
Ferritin, Serum Iron and Hemoglobin as Acute Phase Reactants in Laparoscopic and Open Surgery of Cholecystectomy: An Observational Prospective Study
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
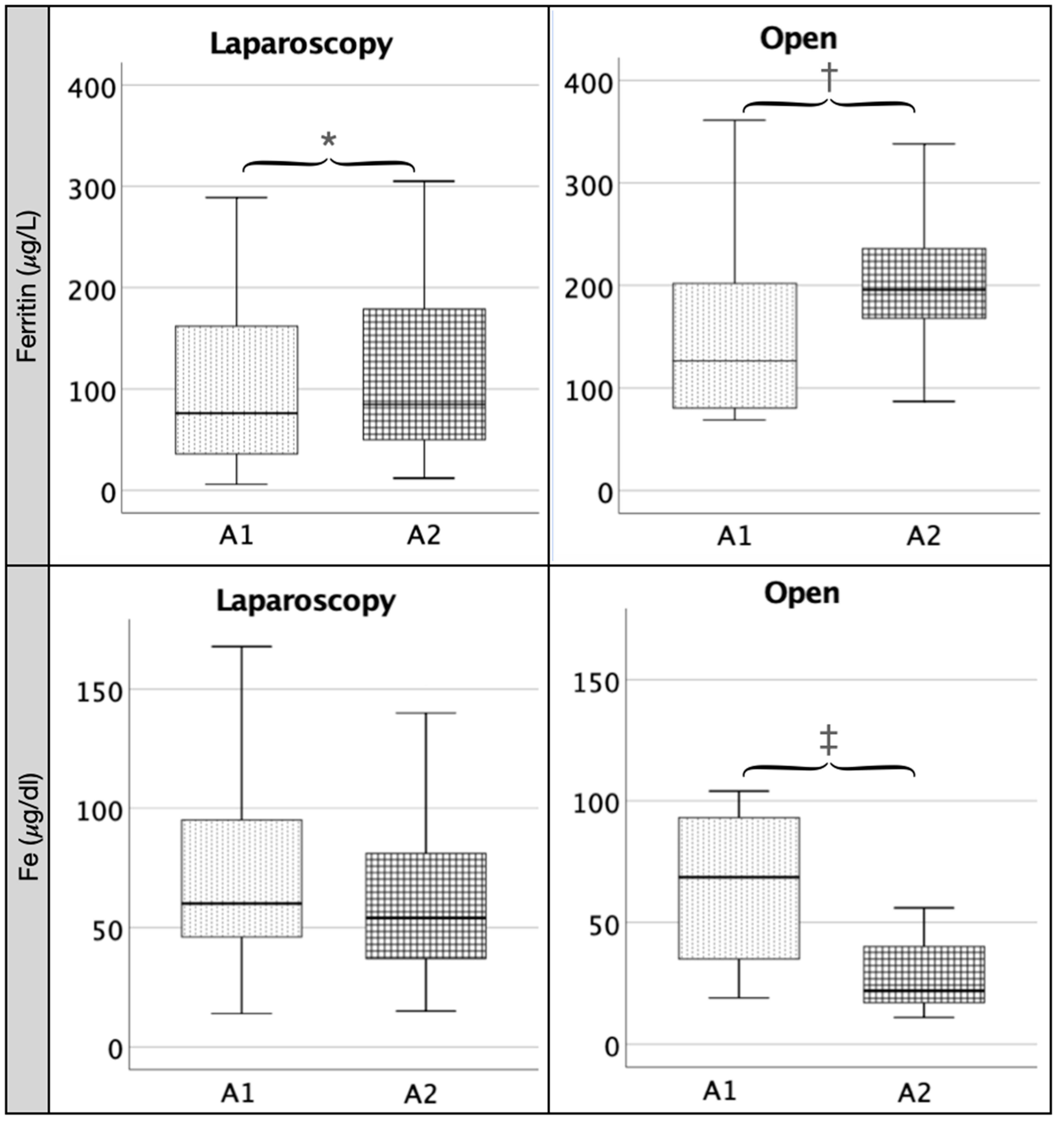
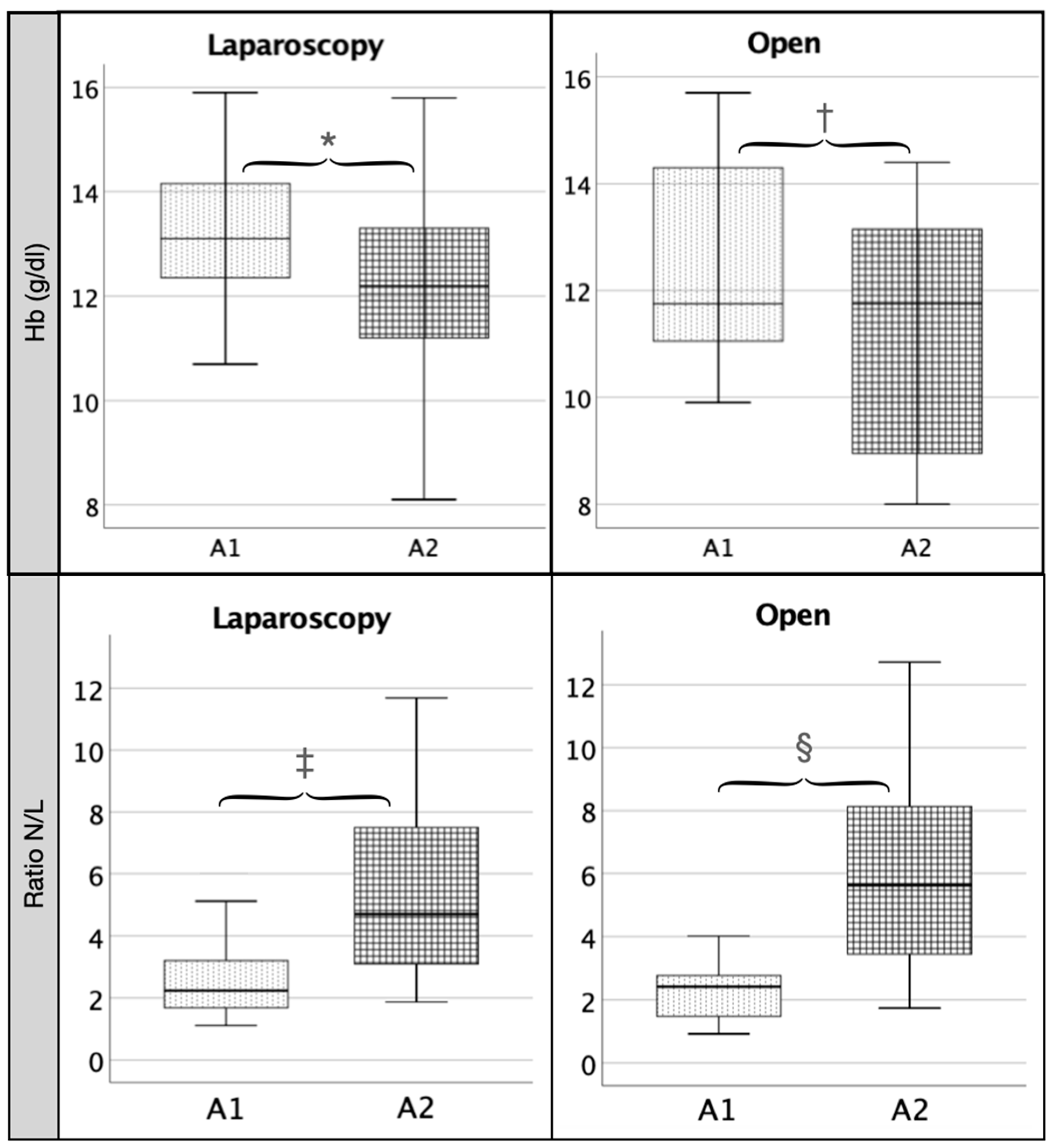
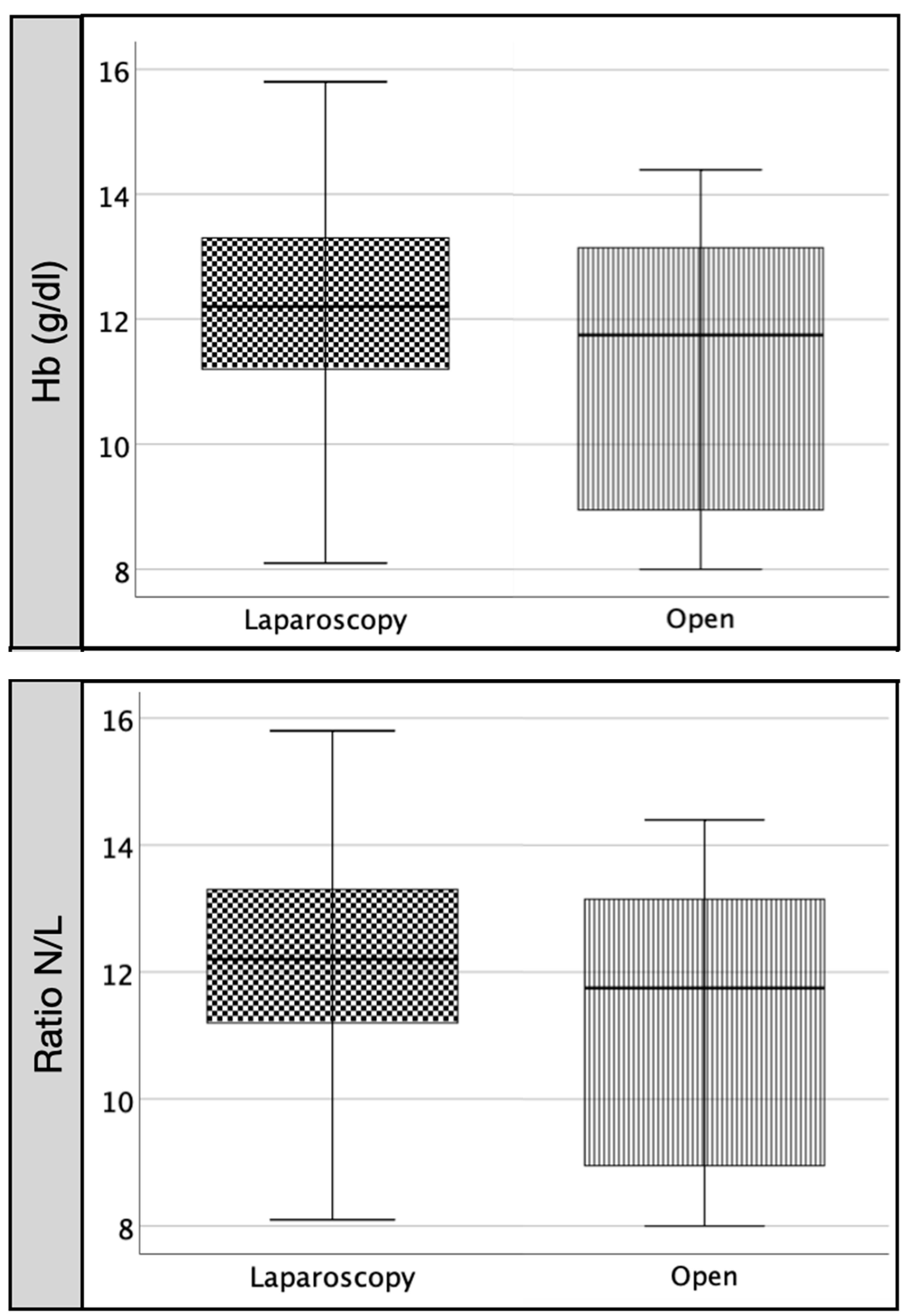
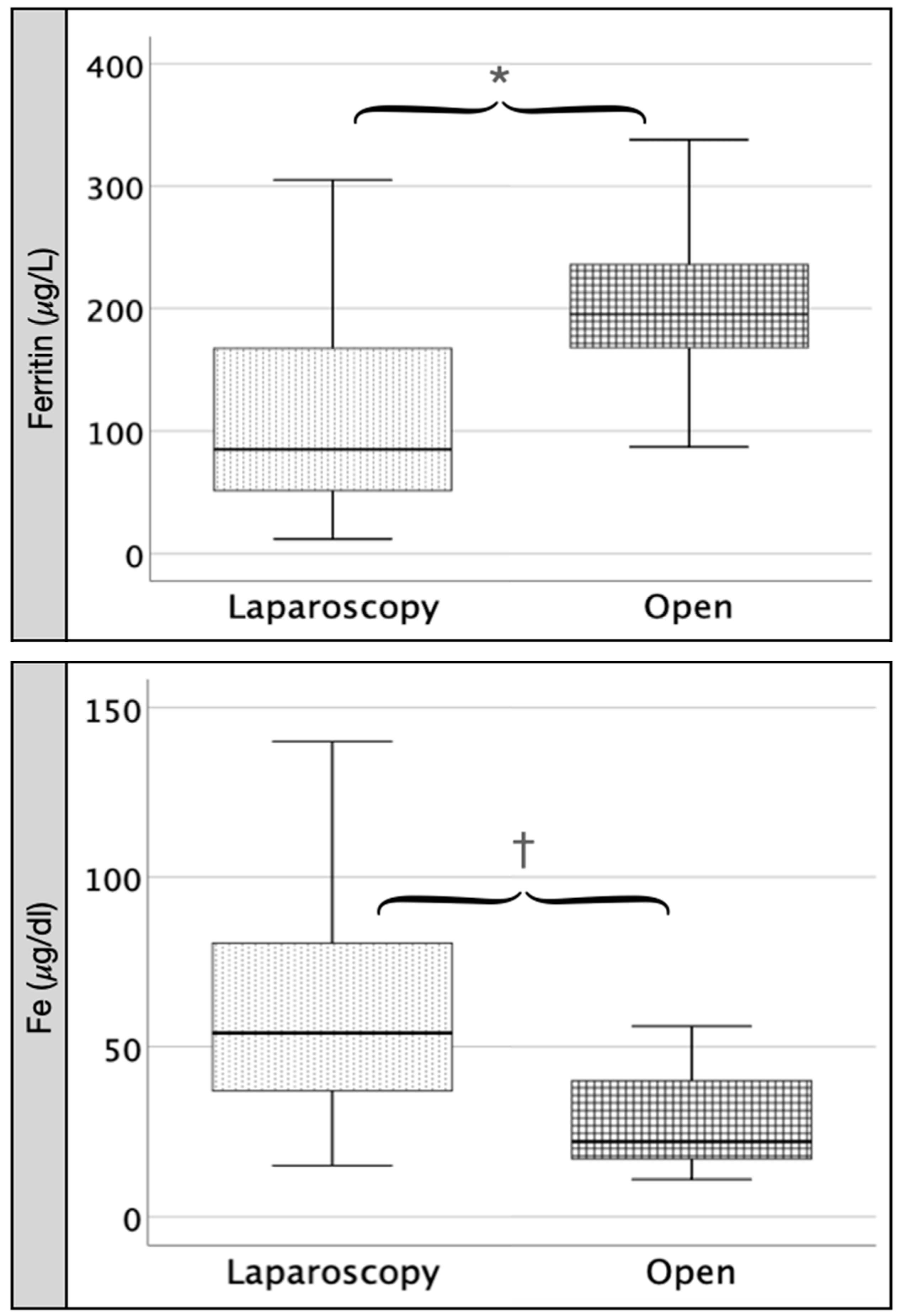
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Migita, K.; Matsumoto, S.; Wakatsuki, K.; Kunishige, T.; Nakade, H.; Miyao, S.; Sho, M. Postoperative Serum C-Reactive Protein Level Predicts Long-term Outcomes in Stage I Gastric Cancer. J. Surg. Res. 2019, 242, 323–331. [Google Scholar] [CrossRef]
- Nurmi, A.M.; Mustonen, H.K.; Stenman, U.-H.; Seppänen, H.E.; Haglund, C.H. Combining CRP and CA19-9 in a novel prognostic score in pancreatic ductal adenocarcinoma. Sci. Rep. 2021, 11, 781. [Google Scholar] [CrossRef]
- Krog, A.H.; Sahba, M.; Pettersen, E.M.; Sandven, I.; Thorsby, P.M.; Jørgensen, J.J.; Sundhagen, J.O.; Kazmi, S.S. Comparison of the acute-phase response after laparoscopic versus open aortobifemoral bypass surgery: A substudy of a randomized controlled trial. Vasc. Health Risk Manag. 2016, 12, 371–378. [Google Scholar] [CrossRef][Green Version]
- Tsamis, D.; Theodoropoulos, G.; Stamopoulos, P.; Siakavellas, S.; Delistathi, T.; Michalopoulos, N.V.; Zografos, G.C. Systemic inflammatory response after laparoscopic and conventional colectomy for cancer: A matched case–control study. Surg. Endosc. 2011, 26, 1436–1443. [Google Scholar] [CrossRef]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl. Lek. Listy 2001, 102, 5–14. [Google Scholar]
