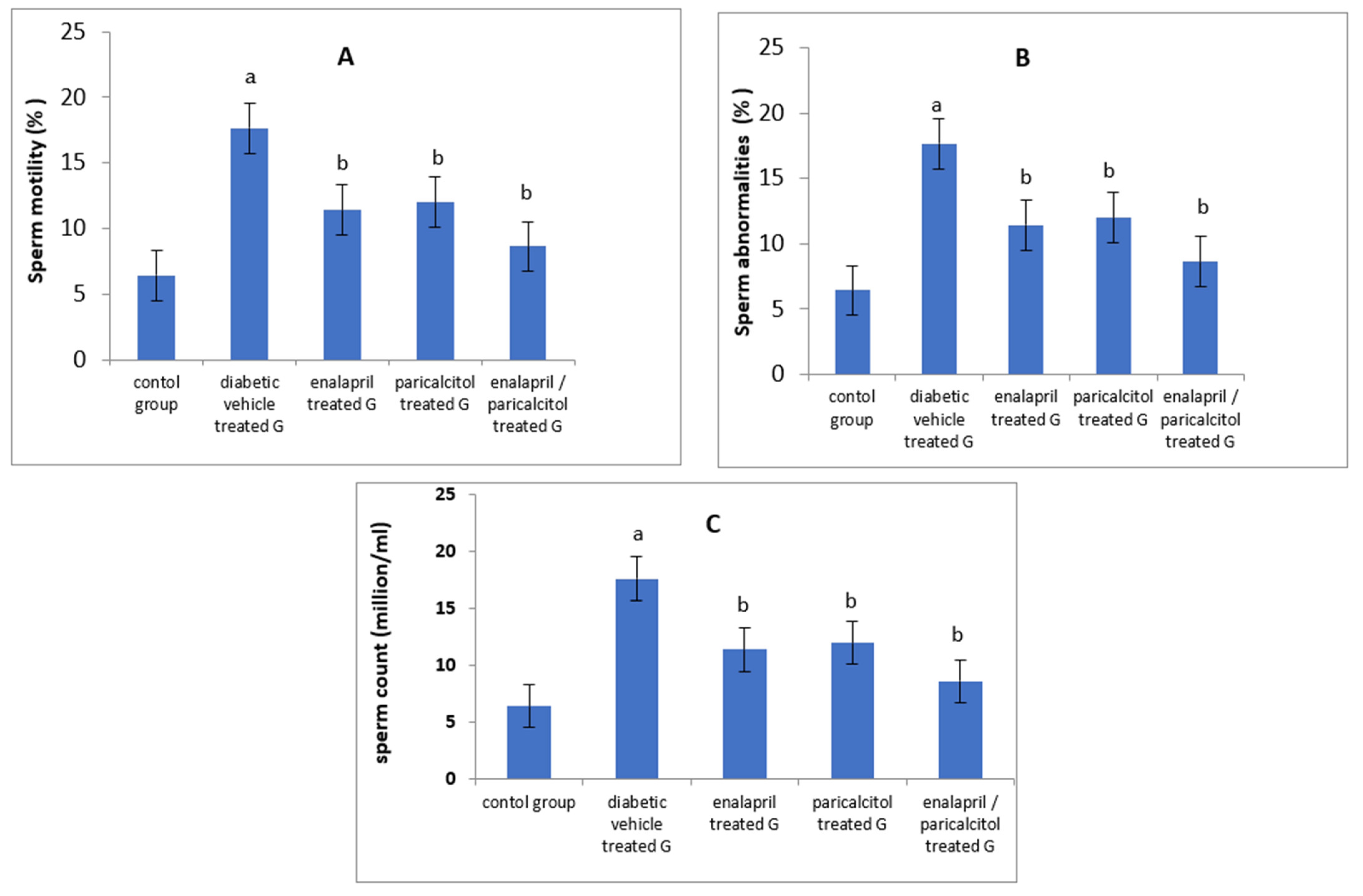
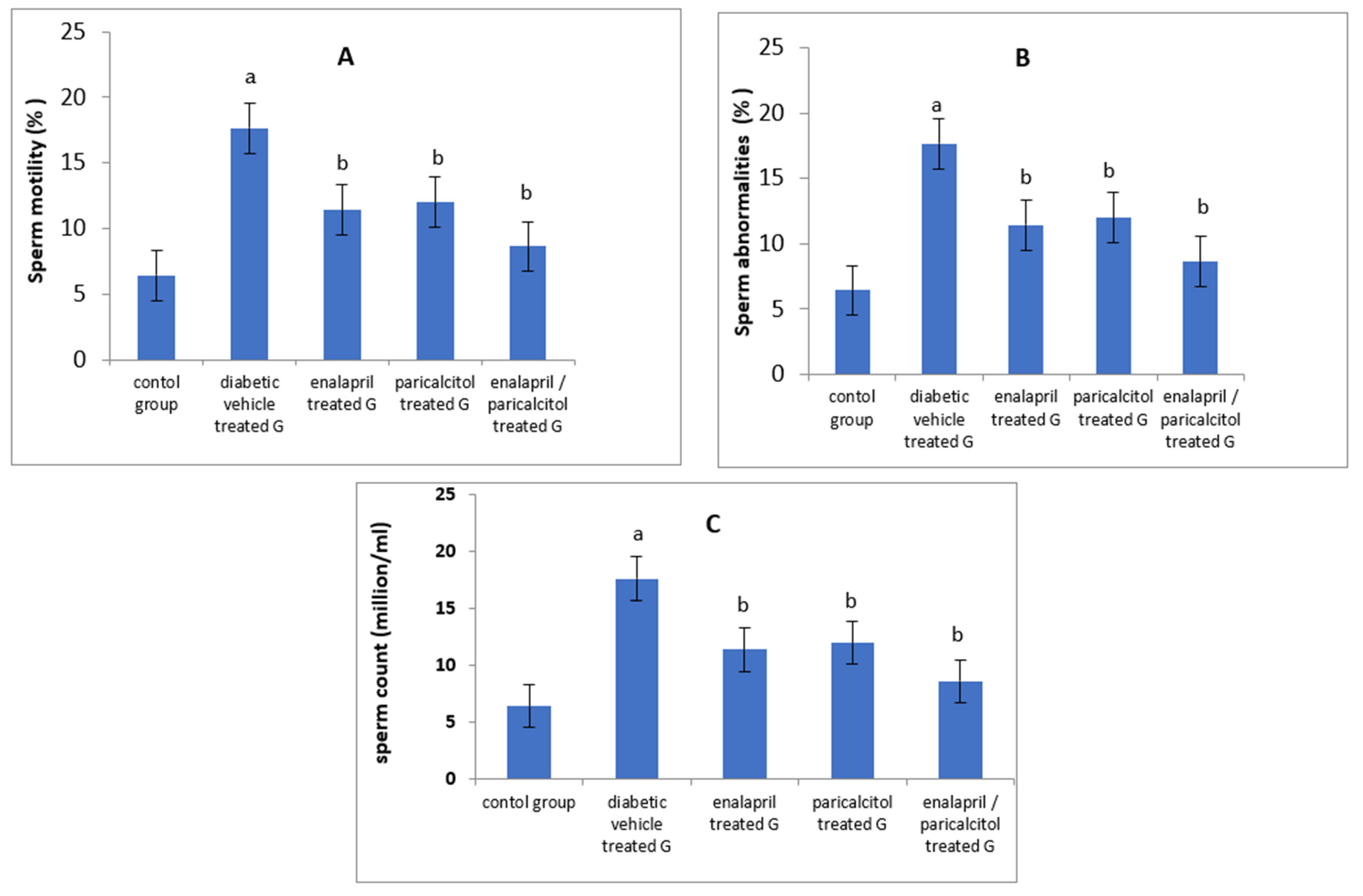
3.2. Impact of Different Treatments on Sperm Parameters in Studied Groups
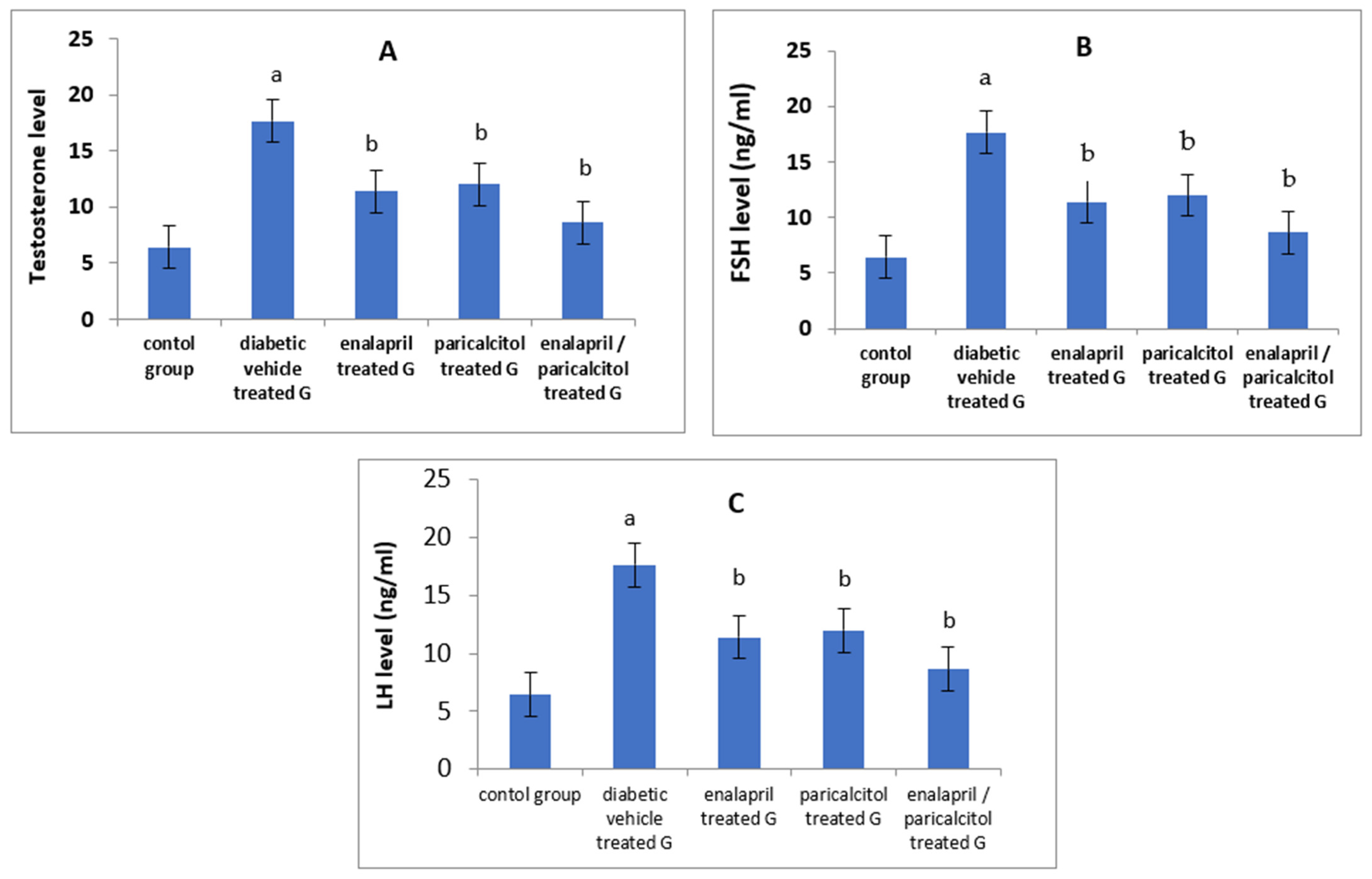
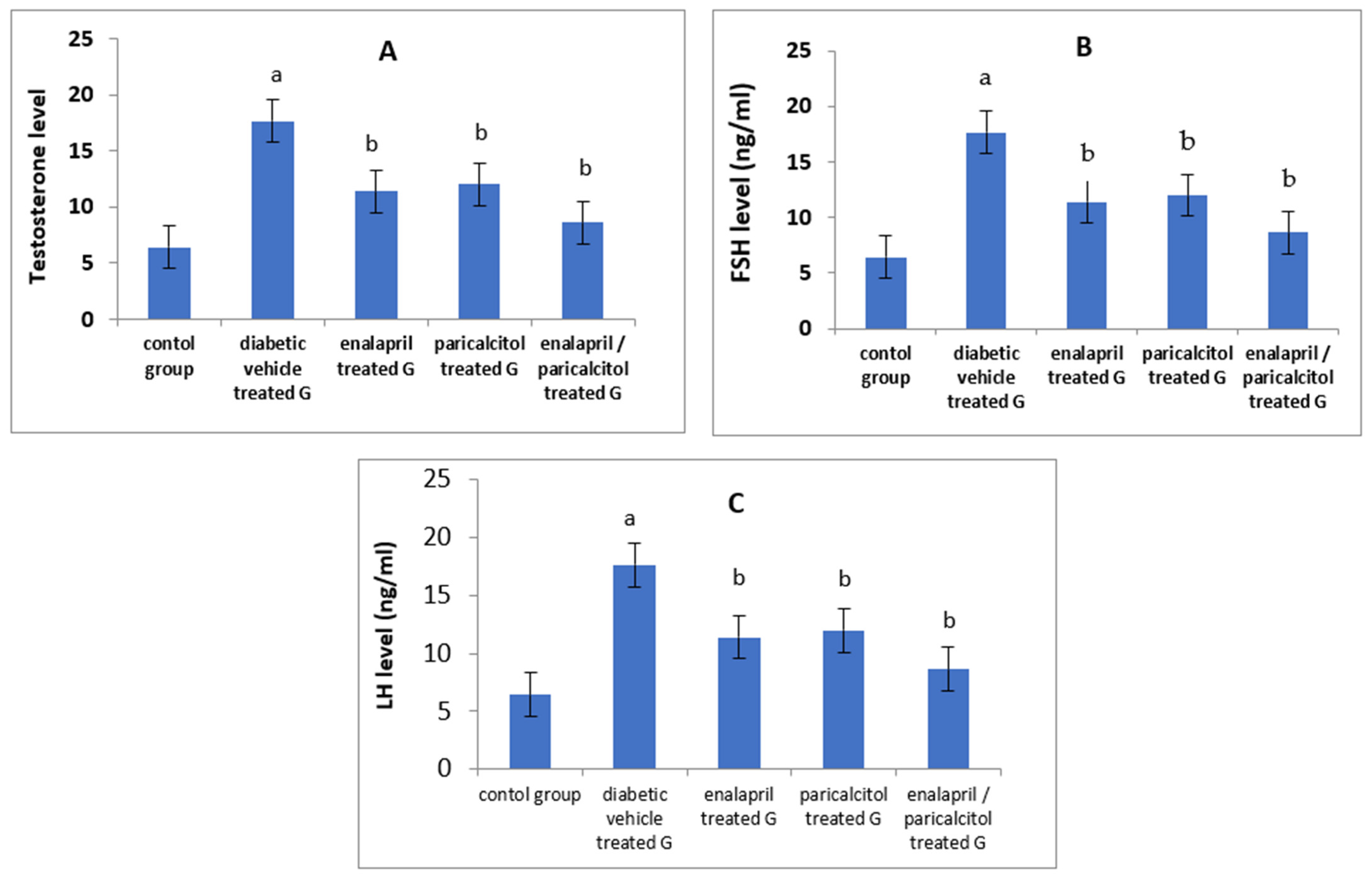
3.3. Impact of Different Treatments on Testosterone, FSH, and LH in Studied Groups
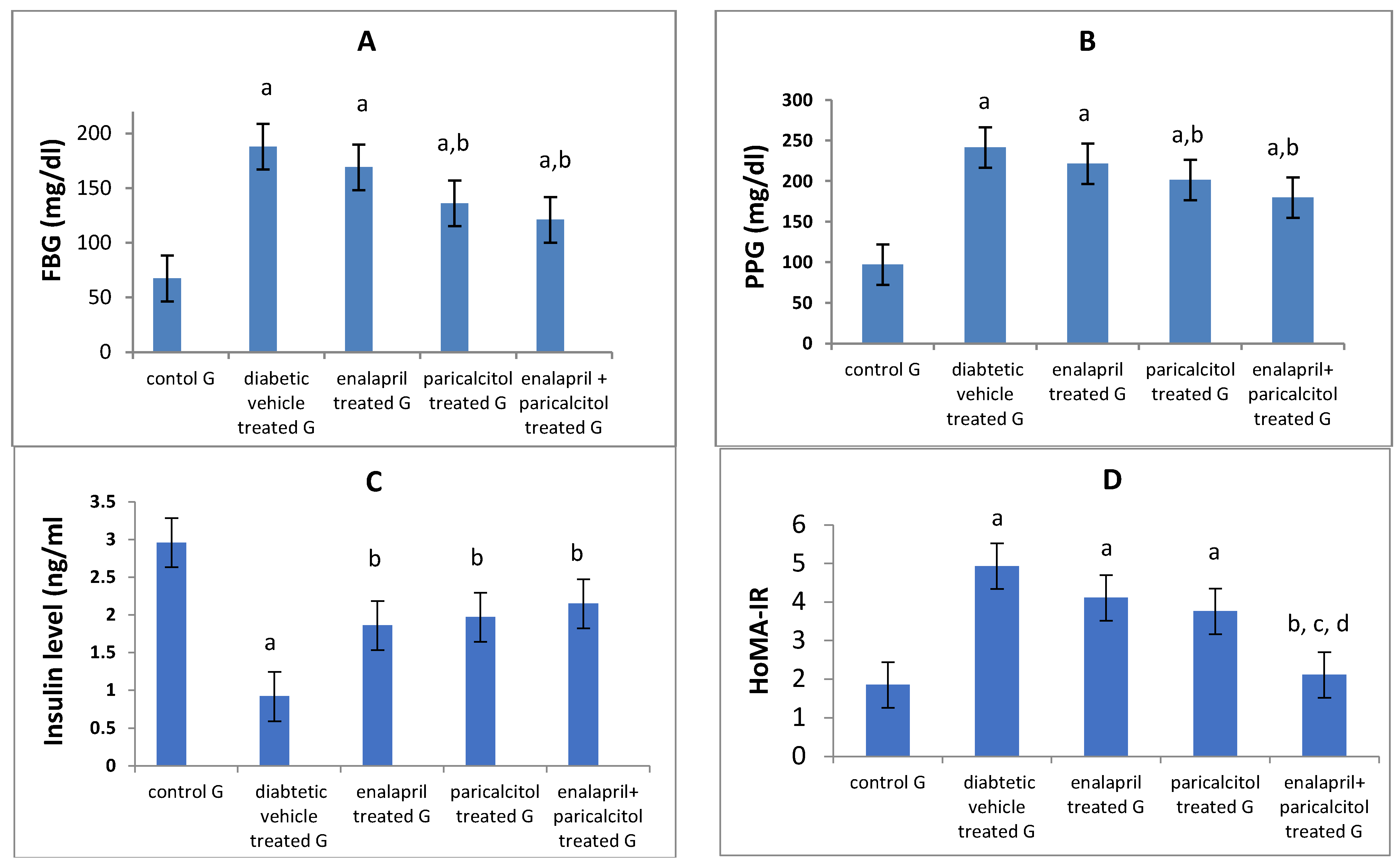
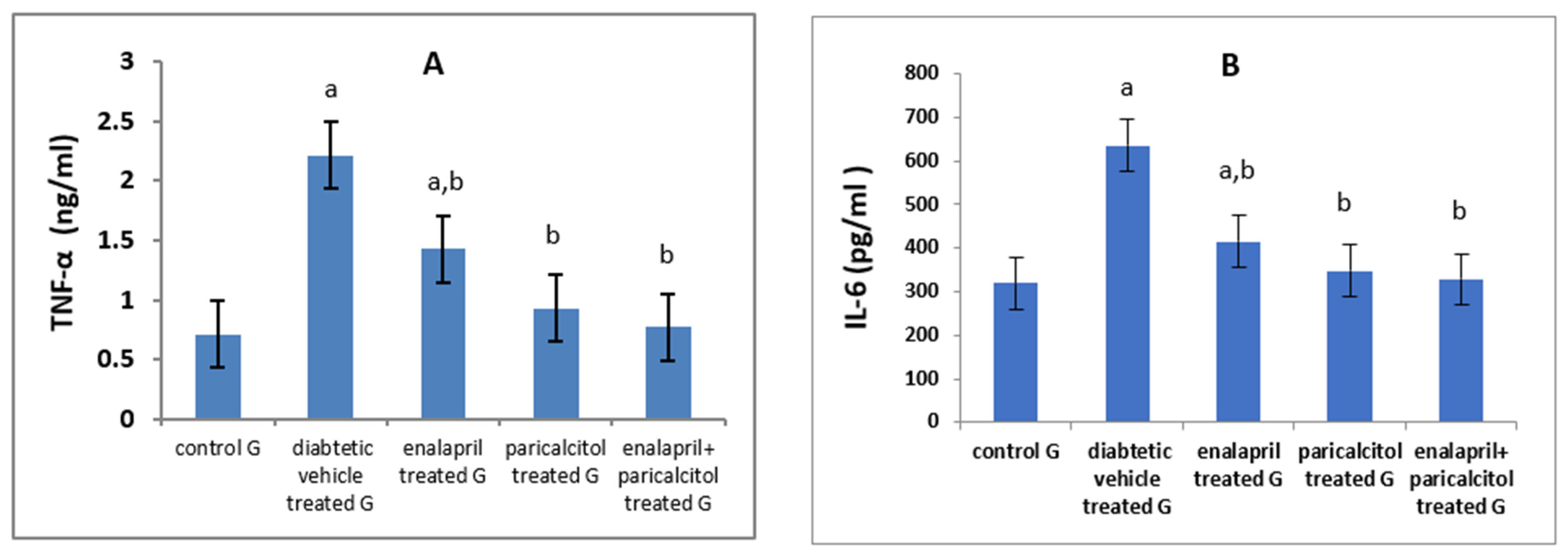
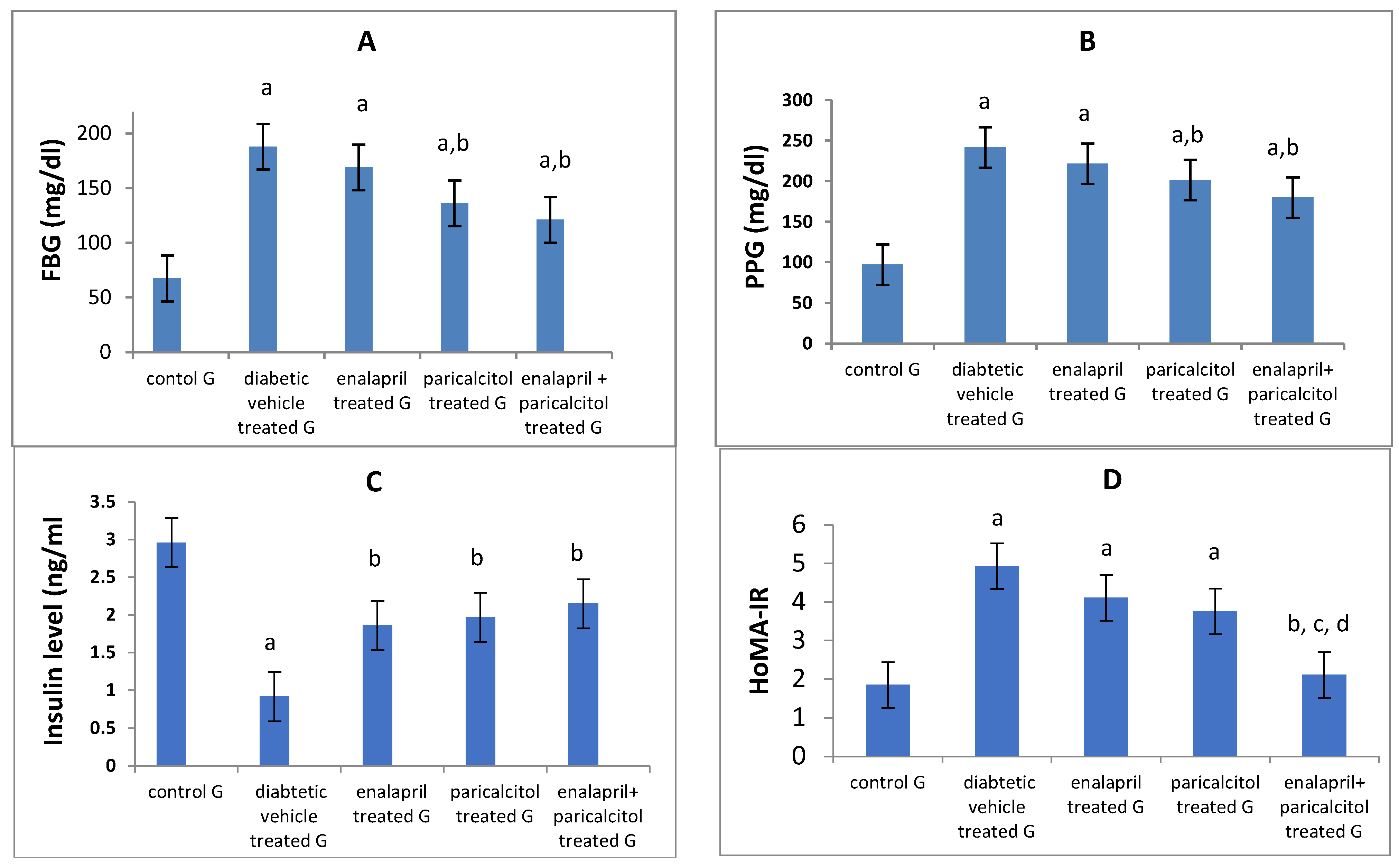
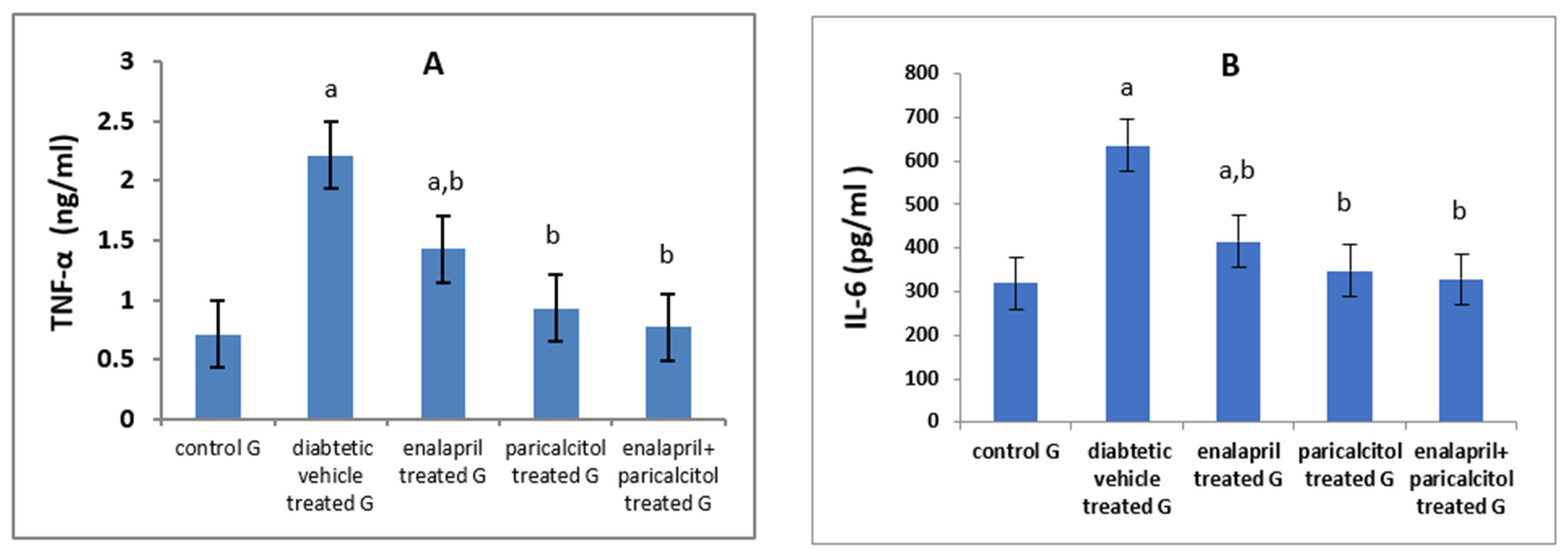
3.4. Effects of Different Treatments on Glycemic Status and Inflammatory Parameters
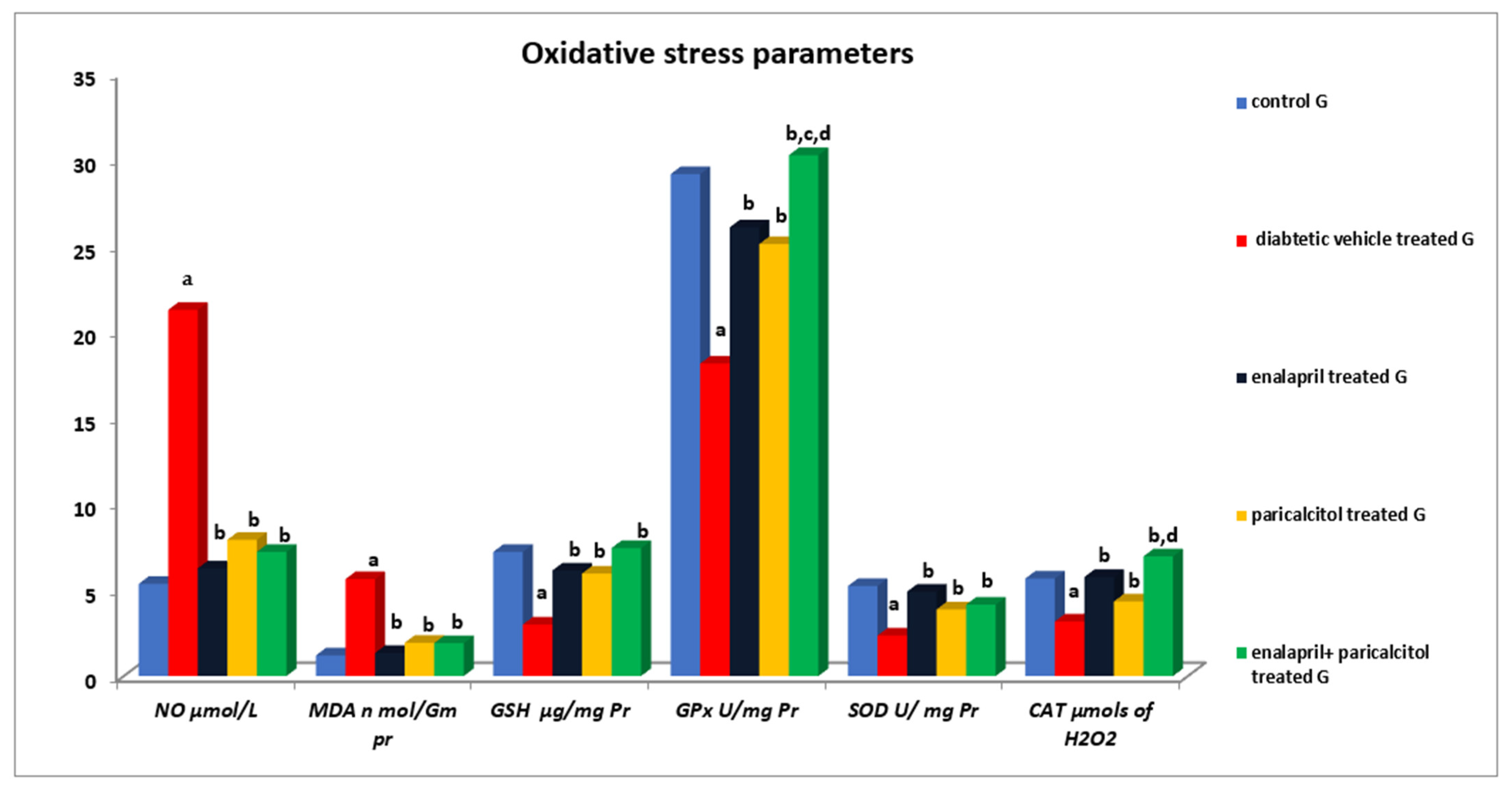
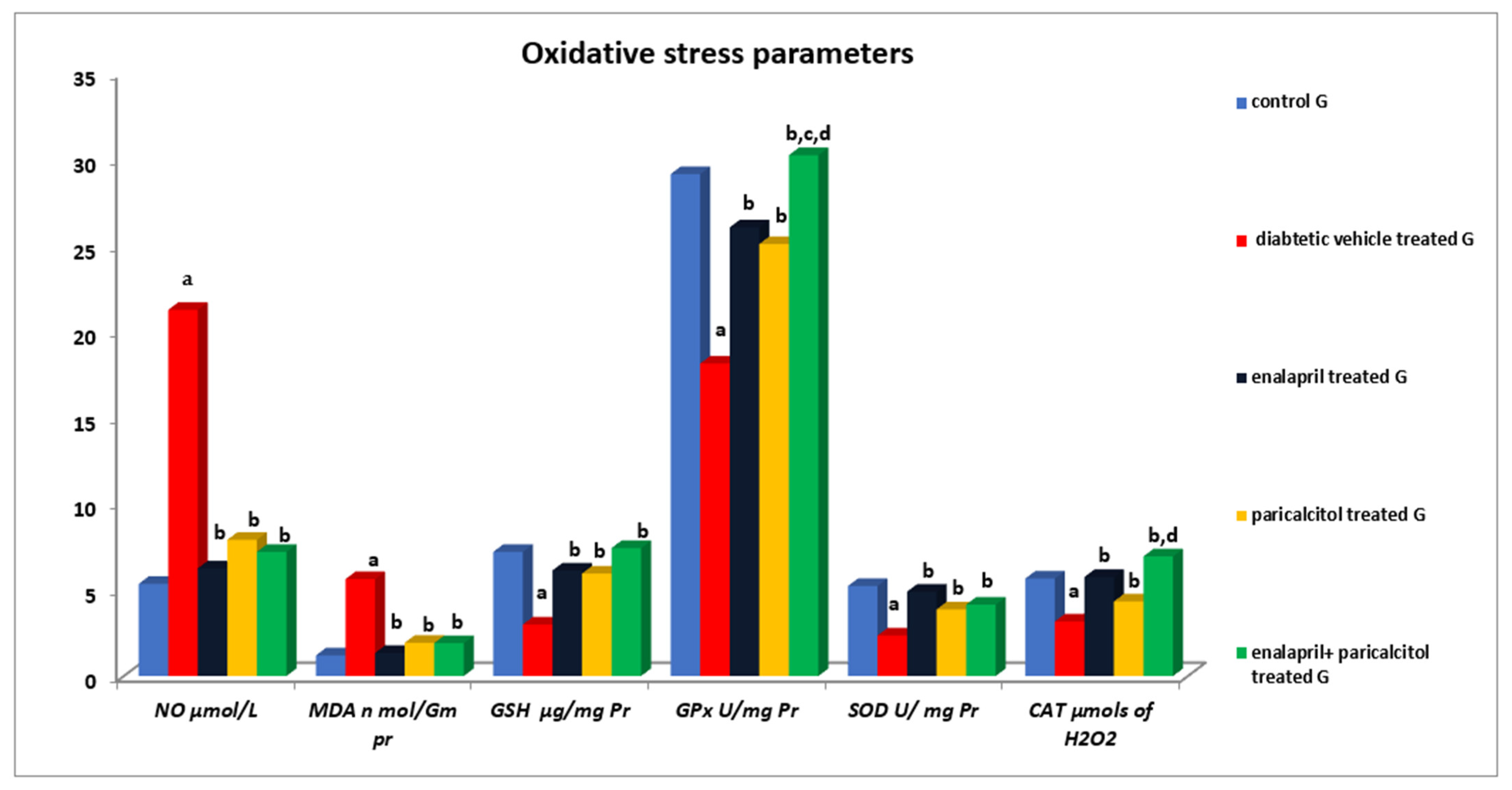
3.5. Impact of Different Treatments on Testicular Oxidative Stress Parameters
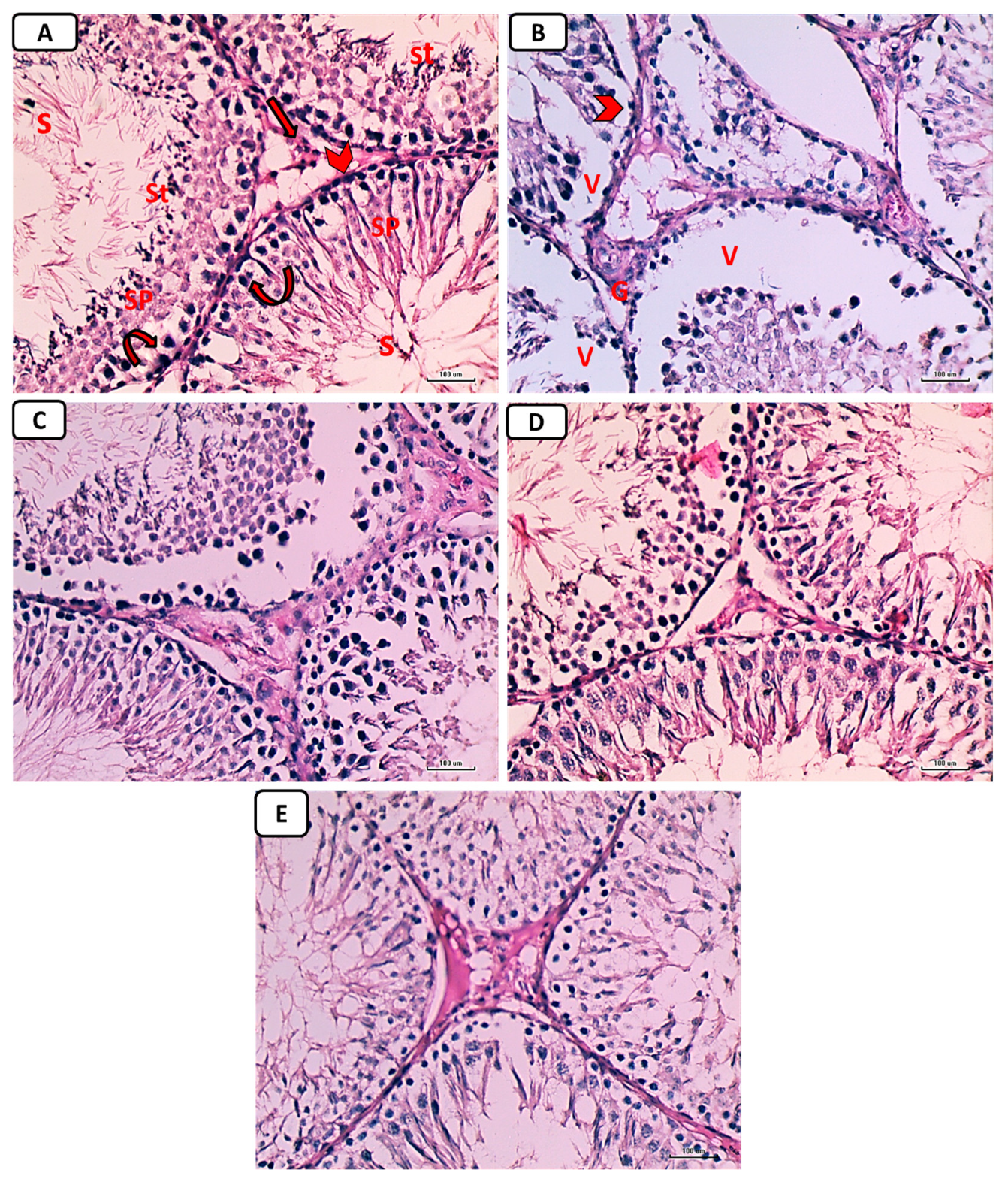
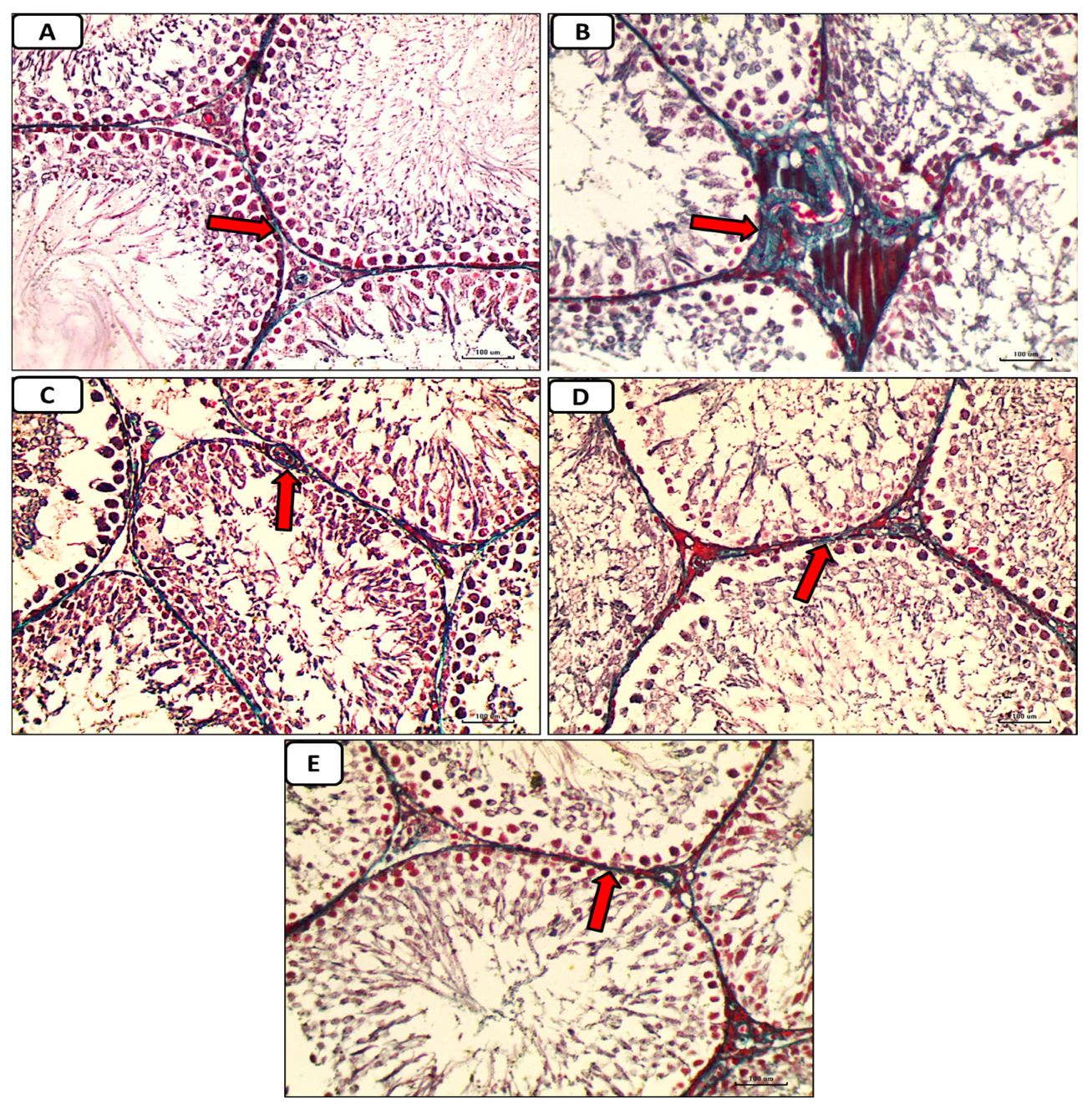
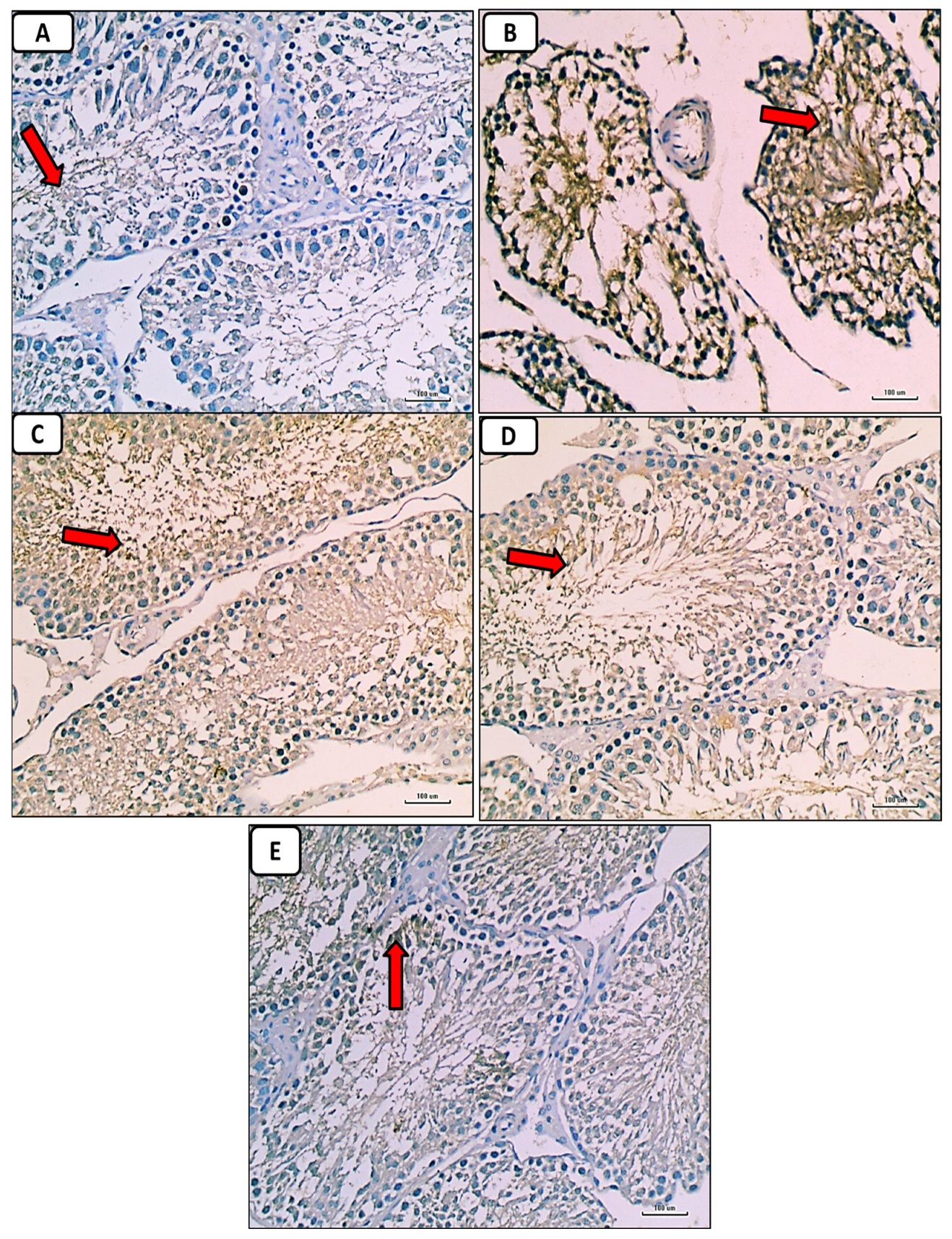
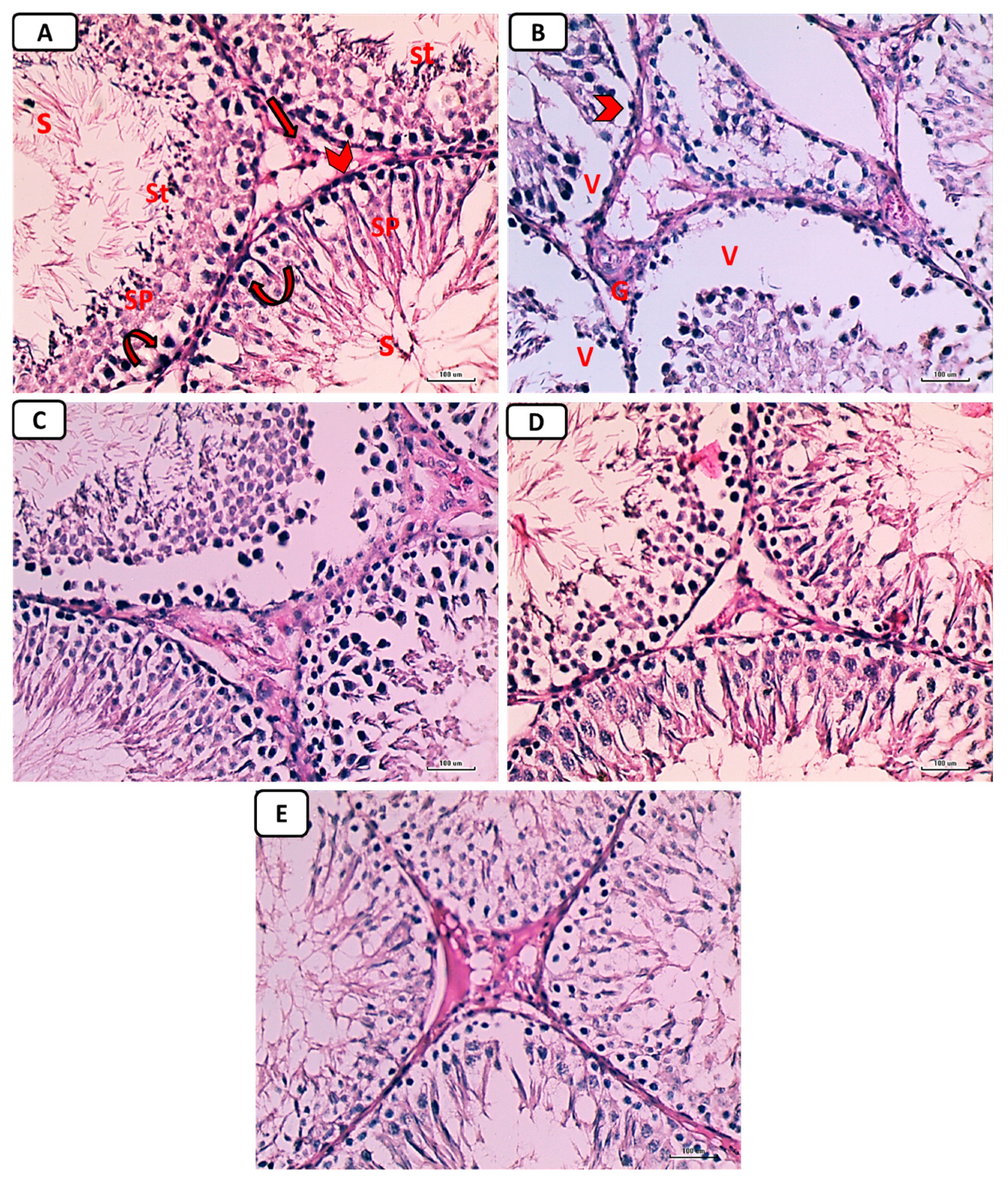
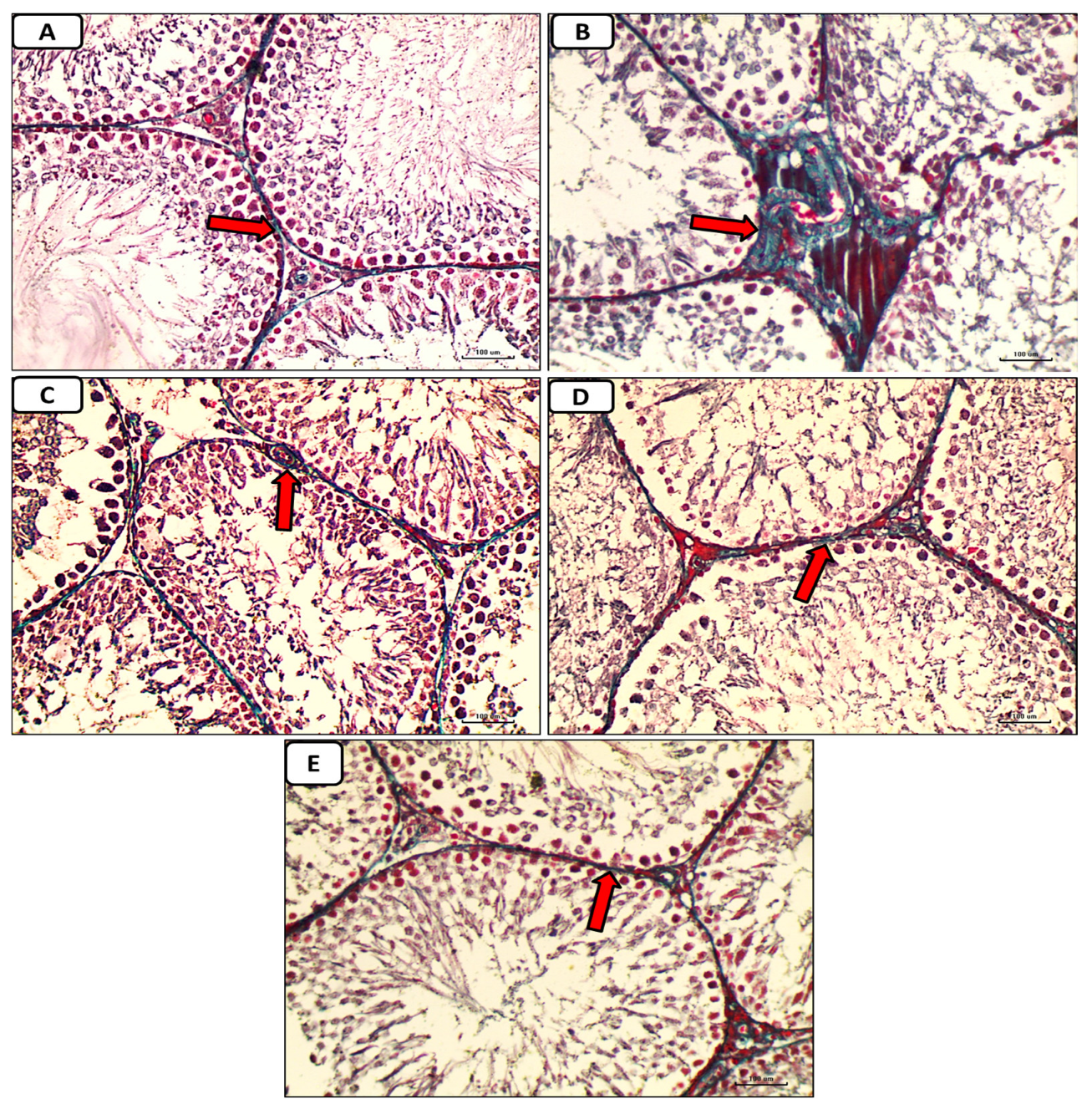
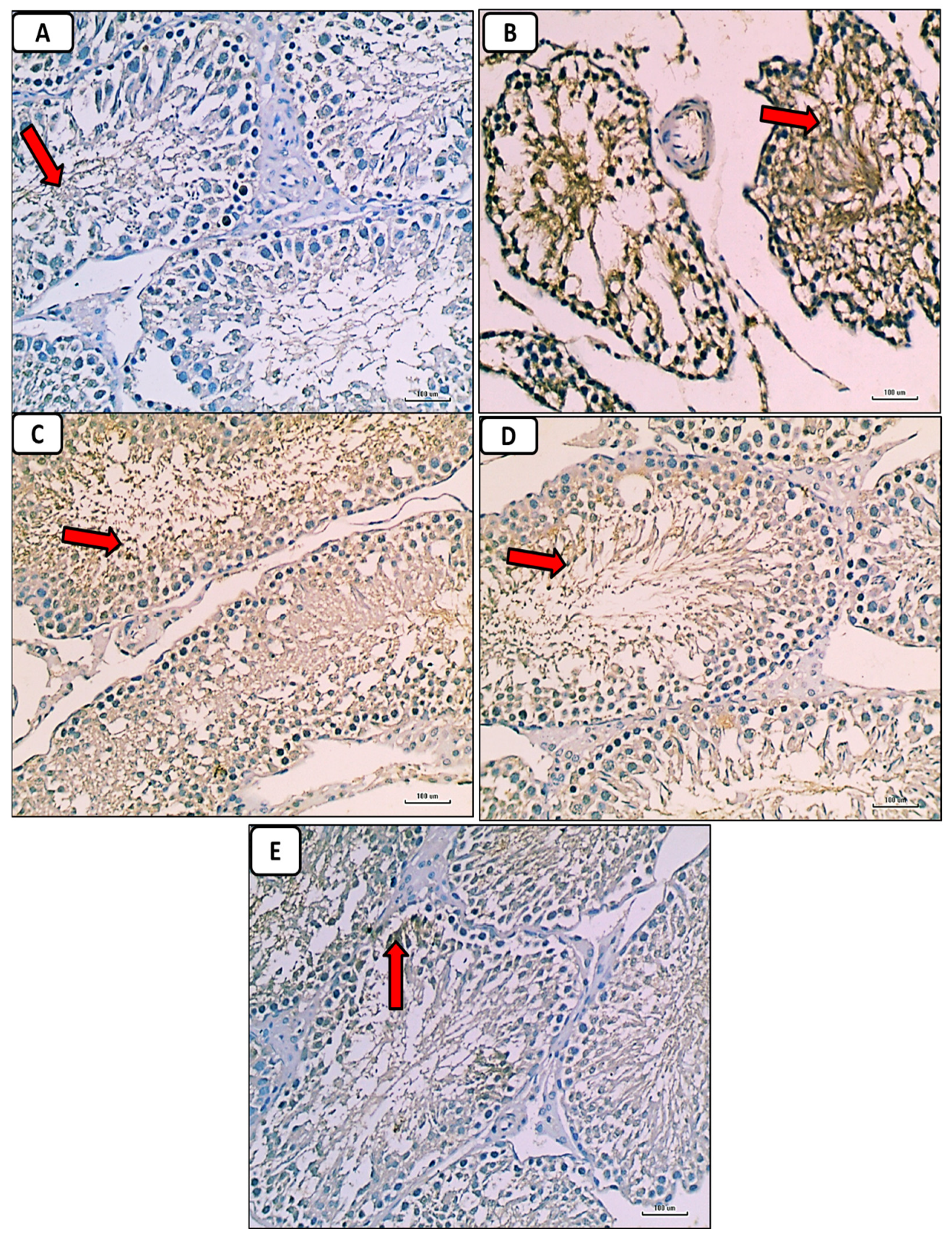
3.6. Histological and Immunohistochemical Results
Results for Hematoxylin-and-Eosin-Stained Sections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Aksu, I.; Baykara, B.; Kiray, M.; Gurpinar, T.; Sisman, A.R.; Ekerbicer, N.; Tas, A.; Gokdemir-Yazar, O.; Uysal, N. Serum IGF-1 levels correlate negatively to liver damage in diabetic rats. Biotech. Histochem. 2013, 88, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Amaral, S.; Moreno, A.J.; Santos, M.S.; Seiça, R.; Ramalho-Santos, J. Effects of hyperglycemia on sperm and testicular cells of Goto-Kakizaki and streptozotocin-treated rat models for diabetes. Theriogenology 2006, 66, 2056–2067. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, C.M.; Santos, D.L.; Seiça, R.; Moreno, A.J.; Santos, M.S. Enhanced mitochondrial testicular antioxidant capacity in Goto-Kakizaki diabetic rats: Role of coenzyme Q. Am. J. Physiol. Physiol. 2001, 281, C1023–C1028. [Google Scholar] [CrossRef] [PubMed]
- Shrilatha, B.; Muralidhara. Occurrence of oxidative impairments, response of antioxidant defences and associated biochemical perturbations in male reproductive milieu in the Streptozotocin-diabetic rat. Int. J. Androl. 2007, 30, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Maresch, C.C.; Stute, D.C.; Ludlow, H.; Hammes, H.-P.; de Kretser, D.M.; Hedger, M.P.; Linn, T. Hyperglycemia is associated with reduced testicular function and Activin dysregulation in the Ins2 Akita+/− mouse model of type 1 diabetes. Mol. Cell. Endocrinol. 2017, 446, 91–101. [Google Scholar] [CrossRef]
- Tiwari, A.K. Imbalance in antioxidant defense and human diseases: Multiple approach of natural antioxidants therapy. Curr. Sci. 2001, 81, 1179–1187. Available online: http://www.jstor.org/stable/24106434 (accessed on 10 November 2001).