- Gao, G.; Li, J.; Zhang, Y.; Chang, Y.-Z. Cellular Iron Metabolism and Regulation. Adv. Exp. Med. Biol. 2019, 1173, 21–32. [Google Scholar] [CrossRef]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef]
- Martín-González, C.; Martín-Ponce, E.; Fernández-Rodríguez, C.; Sánchez-Pérez, M.J.; Rodríguez-Gaspar, M.; De-La-Vega-Prieto, M.J.; Martínez-Riera, A.; González-Reimers, E. Transforming Growth Factor Beta 1 and Vascular Risk in Alcoholics. Alcohol Alcohol. 2019, 54, 472–476. [Google Scholar] [CrossRef]
- Frazee, R.C.; Roberts, J.W.; Okeson, G.C.; Symmonds, R.E.; Snyder, S.K.; Hendricks, J.C.; Smith, R.W. Open versus laparoscopic cholecystectomy. A comparison of post-operative pulmonary function. Ann. Surg. 1991, 213, 651–654. [Google Scholar] [CrossRef]
- Visser, B.C.; Parks, R.W.; Garden, O.J. Open cholecystectomy in the laparoendoscopic era. Am. J. Surg. 2008, 195, 108–114. [Google Scholar] [CrossRef]
- Nebiker, C.A.; Mechera, R.; Rosenthal, R.; Thommen, S.; Marti, W.R.; von Holzen, U.; Oertli, D.; Vogelbach, P. Residents’ performance in open versus laparoscopic bench-model cholecystectomy in a hands-on surgical course. Int. J. Surg. 2015, 19, 15–21. [Google Scholar] [CrossRef]
- Chmielecki, D.K.; Hagopian, E.J.; Kuo, Y.; Davis, J.M. Laparoscopic cholecystectomy is the preferred approach in cirrhosis: A nationwide, population-based study. HPB 2012, 14, 848–853. [Google Scholar] [CrossRef]
- Schietroma, M.; Carlei, F.; Franchi, L.; Mazzotta, C.; Sozio, A.; Lygidakis, N.J.; Amicucci, G. A comparison of serum interleukin-6 concentrations in patients treated by cholecystectomy via laparotomy or laparoscopy. Hepatogastroenterology 2004, 51, 1595–1599. [Google Scholar]
- Buunen, M.; Gholghesaei, M.; Veldkamp, R.; Meijer, D.W.; Bonjer, H.J.; Bouvy, N.D. Stress response to laparoscopic surgery: A review. Surg. Endosc. 2004, 18, 1022–1028. [Google Scholar] [CrossRef]
- Targarona, E.M.; Pons, M.J.; Balagué, C.; Espert, J.J.; Moral, A.; Martínez, J.; Gaya, J.; Filella, X.; Rivera, F.; Ballesta, A.; et al. Acute Phase is the Only Significantly Reduced Component of the Injury Response after Laparoscopic Cholecystectomy. World J. Surg. 1996, 20, 528–534. [Google Scholar] [CrossRef]
- Watt, D.G.; Horgan, P.G.; McMillan, D.C. Routine clinical markers of the magnitude of the systemic inflammatory response after elective operation: A systematic review. Surgery 2015, 157, 362–380. [Google Scholar] [CrossRef]
- Burugu, H.R.; Kandi, V.; Kutikuppala, L.V.S.; Suvvari, T.K. Activities of Serum Ferritin and Treatment Outcomes Among COVID-19 Patients Treated with Vitamin C and Dexamethasone: An Uncontrolled Single-Center Observational Study. Cureus 2020, 12, e11442. [Google Scholar] [CrossRef]
- Huang, Y.-C.T.; Bassett, M.A.; Levin, D.; Montilla, T.; Ghio, A.J. Acute Phase Reaction in Healthy Volunteers After Bronchoscopy with Lavage. Chest 2006, 129, 1565–1569. [Google Scholar] [CrossRef]