- Ali, T.M.; Mehanna, O.M.; Elsaid, A.G.; Askary, A.E. Effect of Combination of Angiotensin-Converting Enzyme Inhibitors and Vitamin D Receptor Activators on Cardiac Oxidative Stress in Diabetic Rats. Am. J. Med. Sci. 2016, 352, 208–214. [Google Scholar] [CrossRef]
- Ahmed, O.M.; Ali, T.M.; Abdel Gaid, M.; Elberry, A.A. Effects of enalapril and paricalcitol treatment on diabetic nephropathy and renal expressions of TNF-α, p53, caspase-3 and Bcl-2 in STZ-induced diabetic rats. PLoS ONE 2019, 14, e0214349. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Kurz, S.; Münzel, T.; Tarpey, M.; Freeman, B.A.; Griendling, K.K.; Harrison, D.G. Angiotensin II-mediated hypertension in the rat increases vascular superoxide production via membrane NADH/NADPH oxidase activation. Contribution to alterations of vasomotor tone. J. Clin. Investig. 1996, 97, 1916–1923. [Google Scholar] [CrossRef]
- Bhuyan, B.J.; Mugesh, G. Synthesis, characterization and antioxidant activity of angiotensin converting enzyme inhibitors. Org. Biomol. Chem. 2010, 9, 1356–1365. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Hekmatdoost, A.; Nourian, M. Antioxidant efficacy of vitamin D. J. Parathyr. Dis. 2016, 5, 11–16. [Google Scholar]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef]
- Ravani, P.; Malberti, F.; Tripepi, G.; Pecchini, P.; Cutrupi, S.; Pizzini, P.; Mallamaci, F.; Zoccali, C. Vitamin D levels and patient outcome in chronic kidney disease. Kidney Int. 2009, 75, 88–95. [Google Scholar] [CrossRef]
- Mitri, J.; Muraru, M.D.; Pittas, A.G. Vitamin D and type 2 diabetes: A systematic review. Eur. J. Clin. Nutr. 2011, 65, 1005–1015. [Google Scholar] [CrossRef]
- Hyppönen, E.; Läärä, E.; Reunanen, A.; Järvelin, M.R.; Virtanen, S.M. Intake of vitamin D and risk of type 1 diabetes: A birthcohort study. Lancet 2001, 358, 1500–1503. [Google Scholar] [CrossRef]
- Yang, J.; Xu, J.; Zhang, H. Effect of Vitamin D on ACE2 and Vitamin D receptor expression in rats with LPS-induced acute lung injury. Chin. J. Emerg. Med. 2016, 12, 1284–1289. [Google Scholar]
- Long, L.; Qiu, H.; Cai, B.; Chen, N.; Lu, X.; Zheng, S.; Ye, X.; Li, Y. Hyperglycemia induced testicular damage in type 2 diabetes mellitus rats exhibiting microcirculation impairments associated with vascular endothelial growth factor decreased via PI3K/Akt pathway. Oncotarget 2018, 9, 5321–5336. [Google Scholar] [CrossRef]
- Shrilatha, B.; Muralidhara. Early oxidative stress in testis and epididymal sperm in streptozotocin-induced diabetic mice: Its progression and genotoxic consequences. Reprod. Toxicol. 2007, 23, 578–587. [Google Scholar] [CrossRef]