- Arsalani-Zadeh, R.; Ullah, S.; Khan, S.; MacFie, J. Oxidative Stress in Laparoscopic Versus Open Abdominal Surgery: A Systematic Review. J. Surg. Res. 2011, 169, e59–e68. [Google Scholar] [CrossRef]
- Chambers, K.; Ashraf, M.A.; Sharma, S. Physiology, Hepcidin. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Suuronen, S.; Kivivuori, A.; Tuimala, J.; Paajanen, H. Bleeding complications in cholecystectomy: A register study of over 22,000 cholecystectomies in Finland. BMC Surg. 2015, 15, 97. [Google Scholar] [CrossRef]
- Tandon, A.; Shahzad, K.; Nunes, Q.; Shrotri, M.; Lunevicius, R. Routine preoperative blood group and save testing is Unnecessary for elective laparoscopic Cholecystectomy. J. Ayub Med. Coll. Abbottabad JAMC 2017, 29, 373–377. [Google Scholar]
- Huilin, L.; Guihua, L.; Zhaoxing, T. Changes in blood lymphocytes in sepsis patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2014, 26, 148–152. [Google Scholar]
- Ai, S.; Sun, F.; Liu, Z.; Yang, Z.; Wang, J.; Zhu, Z.; Du, S.; Guan, W. Change in serum albumin level predicts short-term complications in patients with normal preoperative serum albumin after gastrectomy of gastric cancer. ANZ J. Surg. 2018, 89, E297–E301. [Google Scholar] [CrossRef]
- Komáromi, A.; Estenberg, U.; Hammarqvist, F.; Rooyackers, O.; Wernerman, J.; Norberg, A. Simultaneous assessment of the synthesis rate and transcapillary escape rate of albumin in inflammation and surgery. Crit. Care 2016, 20, 370. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A1 | A2 | Statistic | p | |
|---|---|---|---|---|
| IL-6 pg/mL * | 6.9 (5.6) | 22.2 (17.7) | 3.9 | 0.001 |
| IL-8 pg/mL * | 9.4 (9.15) | 12.48 (17.48) | −2.59 | 0.00 |
| TNF-∝ pg/mL † | 24.45 (12.96) | 19.72 (12.19) | −3.16 | 0.00 |
| MDA μmol/L * | 2.43 (2.84) | 2.38 (1.98) | −1.45 | 0.14 |
| Ferritin μg/L * | 81 (143) | 85 (129) | −3.26 | 0.00 |
| Iron serum µg/dL † | 72.39 (40.61) | 65.25 (40.99) | −0.94 | 0.34 |
| Hemoglobin g/dL † | 13.14 (1.41) | 12.23 (1.72) | −5.12 | 0.00 |
| Prothrombin % * | 99 (9) | 91 (21.25) | −3.94 | 0.00 |
| Leukocytes cells/mm3 † | 7232.01 (2454.87) | 9386.3 (3540.53) | −4.73 | 0.00 |
| Neutrophils % † | 61.71 (9.24) | 74.21 (8.87) | −5.36 | 0.00 |
| Lymphocytes % † | 26.63 (8.4) | 17.01 (7.06) | −5.28 | 0.00 |
| N/L ratio * | 2.24 (1.22) | 4.70 (4.55) | −5.3 | 0.001 |
| CRP mg/L * | 2.6 (8.7) | 15.7 (30.25) | −5.49 | 0.00 |
| Albumin g/dL † | 4.28 (0.38) | 3.79 (0.39) | −5.38 | 0.00 |
| A1 | A2 | Statistic | p | |
|---|---|---|---|---|
| IL-6 pg/mL * | 16.6 (4.7) | 48.4 (23.5) | 1.8 | 0.07 |
| IL-8 pg/mL * | 13.92 (20.71) | 17.17 (15,47) | −0.7 | 0.48 |
| TNF-∝ pg/mL † | 26.60 (14.53) | 19.95 (9.1) | −1.4 | 0.16 |
| MDA μmol/L * | 2.67 (2.44) | 2.08 (1.06) | −1.4 | 0.16 |
| Ferritin μg/L * | 126 (133.25) | 195.5 (86.5) | −2.1 | 0.03 |
| Iron serum µg/dL † | 64.5 (32.28) | 28.12 (17.5) | −2.52 | 0.01 |
| Hemoglobin g/dL † | 12.47 (2.06) | 11.26 (2.46) | −2.1 | 0.03 |
| Prothrombin % * | 78 (13) | 76.5 (22) | −1.36 | 0.17 |