- Finch, J.L.; Suarez, E.B.; Husain, K.; Ferder, L.; Cardema, M.C.; Glenn, D.J.; Gardner, D.G.; Liapis, H.; Slatopolsky, E. Effect of combining an ACE inhibitor and a VDR activator on glomerulosclerosis, proteinuria, and renal oxidative stress in uremic rats. Am. J. Physiol. Renal Physiol. 2012, 302, F141–F149. [Google Scholar] [CrossRef]
- Tietz, N.W. Clinical Guide to Laboratory Tests, 3rd ed.; Pbl, W.B. Saunders Company: Philadelphia, PA, USA, 1995; pp. 509–580. [Google Scholar]
- Temple, R.C.; Clark, P.M.; Hales, C.N. Measurement of insulin secretion in type 2 diabetes: Problems and pitfalls. Diabet. Med. 1992, 9, 503–512. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Huang, H.F.S.; Linsenmeyer, T.A.; Li, M.T.; Giglio, W.; Anesetti, R.; VON Hagen, J.; Ottenweller, J.E.; Serenas, C.; Pogach, L. Acute Effects of Spinal Cord Injury on the Pituitary-Testicular Hormone Axis and Sertoli Cell Functions: A Time Course Study. J. Androl. 1995, 16, 148–157. [Google Scholar] [CrossRef]
- Ellman, M. A spectrophotometric method for determination of reduced glutathione in tissues. Anal. Biochem. 1959, 74, 214–226. [Google Scholar]
- Flohe, L.; Otting, F. Superoxide dismutase assays. Methods Enzym. 1984, 105, 93–104. [Google Scholar]
- Husain, K.; Suarez, E.; Isidro, A.; Ferder, L. Effects of paricalcitol and enalapril on atherosclerotic injury in mouse aortas. Am. J. Nephrol. 2010, 32, 296–304. [Google Scholar] [CrossRef]
- Aebi, H. Catalase in vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for lipid peroxides in animal tissues by thiobarbaturic acid reaction. Anal. Biochem. 1982, 95, 351–358. [Google Scholar] [CrossRef]
- Hortelano, S.; Dewez, B.; Genaro, A.M.; Díaz-Guerra, M.J.; Boscá, L. Nitric oxide is released in regenerating liver after partial hepatectomy. Hepatology 1995, 21, 776–786. [Google Scholar]
- Kushwaha, S.; Jena, G.B. Effects of nicotine on the testicular toxicity of streptozotocin-induced diabetic rat: Intervention of enalapril. Hum. Exp. Toxicol. 2014, 33, 609–622. [Google Scholar] [CrossRef]
- Khaki, A.; Khaki, A.A.; Hajhosseini, L.; Golzar, F.S.; Ainehchi, N. The anti-oxidant effects of ginger and cinnamon on spermatogenesis dys-function of diabetes rats. Afr. J. Tradit. Complement. Altern. Med. 2014, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shalizar, J.A.; Hasanzadeh, S.; Malekinejad, H. Chemoprotective effect of Crataegusmonogyna aqueous extract against cyclophosphamide-induced reproductive toxicity. Vet. Res. Forum 2011, 2, 266–273. [Google Scholar]
- Bancroft, J.D.; Layton, C. The Hematoxylin and Eosin. In Theory & Practice of Histological Technique, 7th ed.; SuVarna, S.K., Layton, C., Bancroft, J.D., Eds.; Churchill Livingstone of Elsevier: Philadelphia, PA, USA, 2013; pp. 172–214. [Google Scholar]