| Leukocytes cells/mm3 † | 7245 (2047.9) | 11,433.75 (2415.89) | −2.38 | 0.01 |
| Neutrophils % † | 58.4 (10.8) | 76.27 (9.52) | −2.52 | 0.01 |
| Lymphocytes % † | 29.27 (9.96) | 16.37 (8.64) | −2.52 | 0.01 |
| N/L ratio * | 2,42 (1.62) | 5.60 (5.28) | −2521 | 0.02 |
| CRP mg/L * | 3.45 (43.97) | 70.2 (47.7) | −2.24 | 0.02 |
| Albumin g/dL † | 3.95 (0.71) | 3.42 (0.66) | −2.52 | 0.01 |
| LC | OC | Statistic | p | |
|---|---|---|---|---|
| IL-6 pg/mL * | 22.18 (28.1) | 48.43 (52.7) | 101 | 0.057 |
| IL-8 pg/mL * | 12.48 (17.48) | 17.17 (15.47) | 124 | 0.21 |
| TNF-∝ pg/mL † | 19.72 (12.19) | 19.95 (9.10) | −0.04 | 0.96 |
| MDA μmol/L * | 2.38 (1.98) | 2.08 (1.06) | 153.5 | 0.56 |
| Ferritin μg/L * | 85 (129) | 195.5 (86.5) | 74.5 | 0.01 |
| Iron serum µg/dL † | 65.25 (40.99) | 28.12 (17.5) | 2.5 | 0.01 |
| Hemoglobin g/dL † | 12.23 (1.72) | 11.26 (2.46) | 1.35 | 0.96 |
| Prothrombin % * | 91 (21,25) | 76.5 (22) | 72.5 | 0.01 |
| Leukocytes cells/mm3 † | 9386.3 (3540.53) | 11,433.75 (2415.89) | −1.56 | 0.12 |
| Neutrophils % † | 74.21 (8.87) | 76.27 (9.52) | −0.59 | 0.55 |
| Lymphocytes % † | 17.01 (7.06) | 16.37 (8.64) | 0.22 | 0.82 |
| N/L ratio * | 5.424 (2.8257) | 6.1103 (3.5481) | −0,6 | 0.54 |
| CRP mg/L * | 15.7 (30.25) | 70.20 (47.7) | 178 | 0.00 |