- Jackson, P.; Blythe, D. Immunohistochemical Techniques. In Theory & Practice of Histological Techniques, 7th ed.; SuVarna, S.K., Layton, C., Bancroft, J.D., Eds.; Churchill Livingstone of Elsevier: Philadelphia, PA, USA, 2013; pp. 381–434. [Google Scholar]
- Ricci, G.; Catizone, A.; Esposito, R.; Pisanti, F.A.; Vietri, M.T.; Galdieri, M. Diabetic rat testes: Morphological and functional alterations. Andrologia 2009, 41, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Take, G.; Ilgaz, C.; Erdogan, D.; Ozogul, C.; Elmas, C. A Comparative Study of the Ultrastructure of Submandibular, Parotid and Exocrine Pancreas in Diabetes and Fasting. Saudi Med. J. 2007, 28, 28–35. [Google Scholar] [PubMed]
- Long, L.; Wang, J.; Lu, X.; Xu, Y.; Zheng, S.; Luo, C.; Li, Y. Protective effects of scutellarin on type II diabetes mellitus-induced testicular damages related to reactive oxygen species/Bcl-2/Bax and reactive oxygen species/microcirculation/staving pathway in diabetic rat. J. Diabetes Res. 2015, 2015, 252530. [Google Scholar] [CrossRef] [PubMed]
- Schoeller, E.L.; Albanna, G.; Frolova, A.I.; Moley, K.H. Insulin rescues impaired spermatogenesis via the hypothalamic-pituitary-gonadal axis in Akita diabetic mice and restores male fertility. Diabetes 2011, 61, 1869–1878. [Google Scholar] [CrossRef] [PubMed]
- Ozdemır, O.; Akalın, P.P.; Baspınar, N.; Hatıpoglu, F. Pathological changes in the acute phase of streptozotocin-induced diabetic rats. Bull. Vet. Inst. Pulawy 2009, 53, 783–790. [Google Scholar]
- Husain, K.; Suarez, E.; Isidro, A.; Hernandez, W.; Ferder, L. Effect of paricalcitol and enalapril on renal inflammation/oxidative stress in atherosclerosis. World J. Biol. Chem. 2015, 6, 240–248. [Google Scholar] [CrossRef]
- Ali, T.M.; Esawy, B.H.; Elmorsy, E.A. Effect of combining an angiotensin-converting enzyme inhibitor and a vitamin D receptor activator on renal oxidative and nitrosative stress in diabetic rats. Natl. J. Physiol. Pharm. Pharmacol. 2015, 5, 222–231. [Google Scholar] [CrossRef]
- Husain, K.; Ferder, L.; Mizobuchi, M.; Finch, J.; Slatopolsky, E. Combination Therapy with Paricalcitol and Enalapril Ameliorates Cardiac Oxidative Injury in Uremic Rats. Am. J. Nephrol. 2008, 29, 465–472. [Google Scholar] [CrossRef]