| Albumin g/dL † | 3.79 (0.39) | 3.42 (0.66) | 1.52 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vila Zárate, C.; Martín González, C.; González Álvarez, R.J.; Soto Darias, I.; Díaz Pérez, B.; Abreu González, P.; Medina Arana, V.; Martínez Riera, A. Ferritin, Serum Iron and Hemoglobin as Acute Phase Reactants in Laparoscopic and Open Surgery of Cholecystectomy: An Observational Prospective Study. Pathophysiology 2022, 29, 583-594. https://doi.org/10.3390/pathophysiology29040045
Vila Zárate C, Martín González C, González Álvarez RJ, Soto Darias I, Díaz Pérez B, Abreu González P, Medina Arana V, Martínez Riera A. Ferritin, Serum Iron and Hemoglobin as Acute Phase Reactants in Laparoscopic and Open Surgery of Cholecystectomy: An Observational Prospective Study. Pathophysiology. 2022; 29(4):583-594. https://doi.org/10.3390/pathophysiology29040045
Chicago/Turabian StyleVila Zárate, Cristina, Candelaria Martín González, Ruimán José González Álvarez, Iván Soto Darias, Beatriz Díaz Pérez, Pedro Abreu González, Vicente Medina Arana, and Antonio Martínez Riera. 2022. "Ferritin, Serum Iron and Hemoglobin as Acute Phase Reactants in Laparoscopic and Open Surgery of Cholecystectomy: An Observational Prospective Study" Pathophysiology 29, no. 4: 583-594. https://doi.org/10.3390/pathophysiology29040045
APA StyleVila Zárate, C., Martín González, C., González Álvarez, R. J., Soto Darias, I., Díaz Pérez, B., Abreu González, P., Medina Arana, V., & Martínez Riera, A. (2022). Ferritin, Serum Iron and Hemoglobin as Acute Phase Reactants in Laparoscopic and Open Surgery of Cholecystectomy: An Observational Prospective Study. Pathophysiology, 29(4), 583-594. https://doi.org/10.3390/pathophysiology29040045