- Ritter, C.; Zhang, S.; Finch, J.L.; Liapis, H.; Suarez, E.; Ferder, L.; Delmez, J.; Slatopolsky, E. Cardiac and Renal Effects of Atrasentan in Combination with Enalapril and Paricalcitol in Uremic Rats. Kidney Blood Press. Res. 2014, 39, 340–352. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.J.; Cavia, M.; Muñiz, P.; de Francisco, A.L.; Arias, M.; Santos, J.; Abaigar, P. Paricalcitol reduces oxidative stress and inflammation in hemodialysis patients. BMC Nephrol. 2012, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.F.; Milena, F.J.; Mora, C.; Leo, C.; Claverie, F.; Flores, C.; Garcia, J. Tumor necrosis factor-alpha gene expression in diabetic nephropathy: Relationship with urinary albumin excretion and effect of angiotensin-converting enzyme inhibition. Kidney Int. Suppl. 2005, 99, S98–S102. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.A.; Fearnley, G.W.; Harrison, M.A.; Tomlinson, D.C.; Wheatcroft, S.B.; Ponnambalam, S. Vascular endothelial growth factors: Multitasking functionality in metabolism, health and disease. J. Inherit. Metab. Dis. 2015, 38, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Pérez Díaz, J.; Benitez, A.; Fernández Galaz, C. Effect of streptozotocin diabetes on the pituitary-testicular axis in the rat. Horm. Metab. Res. 1982, 14, 479–482. [Google Scholar] [CrossRef]
- Salvi, R.; Castillo, E.; Voirol, M.J.; Glauser, M.; Rey, J.; Gaillard, R.C.; Vollenweider, P.; Pralong, F.P. Gonadotropin-Releasing Hormone-Expressing Neurons Immortalized Conditionally Are Activated by Insulin: Implication of the Mitogen-Activated Protein Kinase Pathway. Endocrinology 2006, 147, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Olivares, A.; Méndez, J.P.; Cárdenas, M.; Oviedo, N.; Palomino, M.Á.; Santos, I.; Ulloa-Aguirre, A. Pituitary-testicular axis function, biological to immunological ratio and charge isoform distribution of pituitary LH in male rats with experimental diabetes. Gen. Comp. Endocrinol. 2009, 161, 304–312. [Google Scholar] [CrossRef]
- Shoorei, H.; Khaki, A.; Khaki, A.A.; Hemmati, A.A.; Moghimian, M.; Shokoohi, M. The ameliorative effect of carvacrol on oxidative stress and germ cell apoptosis in testicular tissue of adult diabetic rats. Biomed. Pharmacother. 2018, 111, 568–578. [Google Scholar] [CrossRef]
- Soltani, M.; Moghimian, M.; Abtahi-Eivari, S.H.; Shoorei, H.; Khaki, A.; Shokoohi, M. Protective Effects of Matricaria chamomilla Extract on Torsion/Detorsion-Induced Tissue Damage and Oxidative Stress in Adult Rat Testis. Int. J. Fertil. Steril. 2018, 12, 242–248. [Google Scholar] [CrossRef]
- Nna, V.U.; Bakar, A.B.A.; Ahmad, A.; Mohamed, M. Down-regulation of steroidogenesis-related genes and its accompanying fertility decline in streptozotocin-induced diabetic male rats: Ameliorative effect of metformin. Andrology 2018, 7, 110–123. [Google Scholar] [CrossRef]
- Alahmar, A.T. Role of Oxidative Stress in Male Infertility: An Updated Review. J. Hum. Reprod. Sci. 2019, 12, 4–18. [Google Scholar] [CrossRef]
- Laleethambika, N.; Anila, V.; Manojkumar, C.; Muruganandam, I.; Giridharan, B.; Ravimanickam, T.; Balachandar, V. Diabetes and Sperm DNA Damage: Efficacy of Antioxidants. SN Compr. Clin. Med. 2019, 1, 49–59. [Google Scholar] [CrossRef]
- Alasmari, W.A.; Faruk, E.M.; Abourehab, M.A.S.; Elshazly, A.M.E.; El Sawy, N.A. The Effect of Metformin versus Vitamin E on the Testis of Adult Diabetic Albino Rats: Histological, Biochemical and Immunohistochemistry Study. Adv. Reprod. Sci. 2018, 6, 113–132. [Google Scholar] [CrossRef]
- Samir, S.M.; Elalfy, M.; Nashar, E.M.E.; Alghamdi, M.A.; Hamza, E.; Serria, M.S.; Elhadidy, M.G. Cardamonin exerts a protective effect against autophagy and apoptosis in the testicles of diabetic male rats through the expression of Nrf2 via p62-mediated Keap-1 degradation. Korean J. Physiol. Pharmacol. 2021, 25, 341–354. [Google Scholar] [CrossRef]
- Liu, Y.; He, Y.; Wang, Q.; Guo, F.; Huang, F.; Ji, L.; An, T.; Qin, G. Vitamin D3 supplementation improves testicular function in diabetic rats through peroxisome proliferator-activated receptor-γ/transforming growth factor-beta 1/nuclear factor-kappa B. J. Diabetes Investig. 2018, 10, 261–271. [Google Scholar] [CrossRef]
- Ding, C.; Wang, Q.; Hao, Y.; Ma, X.; Wu, L.; Du, M.; Li, W.; Wu, Y.; Guo, F.; Ma, S.; et al. Vitamin D supplement improved testicular function in diabetic rats. Biochem. Biophys. Res. Commun. 2016, 473, 161–167. [Google Scholar] [CrossRef]
- Borg, H.M.; Kabel, A.; Estfanous, R.; Elmaaboud, M.A. Effect of the combination between empagliflozin and calcipotriol on cadmium-induced testicular toxicity in rats. Bull. Egypt. Soc. Physiol. Sci. 2020, 40, 15–31. [Google Scholar] [CrossRef]
- Sood, S.; Reghunandanan, R.; Reghunandanan, V.; Marya, R.; Singh, P. Effect of Vitamin D Repletion on Testicular Function in Vitamin D-Def icient Rats. Ann. Nutr. Metab. 1995, 39, 95–98. [Google Scholar] [CrossRef]
- Abozaid, E.R.; Hany, A. Vitamin D3 nanoemulsion ameliorates testicular dysfunction in high-fat diet-induced obese rat model. Med. J. Cairo Univ. 2020, 88, 775–785. [Google Scholar] [CrossRef]
- Kushwaha, S.; Jena, G.B. Enalapril reduces germ cell toxicity in streptozotocin-induced diabetic rat: Investigation on possible mechanisms. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2011, 385, 111–124. [Google Scholar] [CrossRef]
- Bechara, G.R.; de Souza, D.B.; Simoes, M.; Felix-Patrício, B.; Medeiros, J.L.; Costa, W.S.; Sampaio, F.J. Testicular Morphology and Spermatozoid Parameters in Spontaneously Hypertensive Rats Treated with Enalapril. J. Urol. 2015, 194, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Gokce, G.; Karboga, H.; Yildiz, E.; Ayan, S.; Gultekin, Y. Effect of angiotensin-converting enzyme inhibition and angiotensin II type 1 receptor blockade on apoptotic changes in contralateral testis following unilateral testicular torsion. Int. Urol. Nephrol. 2008, 40, 989–995. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups Parameters | Non-Diabetic Controls | Diabetic Groups | p-Value | |||
|---|---|---|---|---|---|---|
| Vehicle-Treated | Enalapril-Treated | Paricalcitol-Treated | Enalapril + Paricalcitol-Treated | |||
| Body weight (gm) | 230.2 ± 17.4 | 120.5 ± 15.4 a | 170.3 ± 12.2 b | 173.4 ± 14.4 b | 205.7 ± 14.3 b | <0.05 |
| Testicular weight (gm) | 1.54 ± 0.02 | 0.78 ± 0.04 a | 1.15 ± 0.01 b | 1.12 ± 0.05 b | 1.43 ± 0.04 b | <0.05 |
| Sperm count (mill/mL) | 52.23 ± 6.5 | 25.2 ± 5.85 a | 35.33 ± 3.21 b | 36.11 ± 4.96 b | 45.75 ± 5.22 b | <0.05 |
| Sperm motility (%) | 65.3 ± 5.32 | 35.4 ± 4.76 a | 47.45 ± 5.11 b | 48.32 ± 4.89 b | 58.45 ± 6.39 b | <0.05 |
| Abnormal sperms (%) | 6.43 ± 0.97 | 17.6 ± 1.85 a | 11.42 ± 0.89 b | 12.01 ± 0.76 b | 8.65 ± 0.56 b | <0.05 |
| Groups Parameters | Non-Diabetic Controls | Diabetic Groups | p-Value | |||
|---|---|---|---|---|---|---|
| Vehicle-Treated | Enalapril-Treated | Paricalcitol-Treated | Enalapril + Paricalcitol-Treated | |||
| Testosterone (ng/mL) | 4.71 ± 0.24 | 1.9 4 ± 0.13 a | 3.55 ± 0.34 b | 3.71 ± 0.11 b | 4.4 ± 0.23 b | <0.05 |
| FSH (ng/mL) | 5.61 ± 0.98 | 2.75 ± 0.37 a | 3.97 ± 0.57 b | 4. 02 ± 0.45 b | 4.99 ± 0.31 b | <0.05 |
| LH (ng/mL) | 4.32 ± 0.45 | 1.97 ± 0.36 a | 3.41 ± 0.54 b | 3.56 ± 0.34 b | 4.1 ± 0.65 b | <0.05 |
| Groups Parameters | Non-Diabetic Controls | Diabetic Groups | p-Value | |||
|---|---|---|---|---|---|---|
| Vehicle-Treated | Enalapril-Treated | Paricalcitol-Treated | Enalapril + Paricalcitol- Treated | |||
| FBG (mg/dL) | 67.5 ± 11.3 | 188.02 ± 9.3 a | 169.22 ± 4.71 a | 136.19 ± 5.37 a,b | 121.15 ± 3.54 a,b | p < 0.01 |
| PPG (mg/dL) | 97.11 ± 14.3 | 241.26 ± 7.6 a | 221.32 ± 4.51 a | 201.31 ± 0.65 a,b | 179.69 ± 4.14 a,b,c | p < 0.01 |
| Insulin (ng/mL) | 2.96 ± 0.25 | 0.92 ± 0.58 a | 1.86 ± 2.42 b | 1.97 ± 3.04 b | 2.148 ± 3.34 b | p < 0.05 |
| HOMA-IR | 1.85 ± 0.16 | 4.93 ± 1.58 a | 4.11 ± 1.45 a | 3.76 ± 4.33 a | 2.11 ± 1.51 b,c,d | p < 0.05 |
| IL-6 (pg/mL) | 319.1 ± 9.07 | 634.7 ± 24.5 a | 414.9 ± 10.9 a,b | 347.35 ± 31.2 b | 328.5 ± 13.8 b | p < 0.01 |
| TNF-α (ng/mL) | 0.71 ± 0.16 | 2.21 ± 0.03 a | 1.43 ± 0.19 a,b | 0.93 ± 0.19 b | 0.77 ± 0. 9 b | p < 0.01 |
| Groups Parameters | Non-Diabetic Controls | Diabetic Groups | p-Value | |||
|---|---|---|---|---|---|---|
| Vehicle-Treated | Enalapril-Treated | Paricalcitol-Treated | Enalapril + Paricalcitol-Treated | |||
| NO (μmols/L) | 5.33 ± 1.13 | 21.24 ± 4.6 a | 6.23 ± 1.11 b | 7.89 ± 2.32 b | 7.19 ± 1.44 b | p < 0.001 |
| MDA (nmol/mg pr) | 1.18 ± 0.13 | 5.61 ± 0.34 a | 1.32 ± 0.41 b | 1.91 ± 0.15 b | 1.89 ± 0.11 b | p < 0.001 |
| GSH (μg/mg pr) | 7.19 ± 1.05 | 2.97 ± 0.88 a | 6.11 ± 0.72 b | 5.93 ± 1.08 b | 7.41 ± 1.54 b | p < 0.01 |
| GPx (U/mg pr) | 29.12 ± 2.82 | 18.12 ± 2.02 a | 26.03 ± 3.08 b | 25.06 ± 2.03 b | 30.22 ± 2.08 b,c,d | p < 0.01 |
| SOD (units/mg pr) | 5.21 ± 0.43 | 2.33 ± 1.55 a | 4.88 ± 1.39 b | 3.85 ± 1.13 b | 4.13 ± 1.48 b | p < 0.01 |
| CAT (μmols of H2O2) | 5.64 ± 1.56 | 3.15 ± 0.96 a | 5.73 ± 1.07 b | 4.31 ± 1.16 b | 6.93 ± 1.35 b,d | p < 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsaeed, M.Y.; Mehanna, O.M.; Abd-Allah, E.-E.E.; Hassan, M.G.; Ahmed, W.M.S.; Moustafa, A.E.G.A.; Eldesoky, G.E.; Hammad, A.M.; Elgazzar, U.B.; Elnady, M.R.; et al. Combination Therapy with Enalapril and Paricalcitol Ameliorates Streptozotocin Diabetes-Induced Testicular Dysfunction in Rats via Mitigation of Inflammation, Apoptosis, and Oxidative Stress. Pathophysiology 2023, 30, 567-585. https://doi.org/10.3390/pathophysiology30040041
Elsaeed MY, Mehanna OM, Abd-Allah E-EE, Hassan MG, Ahmed WMS, Moustafa AEGA, Eldesoky GE, Hammad AM, Elgazzar UB, Elnady MR, et al. Combination Therapy with Enalapril and Paricalcitol Ameliorates Streptozotocin Diabetes-Induced Testicular Dysfunction in Rats via Mitigation of Inflammation, Apoptosis, and Oxidative Stress. Pathophysiology. 2023; 30(4):567-585. https://doi.org/10.3390/pathophysiology30040041
Chicago/Turabian StyleElsaeed, Magdy Y., Osama Mahmoud Mehanna, Ezz-Eldin E. Abd-Allah, Mohamed Gaber Hassan, Walid Mostafa Said Ahmed, Abd El Ghany A. Moustafa, Gaber E. Eldesoky, Amal M. Hammad, Usama Bahgat Elgazzar, Mohamed R. Elnady, and et al. 2023. "Combination Therapy with Enalapril and Paricalcitol Ameliorates Streptozotocin Diabetes-Induced Testicular Dysfunction in Rats via Mitigation of Inflammation, Apoptosis, and Oxidative Stress" Pathophysiology 30, no. 4: 567-585. https://doi.org/10.3390/pathophysiology30040041
APA StyleElsaeed, M. Y., Mehanna, O. M., Abd-Allah, E.-E. E., Hassan, M. G., Ahmed, W. M. S., Moustafa, A. E. G. A., Eldesoky, G. E., Hammad, A. M., Elgazzar, U. B., Elnady, M. R., Abd-Allah, F. M., Shipl, W. M., Younes, A. M., Magar, M. R., Amer, A. E., Abbas, M. A. M., Elhamaky, K. S. A., & Hassan, M. H. M. (2023). Combination Therapy with Enalapril and Paricalcitol Ameliorates Streptozotocin Diabetes-Induced Testicular Dysfunction in Rats via Mitigation of Inflammation, Apoptosis, and Oxidative Stress. Pathophysiology, 30(4), 567-585. https://doi.org/10.3390/pathophysiology30040041